
Abstract
Aims
This study aimed to map and analyze scientific evidence on nursing interventions to welcome the families of critically ill patients.
Design
Scoping review.
Data Sources
In January 2024, a comprehensive search of studies published between 2018 and 2024 was conducted across the following databases: PubMed; MEDLINE Complete; Cumulative Index to Nursing and Allied Health Literature (CINAHL) Complete; Cochrane Central Register of Controlled Trials; Cochrane Database of Systematic Reviews; and MedicLatina.
Review Methods
The framework proposed by Arksey and O'Malley guided the scoping review and was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist.
Results
A total of 827 records were initially retrieved and screened. Twelve studies were selected for complete analysis. Nursing interventions for welcoming families of critically ill patients fall into four categories: information provision, emotional support, unit environment adaptation, and family involvement.
Conclusion
Welcoming families provides a valuable opportunity for early identification of their needs, enabling the establishment of a therapeutic relationship and tailored interventions that support family-centred care.
Impact
This study highlights the importance of structured nursing interventions in welcoming families to intensive care settings. By addressing families` needs, these interventions contribute to improved emotional stability, family functioning, and potentially better outcomes for critically ill patients.
Implications for Practice, Education, Research, or Policy
Families of critically ill people experience high emotional distress, uncertainty, and difficulty understanding complex clinical information. Nurses should provide information, offer emotional support, adapt the unit environment, and actively involve the families. Welcoming should be understood not as a single moment, but as a continuous, person- and family-centred process integrated throughout the care trajectory.
Nursing care in the clinical context of critically ill patients is closely tied to the technical and rapid execution of complex procedures. This environment, where the possibility of end-of-life care is ever-present, often leads to anxiety for the patient, their families, and the nurses working in these settings (Sá et al., 2015). Numerous studies have highlighted that nursing teams in critical care units prioritize patient care, often neglecting the families’ needs (Ramos et al., 2018).
Both the patients and their families uniquely perceive the experience of a life-threatening situation. While the patients are often unconscious and may only fully comprehend the severity of their condition during the recovery phase, the families endure the situation intensely, filled with emotions related to changes in their loved one's clinical condition (Sá et al., 2015). From a holistic perspective, families should be regarded not merely as the context of the ill person but as entities deserving of nursing care (Sá et al., 2015). Ramos et al. (2018) asserted that the family is an extension of the person, revealing itself as a recipient of care by the nursing team.
Mendes (2015) emphasized the importance of welcoming the families, starting with the initial moments of building trust between the nurse and the families. Welcoming means receiving, accepting, and acknowledging the other as a subject with rights and desires, and as co-responsible for health promotion, individually and collectively (Maestri et al., 2012). The act of welcoming involves actively listening to the individual and fostering a relationship where both parties can interact and engage in a shared understanding, which is essential for the genuine act of care (Sá & Botelho, 2015). The first contact with families provides insight into how they approach the healthcare service, highlighting the importance of recognizing their vulnerability. Nursing care should be as humanized as possible, addressing critically ill patients and their families (Mendes, 2015). Nurses play a crucial role from the initial moment of the family's reception; during this first visit, opinions about the professionals are formed, making it a vital opportunity to ensure that first impressions are positive (Cabete et al., 2019). However, welcoming extends beyond the first visit and is continuous throughout the patient's hospitalization. It should be centered on family care and viewed as an integral part of the care for the critically ill patients (Mendes, 2019). The same author underscores that welcoming should become a daily intervention for nurses, rooted in careful observation of both verbal and nonverbal communication from each family member.
Given these considerations, this review aimed to map and analyze the scientific evidence on nursing interventions for welcoming the families of critically ill patients.
Methodology
This scoping review was conducted following the five phases outlined in Arksey and O'Malley's (2005) methodological framework. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist was used to ensure transparent reporting and quality of the review process.
Phase 1: Identification of the Research Question
In developing the research question, the mnemonic PCC, which stands for Participants, Concept, and Context, was applied in accordance with the recommendations of the Joanna Briggs Institute (Aromataris et al., 2024) for scoping reviews. This led to the formulation of the following research question: What are the nursing interventions for welcoming the families of critically ill patients?
Phase 2: Identification of Relevant Studies
A comprehensive search was conducted across the following databases: PubMed (568), MEDLINE Complete (109), Cumulative Index to Nursing and Allied Health Literature (CINAHL) Complete (112), Nursing & Allied Health Collection: Comprehensive (18), Cochrane Central Register of Controlled Trials (12), Cochrane Database of Systematic Reviews (2), and MedicLatina (6). The final search was performed on January 25, 2024.
This review used the following indexed Medical Subject Headings descriptors: Nurs*; family; critical illness; critically ill patients and the Boolean operators AND and OR, creating the following Boolean equation: (Nurs*) AND (family) AND [(Critical illness) OR (critically ill patients)].
Phase 3: Study Selection
The initial search across the selected databases included filters aligned with the inclusion criteria. However, some articles were inaccessible in full text and were therefore excluded.
The search results were exported to the RAYYAN bibliographic manager, and all duplicate studies were removed. A researcher then analyzed the titles and abstracts of the remaining articles. The studies deemed relevant were retrieved in full text and evaluated based on the inclusion criteria defined earlier. The PRISMA (ScR) Flowchart (Figure 1) was used as the primary tool by the researcher, outlining the stages of identification, screening, and study selection.
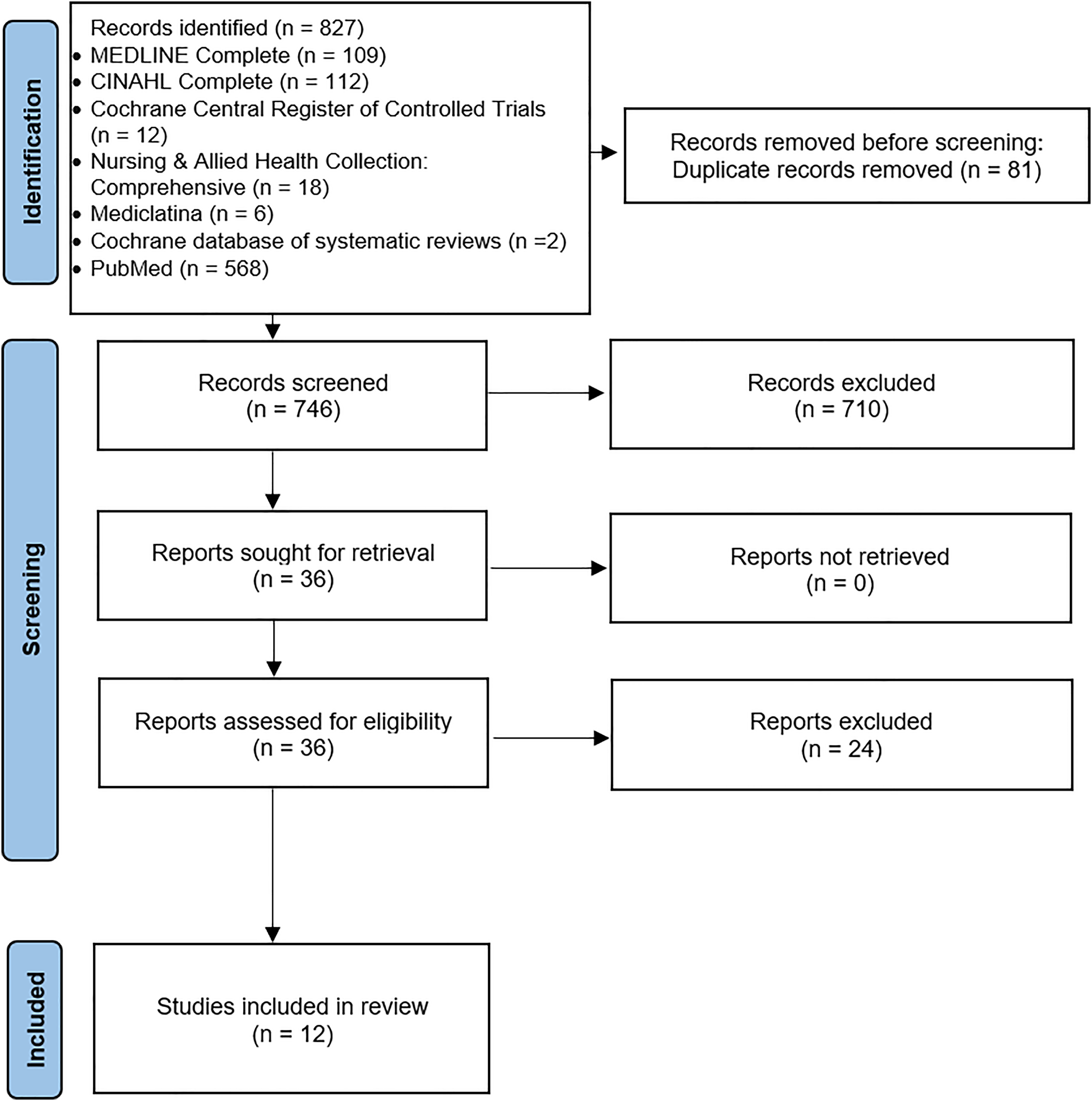
PRISMA flow chart for study selection.
Phase 4: Data Recording
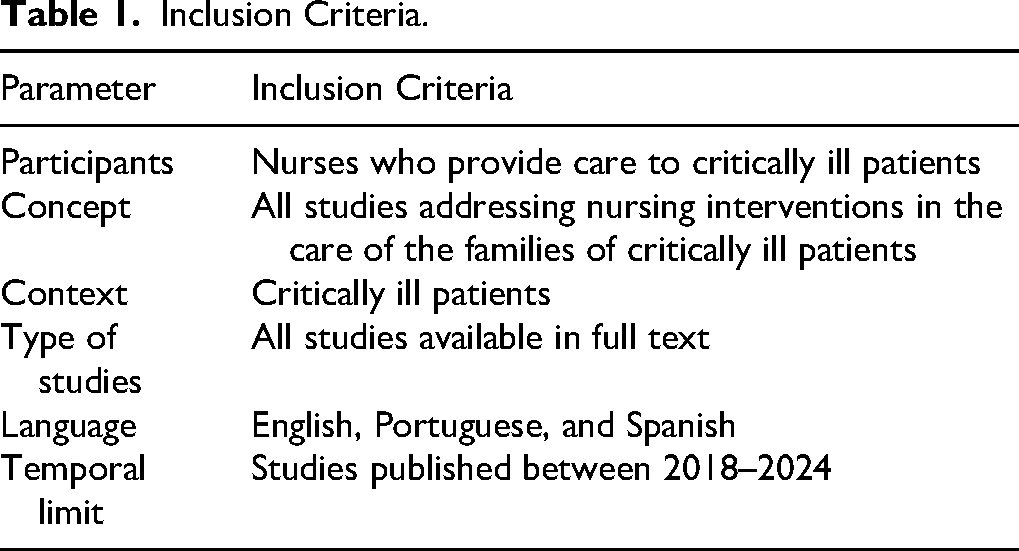
Two researchers extracted the data using a purpose-designed instrument (Table 1), aligned with this scoping review's objective and research question. The following data were extracted: general information (author(s), year, title, and source), study objective, methodology, and results (interventions for welcoming the families of critically ill patients).
Inclusion Criteria.
All documents that did not meet the selection criteria were excluded from this scoping review.
Phase 5: Collection, Summary, and Presentation of Data
Thematic analysis was employed to organize and summarize the data. Inductive categorization was applied within the interventions to gather and analyze the data, allowing them to be grouped into meaningful categories (Braun et al., 2019).
Results
The initial search in this scoping review yielded 827 articles. After eliminating duplicates, 746 titles were reviewed, with 96 selected for abstract reading. From these, 36 articles were eligible for full-text review, and 12 met all eligibility criteria and were included in the scoping review.
Twelve articles published between 2018 and 2024, that addressed nursing interventions in the care of the families of critically ill patients were selected for analysis. Regarding the country of origin of the documents, it is noted that three come from Portugal (Mendes, 2018, 2019; Sá & Henriques, 2021), two from Canada (Kalocsai et al., 2018; Lebel & Charette, 2021), two from Colombia (Parada et al., 2021; Suárez & Blandon, 2021), one on five continents (Australia, Austria, England, Hong Kong, Japan, New Zealand, Saudi Arabia, South Africa, Switzerland, USA) (Naef, Brysiewicz et al., 2021), one in Germany (Hoffmann et al., 2025), one in Australia (Naef, von Felten et al., 2021), one in Switzerland (Naef et al., 2022) and one in South Africa (Beer & Brysiewicz, 2019).
In terms of methodology, the 12 articles are distributed as follows: three integrative literature reviews (Lebel & Charette, 2021; Parada et al., 2021; Sá & Henriques, 2021), two qualitative phenomenological studies (Mendes, 2019; Mendes, 2018), one grounded theory study (Beer & Brysiewicz, 2019), one quantitative cross-sectional descriptive study (Suárez & Blandon, 2021), one qualitative study (Kalocsai et al., 2018), a parallel multicenter superiority hybrid trial (Naef et al., 2022), a prospective study (Naef, von Felten et al., 2021), a narrative review (Hoffmann et al., 2025), and a multifocal qualitative-descriptive study (Naef, Brysiewicz et al., 2021).
Supplemental File 1 summarizes the included articles, consolidating their most significant characteristics and results. The information collected was grouped into four categories in order to answer the research question previously defined.
Information for the Family
Several authors highlight the information category as a critical intervention to inform the families about the patient's care, daily health status, illness, and ICU environment and technology. Nurses should provide this information regularly, fostering trust between the nurse and the families, which helps reduce anxiety and distress in the face of an unfamiliar environment and the sudden onset of illness (Beer & Brysiewicz, 2019; Lebel & Charette, 2021; Mendes, 2018; Mendes, 2019; Naef, von Felten et al., 2021; Sá & Henriques, 2021; Suárez & Blandon, 2021).
Many authors (Beer & Brysiewicz, 2019; Lebel & Charette, 2021; Mendes, 2018; Sá & Henriques, 2021; Suárez & Blandon, 2021) note that while the families often receive clinical information from the medical team, the use of medical terminology can make it difficult for them to understand. Nurses often clarify and translate this information into accessible terms, helping the families comprehend it clearly without feeling confused or overwhelmed by medical jargon. This support also allows the families to better focus on the critical situation and understand the trajectory of the patient's illness.
According to Lebel and Charette (2021), nurses should adjust the information they provide based on families’ level of understanding and the stress they are experiencing, while also assessing families’ prior knowledge of the patient's condition.
Multidisciplinary meetings, including the nurse, and therapeutic conversations can empower families to adapt to the new reality, gain insight into their loved one's health prognosis, and express their emotions, fears, and concerns. During these interactions, the families can feel heard by the nurse without judgment, respecting their right to confidentiality (Kalocsai et al., 2018; Naef et al., 2022; Suárez & Blandon, 2021).
One of the most essential skills in nursing is effective communication, which requires developing strategies to engage with the families in a clear, direct, and honest manner. This approach fosters trust and confidence in the nurse, helping families feel informed while also allowing them space to ask questions without fear of embarrassment (Kalocsai et al., 2018; Naef, Brysiewicz et al., 2021; Parada et al., 2021; Sá & Henriques, 2021; Suárez & Blandon, 2021).
Other authors stress the importance of being attuned to both verbal and nonverbal cues when communicating with the families of critically ill patients, as the families are undergoing significant emotional stress. Nurses should also be mindful of nonverbal communication, offering a welcoming gaze, human touch, active listening, and maintaining eye contact. This fosters trust and ensures the families feel supported throughout their journey (Kalocsai et al., 2018; Mendes, 2019; Sá & Henriques, 2021; Suárez & Blandon, 2021
Nurses should also recognize the potential need for ethical counseling when the families face decisions about their loved one's medical care (Hoffmann et al., 2025). Additionally, in contexts where families may speak a foreign language, nurses should ensure the availability of translators to ensure clear and effective communication (Hoffmann et al., 2025).
Emotional and Psychosocial Support
Initially, nurses must assess the families structure and the support available to them (Naef et al., 2022). A key component of nursing care is promoting the humanization of care for the patients and their families. Understanding the patients’ wishes, as well as those of their families, is crucial for facilitating a welcoming process for both parties (Kalocsai et al., 2018; Mendes, 2019; Parada et al., 2021; Suárez & Blandon, 2021).
Demonstrating empathy and providing human touch fosters a sense of support and helps establish a connection between the nurse and the families (Beer & Brysiewicz, 2019; Mendes, 2018; Naef, von Felten et al., 2021; Parada et al., 2021; Sá & Henriques, 2021). Respecting and understanding the families’ values, beliefs, and attitudes is an inherent aspect of professional nursing care (Beer & Brysiewicz, 2019; Suárez & Blandon, 2021).
Nurses need to identify early signs of vulnerability, anxiety, and stress in the families through verbal and non-verbal cues, enabling them to intervene and mitigate the emotional impact on the families (Mendes, 2018; Naef, von Felten et al., 2021; Parada et al., 2021). Providing advice on the patients’ critical condition and being available for clarification supports the families’ transition and helps manage their expectations and hope (Naef, von Felten et al., 2021; Naef et al., 2022; Sá & Henriques, 2021).
The nurse should also offer emotional support through concrete gestures such as providing water, a smile, or a hug, as well as spiritual and psychological support (Hoffmann et al., 2025; Kalocsai et al., 2018; Lebel & Charette, 2021; Sá & Henriques, 2021; Suárez & Blandon, 2021). Additionally, social support can be facilitated by connecting the families with a social worker (Lebel & Charette, 2021).
If the families desire, the nurse should provide contacts for peer support groups, particularly for families experiencing similar situations. Sharing experiences can alleviate anxiety and foster a sense of mutual support (Hoffmann et al., 2025; Parada et al., 2021; Sá & Henriques, 2021).
Consistent, daily engagement with families (preferably involving family caregivers to enhance nursing staff continuity) enhances the nursing team's sense of connection and reduces the need for the team to proactively seek out families (Mendes, 2018).
Unit Environment
One pertinent issue in critical care services is the lack of physical space for families to stay with their loved ones, compounded by the high-tech environment surrounding patient care (Lebel & Charette, 2021). Another significant challenge for families is the turnover of nurses. Given the size of these services and the large nursing teams, high turnover is expected, making it difficult for families to establish trust with professionals, as each nurse brings their personality and style (Kalocsai et al., 2018).
The unique characteristics of critical care services, along with the often unstable clinical condition of the patients, make it essential for nurses to create a welcoming environment for families, both within the service and the specific unit where their loved one is being treated (Mendes, 2019; Sá & Henriques, 2021).
It is also important to have designated spaces within the service where the multidisciplinary health team can meet and areas where families can reflect communicate with each other and share experiences. Such spaces allow families to mobilize resources and support one another through mutual understanding (Naef, Brysiewicz et al., 2021).
Additionally, because families often spend considerable time on these services, providing a suitable waiting area is vital. This space should be welcoming, comfortable, and equipped with amenities like vending machines for food and drinks, ensuring that families can visit and stay informed about their loved ones’ status (Beer & Brysiewicz, 2019; Naef, Brysiewicz et al., 2021).
Facilitating Family Involvement
Families and significant others are the pillars of support for critically ill patients, and their presence is essential. Nurses play a vital role in reducing the patients’ feeling of isolation, and one way to support this is by encouraging families to bring personal items, such as photographs or sentimental objects, to the patients’ room (Parada et al., 2021; Kalolo et al., 2023).
Flexible or ‘open-door’ visiting hours are also recommended, allowing family members who work or have scheduling conflicts to be present more easily (Hoffmann et al., 2025; Lebel & Charette, 2021; Naef, von Felten et al., 2021; Parada et al., 2021;). In addition, creating a child-friendly visiting space with professional support can help maintain families’ connections for younger relatives in a developmentally appropriate way (Hoffmann et al., 2025).
The nurse's presence during family visits is essential for building trust, answering questions, and simply offering support, which helps sustain the bond between the patients and their families (Hoffmann et al., 2025; Mendes, 2018). Involving family members are basic care activities, like applying lotion or providing water, enhances satisfaction and strengthens the connection between families and patients (Hoffmann et al., 2025; Kalocsai et al., 2018; Lebel & Charette, 2021; Mendes, 2018; Naef, von Felten et al., 2021; Suárez & Blandon, 2021). Observing these care practices also reassures families of the patients’ respectful treatment and care quality (Kalocsai et al., 2018; Suárez & Blandon, 2021).
The presence of nurses during visits can also facilitate health education and self-management guidance, supporting the families’ understanding and involvement in the patients’ care (Hoffmann et al., 2025). Accepting family members’ decisions about their loved ones helps alleviate any guilt they may carry (Suárez & Blandon, 2021). Lastly, ensuring families access during a patient's final moments, if desired, is a fundamental aspect of compassionate end-of-life care (Suárez & Blandon, 2021).
Discussion
Based on the research conducted for this scoping review, a total of 12 articles were selected, each addressing nursing interventions for the families of critically ill patients in response to the research question. Of these, 10 articles focus on interventions within the ICU setting, while two take a broader approach, examining emergency care environments. This limited evidence highlights a gap in research specifically exploring nursing interventions for families in emergency settings.
The studies demonstrate a global concern for this topic, with research spanning four continents, and one study even encompassing all five continents, underscoring a shared emphasis on humanizing care. Authors have consistently affirmed that relationship-building is a fundamental aspect of humanized care. Nurses are encouraged to provide proactive, competent support to patients and families alike, fostering a warm, reassuring environment that conveys stability and continuous presence. When implemented daily, these interventions offer families comfort and peace of mind, as highlighted by various authors (Mendes, 2019; Michelan & Spiri, 2018; Proença et al., 2017).
This evidence suggests that integrating humanizing, family-centered nursing practices can significantly enhance the ICU and emergency care experience for families, underscoring the importance of further research in this area.
Data analysis from this scoping review underscores the critical role of nurse-provided information in supporting families, as clear communication facilitates a feeling of welcome within the healthcare environment. Several authors concur, emphasizing that families benefit significantly from well-communicated, honest information even amid the distress of a loved one's critical illness. This transparency in prognosis helps families adapt to the situation and fosters trust in healthcare providers (Kalolo & Gundo, 2023; McKiernan & McCarthy, 2010; Mendes, 2016).
Nurses’ communication skills significantly affect how families cope with the emotional turmoil of critical illness. Authors affirm that a nurse's competence in relaying information and fostering effective communication is essential in empowering families who face an unpredictable and challenging experience. This need for clarity is a genuine priority for families, positively impacting the therapeutic relationship with health professionals and helping families feel more supported in their journey (Edward et al., 2020; Harlan et al., 2020; Hetland et al., 2018; Kalolo & Gundo, 2023; Proença et al., 2017).
In examining the unit and waiting room environments within critical care settings, it is evident that family members often face limited conditions when staying with their loved ones and spending time in the waiting area. Such constraints affect how welcome families feel within the clinical setting; a lack of comfortable accommodations can diminish their experience, particularly when enduring extended periods in these spaces (Edward et al., 2020; Kalolo & Gundo, 2023).
Nurses must recognize and empathize with the complex emotions families encounter – anguish, sadness, anger, and fear – as these are natural responses during a health crisis. By acknowledging the strain illness places on families’ routines, nurses can be supportive, providing families with outlets to express these feelings and validating their beliefs. When desired, offering spiritual or psychological support helps ease their suffering, creating a more compassionate environment (Edward et al., 2020; Harlan et al., 2020; Kalolo & Gundo, 2023).
Moreover, involving families in the care process—whether by facilitating visits, allowing them to witness caregiving interactions, or teaching them specific aspects of their loved one's care—strengthens their sense of inclusion and support. This active engagement enhances families’ well-being and fosters a greater connection with the nursing team (Haave et al., 2021; Kalolo & Gundo, 2023).
Implications for Nursing
The findings of this scoping review highlight the relevance of family-centered care in critical care settings. The identified interventions reinforce the nurse's role in promoting effective communication, welcoming families, and recognizing them as an integral part of the care process. These results may support the development of protocols and strategies that encourage families’ presence, participation, and emotional support, contributing to the humanization of care, the reduction of family distress, and improved experiences during hospitalization in critical care units.
Limitations of Study
This scoping review has several limitations that should be considered when interpreting its results. First, the selection of studies was limited to articles published in specific databases and certain languages, which may have excluded other relevant evidence available in different languages or lesser-known sources. Another limitation is the scarcity of studies specifically addressing the topic in emergency settings, which restricts our understanding of the full scope of nursing interventions across different clinical settings. Finally, it is essential to note that a scoping review, by its nature, does not allow for a quality assessment of the included studies, preventing robust inferences regarding the effectiveness of the interventions analyzed. Consequently, the findings of this review should be interpreted as indicative of current practices and gaps in the literature, serving as a foundation for future research to explore nursing interventions for family support in critical care settings more in-depth and systematically.
Conclusion
Nurses should prioritize caring for families as an integral part of the support provided to critically ill patients, recognizing that involving families in care can positively influence patients’ recovery. The complex environment and intensity of care in critical care settings can profoundly impact family members, often creating feelings of stress and helplessness.
In this context, welcoming families becomes an essential opportunity to identify their needs early on and establish a therapeutic relationship. This allows for planning personalized interventions that can mitigate the emotional impact on families. Nurses should view welcoming as an initial contact and an ongoing process, recognizing that families face emotionally challenging experiences and significant changes in their daily lives. By approaching families with empathy and building a relationship of trust, nurses become a supportive figure to whom families can turn for emotional support and information about their loved one's condition.
Additionally, involving families in caring for their loved ones can promote satisfaction and build trust in the nurse, as it allows family members to witness the quality of care their loved one is receiving, thus reducing anxiety. In this role, the nurse facilitates the transition process, helping both patients and families adapt to the new reality by equipping them with skills and knowledge to cope with the situation as effectively as possible.
Supplemental Material
sj-docx-1-cng-10.1177_10784535261450611 - Supplemental material for Welcoming Families in Critical Care: A Scoping Review
Supplemental material, sj-docx-1-cng-10.1177_10784535261450611 for Welcoming Families in Critical Care: A Scoping Review by Inês Romão, Célia Tavares Vaz, Júlio Belo Fernandes and Cidália Castro in Creative Nursing
Footnotes
Author Contributions
Conceptualization, I.R. and C.T.V.; methodology, I.R., C.T.V. and C.C; formal analysis, I.R., C.T.V., C.C. and J.B.F.; investigation, I.R., C.T.V., C.C. and J.B.F.; data curation, I.R. and C.T.V.; writing—original draft preparation I.R., C.T.V., C.C. and J.B.F.; writing—review and editing I.R., C.T.V., C.C. and J.B.F.; visualization, I.R., C.T.V., C.C. and J.B.F.; supervision, C.T.V. and C.C.; project administration, I.R.
All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.