
Abstract
Nurses are at the forefront of providing health education for the general public and are leaders in developing health education programs for all ages. Research has shown that the pediatric population often experience anxiety surrounding common medical procedures. However, evidence-based health education has been shown to enhance self-management, increase knowledge, and decrease anxiety in the pediatric population. One such successful evidence-based health education approach designed for the pediatric population is the Teddy Bear Clinic. The purpose of this article is to report on the efficacy of a nursing student-led Teddy Bear Clinic designed to increase the awareness of common medical equipment and procedures in the pre-school pediatric population. This quality improvement project used a program evaluation design to assess the children's knowledge of common medical procedures and equipment. Participants were a convenience sample of 16 children aged 3–5 years old, attending one daycare center in a large city in Atlantic Canada. Findings showed that after participation in the clinic, the pre-schoolers reported a high level of knowledge of common medical equipment and procedures. This project shows that a Teddy Bear Clinic run by senior nursing students can promote community partnerships and enhance health knowledge in pre-school children.
Implications for Research and Practice
Undergraduate nursing students can and should be involved in the research process with nursing faculty members. Undergraduate nursing students can work effectively with community partners to empower and promote health promotion in the community. Nursing students gain experience caring for pediatric clients while implementing the Teddy Bear Clinic which also leads to increased interest in pediatric nursing. At the beginning and end of each station, the “How is Teddy Feeling” coping scale was used to assess the child's perception of their Teddy Bear's feelings, which was an indirect measurement of the child's feelings.
The pediatric population often experience anxiety surrounding common medical procedures (Alexander-Ruff et al., 2024). However, evidence-based health education has been shown to enhance self-management, increase knowledge, and decrease anxiety in the pediatric population (Burns-Nader et al., 2011; Leonhardt et al., 2013; Lerwick, 2016; Nheu et al., 2018; Ni et al., 2016). Teddy Bear Clinics are one example of an evidence-based health education program for the pediatric population that has been shown to reduce anxiety while increasing knowledge and self-management skills and helping them manage their own health (Dalley et al., 2017; Dalley & McMurtry, 2016; Ni et al., 2016; Santen & Feldman, 1994; Zimmermann, 1997).
Teddy Bear Clinics are fun ways to engage families, communities, and the pediatric population in health education. Children bring their teddy bear or other toy to a make-believe “health check-up” or clinic with a health-care professional, and the child pretends to be the teddy bear's primary caregiver. The clinics often include a tour through several different stations that provide opportunities for the children to participate in health education on various topics such as postoperative care and medical procedures (Dalley et al., 2017; Dalley & McMurtry, 2016; Ni et al., 2016; Santen & Feldman, 1994; Zimmermann, 1997). The purpose of the Teddy Bear Clinic designed for this project was to teach about common medical equipment and procedures through developmentally appropriate strategies for the pre-school-aged child.
Evidence-based health education can empower pediatric patients to develop skills in self-management and provide them with the knowledge they need to make informed decisions; an empowerment-based approach to health education can increase the leaner's autonomy and their ability to think critically in making informed decisions about their health (Anderson & Funnell, 2010). Empowerment-based approaches in health education can be considered as both a process and an outcome. The process occurs when the health education is implemented with strategies to increase the child's ability to think critically and make informed decisions. The outcome occurs when the child makes an informed decision. This project used an empowerment-based approach to enhance understanding of common medical procedures and help children make informed decisions about participating in clinics.
Providing targeted health education designed for the developmental stage of the child can also help empower patients and families to better adapt to their health needs (Kaul et al., 2023). This project was designed for the pre-school-aged child who is in Piaget's preoperational stage of development which includes egocentric thinking and magical thinking (Piaget, 1964). Asokan et al. (2014) conducted a descriptive cross-sectional study with 200 children aged four to seven to assess the prevalence of Piaget's stage of preoperational development. Asokan and colleagues assessed children's egocentrism and their understanding of the concept of cardinal numbers with experiments and interviews and concluded that these features of the preoperational stage as described by Piaget are still valid today. This would indicate that the egocentric child focuses on their own opinion; therefore, they need health education to help them develop their own informed decisions.
Health education programs such as Teddy Bear Clinics can empower pediatric patients through enhancing knowledge and decreasing anxiety. Modabber et al. (2022) used a qualitative approach to conduct interviews to explore a purposive sample of 12 children's perceptions of their dental experiences and their comfort with a health education program designed to address fear and anxiety. Findings showed participants wanted to be actively engaged in their care and valued health education to reduce their anxiety. One of the themes from this study was “empowering the person”; the authors state that empowerment meant the participants had the resources needed to fully manage their dental procedures (Modabber et al., 2022).
Methods
Project Design
The project used a program evaluation design to assess the participants’ knowledge of common medical procedures and equipment after participation in the Teddy Bear Clinic. Participants were a convenience sample of 16 pre-school-aged children at one daycare center in a large city. The project was implemented over 4 hours on one morning at the daycare center.
Ethics Review
The Health Research Ethics Authority (HREA) of Newfoundland and Labrador determined that full approval of the study was not required because it was considered a program evaluation and no research questions were involved (HREA, 2023). The participation in the Teddy Bear Clinic was voluntary and an information pamphlet was developed for parents to discuss with their children to outline to contents of the clinic. The parents and children were informed that there were no consequences for not participating and no identifying information was collected.
The Teddy Bear Clinic
The Teddy Bear Clinic implemented in this project was an educational activity designed to enhance the pre-school child's understanding of the common medical procedures and equipment they could be exposed to during clinic visits, hospital visits, and check-ups with health-care providers. It was designed to maximize the teaching and learning needs of children who are in Piaget's preoperational stage of development, as well as incorporating appropriate teaching strategies for those in this stage of development. During the preoperational stage, children like to engage in pretending and role-playing. They like to play the role of “mommy” or “daddy,” and they understand symbols and use an object to represent something else (Edelman & Kudzma, 2022).
Teaching strategies that are appropriate for the preoperational stage of development include dramatic play, imaginative activities, and studying cardinal numbers (Asokan et al., 2014). Using their toys to express themselves is very common for pre-school children, who learn through role play and make-believe experiences. The Teddy Bear Clinic in this project implemented developmentally appropriate teaching strategies including role play, make believe, demonstration, and examining the world using sensory experiences. These concepts came together within the Teddy Bear Clinic, as the children brought their Teddy Bears to nursing students for a “check-up” and can explore the medical equipment and procedures within their developmental age.
Teddy Bear Clinic Content
The Teddy Bear Clinic was divided into seven different stations: (1) admission, (2) heart rate and temperature, (3) respiratory rate and blood pressure, (4) ear exam, (5) vaccinations, (6) bandaging, and (7) discharge. Each station was labeled using an animal (e.g. tiger) whose corresponding stamp was marked on the chart as each station was completed. At the beginning and end of each station, the “How is Teddy Feeling” coping scale, a 4-point Likert scale, was used to assess the child's perception of their Teddy Bear's feelings, which was also an indirect measurement of the child's feelings. If the scale indicated the child was feeling anxious, coping strategies were employed (e.g. jokes, stickers). The student nurses were guided by the teaching plans developed for each station. An example of the Ear Exam Station teaching plan is presented in Table 1.
Ear Exam Station Teaching Plan
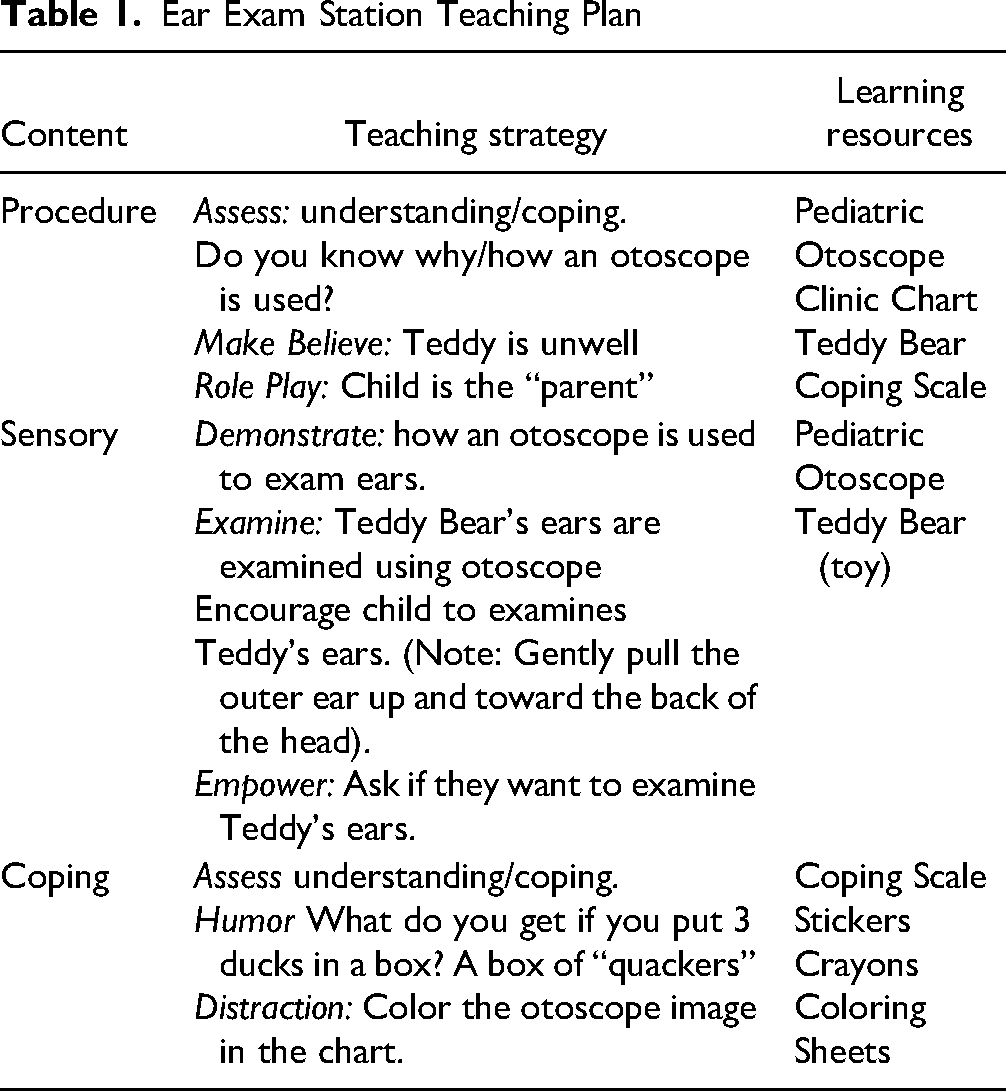
During the Admission Station, the child was asked their name and age, their Teddy Bear's name, and the reason behind the visit to the Clinic. The Teddy Bear was given a hospital-style bracelet, and the child was given Teddy's chart. At the Heart Rate and Temperature Station, the child's understanding of why and how a thermometer and stethoscope are used was assessed and then demonstrated on the Teddy. During the Lung Sounds and Blood Pressure Station, the child's understanding of why and how a stethoscope and blood pressure cuff are used was assessed and then demonstrated on the Teddy. At the Ear Exam Station, the child's understanding of why and how an otoscope is used was assessed and then the procedure was demonstrated on the Teddy. During the Vaccinations the child's understanding of why and how a needle and syringe is used was assessed and then the procedure was demonstrated using a needleless syringe, including how an immunization is drawn up, how the Teddy Bear will be prepared prior to the vaccine (e.g. positioned, site cleaned with an alcohol swab), and where the Teddy Bear will get their vaccine (e.g. in their arm). The child was then allowed to demonstrate the procedure on their Teddy Bear, using the needleless syringe.
At the Bandaging Station, the child's understanding of why and how a bandage is used was assessed and the procedure was demonstrated on the Teddy, including applying a “Band-Aid” as well as a spiral arm and leg bandage. At the Discharge Station, the child's understanding of common medical equipment and procedures as assessed using the Matching Game. The child was given their Clinic chart, a certificate of Clinic completion, a donated crocheted Teddy Bear, and a “loot” bag containing crayons, markers, stickers, coloring sheets, a needleless syringe, and pediatric Band-Aids. The chart was also reviewed to ensure all stations were completed and the Matching Game was retained for analysis.
Matching Game
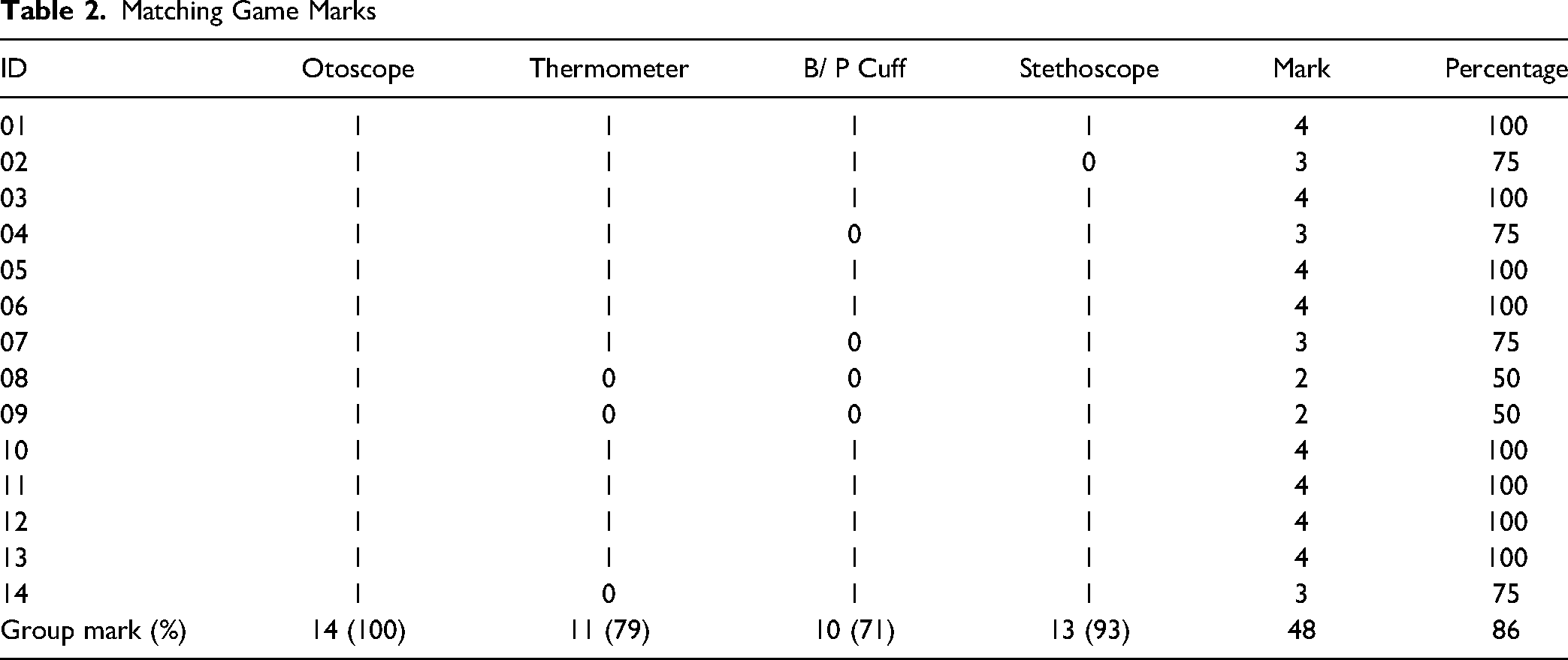
The Matching Game was played at the last station of the Clinic, the Discharge Station. This game was designed by the authors specifically for this project, to measure the children's understanding of the medical equipment and procedures using a stethoscope, thermometer, otoscope, and blood pressure cuff. The child was asked to draw a line to the place on the body of a picture of a teddy bear, where the medical equipment was placed during the procedures, and received one point for each of the four procedures if they identified the correct place. Of the 16 participants, 14 fully completed the “How is Teddy Feeling” scale and the matching game.
Results
The results of the Matching Game are presented in Table 2. Findings showed that all of the children (100%) knew that the otoscope was placed in the ear, and almost all (93%) knew that the stethoscope was placed on the chest. Three of the children (21%) did not know where the thermometer was placed, and four (29%) did not know where the blood pressure cuff was placed. The overall group mean on the Matching Game was 48/56 or 86%.
Matching Game Marks
Discussion
The findings of this project showed the participants had an excellent awareness and knowledge of common medical equipment and procedures after participation in the Clinic. These findings support the design, implementation, and evaluation of a Teddy Bear Clinic for this population. Findings also support using empowerment-based health education strategies for pre-school children.
The low group mean for the position of the blood pressure cuff (71%) may be related to confusion with using the stethoscope for both blood pressure and heart auscultation. It could also be related to not being able to distinguish where to place the cuff because the arm on the picture of the teddy bear used in the Matching Game was short and connected too close to the body. The low group mean for the axilla thermometer may be related to confusion between the use of the thermometer for oral and axilla because two of those participants drew a line to the mouth versus the axilla. This could also be related to the way the child is used to having their temperature checked at home. This indicates the need to revise the matching game to better accommodate the pre-school-aged child's previous understanding of these procedures.
These findings indicate the need to enhance the visual resources used at each station in the Clinic to demonstrate the procedures. Each station could have a standardized teddy bear model that could be used at each station to show the correct position of the equipment. Recommendations arising from these findings indicate the need to use a valid and reliable tool to measure pre- and post-test knowledge; a larger sample size is also needed to increase the chance that the findings are representative of this population. Feedback from the Clinic staff included “the children were excited when they left the Clinic and were overheard telling others about how much fun it was.”
Lessons Learned
The Teddy Bear Clinic used in this project provided nursing students with hands-on experience with the pediatric population, which is important since currently nursing schools are challenged in obtaining clinical hours in pediatric settings. Nursing students and their faculty can plan and implement a Teddy Bear Clinic to enhance their pediatric clinical experience. The second lesson is that collaborating with an organization such as daycare centers can create valuable opportunities for learning for the pediatric population and nursing students.
Limitations
The post-test only project design does not have a comparable pre-clinic score; therefore, we cannot conclude that the Clinic was the sole cause of the high level of knowledge and awareness of common medical equipment and procedures. This was also a small convenience sample of children in one daycare and cannot be considered representative of the population as a whole. The results cannot be generalized to the greater population of pre-school-aged children. Finally, the Matching Game tool did not have validity and reliability established. Therefore, the findings of this project can only apply to this small group of children and cannot be generalized to a larger population.
Conclusion
This project showed that an empowerment-based Teddy Bear Clinic run by senior nursing students can promote community partnerships and enhance health knowledge of pre-school-aged children. These findings support other research that had shown the health promotion benefits of participation in a Teddy Bear Clinic for pre-school children. It recommended that this project could serve as a guide to implement annual Teddy Bear Clinics during the pediatric clinical courses in any undergraduate nursing education programs in Canada.
Footnotes
Acknowledgements
The authors would like to acknowledge the funding received from the Memorial University of Newfoundland, Quick Start Public Engagement Funds.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Memorial University Quickstart Program.