
Abstract
Implications for practice and research
Acculturation is the process of adapting to a new culture while balancing the realities of what was known and what is current. The aim of this review is to provide clarity on the mental health effects of acculturation in adolescent and adult children of immigrants by focusing on internalized symptoms such as depression, anxiety, perceived acculturative stress, and somatic symptoms. Conflict emerges as individuals face distinct value systems with accompanying expectations and are forced to make difficult choices; acknowledging cross-cultural conflict allows for individual differences in perception, responses, and mental health outcomes associated with cultural marginality. Studies comparing acculturative stress in places with structures to help with acclimation to the host culture to locations with few members of minority groups and limited support can help build systematic processes to assist acculturating immigrant groups.
Children living with at least one foreign-born parent represent one of the fastest-growing segments of the U.S. population and are projected to represent up to one-third of the child population by 2050 (Georgiades et al., 2018; Kim, Nicodimos et al., 2018; Kim, Schwartz et al., 2018). Second-generation immigrants are the first in their families to be born in the United States, yet the dominant culture that is practiced and acknowledged in their home is their parent's culture of origin. These children of immigrants are caught between parents representing the influence of their country of origin, and school and peers representing the ways of the host society (Montazer & Wheaton, 2011). Living between two cultures can be difficult when the ideals of each do not coincide, adding strain and stress on mental health to that of typical developmental occurrences (Sirin et al., 2019). For example, emerging into adulthood can be characterized by moving away from home to attend school, financial independence, exploring career options, and forming lifelong relationships, but second-generation immigrants have to balance these mainstream expectations with their family's cultural traditions and expectations (Obradovic et al., 2013).
The literature offers two perspectives when evaluating immigrant mental health (Kim, Nicodimos et al., 2018). One perspective is that of acculturative stress. Acculturation is the process of adapting to a new culture while balancing the realities of what was known and what is current (Berry, 1997; Sirin, Gupta et al., 2013; Sirin, Ryce et al., 2013). The stress that comes from this process is termed acculturative stress. Through this focus, children of immigrants have higher rates of mental health issues than their non-immigrant peers (Kim, Nicodimos et al., 2018; Sirin et al., 2019). This framework suggests that first-generation immigrants would have the worst mental health symptoms, decreasing with each generation as the divide between native and host cultures lessens.
The second perspective is the healthy immigrant paradox also known as the healthy immigrant effect. This phenomenon posits that immigrant groups, whether adult or child, have better health outcomes than non-immigrant peers (Bowe, 2017; Kim, Nicodimos et al., 2018; Obradovic et al., 2013). This phenomenon suggests that first-generation immigrants would have better mental health, with worsening mental symptoms as the generations progress. This effect is seen in both externalized symptoms (aggression, behavioral issues) and internalized symptoms (depression, anxiety, somatic symptoms).
The perspectives of acculturative stress and the healthy immigrant effect contrast in the mental health outcomes of the immigrant population and the generations that follow. These contrasting viewpoints may explain the variability in current research findings, as the findings about the mental health of children of immigrants are mixed and evolving (Montazer & Wheaton, 2011, p. 25). The dearth of studies and the variability in study findings make it difficult to draw firm conclusions about the mental health status of children of immigrants (Kim, Nicodimos et al., 2018, p. 168).
Review Methods
Aim of Review
The aim of this scoping review is to provide clarity on the mental health effects of acculturation in adolescent and adult children of immigrants by focusing on internalized symptoms such as depression, anxiety, perceived acculturative stress, and somatic symptoms. Current literature was reviewed to draw conclusions about the experiences pertaining to the expression of anxiety and acculturative stress among children of immigrant parents. This study is part of a larger project that aims to evaluate the mental health effects of acculturation in second-generation immigrants.
Design
A scoping review was conducted to obtain an overview of the available literature in order to answer the research question. Scoping reviews are conducted to identify and map the available evidence about a concept in order to clarify key concepts and definitions in the literature, and to identify key characteristics. (Munn et al., 2018). Arksey and O’Malley's methodology (2005) used for this review has five stages: (1) identifying the research question, (2) identifying relevant studies, (3) selecting studies, (4) charting the data, and (5) collating, summarizing, and reporting the results (Arksey & O’Malley, 2005). See Supplemental File 1 for PRISMA Flow Diagram.
For mental health: “internalizing symptoms” OR “anxiety” OR “stress” OR “acculturative stress” OR “mental health” OR “depression” OR “acculturation.” For population: “second-generation immigrants” OR “second-generation” OR “children of immigrants” OR “children with immigrant parents” OR “middle school age children” OR “high school age students” OR “adolescents/adolescence” OR “teenagers” OR “emerging adults” OR “college-age students” OR “young adults” OR “children” OR “children of first generation.”
Keywords present in the title, abstract, or as subject terms. Studies from 2010 to 2020, peer reviewed, and published in English. Studies conducted in the United States and focused on acculturation in the United States or list American culture as the host culture. This is the host country of interest due to migration of various immigrant groups into the United States. Studies that focused solely on the migration process were excluded. Original study or secondary review of data. Population sample must include offspring of immigrants aged 13–28 years. Children of immigrants are defined as having at least one foreign-born parent and/or being the child of a first-generation immigrant. Conceptually measured or evaluated how acculturative stress, cultural stress, or generation status affected internalized symptoms. Study could focus on one or all of the internal symptoms. Study must focus on the acculturative process as a whole, not solely on one aspect of acculturation (e.g., language, academics, socioeconomic standing). These aspects can be measured along with acculturation, but cannot be the sole measure of acculturation.
Figure 1 presents the screening process for articles against the inclusion criteria and keywords.
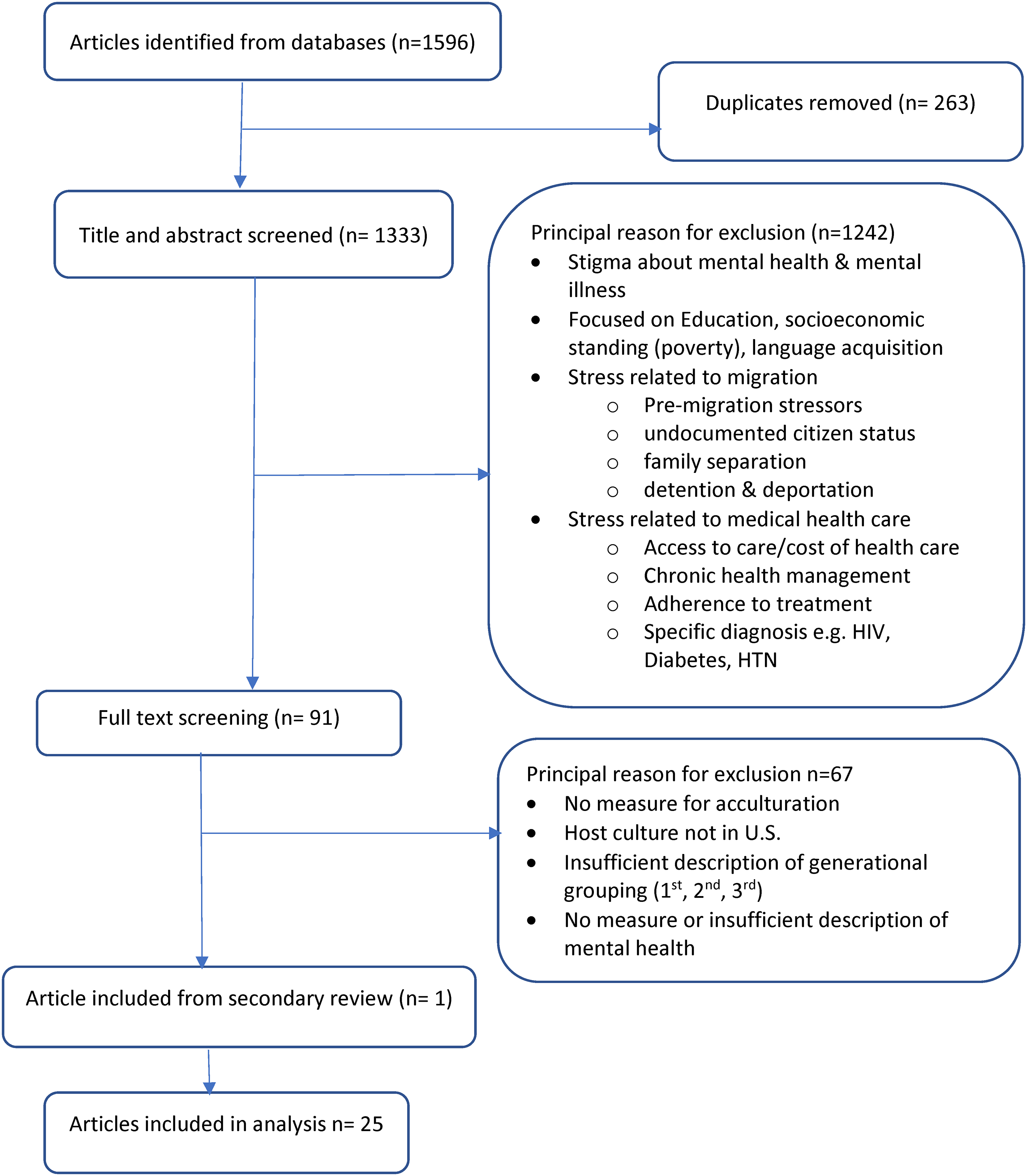
Selection flow chart.
Results
Data Extraction
The relevant studies were classified by author(s), year of publication, cultural sample of study, age of sample, generation, concepts measured, and the relationship between acculturation variables and mental health effects/expression. Generation was defined as the sequence of birth in the United States and determined by the immigration status of immediate older family members living in the United States. The concepts measured and the measurement tools revealed how the study evaluated acculturation in the sample population. The sample reflected how the participants identified their cultural heritage. The data extraction sheet was primarily developed using principles identified by PRISMA for scoping review of individual sources of evidence. Researchers on the review team identified further areas of necessary data relevant to the research question to expand this form. Data extraction and review of articles occurred independently by members of the researcher team. The articles used in data analysis are presented in four tables (see Supplemental File 2). According to Arksey and O’Malley (2005), scoping reviews do not seek to assess the quality of evidence and cannot determine whether studies provide robust and/or generalizable findings; therefore, appraisals of article quality are not required.
Synthesis
An online portal was utilized to facilitate the members of the research team’s review of all article selection and rejection for the review. After the initial count of articles that met the inclusion criteria, a secondary review of all the rejected articles was conducted against the inclusion criteria. Scheduled meetings with research team provided an opportunity for further discussion of the process, the selected articles, and researcher bias. Post-article selection and review, articles were grouped by study participant’s cultural group and examined for cultural nuances that may be otherwise masked when articles are considered as one large body of work. Studies were analyzed according to the behaviors measured as stated in the research question and the relationships to acculturation stress. Generational status and study population were summarized along with measures used and broad findings.
Characteristics of Studies
Of the 25 articles selected for review, all were quantitative in nature except for one. Tummala-Narra and Sathasivam-Rueckert (2016), the only qualitative study included in this review, conducted group interviews with a diverse population of first- and second-generation immigrants 14–20 years of age to highlight the relationship between the lived experience of acculturative stress and associated coping mechanisms. Population included 64 adolescents in the Northeastern United States (19 Asian-Americans, 10 South Asian Americans, 18 Haitian-Americans, and 17 Latino Americans). Twelve of the studies included a diverse sample of participants (see Supplemental Table 1). The remaining 13 articles focused on one population: Hispanic/Latino (7 articles), Asian (5 articles), or Middle Eastern (1 article). These are represented in Supplemental Tables 2–4, respectively. Sixteen of the studies correlated acculturative stress with psychological distress and internalized symptoms (depression, anxiety, somatic symptoms), but four articles did not find a relationship between acculturation and depression. Fifteen articles specified results by immigrant generations. Three articles concluded that acculturative stress was higher in first-generation immigrants (Katsiaficas et al., 2013; Sirin, Ryce, et al., 2013; Sirin et al., 2019) while four concluded that second-generation immigrants had greater acculturative stress (Mancenido et al., 2020; Salas-Wright et al., 2014; Tan, 2016) and three concluded that there were no generational differences (Cervantes et al., 2013; Sirin, Gupta et al., 2013; Wilson & Thayer, 2018).
Diverse Participants
Populations in the articles with samples from multiple ethnic and geographic backgrounds included Afro-Caribbean, African, Middle Eastern, Asian, Hispanic/Latino, European, and non-immigrants. All studies except one reported an increase in internalized symptoms with rising acculturative stress. This diverse sample gives an overall view of various cultural groups but does not highlight individual experiences and manifestations as they relate to acculturative stress. Studies in which non-immigrants were compared with immigrant groups revealed that non-immigrants had the highest rates of anxiety and depression, which supports the healthy immigrant theory (Mancenido et al., 2020; Tan, 2016). By cultural group, African American and Asian adolescents had higher levels of acculturative stress than Hispanic/Latino adolescents (Katsiaficas et al., 2013). The lower level of acculturative stress viewed in Hispanic/Latino populations compared to other cultural groups can be explained by the type of stress being measured in these studies (internalized vs. externalized).
The only qualitative study in the review (Tummala-Narra & Sathasivam-Rueckert, 2016) provided insight into the similarities and differences these diverse groups face when acculturating to American culture. Similarities include cultural identity, pride in culture, cultural adjustments, and relationships while experiencing different types of discrimination, stereotypes, and coping mechanisms.
Hispanic/Latino Population
The seven articles about the Hispanic/Latino population showed an increased focus on externalized symptoms and behavioral expressions of stress and anxiety compared to internalized symptoms. Six articles found that greater acculturative stress was associated with greater levels of externalized (behavioral) symptoms. Three articles addressed topics such as self-harm, substance abuse, and aggressive behavior. Suicidal ideations/thoughts were measured in two articles (Cervantes et al., 2014; Mayorga et al., 2018). Generations did not differ in internalized symptoms but differed significantly in externalized symptoms. Second-generation immigrants reported significantly more aggression and delinquent behaviors than the first generation (Cervantes et al., 2013, p. 462). This supports findings by Pena et al. (2008) in which generational status was significantly related to suicide attempts, problematic alcohol use, and repeated marijuana and other drug use. Suicidal ideation and self-harm in Hispanic/Latino adolescents remain a significant concern for acculturative stress (Cervantes et al., 2014).
Anxiety appears to be more prevalent than depression in the first-generation Hispanic/Latino population, with rates of 28.8 and 6.8%, respectively (Potochnick & Perreira, 2010).
Asian Population
Taking a closer look at the target populations through studies of specific cultural groups may provide insight into the people, beliefs, and values, and the relationships with acculturative processes and mental health. The subgroups of the Asian population revealed varying aspects of acculturative stress that were associated with their psychological distress (Singh et al., 2015). Although Cho and Haslam (2010) found increased time in the United States was associated with greater distress, acculturative stress did not always have a significant effect on outcome measures. Specific factors like ethnic identity, language difficulties, and discrimination were important aspects of acculturative stress that exerted a strong effect on mental health (Cho & Haslam, 2010; Levinson & Rodebaugh, 2013; Singh et al., 2015; Vaghela & Ueno, 2017). Social support and identification with Asian family and culture appeared to be protective factors. Decreased identity conflict was associated with decreased depression as well as lower anxiety for those who were not acculturated to the host culture (Ando, 2014; Cho & Haslam, 2010; Singh et al., 2015; Vaghela & Ueno, 2017). Among college students from various generation classifications, individuals who were not acculturated to the American culture exhibited less anxiety than other population groups inclusive of Caucasian and immigrant groups. While those who experienced low levels of immersion in the Western culture, but struggled with reconciling their ideal cultural identity with their current identity exhibited high levels of anxiety similar to Asian groups who were highly immersed in Western culture (Levinson & Rodebaugh, 2013). The Asian population seemed to fare worse than other immigrant groups when acculturation of any level occurred in the American host culture. The consistent theme among these five articles is that strong ties to the Asian culture are imperative for the mental health of this population across many generations.
Middle Eastern Population
One study cannot represent an entire group of people or their experiences, but it does provide insight into their acculturative processes and the effects on mental health. In order to assess acculturation Wilson & Thayer (2018) utilized Berry's four-category model of acculturation which posits these levels: integrated, separated, assimilated, and marginalized. According to this model, integrated individuals retain their heritage culture while acquiring cultural competency in the host culture. Separated individuals identify with their heritage culture but refrain from participating in the host culture. Assimilated individuals interact and participate with the host culture and do not maintain or identify with the heritage culture. Marginalized individuals adopt neither the host nor the heritage cultures (Wilson & Thayer, 2018, p. 347).
Wilson and Thayer (2018) reported that integrated individuals had significantly lower stress and depression levels than assimilated individuals. This result can be explained by the protective nature of integration which is likely due to an increase in social support in both heritage (family) and host (friends) cultures. It may also be related to a decrease in stressful cultural interactions between the individual and the two cultural environments (p. 350). Furthermore, there were no differences in acculturation between generational statuses.
Discussion
Acculturation is unique to cultural values, beliefs, and ways of life, so understanding the uniqueness of cultural perspectives provides insight for nurses—not only those working in intake, mental health and psychiatric facilities, discharge placement, and other areas where patients exhibiting psychological distress may present with anxiety and depression—to make culturally relevant recommendations for support, therapy, care, and mental health services and treatment. Children of immigrants, inclusive of adult years, may face more intergenerational conflict than their non-immigrant peers, with parents and family members as well as heightened insecurities, as they seek to find esteem, value, and identification from the host culture. Youth and young adults in immigrant families not only experience the typical developmental challenges of growing up like their non-immigrant peers, but also have to negotiate multiple cultural demands from their home and host cultures (Sirin et al., 2019). The emphasis on providing culturally competent and sensitive services to ethnically diverse populations makes it imperative that health-care providers are aware of their client's culture and the ways in which culture interacts with everyday life (Schwartz et al., 2012).
Mental health care providers can explore with their patients how internal conflict would manifest in various aspects of life and health and can bridge the intersection of acculturation and mental health in everyday life. Acculturation is a complex process when considering the individual (education, financial burdens, familial conflicts, cultural discrepancies), societal (job opportunities, racism, social communities), and organizational (medical and mental health care) factors. Each cultural group experiences various components of acculturative stress, but culture will depict how this stress is interpreted and exhibited.
Asian Participants
The results of the studies pertaining to the Asian culture highlighted the importance of being connected to heritage culture. It appeared that acculturation stress was key for identifying anxiety and depression within this culture, otherwise it would go undetected. Anxiety and depression were revealed through self-critical thoughts of failure, underperforming, and rejection. Focus on self-improvement and high academic performance were common factors. Keeping to oneself has often been classified as introverted behavior but can actually mask social anxiety and intrusive thoughts. Negative social reactions also play into the acculturative process as this population may seek validation from peers.
Hispanic/Latino Participants
The Hispanic/Latino culture studies reported this population demonstrating more externalized symptoms than internalized symptoms, as evidenced by increased aggressive behavior particularly in second-generation children (Cervantes et al., 2013). Behavioral issues are not unique to one racial/ethnic group, but the findings in this group could be explained by intergenerational conflict and lack of social support, which is a part of acculturative stress. Reported risky behaviors included self-harm and drug and alcohol use. All the articles about this participant group revealed an increase in anxiety, depression, suicidal thoughts/ideations, and psychological distress across all generations measured, compared to other groups. Acculturation stress includes many factors, and it is unclear if these mental health symptoms are correlated with specific concepts of acculturative stress, but as this population struggles to live between cultures and cultural expectations, there are risks.
Due to the age of the target population, mental health symptoms can be masked as “coming of age” or “finding one's self-identity.” Acculturation studies revealed that acculturative stress is an added layer of psychological distress during an already tough and confusing time in development. Identifying acculturative stress in assessments and therapies triggers the necessity for cultural interventions. Studies that included other populations such as Afro-Caribbean, African American, and Middle Eastern groups revealed similar results: a positive correlation between acculturative stress and anxiety and stress. In the studies with multiple populations, it is difficult to draw firm conclusions about how each group expressed anxiety and/or depression, but what emerged is a common acknowledgment of a cultural strain, and a need for coping strategies.
Highlighting the intersection between acculturative stress and mental health symptoms will provide language and awareness for patients’ current situations while providing an avenue for self-awareness of their mental health needs and the necessary steps for growth. In explaining cross-cultural conflict as a concept in a middle-range theory of cultural marginality, Choi (2014) stated, “Conflict emerges as individuals face distinct value systems with accompanying expectations and are forced to make difficult choices… Acknowledging cross-cultural conflict …allows for individual differences in perception, responses, and mental health outcomes associated with cultural marginality” (p. 296).
Limitations
Although this review has several strengths, it also has a few limitations. This review only focused on acculturation as it pertains to the United States as the host culture. Other host cultures provide varying acculturating experiences for different migrating groups. Also, this review incorporated acculturation in its entirety. The acculturative process has many facets which may not be reflected through this lens. Looking at acculturation through its individual aspects such as language, discrimination, social integration, or socioeconomic status can provide additional dimensions and understanding of this complex human process.
Conclusion
Acculturation is the process of coming to be, functioning, and living in a new host culture while trying to maintain heritage culture. This process of cultural adjustment/change occurs when a group or individual experiences the interaction of previously separate cultures (Wilson & Thayer, 2018). The stress that arises from this is termed acculturative stress. Although children of immigrants were born in the host culture, they still experience acculturative stress. Youth and young adults in immigrant families experience the same development challenges of growing up as their nonimmigrant peers do, but they also have to negotiate multiple cultural demands from their home and host cultures (Sirin et al., 2019). Studying internalized symptoms resulted in mixed conclusions and a call for more studies on acculturative stress. Narrowing the focus to a specific stress stemming from acculturation may help us understand this complex process. As the scope of mental health nursing continues to grow, this review can broaden our knowledge base, particularly for those serving in mental wellness and in pediatric and adult psychiatric facilities, building therapies that not only provide a space for self-expression, but also cultivate culturally appropriate responses to these stressors. There is naturally a stronger response to learning coping strategies and integrating therapies when patients feel understood. As culture is a part of self, understanding of culture, cultural expectations, and cultural behaviors helps to foster therapeutic relationships between patient and nurse.
Implications for Practice and Research
Building on this research to evaluate the variations in acculturative stress according to region and location can further support the growth of this knowledge base. Studies that compare the differences and/or prevalence of acculturative stress in geographic locations where there are systematic structures in place to assist with acclimation to the host culture due to large numbers of minorities, to geographic locations and/or regions where there are few members of minority groups and limited support can help build systematic processes necessary to assist acculturating immigrant groups. Ultimately, understanding acculturative stress, its effects on mental health, and current coping systems, can lead to the development of effective coping strategies, structures, and programs.
Supplemental Material
sj-docx-1-cng-10.1177_10784535241229146 - Supplemental material for Acculturation and Mental Health: A Scoping Review
Supplemental material, sj-docx-1-cng-10.1177_10784535241229146 for Acculturation and Mental Health: A Scoping Review by Cassandre V. Horne in Creative Nursing
Supplemental Material
sj-docx-2-cng-10.1177_10784535241229146 - Supplemental material for Acculturation and Mental Health: A Scoping Review
Supplemental material, sj-docx-2-cng-10.1177_10784535241229146 for Acculturation and Mental Health: A Scoping Review by Cassandre V. Horne in Creative Nursing
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.