
Abstract
Background
Publicly funded health services face persistent challenges in meeting demand for specialty care, particularly in rhinology. Task shifting—the redistribution of clinical tasks from specialists to trained non-specialists—may offer a strategy to optimize health-care delivery. This study evaluates the outcomes of a nurse-led assessment pathway within an outpatient rhinology service in New Zealand.
Methods
To address increased demand for rhinology services, a registered nurse (RN) at Waikato Hospital was trained to perform initial assessments for patients referred for undifferentiated chronic nasal symptoms. We describe outcomes of this approach over the initial 18-month period.
Results
A total of 309 patients were assessed through the nurse-led pathway. The average wait time from referral to assessment decreased when compared to the specialist-led clinic. Most patients were discharged with a treatment plan that did not require specialist care. Patient feedback indicated high satisfaction with the nurse-led consultation.
Conclusion
Task shifting offers a promising solution to address resource constraints in publicly funded health-care systems. Nurse-led assessments can enhance efficiency and optimize care delivery without compromising quality. These findings suggest that task-shifting may be broadly applied to improve outcomes in other resource-constrained health-care settings.
Implications for Practice, Education, Research, or Policy
When pathways are appropriately customized, task shifting facilitates improved productivity. Complete rhinologic assessment through to discharge can be undertaken via a nurse-led pathway. Our nurse-led pathway was well received by patients.
Context
Rhinology encompasses the care of the nose, sinuses, anterior skull base, and related adjacent structures (Gao et al., 2025). Pathologies in these regions are relatively common and can have significant impact on quality of life (Blauwblomme et al., 2023; Hillerich et al., 2024; Kuiper et al., 2019). While rhinology disorders can be effectively treated by surgical and nonsurgical interventions (Wood et al., 2017), publicly funded health-care systems often face resource constraints. The ongoing impact of the recent COVID-19 pandemic, funding limitations, and workforce shortages has recently exacerbated inequities in patient access (Cate et al., 2021; Papagiannopoulos et al., 2021). With the growing demand for specialist services, there is increasing pressure for public health-care services to explore innovative models of care delivery (Duerson et al., 2019).
Task shifting is a process involving the systematic redistribution of tasks from specialists to trained non-specialists (Das et al., 2023). It has emerged as a strategy to address workforce shortage and improve efficiency in resource-constrained settings (Yankam et al., 2023). While task shifting has been adopted in global health contexts, its integration into specialist outpatient care in high-income settings remains limited (Seidman & Atun, 2017).
The initial assessment of rhinology patients is relatively stereotypical, making it suitable for remodeling through a task-shifted approach (Hopkins et al., 2022). In this project, we sought to evaluate the outcomes of a novel nurse-led rhinology assessment model in a tertiary hospital's publicly funded rhinology service.
The nurse led process was developed in alignment with task-shifting principles, emphasizing a systematic approach to optimize workload distribution and resource utilization. This initiative aimed to determine whether expanding the registered nurse (RN) role could improve health-care delivery without compromising clinical quality (Yankam et al., 2023). In doing so, this project contributes to the evidence base on how advanced nursing practice and interprofessional collaboration can drive creative solutions to systemic challenges in publicly funded health services. While this article focuses on the outcomes of task shifting within a tertiary otorhinolaryngology (ORL) clinic, the principles of task shifting may be applicable to a diverse range of clinical contexts.
Methods
Pathway Development
The nurse-led assessment pathway was developed collaboratively by a team of ORL specialists, RNs, and hospital administrative personnel. The task-shifting process was purposely structured to ensure that all tasks delegated to the nurse were supported by appropriate clinical training, supervision, and ongoing specialist oversight. Key aspects of the development process included:
With this framework, the task-shifted pathway was implemented.
Nurse-Led Assessment Process
The nurse-led assessment consisted of the following components.
Assessment Steps
Completion of a standardized rhinology history questionnaire which was developed internally, the 22-item Sino-Nasal Outcome Test (SNOT-22) (Hopkins et al., 2009), and the Impact on Life questionnaire (New Zealand Ministry of Health, n.d.), a prioritization tool utilized in New Zealand public hospitals.
A video-recorded nasal endoscopy to document mucosal health and identify anatomical pathologies.
A cone-beam computed tomography (CBCT) scan to examine paranasal sinuses and skull base.
An Epworth Sleepiness Score (Johns, 1991) was completed if symptoms suggesting sleep pathology were reported.
Virtual Appointment With a Subspecialty Rhinologist
Following the nurse-led assessment, a subspecialty rhinologist conducted a brief (approximately five minutes) virtual review of the data collected by the nurse.
Management Planning and Communication
Following the virtual clinic, the rhinologist generated a clinical summary outlining the observations, diagnosis, and recommended management plan. This summary was provided to the patient and their referring clinician.
Patient-Specific Care
Patients were provided with recommended management options following the rhinologist's evaluation of their assessment. Management options included recommendations for medical therapy in the primary care setting, follow-up consultation to discuss possible surgical intervention with an ORL specialist, or referral to a more appropriate service to deliver targeted management. The task-shifted assessment pathway is summarized in Figure 1.
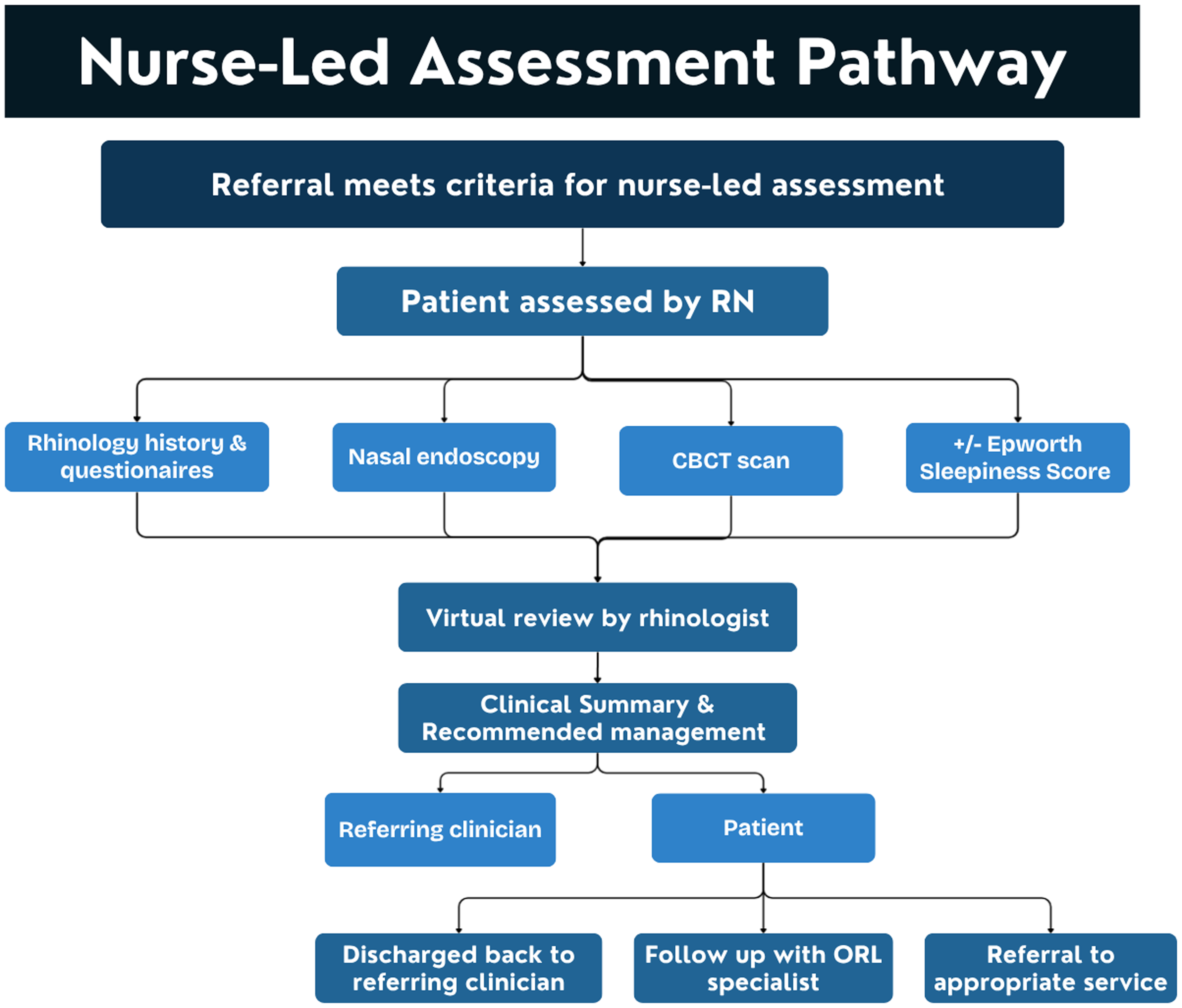
Overview of the nurse-led assessment.
Data Collection
Evaluation measures included both process measures and outcome measures. Quantitative data, including days between referral and initial assessment, number of patients assessed, and proportion of cases referred for follow up, were extracted from hospital records on the basis of a prospectively collected database.
Data from the initial 18 months of the nurse-led pathway (January 2023–July 2024) were compared to baseline data from the specialist-led pathway in the preceding 12-months (January 2022–December 2022).
In line with the institution's processes for patient surveys, qualitative data was collected using a brief, structured survey over a three-week period in 2023. Consecutive patients attending the nurse-led consult during the study period were included. Surveys were provided to the patient by the receptionist upon arrival to the clinic. Participation was voluntary and anonymous. Patients submitted their completed surveys into a box within the reception area before departure. Survey responses were collated with assistance from Waikato Hospitals Quality and Patient Safety team.
The survey explored six key domains:
Overall satisfaction with the nurse-led consultation Perceived medical competence of the nurse Perceived cultural competence of the nurse Quality of information delivery during the consultation Support for patient autonomy Patient's comfort during the assessment
Each item was rated on a four-point Likert scale (1 = very unsatisfied, 4 = very satisfied).
Two open-ended questions were included to gain deeper context of the participants’ responses.
What would you like to see change to improve the experience of receiving Ear Nose and Throat Service? What one thing would you like us to know about your experience with Ear Nose and Throat service?
Results
Over the initial 18-month period, 309 rhinology patients were assessed via the task-shifted, nurse-led pathway. Figure 1 shows a schematic overview of the assessment process from referral to clinical management.
Process Measures
Process measures evaluated the operational outcomes of the task-shifted model. Observed process measures included:
Outcomes Measures
No safety concerns or unexpected consequences were raised during the pathway's evaluation period.
Outcome measures evaluated the qualitative aspects of the pathway. Patient experience was assessed using survey responses collected over the 3-week study period in 2023.
Thirty consecutive patients were given surveys; and 28 patients completed them (response rate 93%). Survey responses reflected a universally positive experience with the nurse-led assessment. Key findings are summarized in Table 1.
Summary of Patient Survey Responses (N = 28).
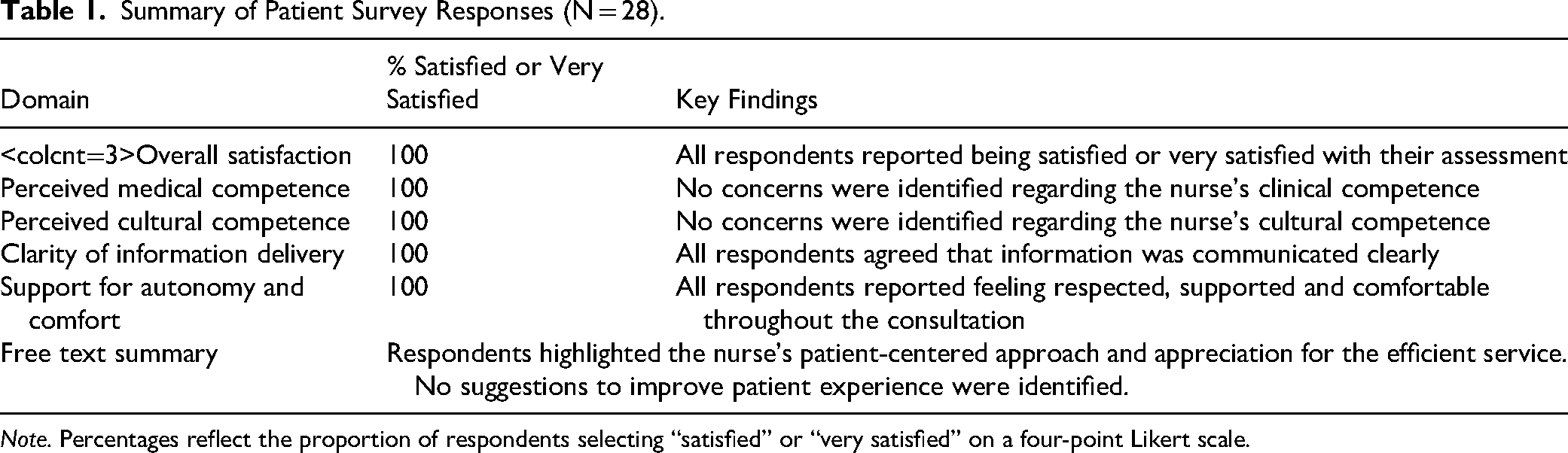
Note. Percentages reflect the proportion of respondents selecting “satisfied” or “very satisfied” on a four-point Likert scale.
Discussion
This project evaluated the outcomes of implementing a nurse-led assessment model in a high- income country (HIC) tertiary outpatient rhinology service. The findings demonstrate that implementing an appropriately structured task-shifting model was both safe and effective. This was reflected by patients experiencing reduced wait times for initial assessment, improved department workflow, and universally positive patient experience. Notably, 213 (69%) patients were discharged with a management plan that did not require in-person follow up with an ORL specialist. This optimized the use of specialist time. In settings where increasing demand and resource constraints challenge equitable access to care, these results reinforce task shifting as a feasible strategy to optimize service delivery.
The outcomes of this study align with evidence of task shifting in lower-middle income countries (LMIC). In these settings, well-defined task shifting models have been shown to increase accessibility, reduce costs, and improve outcomes without compromising clinical quality (Seidman & Atun, 2017). Our findings mirror these benefits, suggesting that task shifting rhinology care in a HIC is consistent with broader trends observed in diverse clinical settings. This contributes to the growing literature that, alongside strong governance and training, advanced nursing practice can safely manage the care of targeted patient cohorts (Htay & Whitehead, 2021).
Several contextual elements appear to have supported the successful implementation of the nurse-led assessment pathway.
Interdisciplinary Collaboration
The pathway was co-designed by a multidisciplinary team of RNs, ORL specialists, specialty radiologists, and hospital administrative staff. The collaborative development process ensured shared ownership, alignment with service needs, and clarity of scope.
Structured Training and Supervision Program
A well-defined training program and ongoing specialist oversight strengthened the RN's clinical competence and safeguarded patient welfare.
Stakeholder Engagement
The nurse-led assessment model was endorsed by the departments senior clinicians and aligned with the institutions priorities to improve equity and delivery of patient-centered care. Strong stakeholder support facilitated its timely integration into practice.
Positive Patient Engagement
Patients demonstrated a high level of appreciation and acceptance of nurse-led care, which likely contributed to its success.
Challenges
The nurse-led assessment model was implemented primarily at Waikato Hospital but was also extended to the outpatient clinic at Thames Hospital, a rural satellite site without direct access to CBCT imaging. To preserve the pathway's integrity, the rhinology team collaborated with the radiology department to establish linked appointments. Patients were scheduled to obtain CT imaging with the radiology team immediately prior to their nurse-led assessment. This enabled the same nurse-led pathway to be implemented at Thames Hospital. After this adaptation was established, similar improvements in process measures and patient outcomes observed at Waikato Hospital were seen at Thames Hospital. Although contextual barriers exist, this demonstrated that with multidisciplinary collaboration and effective communication, task-shifted models are adaptable to diverse clinical contexts.
At Waikato Hospital, no concerns or unexpected challenges were raised during the evaluation period. No changes to the nurse-led assessment pathway have been made since its inception.
Limitations
Despite the promising findings, several limitations warrant consideration. The sample size (309) was modest and drawn from a single tertiary center, which may limit generalizability. The absence of randomization and blinding introduces potential investigator bias. Retrospective evaluation of the comparator group carries risk of confounding variables such as seasonal variation in referral volumes and fluctuating specialist availability. Additionally, participation in the patient survey was voluntary, introducing the risk of response bias in observed outcome measures.
Future research using prospective and/or randomized control study designs would strengthen the evidence base for the task-shifted model. Additionally, cost-effectiveness analyses, long term observational studies to evaluate clinical impacts such as earlier detection of malignancy, and measuring reduced need for specialist review would provide valuable insight.
Despite these limitations, this study provides important early evidence to support task shifting as a safe, efficient, and acceptable approach to address resource constraints in health-care services within HICs.
Conclusion
This project demonstrates that a nurse-led assessment pathway can safely and effectively manage a defined cohort of patient referrals within a tertiary rhinology service. The task-shifted pathway decreased wait times for initial assessment, reduced specialist clinician workload, and optimized resource utilization. Patients reported high levels of satisfaction when engaging with the nurse-led care. These findings contribute to the growing evidence that an appropriately structured task-shifting initiative can increase access and enhance service efficiency without compromising clinical quality.
Implications for Practice
The study findings suggest several key implications for clinical practice. Nurse-led assessment pathways can safely reduce wait times and improve service efficiency in resource-constrained settings. Task shifting optimized the use of an RN's expertise, increasing specialists’ availability for clinically complex tasks. High patient satisfaction demonstrated that nurse-led care can uphold provision of quality health care. Structured training, interdisciplinary collaboration, and ongoing specialist supervision were essential for the pathway's safe implementation and for protection of patient welfare. The task-shifted model demonstrated adaptability across diverse clinical settings, suggesting that these findings may be applicable to other outpatient services with standardized assessment pathways.
Footnotes
Acknowledgments
The authors thank the Waikato Hospital ORL service, administrative staff, and institutional personnel for their support in developing and evaluating the nurse-led assessment pathway. We extend our appreciation to the patients who participated in the service evaluation.
Ethical Approval
Ethical approval for this study was granted by the Central Health and Disability Ethics Committee (HDEC) (Reference: 2025 EXP 21170). Locality approval was provided by the Te Whatu Ora Waikato Research Committee.
Informed Consent
The patient feedback survey was administered in accordance with hospital consumer engagement guidelines. Patients were fully informed of the purpose of the study, and all responses were anonymized. Consent was implied through voluntary completion of the survey.
Author Contributions
ES: writing—original draft and review and editing . SB: conceptualization, methodology, and data curation. MR: formal analysis and writing—review and editing . AJW: conceptualization, data curation, and methodology and supervision .
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
This service evaluation was conducted within the Otorhinolaryngology service at Waikato Hospital as part of ongoing quality improvement activities.
Data Accessibility
The data supporting the findings of this study are openly available in Clinical Nursing Research at the following.