
Abstract
Keywords
Implications for Practice and Research
Domestic violence and abuse (DVA) is complex and multidimensional, affecting people of all ethnicities, cultures, sexual orientations, gender identities, socioeconomic classes, mental capacities, physical abilities, and age at any point during the life-course. It is possible that pandemic-related public health measures could have contributed to explain the rise in reported incidents and that lockdown measures created enabling environments that exacerbated existing abusive situations. Assessing and responding to the needs of persons experiencing DVA is complex even in normal circumstances; remote consultations added extra pressures, especially in determining their safety needs.
Domestic violence and abuse (DVA) refer to any incident or pattern of incidents of controlling, coercive, or threatening behavior, violence, or abuse between those aged 16 or over who are, or have been, intimate partners or family members, regardless of gender or sexuality; this can encompass, but is not limited to, psychological, physical, sexual, financial, or emotional abuse (Home Office, 2023). Acts of so-called “honor”-based violence, female genital mutilation, and forced marriage are also included in this definition (Home Office, 2023). DVA is complex and multidimensional, affecting people of all ethnicities, cultures, sexual orientations, gender identities, socioeconomic classes, mental capacities, physical abilities, and age at any point during the life-course. Strong evidence highlights the social, economic, physical, and mental health impacts of DVA (Black, 2011; Reuter et al., 2017; World Health Organization, 2013). As a result, responding to DVA is a global challenge for health and social care services, made more challenging during the coronavirus disease 2019 (COVID-19) pandemic (Ali et al., 2021).
Calculating the economic costs of DVA to health-care provision in the UK is problematic due to the varied ways data are collected and definitional inconsistencies found across existing studies. However, Oliver et al. (2019) have estimated these costs at £66 billion (Oliver et al., 2019). This high estimate is predictable, as it has become increasingly apparent in scholarship that it is practitioners in primary and secondary health services (including general practitioners [GPs], nurses, health visitors, emergency and ambulance staff, midwives, and sexual health practitioners) who are often the first point of contact for people experiencing DVA rather than police, social care, or other helping professions (Centre for Social Justice, 2022). Indeed, victims–survivors of DVA frequently identify health-care practitioners as the professionals whom they would be most likely to speak to about their experiences (SafeLives, n.d.). However, Al-Natour et al. (2016) state that health-care professionals are often reluctant to ask about DVA due to a lack of confidence, not wanting to offend patients, not knowing where to refer DVA victims–survivors for further support, and/or a lack of time.
Despite these challenges to engaging with victims–survivors, effective recognition, management, and pathways to care in response to DVA are now acknowledged to be key priorities for health-care settings in the UK (McGarry & Ali, 2016). Professional standards across health care reflect the recognition that responding to DVA is “everybody's business” (Home Office, 2016; National Institute for Health and Care Excellence [NICE], 2014). To support the rhetoric of DVA being “everybody's business,” there is national guidance on how to respond and in relation to recording information (Department of Health, 2017). These guidelines have been described as ambiguous in terms of which health-care professionals should have access to a patient's information pertaining to DVA (Chandan et al., 2020). In addition, Dheensa (2020) claims that DVA is still under-recorded in GP; an analysis of domestic homicides (Sharp-Jeffs & Kelly, 2016) cites poor record keeping as a factor in failing to prevent harm or death.
Helping Health-Care Professionals Respond to Domestic Violence and Abuse
As doctors, nurses, midwives, and other health-care professionals often do not feel confident and competent in their ability to identify and respond to DVA (Al-Natour et al., 2016), there is a need to increase awareness and provide appropriate training for health-care professionals in order to understand what they can do to support patients affected by DVA. Training and interventions do exist. In 2011, Feder et al. (2011) published the results of a pilot study of the Identification and Referral to Improve Safety (IRIS) program. Conducted in GP practices across two cities in the UK, the pilot study had considerable success demonstrating that the IRIS intervention increased the identification and referral of patients experiencing DVA. IRIS was found to be cost-effective (Barbosa et al., 2018) and is now cited as an example of best practice in national policy as an evidence-based DVA intervention (Home Office, 2016).
IRIS is a collaboration between health-care systems and charitable organizations who support DVA victims. IRIS aims to improve recognition of and responses to DVA through referral from GP teams to support provided by DVA specialists. The core components of the IRIS program include ongoing training and education on DVA for GP teams; consultancy for the clinical team and administrative staff; and a process for direct referrals for patients experiencing DVA to specialist DVA practitioners (the IRIS service). The IRIS program involves the addition of computer software into GP infrastructure to prompt health-care professionals and other staff members to ask patients about DVA to improve disclosure rates, recording, and access to specialist support. These training and infrastructure changes create an enhanced referral pathway for primary health-care practitioners to refer patients who experience DVA to specialist services. Through the IRIS program, health-care professionals in more than 850 GPs have been trained, and these practices have referred more than 14,000 patients since 2011 (IRISi, 2024).
The onset of COVID-19 and subsequent national response elicited diverse literature describing the impact of COVID-19 on DVA (Ali et al., 2021). It is possible that the impact of pandemic-related public health measures (shielding, multiple national lockdowns, social distancing, and working from home measures) could have contributed to the rise in reported incidents; Peterman et al. (2020) argued that lockdown measures created enabling environments that exacerbated existing abusive situations. While there were indeed reports of increased DVA during the first lockdown period in 2020, caution should be taken not to conflate this with evidence of a rise in prevalence, as DVA existed prior to the pandemic, but these measures indisputably changed social, economic, and individual conditions, altered the response of victims–survivors to abuse, and may have triggered other behaviors such as increased help-seeking.
COVID-19 affected not only patients/service users but also health-care professionals and the way they interacted. The pandemic put a lot of pressure on nurses, midwives, and other health-care professionals, especially those working in primary care settings, who were required to adapt quickly by learning new ways to assess and manage their patients, mostly using remote consultations. Assessing and responding to the needs of persons experiencing DVA is complex even in normal circumstances, and remote consultations added extra pressures, especially in determining safety needs. As modern health-care systems have not been exposed to events like the COVID-19 pandemic, there was no guidance about how to appropriately identify and support people who may be experiencing DVA in situations governed by measures such as the national lockdown. However, principles and practices were developed to enable professionals in supporting patients/service users. Much research is needed to understand the usefulness of interventions such as remote consultations generally and for assessing and addressing the needs of those affected by DVA, to establish what can be learnt about the modifications that the pandemic necessitated.
This paper reports the findings of an evaluation of the IRIS program based in a city in England. The authors were commissioned to explore victims’–survivors’ access to and experience of support via remote interventions during COVID-19, as well as the perspectives of referring agents (doctors and other health-care practitioners based in GP).
Identification and Referral to Improve Safety
IRIS is a specialist DVA training, support, and referral program for GPs that has been positively evaluated in a randomized controlled trial (Feder et al., 2011). It is a partnership between primary health care and the specialist DVA sector. IRIS provides in-house DVA training for GP teams and a named advocate to whom patients can be referred for support.
Referral Pathway
The advocate educator is a specialist DVA worker who is linked to the practices and based in a local specialist DVA service.
The advocate educator provides training to the practice teams and acts as an ongoing consultant as well as the person to whom they directly refer patients for expert advocacy.
The advocate educator works in partnership with a local clinical lead to engage with practices and codeliver training.
The Study
Aim
The aim of the present study was to understand patients’/service users’ perspectives about the IRIS service in general and specifically in relation to the impact of COVID-19. By “IRIS service” we refer to the process by which a patient was asked about DVA and made a disclosure leading to the referral and subsequent support from an IRIS advocate. We wanted to explore the impact of COVID-19 on experiences of DVA, access to services, changes to the referral pathway of IRIS, and the provision of specialist support, to understand what worked and what was less effective during the pandemic period. We wanted to identify barriers and facilitators to engagement for patients/service users (see previous section for a description of the referral pathway).
Study Design
This paper reports the qualitative descriptive findings only, of a mixed-method evaluation. Qualitative research provides a systematic way of exploring the subjective experiences and perspectives of people about a phenomenon of interest (Grove et al., 2012). Qualitative research helps to advance understanding about a social or human problem and can facilitate the development of a complex and holistic picture of participants’ experiences and perspectives about a particular phenomenon at a particular juncture in time and space (Creswell & Poth, 2016). The qualitative descriptive approach was considered suitable for this study as a response to the societal changes that the global pandemic has brought about.
Participants and Recruitment
A purposive snowball sampling strategy was used to ensure appropriate identification and recruitment of participants. Project staff working at the IRIS project acted as gatekeepers (Johnson, 2018) by approaching victims–survivors who met the inclusion criteria:
Received support from IRIS in the period following the first national lockdown (March 2020) No ongoing risk from violence and abuse Over age 18
Once identified, potential participants were contacted through their preferred methods (phone or email).
Data Collection
Telephone interviews were held with patients/service users (n = 11) during January and March 2021, using a semistructured format. For these participants, telephone support had also been the singular form of contact with the project. Questions were asked in a nonjudgmental and culturally sensitive manner. All discussions were recorded via notes or a digital device. Each interview lasted between 20 and 45 min.
Data Analysis
Transcripts of individual interviews were anonymized prior to reflexive thematic analysis (Braun & Clarke, 2021). NVivo 11 was used to aid data management and analysis. Interview data were initially coded line-by-line, and themes were iteratively developed following an inductive analysis.
We first read and re-read the interview transcripts to become intimately familiar with the content, noting initial impressions and potential themes. We then highlighted significant segments of text and assigning labels (codes) that captured the essence of each segment. The coding process was flexible and iterative, allowing for new codes to emerge as we worked through the data. The next step involved examining the codes to identify broader patterns of meaning. We grouped related codes together to form initial themes that reflected significant aspects of the data. This process was dynamic, with themes being refined and adjusted as we progressed. We reviewed the initial themes to ensure they accurately captured the data. This involved checking the coherence of themes and considering whether they worked both within each theme and across the entire dataset. Themes were refined by merging similar themes, breaking down complex themes, or discarding themes that did not have enough supporting data. Once the themes were finalized, we defined and named them. Finally, we compiled the findings into a coherent narrative that provided a rich, insightful account of the data. The report was structured to highlight the key themes, supported by direct quotes from participants to provide authenticity and depth.
Rigor
To generate new knowledge through thick description, we adopted an ethical and rigorous strategy for data analysis (Harley & Cornelissen, 2022). Four elements determine trustworthiness of a qualitative study: credibility; transferability; dependability; and confirmability (Denzin & Lincoln, 2011). To enhance rigor of the study, we adopted the framework offered by Harley and Cornelissen (2022) which argues for methodological coherence (ensuring consistency across epistemology, ontology, methodology, and theory); logical consistency (from data collection to analysis); contrastive reasoning (asking questions such as: Have I interrogated data thoroughly? And have I considered all explanations?); and explicating explanations (seeking the best explanation based on empirical findings rather than the likeliest explanation).
Ethical Considerations
The study was subject to the procedures required by the ethics approval process of The University of Sheffield (Approval Number 037468). An information sheet and consent form were distributed via email prior to the telephone interviews. This information detailed the aims of the study, data collection methods, reporting protocols, and information regarding withdrawal, participation, and postinterview support. Informed consent was gained from all participants, and ethics was treated as an ongoing process, enabling participants to contribute as they wished and to end interviews when they wished. Throughout the study, great care was taken to ensure the confidentiality and anonymity of participants; pseudonyms are used in this article.
Findings
Demographics of Participants
A total of 11 participants contributed to the study. The ages of participants ranged from 30 to 49 years; this is not representative of all patients/service users of the IRIS service, which supports adults age 18+ with no upper age limit. In terms of ethnicity, the sample illustrated varied backgrounds, reflecting the ethnic diversity of the city where the project was based. The background of participants is detailed in Table 1.
Demographic Characteristics of Participants.
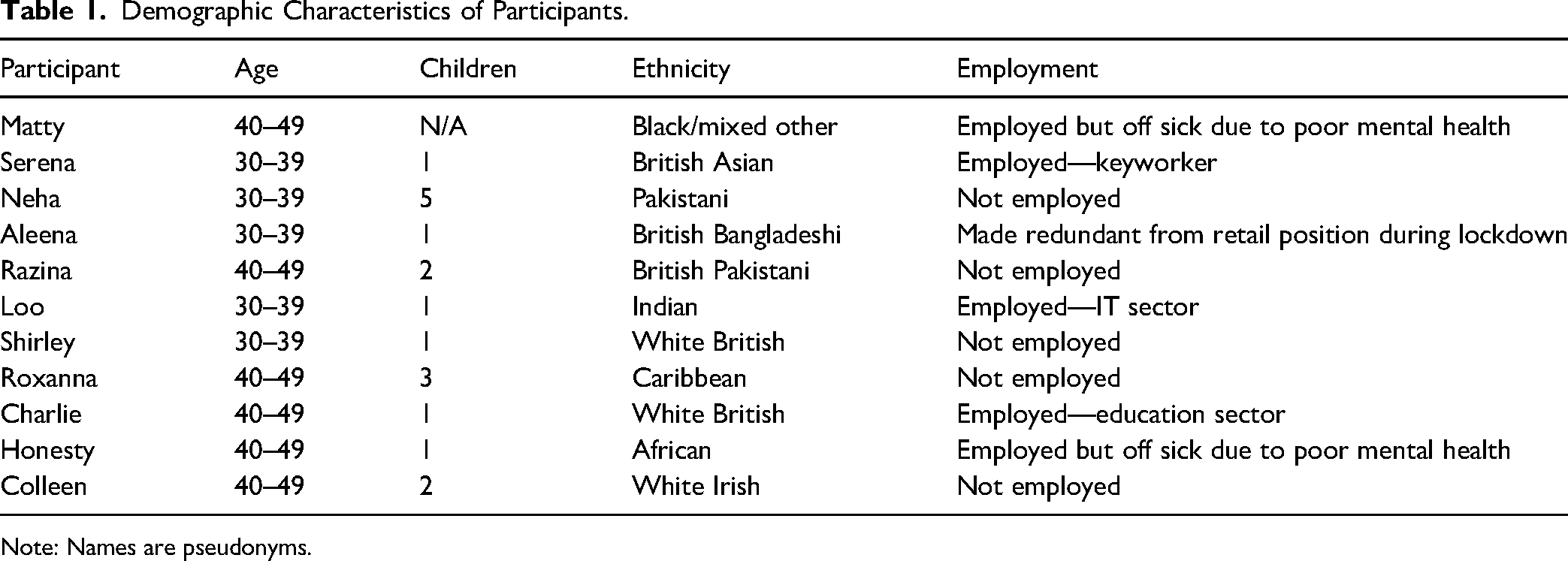
Note: Names are pseudonyms.
Themes Identified
All participants of the study reported feeling supported around DVA by the health-care professionals working in primary care and were referred to the IRIS service. In the following, we present their views categorized by the themes identified.
Experience of DVA during COVID-19 Awareness of the IRIS service Pathway to care Accessibility, safety, and remote consultations Adequacy of telephone support Impact of IRIS support
We have used pseudonyms throughout to ensure confidentiality of the participants.
Experience of DVA during COVID-19
Most participants described the social lockdown measures resulting from COVID-19 as having a negligible impact in relation to their abuse experiences, as abuse continued and did not change substantially. However, in framing how their experiences of DVA changed during COVID-19, two participants referred to social isolation. For one participant, the isolation was self-imposed as she attempted to keep herself and her daughter safe: My experiences did change during COVID-19 mainly because I did not have anywhere to go and I was locked in the house. For three months between March and July 2020, myself and my daughter spent all our time in the attic of the house. I will go to make something early in the morning before anyone else was awake in the house, cook something and come back upstairs. I felt really isolated. (Razina)
Razina was a mother of two who lived in the family home with her husband, along with his extended family. She described how she kept herself and her daughter away from other family members and describes the types of experiences she had when she was in the family space: One day, I came downstairs and washed my children's clothes. To do so I took clothes already in the washing machine out and washed my children's clothes. The clothes that I took out of the washing machine were of my brother-in-law and when he saw that he started abusing me, cursing me and calling me names in front of his mother and my 12-year-old daughter. He then started talking bad about my daughter and swearing and screaming at her and I just could not bear that. (Razina)
After this incident Razina contacted the police and managed to leave. Paradoxically, the increased isolation represented a catalyst for another participant who described this as a period for reflection that enabled her to decide that “it was a high time for me to get out of the situation and so I decided to speak about it and shared it with my GP” (Loo).
Awareness of the IRIS Service
Across the sample, there were different levels of awareness that DVA specialist services existed. None of the participants were aware of IRIS prior to the support they had received, as Aleena illustrates when responding to a question about prior knowledge of IRIS: “Never in my life. I never knew that type of service can be available…I never knew that there were refuges. I never knew that Social Services can provide help in transport.” Another participant was similarly unaware of IRIS until being offered an IRIS referral: “I was referred to IRIS by my GP… I didn’t know anything about the service before but when I told GP about my situation, and he referred me to IRIS” (Razina).
At the start of interviews, when asked about IRIS, some participants said that they did not know what IRIS was. Other responses indicated that participants had heard of Women's Aid, but not IRIS: “I’d heard of Women's Aid and various other things, like, you know, helpline numbers. But I wasn’t aware of the group IRIS at all until my GP mentioned it” (Colleen).
Overall, awareness of IRIS and specialist DVA services were poor. The participants only learned about it once their GP had mentioned this to them and suggested a referral. This happened when either the GP asked questions about DVA or the patient/service user disclosed their experiences themselves during their consultation for a health problem/symptom as explained further in the theme below. Despite the IRIS program aiming training and education at all staff in GP, including all practice nursing team members, only GPs had asked about DVA and referred participants for IRIS support.
Pathway to Care
In order to understand the referral pathway and initial contact, interviewees were asked how they came to receive support from the IRIS service. All participants were referred by their GP, as opposed to another professional at their GP surgery: “I explained my situation to my GP who then put me in touch with the social worker and the [IRIS] service and they helped me” (Loo): It was actually a visit to my GP surgery, and through a very thorough conversation about events that had happened over the years, [my GP] suggested that I talk to somebody from IRIS just to clarify certain things. Sometimes when things happen you kind of brush them off and you don’t know how to pinpoint them, or what they are, or what type of behaviour you’re having to put up with… I explained several scenarios to her, and she identified those as emotional abuse… And that's why my GP, when I was after speaking to her, she suggested that I speak to somebody from IRIS. (Matty)
One participant, Aleena, had attended her GP appointment to discuss postnatal depression and appreciated being questioned by her GP: “… [S]he asked me a question…how are things at home? And no one says that to me.” This participant benefitted from the GP's “professional curiosity” which is something that is encouraged during the delivery of IRIS training. It may also demonstrate the benefit of the remote consultation, as Aleena explained: […] I used to always tell my GP, whenever I speak to them, that my husband doesn’t believe in mental health…and I once spoke to her, and I was speaking in a coded language. So, my husband was right next to me, and I wasn’t giving her all the details. And then she decided to call later, and just say, how are things in the house? And I replied back, that no, things are actually really bad, he's very, very abusive. And she was the one who referred me to IRIS. (Aleena)
Postnatal depression is associated with DVA, and on making the appointment, this would be flagged on the computer system in the GP to prompt the health-care professional to ask the patient about DVA. Aleena's experience provided a positive indication that this aspect of the referral pathway was working well in that practice. Some participants commented on the speed from the point of referral to the first contact with IRIS: It was really quick… the contact, so I wasn’t kind of waiting around for a phone call or anything, things happened quite quickly…I don’t think it was any longer than a week… It was quite quick, and I thought, oh, that's good, someone's got back to me. (Matty)
All participants who commented on initial contact from IRIS represented the view that the time between the initial referral and contact made was short.
Accessibility, Safety, and Remote Consultations
All participants engaged in remote consultations via telephone; none had in-person contact or were offered videoconferencing meetings. This was true for consultation with the health-care professionals at the GP surgery and IRIS service. Participants shared that despite the shift to remote consultations, IRIS advocates maintained good practice in promoting safety and completing risk assessments for each victim–survivor: The person contacted me in the GP surgery and then via phone afterwards… I was experiencing abuse for more than 13 years and by this time I was ready to explain my situation to anyone. They always asked me if it was safe to talk and if my children were around or not so we could talk privately. (Roxanna)
Participants reported few barriers in accessing support via remote consultation. Some had already escaped from abuse and were living separately. They framed this as meaning that there were no or low risks for themselves and their children. This is counter to what is known about DVA: that often risk escalates immediately after a woman leaves an abuser (Katz et al., 2020). One participant described the main barrier for her was that on arriving in the country she did not know “any of these services and how to access them.” On being asked if meeting in-person in a safe, socially distanced way would that have made a difference to the support that she received, Matty replied that she was happy with remote consultations, but she recognized that for victims–survivors in more controlling environments, accessing telephone support could be more problematic: For me it was enough. He wasn’t controlling in terms of me going out or anything, so I knew that because I’d got family that live near to me, that I could just get in my car and drive off somewhere. But there may be other situations where people didn’t have that freedom. (Matty)
Participants recognized the different barriers posed by the pandemic and lockdown measures: … [I]f there was a place where you could go to for support, in the lockdown, even that would have been hard to do, to access … but, like I said, if it's lockdown and it's not open, or there's nobody there, you’re just better knowing that there's a number that you can reach out to somebody. (Charlie)
Serena illustrates some of the barriers to accessing support remotely in relation to a very specific context, during legal proceedings, but one that is pertinent to many victims–survivors with children. When COVID hit, you can’t have your caseworker on the telephone, a telephone conference type of thing, and that's where I felt, oh my gosh…And then you can’t go and see your caseworker and it's very difficult…You don’t want to be sending legal documents via email, type of thing. (Serena)
Adequacy of Telephone Support
Most participants felt that support offered remotely via telephone was sufficient and met their needs: I had a number that I could access if I needed it. … [A]s long as you know that there's a number there, a contact that you can reach out to somebody, then that's the main thing. Because lockdown, we’re all at home, and obviously everyone's in, and you need that reassurance that you can pick the phone up. And she did (the IRIS advocate) … it's that layer of support and confidence that somebody will be there to listen. (Matty)
In contrast, another participant responded “no” to the question of sufficiency of telephone support but found it difficult to articulate what could have been more helpful. Another participant described disjointed telephone contact and the effect this had: Then all of a sudden, [IRIS advocate] disappeared because the phone broken or something. It was all a bit of a mess and I just felt like I was being a burden…It was just, yeah, I don’t know, I just felt so uncomfortable but that's probably due to lockdown. (Neha)
Neha did admit to the whole incident being confusing and she was unsure whether she had understood aspects communicated to her. She did also appreciate the help that she had received (e.g., access a food bank), but described this as “inconsistent.” When asked if a face-to-face meeting in a safe, socially distanced space at the GP surgery would have been preferred to telephone, Neha replied “Yes, definitely,” but that “it was just not offered at all.” Neha also indicated that she would have preferred to have used videoconferencing (e.g., Skype or FaceTime) to the telephone support that she received. Serena described some dissatisfaction with the ending of her support which she felt was due to one staff member leaving and the project wanting to close cases, noting, “I feel that I still need that ongoing support because I’m still going through a lot of legal proceedings.”
Aleena felt that short-term telephone support was adequate when she needed it (when she had decided to leave) but highlighted a problem when services do not operate the usual 9a.m. to 5p.m. office hours. Arrangements that the IRIS advocate had made on behalf of Aleena did not go to plan as a prebooked taxi that was tasked with taking Aleena and her child to the train station on the night she was leaving failed to arrive: I told [IRIS advocate] to organise a taxi at 5.30, so that I can leave before he comes home from his night shift. But the taxi never turned up that night… At that moment, yes, I was very angry, I was like, what's happening, I was meant to leave, but, you know, the cab's not coming, the 24-hour helpline, no one's answering. (Aleena)
Another participant reflected on how to manage telephone support. In this quote, Colleen reflects on the safety for women who might be subject to surveillance by abusers, offering a creative and practice solution: Looking through your phone, like, instead of putting women's helpline, or Women's Aid, that starts ringing alarm bells then if you’ve got a partner that goes to your phone, they’d be thinking, oh, she's in touch with somebody. But if you went through and saw Iris, or whatever… So, IRIS is actually quite a good name, because you can store it in your phone as a person…. So, I did. I stored it in my phone as Iris, and it just comes up, you’d just think it was a lady's name. (Colleen)
Impact of IRIS Support
Most participants described the support that they received as wholly beneficial. Mostly this was emotional support; a small number additionally benefit from advice and information. Quite often support was after separation or at the point at which women decided to leave the abusive relationship. Matty had support over four telephone conversations at the point at which her relationship ended, and, while the IRIS support was brief, she found it helpful in validating her experiences of abuse: An [IRIS advocate] actually just confirmed, because I was asking the question “Has it been abuse?’ What is it, like what is it when somebody plays with your mind so much that you just you get to that point where you think, I can’t, like, this is awful, I can’t keep hearing those words, I can’t…you know, the comments, the criticism, you know, it's not right? And I suppose now I know that if something doesn’t sound right or feel right, or you’ve got to question it, then it's not right, it can’t be. (Matty)
Serena described how during court proceedings around child contact, her ex-partner was making threats of suicide, and the support she got from her allocated IRIS AE enabled her to make sense of his behavior: With this threat of suicide and things like that, I thought, oh my goodness, what's he playing at? What's he trying to do, take me back to the relationship of a year and a half ago? Is he still not moving on? … And again, is it that narcissistic traits and behaviours? I even…because I really wanted to know the science of why someone behaves or has these traits… And with IRIS, they really helped me to understand that this is how perpetrators behave and (by leaving) you’ve taken the power away from them. (Serena)
Several participants benefitted from practical support from IRIS when they left their abusive relationship. Aleena said: I never knew that I could have that much support. I only had £250 on me, and I made the decision to move back to London in a refuge. I didn’t want to bother my family, because it's just, they will get blamed for everything, if, you know, I move into them…So I moved into a refuge. And they organised everything for me.…I wanted something to be self-contained…you know, with a young child…So [IRIS advocate] organised all of that for me.…she was amazing. (Aleena)
Another participant, Honesty, had arrived in the UK just prior to the first lockdown and described practical intervention in getting help to secure housing and helping to arrange utilities. She saw this as helpful in her attempts to settle with her children in a new country where she had no existing support network. In addition to emotional and practical support, a number of participants referenced the value of information and advice around legal proceedings: And my caseworker…really helped me to understand about the child proceeding, the procedures, when I don’t understand things, and really helped. And one of the things she said to me is, when it comes to your trial, I’ll be able to offer you that support. I’ll be able to come in court, hopefully. Because we all thought, oh yeah, in six months’ time, everything will be back to normal…. (Serena)
Discussion
Despite diverse literature that describes the impact of COVID-19 on DVA, participants in this study did not report significant changes in their experience of abuse as a result of any life changes caused by the pandemic or public health measures resulting from it. Of the minority who did report an impact, it was in relation to increased social isolation and had differing consequences for two women: while it did affect the type of abuse experienced by one woman, for another it served as a catalyst to leave the abusive relationship. In the same way, the depictions of DVA were not that different from experiences prior to the pandemic, nor were the support needs described as being radically impacted.
The most impactful change resulting from the pandemic was the shift from in-person support to remote consultations and telephone support as the primary intervention offered by health-care professionals at GP surgeries as well as via the IRIS team. The shift to remote consultations, along with advice and guidelines across health-care and other sectors, was fast and resulted in unintended or unforeseen problems (Rimmer, 2020). A rapid review of evidence around mental health support found a plethora of challenges described including access to technology and technology failure (e.g., interconnections suddenly lost); background distractions and disturbances; ethical issues around confidentiality and privacy and practitioners’ limited technical knowledge thereof; barriers to reading nonverbal communication; increased chance of miscommunication; practitioners feeling “helpless” when unable to further support or take action to protect patients/service users; and managing boundaries (James, 2020). The problem of miscommunication appeared to be an issue for two of the IRIS service users. However, these issues are often written about from the perspective of health-care professionals and not necessarily from the perspective of those receiving care. James’ review provided important and useful insight from the perspective of patients/service users, especially with regard to effectiveness of interventions. It did also find that while existing studies were not rigorous, there were some promising findings that remote intervention was accessible, flexible, and well-received by individuals needing support (James, 2020).
From the perspective of patients/service users, what worked well in the remote delivery of the referral pathway from GP to support from the IRIS team was a responsive service with minimal waiting time following a disclosure of DVA to their GP and the subsequent referral for specialist support. Participants spoke enthusiastically about IRIS intervention, with clear appreciation for the amount of emotional and practical support as well as legal, housing, and justice information and advice from IRIS advocates. Despite the problems associated with remote interventions identified by James (2020), in our study, patients/service users did not describe many communication barriers and, instead, articulated the ways in which support from IRIS advocates enabled them to recognize their experiences as abuse when they previously had not recognized nor named particular behaviors (mostly, nonphysical violence) as abuse. Importantly, this validated their experiences, and patients/service users described this as empowering. The recognition and acceptance of experiences as abuse had begun during remote consultations and discussions with health-care professionals (in all cases here, this was with GPs), positioning this first exchange as critical in triggering disclosure and the process of validation.
It is difficult to ignore the contextual circumstances of this initiative in terms of the impact of the pandemic, national lockdown measures, and the move to remote interventions. It is also important to frame the feedback from women within the context of their lack of knowledge about specialist DVA support. That most of the participants had no or little prior knowledge of IRIS was important in that none had expectations of the type of support they could access. Therefore, it is no surprise that the women found their journey to and through IRIS as empowering, as it enabled them to understand their experiences as abuse and enabled them to benefit from professional support and advice. Again, this serves to reinforce the critical importance of practitioners in primary and secondary health services (including GPs, nurses, health visitors, emergency and ambulance staff, midwives, and sexual health practitioners) as often the first point of contact for people experiencing DVA (Centre for Social Justice, 2022). Moreover, it supports those claims that victims–survivors of DVA frequently identify health-care practitioners as the most trusted professionals whom they would be most likely to speak to about their experiences (SafeLives, n.d.).
All participants had been referred to IRIS by their GP rather than other health-care professionals in the GP. As a GP-based program, IRIS seeks to train and support all health-care professionals in a surgery as well as other key personnel who have contact with patients such as nurses, midwives, receptionists, and other administrative workers. Despite the role of health-care professionals as gatekeepers or facilitators in this respect, this whole-system approach is yet to be fully successful (Al-Natour et al., 2016). That primarily GPs refer through IRIS, as opposed to other health-care practice-based workers, is reflected in other literature which shows that health-care professionals other than GPs based at GP do not frequently respond to and ask about DVA (Al-Natour et al., 2016). Indeed, scholarship suggests that health-care professionals are often reluctant to ask about DVA for myriad reasons including a lack of confidence, not wanting to cause offense to the patient, lack of time, and not knowing where to refer people once they have disclosed DVA (Al-Natour et al., 2016). Notwithstanding the limited adoption of IRIS training and principles (i.e., the need for health-care professionals other than GPs, such as nurses and midwives) to ask about DVA, this study has shown that IRIS offers an important pathway to support for victims–survivors.
Talking through their experiences with GPs and then with IRIS advocates also enabled some women to gain greater insights about the strategies that abusers adopt and the impacts of DVA on their children. Having this better understanding of the complexity and dynamics of DVA was clearly valued by women and had a lasting impact. For example, two participants spoke about their desire to volunteer to work with other DVA victims–survivors once they were further along in their recovery. This desire was expressed in appreciation of the support they had received, and both framed their intentions in relation to their desire to enable more victims–survivors to recognize their experiences as abuse and, consequently, access help to escape. This desire provided a counter to the finding that there was little awareness of IRIS and other DVA specialist support among participants prior to their discussion with the GP and subsequent referral. Put simply, these women described their interaction with IRIS as being empowering, and they strongly articulated their desire to have the opportunity to empower other women in similar ways.
While two participants described dissatisfaction with aspects of remote intervention, it is also important to contextualize their experience and to locate it within a challenging time for health- and social-care providers. The confused arrangements occurred when everyday service delivery had been severely disrupted by COVID-19 for both IRIS and primary health care. Another study of DVA support during COVID-19 similarly found potential for digital intervention but also “missed opportunities” for engagement (Alderson et al., 2022). This raises questions for future remote delivery of DVA support via digital means such as video conferencing (rather than telephone alone), apps, social networking sites, and other uses of technology. Digital methods have seen a surge in other areas of support such as the field of mental health care. Indeed, the use of digital technology has the potential to empower victims–survivors to engage more proactively in technology-facilitated resistance (the use of technology and digital methods to end abuse or seek redress in relation to their experiences, e.g., using technology to record incidents of abuse to use as evidence; Rogers et al., 2022). Remote interventions also have the potential to negate some of the negative effects associated with being a victim of DVA, such as shame, embarrassment, and fear (James, 2020). Future research should explore the potential for a combination of remote and in-person intervention.
Limitations
One methodological limitation of the evaluation is the sample size and single site location. This is a common feature of locally commissioned evaluations, but such projects can still yield rich data with important implications for policy and practice. A more practical limitation related to interviewees’ knowledge about IRIS, in that they were not asked how long they had been patients registered with their GP practices: this may have been the first time that they had been registered in a location that commissioned IRIS. However, it is prudent to consider that there is work to do to raise awareness of IRIS and DVA more generally.
Implications
Health-care professionals, especially those working in primary care including GPs, nurses, and midwives, can play an important role in identifying and supporting those experiencing DVA, as people use primary care services and especially GP surgery for various health-care problems for themselves and others (such as children). This is a place where the requirements of providing safe and effective care within a private environment cannot be denied, and therefore it provides health-care professionals a legitimate excuse to speak to the patient/service user individually in a private environment, making it possible for them to ask DVA-related questions.
The findings of the study highlight the importance of health-care professionals other than GPs becoming confident and competent in exploring DVA during remote consultations while ensuring confidentiality and safety of the patient/service user, as well as the need to explore further why the referrals only came from GPs and not from nurses, midwives, and other professionals working in GPs (see Table 2 for guidelines for remote consultations). It may also be useful to explore existing pathways and protocols as implemented in various GP settings to explore what affects confidence, competence, and the ability of health-care professionals other than GPs in supporting those experiencing DVA and what can be done about it. The closure of GP surgeries in order to deal with the demands of the pandemic and more recently the rollout of the vaccination program have resulted in additional local demands. However, there are still some clear messages for reflection in relation to support offered to those experiencing DVA; these include developing ways to communicating with patients/service users via video conferencing rather than telephone alone; engaging patients/service users in the decision-making and referral process to ensure they feel empowered and engaged to make decisions and are able to refer themselves in future when needed; and, finally, ensuring that the needs of children and young people are met.
Guidelines for Remote Consultations.
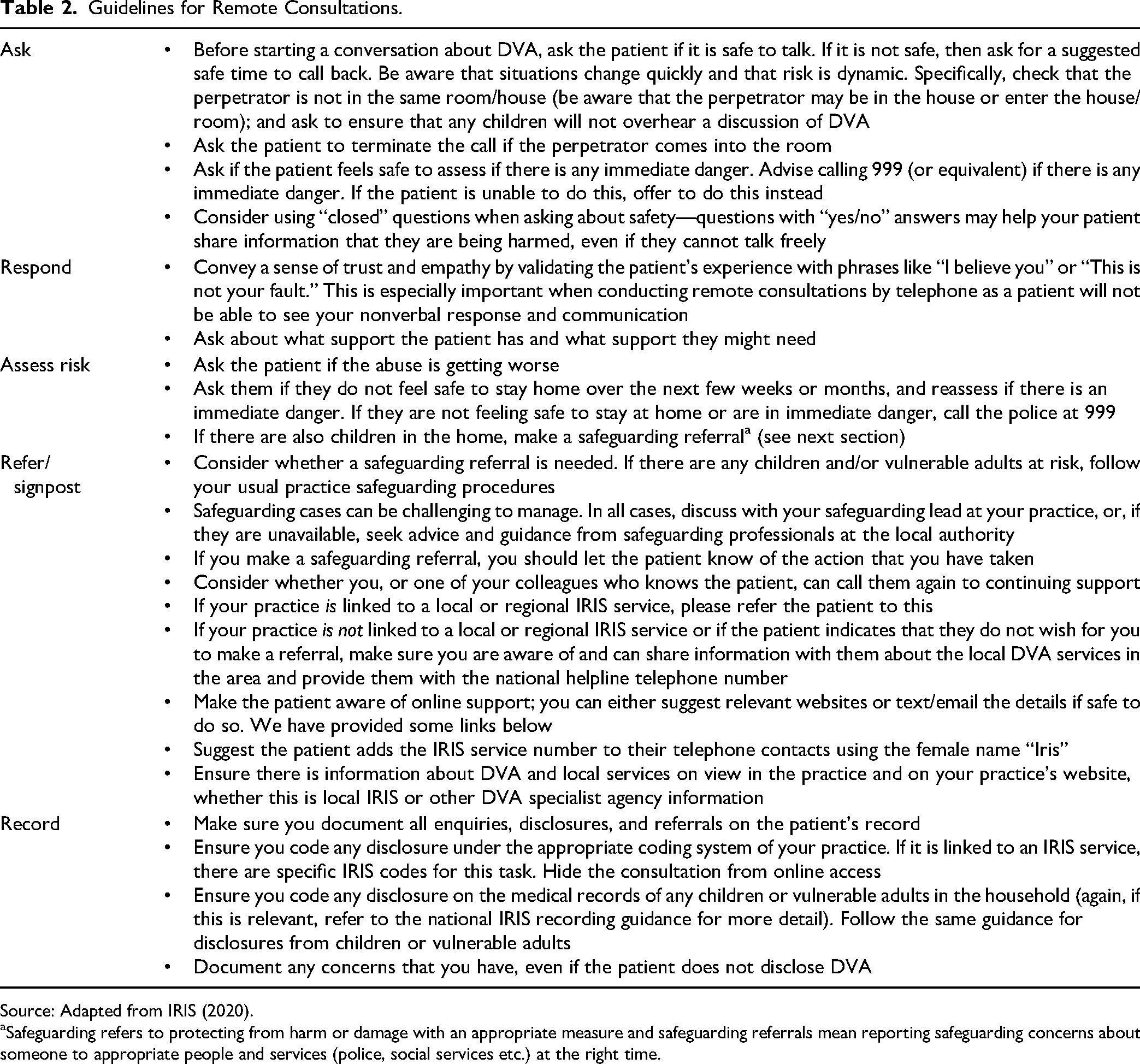
Source: Adapted from IRIS (2020).
Safeguarding refers to protecting from harm or damage with an appropriate measure and safeguarding referrals mean reporting safeguarding concerns about someone to appropriate people and services (police, social services etc.) at the right time.
Conclusion
This study provided important insight about changes to practice during the global pandemic, the most significant being the shift to remote consultations. Participants offered positive feedback on the role of health-care professionals in facilitating access to specialist support for victims–survivors of DVA during the COVID-19 pandemic using remote consultation as the primary intervention. In addition, it was clear that for many victims–survivors, dialogue with their GPs had led to a recognition of their experiences as abuse which, in turn, was validating. While the IRIS services train and encourage all employees in a GP to identify and ask about DVA, participants described having such conversations with their GP only, raising a question about whether other members of the GP did routinely ask patients about DVA and subsequently make referrals. All conversations with GPs and IRIS advocates were via remote consultation, through telephone calls, and, overall, this mode of intervention was reported in a positive light. This was a small-scale evaluation, however, and further research is warranted to explore the utility of remote consultation as a means of supporting victims–survivors of DVA as a singular approach or in conjunction with in-person support.
Footnotes
Acknowledgments
The authors would like to thank everyone who has contributed to this research.
Disclosure
The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Biographies