
Abstract
Hygge practices embody joy, peace, mindfulness, coziness, and conviviality. Cystic fibrosis (CF) is a progressive condition with complex therapies and physical limitations. Little is known about how hygge practice may impact individuals living with CF. A qualitative study explored how adults with CF use hygge practices to promote wellness and cope with their disease. A purposive network sample of 15 adults with CF who utilized hygge practices completed semistructured audio-recorded telephone interviews. Recordings were transcribed and analyzed using Colaizzi's thematic analysis approach. Results reveal that hygge practices influenced individuals’ aesthetics, attitudes, and activities, deeply impacting the physical and emotional experience of living with CF. Incorporating hygge into CF care may improve psychological well-being and quality of life for members of this community.
Implications for Practice and Research
Most individuals with cystic fibrosis (CF) spend approximately 2–3 h per day on maintenance therapies to prevent lung infections, promote food absorption, and manage multisystem issues. Hygge is characterized by accepting conditions out of one's control, communal engagement, slowing down, finding balance, practicing mindfulness, and appreciating nature. Hygge practices offer individuals with chronic illness an opportunity for respite from the challenges of daily life, supporting coping and self-care by promoting resilience and improved quality of life and fostering intentional moments of comfort, joy, and connection. A phenomenological study of 15 adults with CF revealed the value of hygge practices in promoting wellness and coping with their disease.
Cystic fibrosis (CF) is a chronic, progressive condition impacting almost 40,000 people in the United States (Cystic Fibrosis Foundation, 2023a). Scientific and clinical advances have changed CF's diagnosis, treatment, and prognosis in the past decade. Currently, adults comprise over half of the CF community (Cystic Fibrosis Foundation, 2019). Still, for individuals diagnosed with CF, this complex disorder carries a high degree of burden. Most individuals with CF spend approximately 2–3 h per day on maintenance therapies to prevent lung infections, promote food absorption, and manage the multisystem issues that result from CF (Sawicki et al., 2009). Multiple studies have reported the experiences of individuals living with CF, exploring how intense therapy regimens, physical limitations, and disease progression limit quality of life, leading to increased mental distress, anxiety, and depression (Bathgate et al., 2022; Guta et al., 2021; Lord et al., 2023; Tickner et al., 2022). These psychosocial challenges diminish motivation to adhere to burdensome therapies, which can lead to worsening health outcomes (Havermans & Willem, 2019; Knudsen et al., 2016; Quittner et al., 2014; Sawicki et al., 2009; Smith et al., 2010; Trandel et al., 2019).
Coping mechanisms have long been explored to enhance the lives of individuals with CF (Abbott et al., 2001). Abbott et al. (2001, 2023) describe four primary ways of coping: optimistic acceptance, hopefulness, distraction, and avoidance (Abbott et al., 2001, 2023). A 20-year longitudinal study evaluating ways of coping with CF found that optimistic acceptance was the only coping style that predicted increased survival (Abbott et al., 2023). Gratitude and positive spiritual/religious coping mechanisms (which are also described as optimistic coping mechanisms) are linked with diminished prevalence of anxiety, depression, and treatment nonadherence for individuals with CF (Burgess et al., 2021; Grossoehme et al., 2020; Sherman et al., 2020; Sherman et al., 2021). Each of these ways of optimistic coping demonstrates the characteristics of resilience. The American Psychological Association defines resilience as adapting positively despite unfavorable circumstances through mental, emotional, or behavioral flexibility (American Psychological Association, 2023).
The Nordic region is known for long, dark, cold winters (Jensen & Nielsen, 2018). The Norwegian term hygge (pronounced “hoog-uh”) describes a mindset focused on well-being that seeks contentment in the ordinary aspects of life and challenges one to make the most of difficult circumstances, thus exemplifying resilience (Søderberg, 2017). While Nordic peoples all have culture-specific words to describe similar concepts, the Danes are known for using hygge to cope with harsh environments by appreciating simple comforts and connecting with others. Hygge is characterized by accepting conditions out of one's control, communal engagement, slowing down, finding balance, practicing mindfulness, and appreciating nature (Altman, 2016). According to The Happiness Institute in Copenhagen, hygge activities release oxytocin, which decreases hostility and increases social connection, fostering feelings of love, warmth, and safety (Wiking, 2017).
Hygge is increasingly recognized as a way of life in Western cultures (Princing, 2019). The New Yorker magazine declared 2016 the “Year of Hygge” (Altman, 2016). The following year, eight books and a documentary film were produced about hygge (Altman, 2016). In the wake of the COVID-19 pandemic, the stage was set for hygge, a lifestyle that embraced finding solace in the new normal of social isolation (Kurtz, 2020). Hygge is also being gradually incorporated into various communities facing chronic illness as a coping and self-care mechanism to promote well-being (Hobson, 2023; Ladores et al., 2022; Roth, 2017). Self-care encompasses a holistic approach to well-being, involving deliberate practices that address physical, emotional, and mental needs (Riegel et al., 2012). Hygge practices offer individuals with chronic illness an opportunity for respite from the challenges of daily life, supporting coping and self-care by promoting resilience and improved quality of life despite ongoing health challenges and fostering intentional moments of comfort, joy, and connection (Søderberg, 2017). However, using hygge to improve quality of life and well-being among individuals with chronic illness has not been empirically studied.
The purpose of this qualitative study was to explore how adults with CF use hygge practices to promote wellness and cope with their progressive disease. The study was informed by the lived experience of a member of the CF community who found restoration and focus through the incorporation of hygge into her lifestyle (Ladores et al., 2022). To our knowledge, this is the first exploration of how individuals with CF use hygge practices in their daily lives.
Methods
Descriptive phenomenology was used to explore the lived experiences of adults with CF who practice hygge to promote coping. Rather than an interpretive approach that relies on the prior knowledge of the researcher, the descriptive approach was chosen to explore the unique experiences of how hygge practice influences life with CF and to ensure that no prior knowledge about the phenomenon or biases of the researchers would influence the study findings (Harvey & Land, 2016). The study was guided by Riegel et al.'s (2012) Theory of Self-Care of Chronic Illness, which explores the concepts of self-care maintenance, monitoring, and management as they relate to health promotion for individuals with chronic illness. This theory highlights that those with chronic illness who can maintain self-care benefit from the outcomes of well-being, quality of life, perceived control over the illness, and decreased anxiety.
Descriptive phenomenology is an inductive method of qualitative inquiry that evokes a rich understanding of an individual's lived experience without introducing researchers’ preconceived ideas (Creswell & Poth, 2018; Giorgi, 2009; Moustakas, 1994). Through individual semistructured interviews, participants are invited to share their personal experiences in their own words. These combined experiences are then synthesized to describe the meaning of the phenomena of interest (Creswell & Poth, 2018; Holloway & Galvin, 2017).
Participants
We used purposive sampling to recruit adults over 18 years of age with a diagnosis of CF who have a rich knowledge of hygge practice (Polit & Beck, 2021). The study flyer was distributed to social media groups that support hygge to cope with CF. Additional participants were recruited via snowball sampling. See Table 1 for study-specific inclusion and exclusion criteria.
Study Inclusion and Exclusion Criteria.
Potential participants were emailed additional information about the study's purpose, risks, benefits, and compensation. The eligibility criteria were reviewed with the participants, who were provided the opportunity to ask questions before informed consent was obtained. The final sample size of 15 participants was determined by reaching a point of data saturation, a level of redundancy within interviews where further sampling or data collection is unlikely to yield new or different information (Polit & Beck, 2021). The University of Alabama at Birmingham Institutional Review Board [IRB-300008628] approved this study.
Data Collection and Analysis
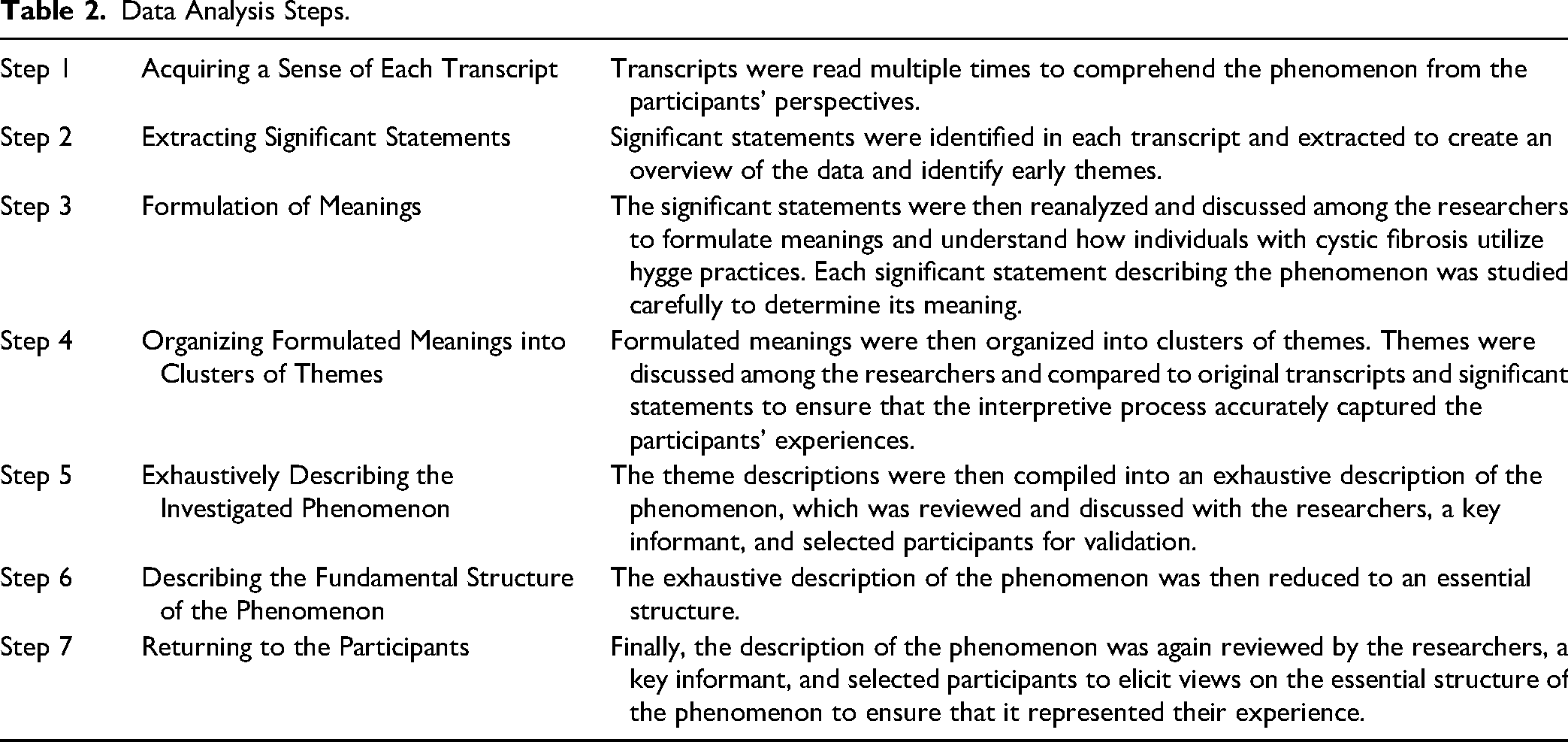
After obtaining verbal consent from participants, semistructured telephone interviews (average length 43 min, range 28–68 min) were conducted by trained research assistants using an interview guide to ensure that essential aspects of the participants’ experiences were captured. Interviews were audio-recorded, transcribed, and uploaded into NVivo (Version 12.7.0), a computer-assisted qualitative data analysis software, to assist in managing data and simplify the coding process (Merriam & Tisdell, 2016). Transcript data were analyzed using Colaizzi's (1978) phenomenological method. See Table 2 for an outline of data analysis steps. Participants were compensated for their time with a curated box of items (valued at $50) that embody hygge and foster its continued use for health and wellness.
Data Analysis Steps.
Study Rigor
Throughout data collection, bracketing of personal experiences and perceptions was performed using field notes to record personal reflections, thoughts about emerging themes, and potential biases (Merriam & Tisdell, 2016). Interviews were completed by two research assistants (LP and BW), and emerging ideas, codes, and themes were constantly compared to the original data to establish interrater reliability. Member-checking was performed with participants to ensure adequate representation of experiences (Holloway & Galvin, 2017). Significant time was spent on data immersion, preliminary analysis, and reflection to ensure adequate data saturation (Merriam & Tisdell, 2016). Thick descriptions of participant characteristics, study design and setting, and direct participant quotes (all names are pseudonyms) allow researchers and clinicians to determine the generalizability of results to their patient population.
Results
Demographics
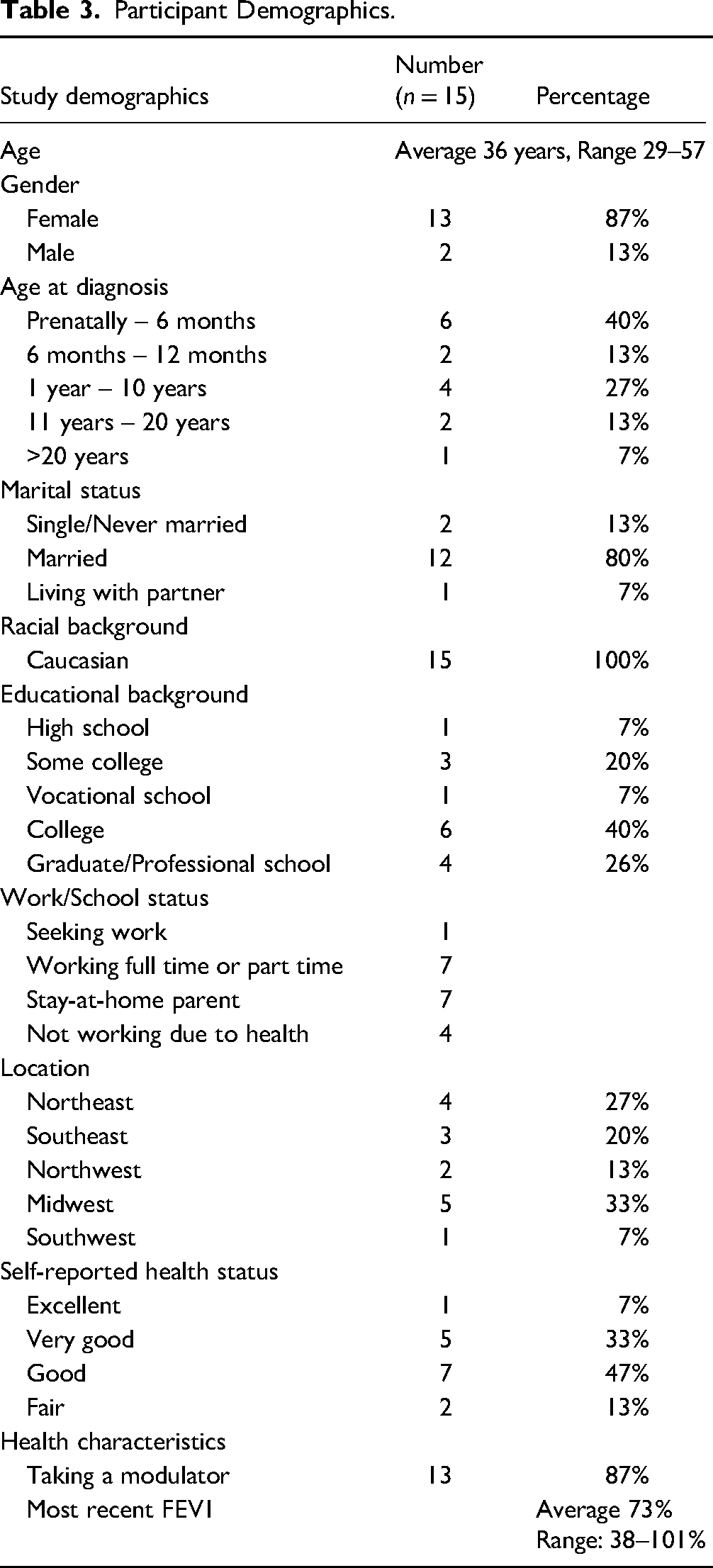
Fifteen individuals with CF who practice hygge completed interviews. Participants were primarily females (87%), Caucasian (100%), and married (80%). The average age of participants was 36, with a range of 29–57. The demographic characteristics of the participants are presented in Table 3.
Participant Demographics.
Health Status
Participants’ health status, partially characterized by their CF-related comorbidities, is shown in Figure 1. Of interest, 11 of the 15 participants reported experiencing anxiety related to CF, and seven reported experiencing depression related to CF. Of the individuals reporting anxiety, five reported receiving both counseling and prescription medication as treatment, while four reported not receiving any formal anxiety treatment (counseling or medication). One individual was taking anxiety medication only, and one other was receiving counseling only for anxiety. Among the seven individuals reporting depression, five reported that they were currently taking medication(s) prescribed for depression, and three were currently receiving counseling. All participants reported that talking with others and leisure activities were stress-relieving activities.
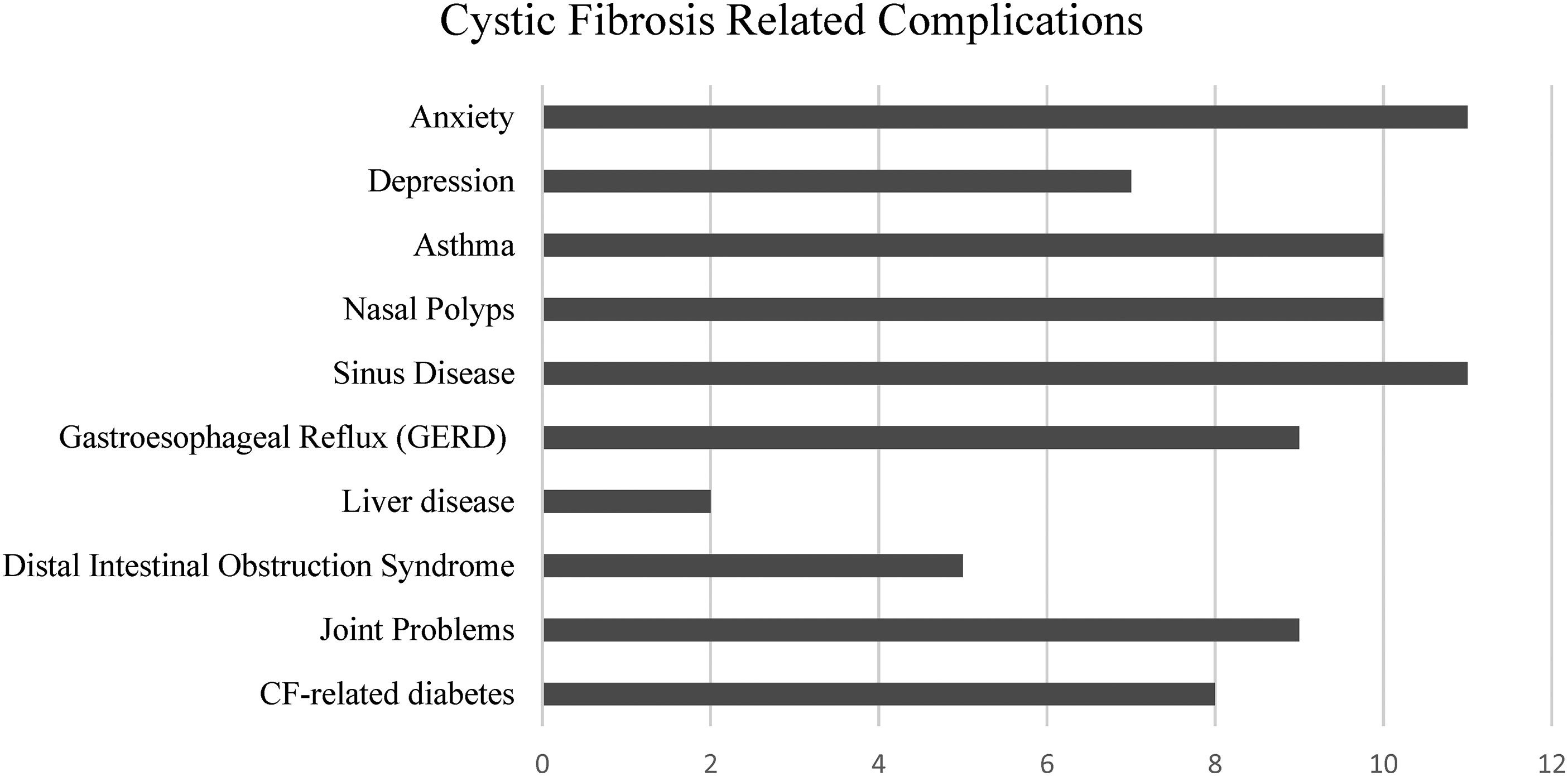
Participant-reported cystic fibrosis-related complications.
Themes
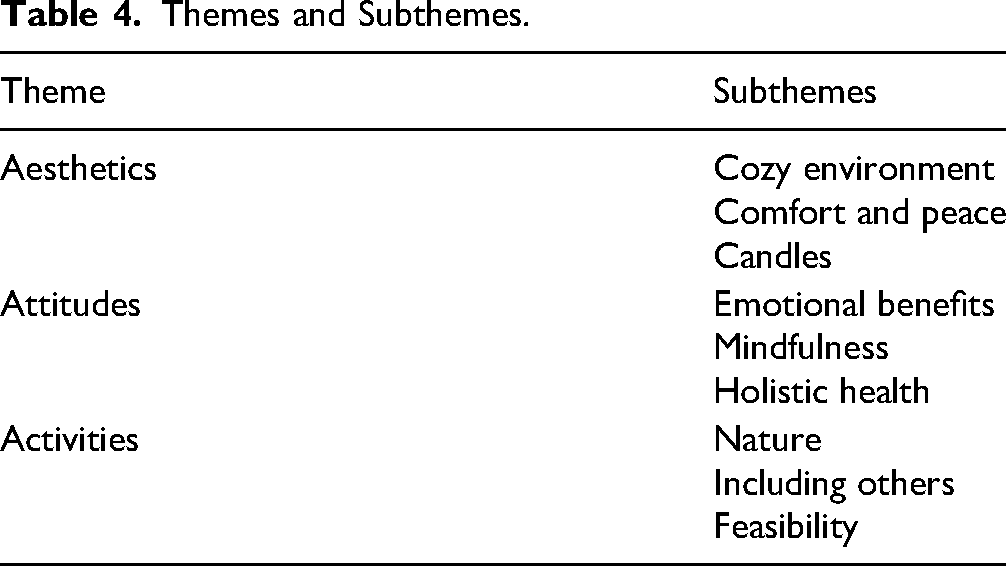
Participant interviews elicited insight into how hygge practices facilitated well-being for individuals with CF. The data initially generated 58 codes or fundamental elements that were meaningful to the phenomena of interest (Colaizzi, 1978). The underlying meanings of the codes were then explored and organized into three major themes, each with three subthemes, which identified how participants used hygge practices to promote wellness and cope with their progressive disease. These themes and subthemes are outlined in Table 4.
Themes and Subthemes.
Aesthetics
Individuals with CF who embraced the practice of hygge described how intentional environmental changes significantly enhanced their quality of life in the context of living with CF. Many participants articulated that creating a cozy, comforting environment made their treatments more tolerable and transformed their overall experience with CF. Soft textures, warm lighting, and carefully curated art played pivotal roles in fostering comfort. For some, the tactile sensations of cozy blankets or the glow of strategically placed lighting contributed to a tangible shift in their emotional well-being. Others emphasized that the revitalization of their surroundings transformed their spaces into “safe havens” that positively influenced their mental energy and overall sense of wellness. Environmental changes guided by the principles of hygge were integral to coping strategies and improved quality of life for individuals navigating the challenges of CF.
Cozy environment
Embracing the essence of hygge, participants recounted the transformative power of incorporating coziness into their surroundings, whether at home or in the hospital. Participants crafted hygge environments to interplay between physical spaces and mental states, allowing their hygge practices to reshape their psychological well-being. As Allie aptly expressed, “I want my environment to match what I would like my mental state to be, so to me [hygge] is about making my physical environment feel a little bit cozier,” capturing the depth of intentionality behind the pursuit of coziness.
The concept of coziness extended beyond physical comfort, with soft blankets, a fire in the fireplace, the soothing warmth of heated blankets, and snuggling with pets or loved ones emerging as recurrent motifs within their accounts. Detailed descriptions of sensory aspects of coziness painted a vivid picture of the emotional sanctuary these elements collectively created. For some, coziness emerged as a transformative force, rendering otherwise arduous self-care tasks more bearable: I always do my morning and evening treatments in my bed. It is just a cozier and more comfortable space. I snuggle with my heated blankets, have a warm cup of coffee or tea, and watch television. It makes something I used to dread something I now enjoy. (Casey) I would bring Christmas lights and pictures to put up to make it feel more cozy…half of my suitcase would be filled with cozy pajamas and socks. I would paint and put those pictures on the wall—anything to make the space feel more calming and not too overwhelming.
Comfort and peace
Feelings of coziness were also coupled with a deep sense of comfort and peace in the environment. Sometimes, this had to be cultivated to ease psychological or physical stressors: “[Hygge] means something that makes me happy, something that makes me feel comforted, something that is just kind of a reset or takes me out of whatever it is I’m dealing with at the moment” (Brandy). For many participants, the peace created by hygge extended beyond mere aesthetics; it emerged as a mindful practice, inviting a deliberate slowing down and a heightened appreciation of their surroundings. Fritz expressed the transformative power of hygge: “[Hygge] gives me permission to slow down and pay more attention.” Sam echoed this sentiment, underscoring the importance of cultivating stillness: “It's so important to have the balance of not being frantic and busy every day, all the time—cultivating that stillness and time to care for your body.” Moreover, participants identified warm baths as a hygge ritual, employing bath salts, aromatherapy, bath bombs, or bubbles to promote physical and mental comfort: “I think taking a bath is a way to find comfort. Soaking my muscles has a physical effect on me and is always fun and relaxing and just relieves my stress” (Astrid).
Candles
Though candlelight is a cornerstone of hygge aesthetics (Søderberg, 2017), its integration within the CF community was more contentious. Within this community, several participants acknowledged the potential for irritation to their lung tissue or sinuses. Other participants incorporated candles into their hygge aesthetics to enhance spaces of warmth and connection. For Sam, candles were a catalyst for shared moments of tranquility and bonding, encapsulating the essence of hygge as a family ritual: “I have a practice with my kids now where we light a candle and sing a song before bed. It's such a good way for us to calm down at the end of the day.” Similarly, J.J. highlighted the sensory joy derived from candle use despite the challenges associated with CF: “I’ve noticed that because I can’t smell very well because of CF, candles bring me a whole bunch of joy. I love looking at them.” In this revelation, the act of candle gazing transcended the limitations of CF, becoming a visual experience that invoked feelings of joy and aesthetic appreciation. Thus, within the CF community, the diversity of experiences underscored the personal and sometimes unexpected ways individuals navigate the interplay between hygge aesthetics and the unique challenges CF poses.
Attitudes
Within the challenging landscape of life with CF, participants revealed a profound narrative of resilience and transcendence through the practice of hygge. Hygge was a transformative force in reframing mindsets, fostering acceptance, and enhancing overall well-being. Participants embraced the emotional benefits of hygge and portrayed the practice as a mechanism for cultivating comfort with oneself amid the myriad of challenges CF presents. Hygge acted as a catalyst for improving quality of life, increasing contentment, and embracing the acceptance of elements beyond one's control. Participants described how hygge practice had increased their joy—a powerful emotional shift that resonated as a source of resilience in the face of adversity.
Moreover, mindfulness was inherent in hygge practices, highlighting intentional actions that distinguished them from ordinary daily occurrences. The cultivation of self-awareness and the art of appreciating simplicity in life are integral facets of the hygge experience. This mindfulness extended beyond activities to a more holistic approach to self-care that improved overall health and well-being. Hygge emerged as a profound and intentional way to engage with life, a transformative practice that offered solace, joy, and a holistic embrace that surpassed traditional medical approaches.
Emotional benefits
Hygge practices fostered resilience for individuals with CF, allowing them to move beyond the negative experiences of chronic illness and find solace. Casey recounted the emotional turmoil intertwined with daily treatments and the transformative role of journaling as a hygge activity during these moments. In her narrative, journaling became a space to grapple with the realities of treatment—a deliberate choice to embrace positivity and self-discovery amid the repetitive and challenging routine. She reflected, “I can use this time to foster hygge thoughts… getting to know myself outside of the lady sitting in the chair who has to do stupid treatments again,” highlighting the power of hygge in reshaping one's internal narrative. For Fritz, hygge became a tangible lifeline that was steadfast regardless of health fluctuations: I have remained able to do these things regardless of my health, whether I’m feeling well or unwell. As I’ve gotten older, I have more health complications, but I can still enjoy these things. It's not like a sport that I have to give up. Hygge is accessible regardless of where I’m at. [Hygge] adds to my quality of life because I can deal with my CF in a more positive way. When I’m going through things that are harder, practicing hygge makes me feel good even if my health isn’t good. I was just focusing all my time on how much pain I was in, how I didn’t feel good, and just not being very hopeful about things. Since I started practicing hygge, I have been able to take control over that, and it has helped me a lot.
Mindfulness
While hygge activities seemed to be ordinary occurrences, such as reading a book, having a meal with friends, or lighting a candle, mindfulness was the common thread that elevated these simple practices into a way of intentional living that sparked deep contentment for participants. Fritz expressed, “It is tweaking the things you do that bring you joy, to slow down and appreciate them, so that it takes on a little extra meaning.” By making these subtle adjustments, the mundane became extraordinary, and the everyday rituals took on heightened meaning and joy. Cultivating self-awareness became a cornerstone for navigating the complexities of living with CF: The biggest difference I notice in my life is the ability to be present and to feel this self-awareness. To take time to listen to my body, be aware of the moment, and focus on what I need to be healthy and well. (Sam)
Holistic health
Hygge practices are not a one-size-fits-all way of living. Personal and deeply meaningful engagement with hygge became a testament to its adaptability, tailoring a lifestyle that offered participants a holistic approach to health and overall wellness. Each had unique expressions of hygge that resonated with their needs and preferences. This personalization underscored that hygge offered a nuanced way of engaging with life.
Hygge practices influenced various dimensions of well-being, bringing about tangible improvements in breathing, mental well-being, body image, and pain control. Everyday activities (e.g., a bath, a warm shower, a foot massage, or a walk outside) were transformed into therapeutic tools for alleviating physical and mental ailments.
Christie provided insight into the transformative and holistic nature of hygge by stating: When I am feeling off-balance in some way, or if I am feeling overwhelmed with my CF, I am reminded to tap into the tools and practices that I have learned from hygge—to take care of myself, my whole self. I may go outside in nature and go for a walk. I just focus on those self-care needs that are easy to ignore or push through.
Activities
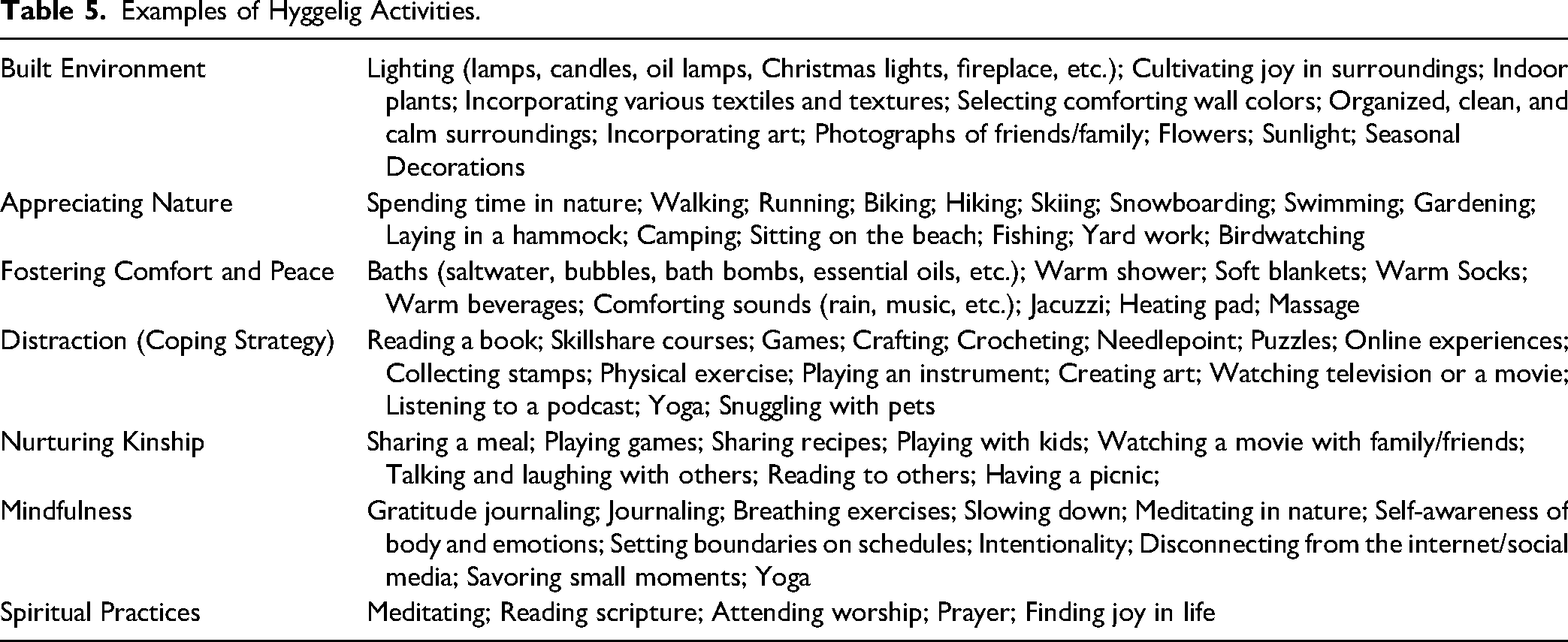
Participants described many activities as hyggelig [pronounced hoo-ga-li; adjective for hygge]. A list of all named hyggelig activities described in participant interviews is in Table 5. Activities were central to hygge practice for individuals with CF, from being in nature to sharing a home-cooked meal with family. The activities described by participants transcended the mundane, becoming profound experiences and tools for improving health. Each activity, whether pursued in solitude or shared with others, carried the potential for a profoundly personal and meaningful experience. The richness of these descriptions exemplified the versatility and accessibility of hyggelig activities, proving that the practice was accessible and feasible for individuals with CF.
Examples of Hyggelig Activities.
Nature
Appreciation for nature is a fundamental element of hygge (Søderberg, 2017), which held true for participants. Simple elements of nature (e.g., sitting in the sunshine, listening to the rain, or appreciating the crunch of leaves underfoot while walking in the woods) brought joy to participants’ lives. Despite being dispersed across the United States, participants shared a collective sentiment—the therapeutic embrace of the outdoors—underscoring the universality of the hygge-nature connection that transcended regional differences.
Astrid described hygge as a “two-armed branch,” symbolizing the delicate equilibrium between indoor coziness and the transformative power of spending time outdoors. In her words, hygge urges individuals not to confine themselves indoors but to venture into the therapeutic expanses of nature. Even during the harshness of unfavorable weather, Astrid highlighted the conscious effort to prioritize time outdoors, recognizing the symbiotic relationship between the outdoor environment and her well-being. Her sentiment reveals the cascade of benefits of nature, “I prioritize some time outdoors because I know that my mind will start feeling better, which means that my body will start feeling better.”
Including others
Practicing hygge was often a journey of self-care and a way to nurture kinship and community. Hygge was not merely a solitary pursuit but a way of living that resonated with familial and community connections. Sam shared the effect of hygge within their family: “What was important to me became important to my spouse and is now important for our family in the way that we live our life.”
Hygge practices were often a collective endeavor, extending beyond the immediate family. J.J. described sharing the hygge experience: My family—I have a lot of cousins and an older sister—we are very much a cozy, loving family. We have a bunch of game nights or movie nights, and it is very cozy and warm, with delicious food and hot tea. It is definitely hygge.
Feasibility
Responses indicated that living a hygge lifestyle within the context of a chronic illness like CF was indeed feasible but that this lifestyle required dedication, mindfulness, and self-awareness. Stacy emphasized the need for a deliberate and mindful approach: People have to be willing to find out what is right for them. You must be mindful of it. It can be hard because you’re running here and there, and suddenly, you realize that you aren’t taking care of yourself. It is important, too, because that can define or change your mood for the entire day.
Amid the affirmations of feasibility, participants also acknowledged the pragmatic aspects of integrating hygge into life with CF. Sam articulated the balancing act required, recognizing that hygge, while not necessarily expensive, demanded setting boundaries: “Sometimes hygge means saying no to things. You have to decide your priority with your time and health and be willing to let some things go for the sake of your sanity.” Hygge is a deliberate choice—a commitment to prioritize well-being despite external demands and obligations. For participants, the feasibility of a hygge lifestyle was marked by the intentional navigation of challenges and the conscious cultivation of a mindset that prioritized self-care, demonstrating that hygge practice was a dynamic and ongoing journey set against the backdrop of life with chronic illness.
Discussion
This is the first study to describe how hygge practices can enrich the lives of individuals with CF. This study demonstrates how practicing hygge cultivates resilience, coping, and well-being for individuals facing a chronic illness with a high treatment burden. Interestingly, most participants reported having anxiety (73%) or depression (46%) related to their CF diagnosis. This was a higher percentage than published population estimates for adults with CF, which provide a 95% confidence interval of 19.6–33% for adults with CF and anxiety and 23.6–31% for adults with CF and depression (Lord et al., 2023). It is possible that individuals with CF who have sought out hygge as a coping mechanism may have a higher baseline prevalence of mental distress, which prompted their search for alternative management approaches.
This study demonstrated how a singular approach does not define hygge practices. Participants described many environmental factors, psychological adaptations, and physical activities that they considered hygge. For participants, hygge was defined as a way of living or coping with chronic illness. Ways of coping with CF have been described as having direct positive or negative influences on health-related quality of life (Abbott et al., 2001; Abbott et al., 2008; Abbott et al., 2023). Abbott et al. (2008) highlight how coping with CF is often complex, with individuals frequently using multiple coping methods, and describe how optimistic acceptance and distraction coping styles can have a synergistic effect on improving health-related quality of life for individuals with CF. In the present study, participants’ experiences with hygge as a coping mechanism for CF frequently captured this synergy between optimistically accepting their reality of chronic illness and distracting themselves from the negative aspects of their disease to refocus their mindset and achieve self-care.
One distracting coping behavior participants described was linking dreaded tasks with rewards. This was portrayed as performing daily care rituals in a cozy environment or partnering dreaded care rituals with a positively perceived task, such as journaling, watching TV, or enjoying a warm beverage. In his book, The Power of Habit, Duhigg (2014) describes the neurological pattern that governs habit creation—a cue prompts a routine, followed by a reward. In time, the cue and reward create a sense of craving; the ritual becomes a habit. For some participants, self-care meant being away from what they enjoyed, but when treatments were partnered with a hyggelig task, there was a greater incentive to perform self-care. This partnership between undesirable but necessary care tasks and desirable rewards may have implications for improving care adherence for individuals with CF who suffer from depression and burnout related to their chronic illness care.
For participants in this study, hygge practices fostered resilience, which is positively linked to improved mental and physical outcomes in CF (Havermans & Willem, 2019; Muther et al., 2018). In a qualitative study examining experiences of coping with CF, Friedman et al. (2022) described strategies that individuals with CF employed to build resilience: relaxation, meditation or mindfulness, physical activity or exercise, distraction, breaking down sources of anxiety into manageable tasks, practicing disclosing CF to others, reframing negative thoughts, positive self-talk, and use of social support. These actions closely mimic the activities described in the present study.
The aesthetic qualities of participants’ environments were interwoven with their sense of peace, comfort, and tranquility. Individuals with CF explained how their built environment aided their mental and physical well-being. For many, due to the nature of CF, this environment extended beyond the home and into the hospital setting. Participants frequently spoke of how they “brought hygge to the hospital” by manipulating the hospital room's aesthetics using lighting, art, and comfort measures from home.
Lighting is a crucial aspect of hygge in Nordic culture (Sodergren, 2017), and the impacts of indoor lighting on psychology and mood have been extensively studied both in and outside health-care settings. A review of 64 research articles on indoor lighting reported that warm artificial lighting and increasing daytime sunlight exposure optimized feelings of relaxation (Kong et al., 2022). Light exposure and aesthetics have been studied more extensively in specific healthcare settings such as labor and delivery rooms, children's hospitals, psychiatric facilities, dementia care units, and neonatal care units (Balabanoff, 2023; Chaudhury & Cooke, 2014; Hazelhoff et al., 2021; Nourmusavi Nasab et al., 2020; Ulrich et al., 2018). Still, only one study has examined hospital light exposure and depression in adults with CF, a population known to have frequent and extended hospitalizations (Kopp et al., 2013).
Participants reported that hygge practices were both accessible and feasible for incorporation into everyday activities. It is, however, important to acknowledge that, even when inexpensive or free, many of the hygge activities described by study participants require a certain degree of privilege. Not all individuals with CF can take the time required for self-reflection and mindful self-care behaviors. Many individuals with CF face socioeconomic burdens (e.g., poverty, unemployment, unreliable housing or utilities, food insecurity, lack of transportation, and limited access to health care or medications), all of which negatively impact CF outcomes (Jennings et al., 2022; Oates & Schechter, 2021). Thus, exploring screening and support for individuals with socioeconomic burdens in the CF community must be a primary step in identifying ways to improve self-care.
Participants described how this way of life enhanced their ability to achieve self-care through mindful self-reflection, mitigation of health-related burdens, coping with what was out of their control, and appreciating the small comforts of nature and the aesthetics in their environment. They described hygge as enhancing their overall well-being, quality of life, and perceived control over CF. These findings are consistent with the Self-Care Theory of Chronic Illness (Riegel et al., 2012). Figure 2 depicts how hygge practices for individuals with CF accord with the Self-Care Theory of Chronic Illness.
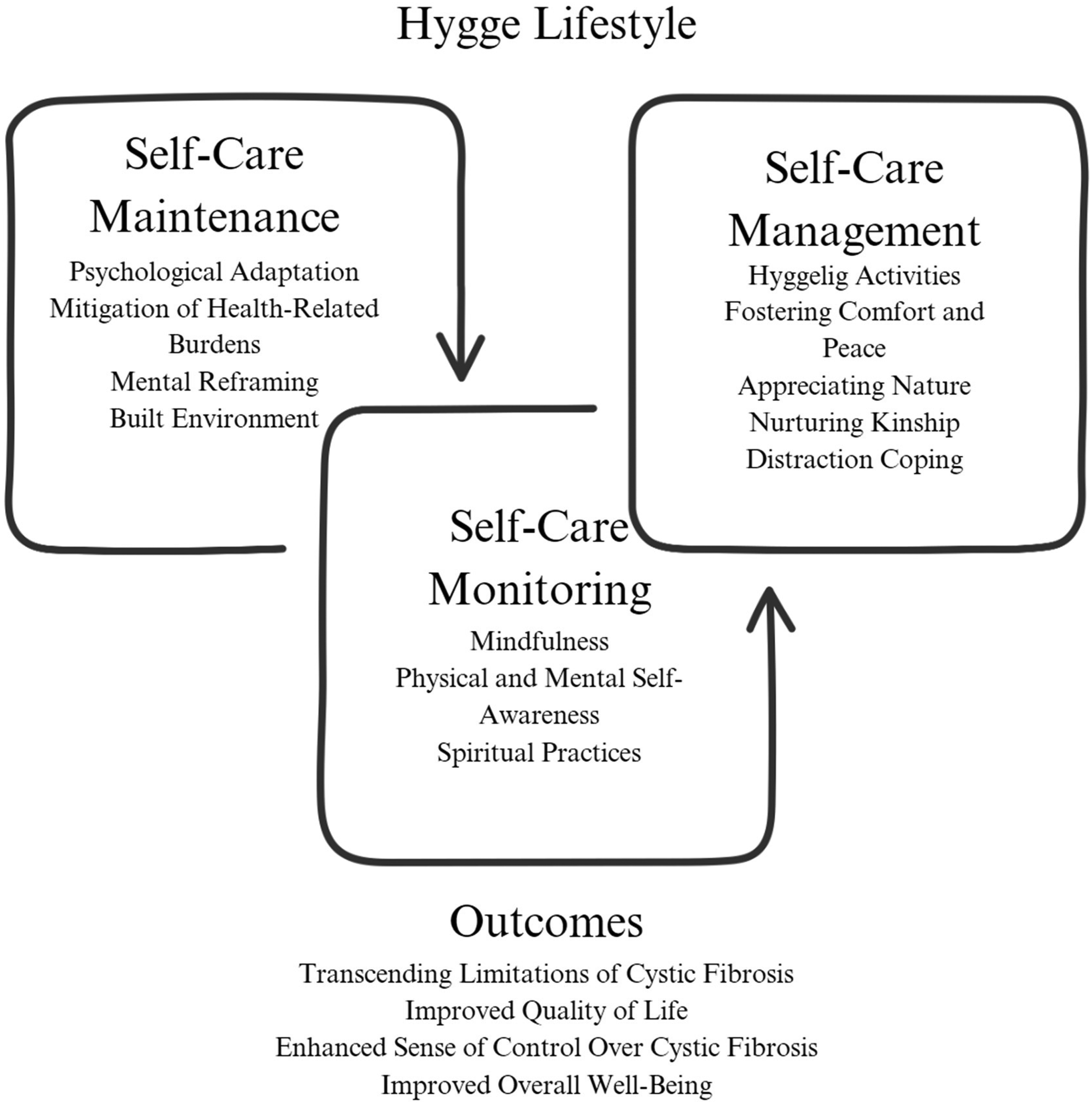
The self-care theory of chronic illness: how hygge practices promote health for individuals with cystic fibrosis.
Strengths and Limitations
The strengths of the present study include (1) involvement of an integral member of the CF community from study conception through completion; (2) rigor of data collection and analysis; (3) richness of data obtained from study participants; and (4) innovation of evaluating coping mechanisms for this vulnerable population. Consistent with a phenomenological approach, the present study included a small sample size of individuals with CF who utilize hygge practices for coping with their chronic illness. Participants self-selected based on the eligibility criteria listed in the study flyer or through snowball sampling, introducing the potential for self-selection biases. Individuals in this study had a higher prevalence of reported comorbid anxiety and depression than the published population prevalence, which could indicate that those with less anxiety and depression chose not to participate.
Purposive sampling, while valuable for gaining a deeper understanding of the lived experience of a phenomenon, limits generalizability (Polit & Beck, 2021). The focused recruitment of individuals with CF who practice hygge intentionally resulted in findings not representative of the broader population.
The homogeneity of the sample was another limitation. Despite strategic recruitment efforts, we faced difficulties recruiting male and minority individuals with CF who practice hygge. It is important to note that more than 90% of individuals diagnosed with CF are of Eastern European Caucasian descent (Stephenson et al., 2017); however, including racial and ethnically diverse participants would strengthen the study's generalizability (Ladores et al., 2023). Additionally, most participants’ socioeconomic status (estimated by education attainment and employment status) was above average, which limits the understanding of the usefulness of hygge as a coping mechanism for individuals of lower socioeconomic status.
Implications
This project directly addresses the mission of the Cystic Fibrosis Foundation, which is to improve the quality and quantity of life of everyone with CF (Cystic Fibrosis Foundation, 2023b). The practice of hygge outlines simple self-care behaviors that have the potential to make a positive impact in the lives of individuals with CF. Table 6 outlines strategies for clinicians who wish to incorporate information on hygge as a coping mechanism in the clinical setting. Findings from this study can be applied beyond the CF population and can be used to raise awareness about the benefits of hygge for anyone with a chronic illness who would like to improve their physical, emotional, and mental health. Future research to explore hygge practice integrated with traditional Western medicine may provide critical information about its potential utility in clinical care. Lastly, educating clinicians about hygge's practical benefits would advance its reach and acceptability.
Incorporating Hygge in the Clinical Setting.
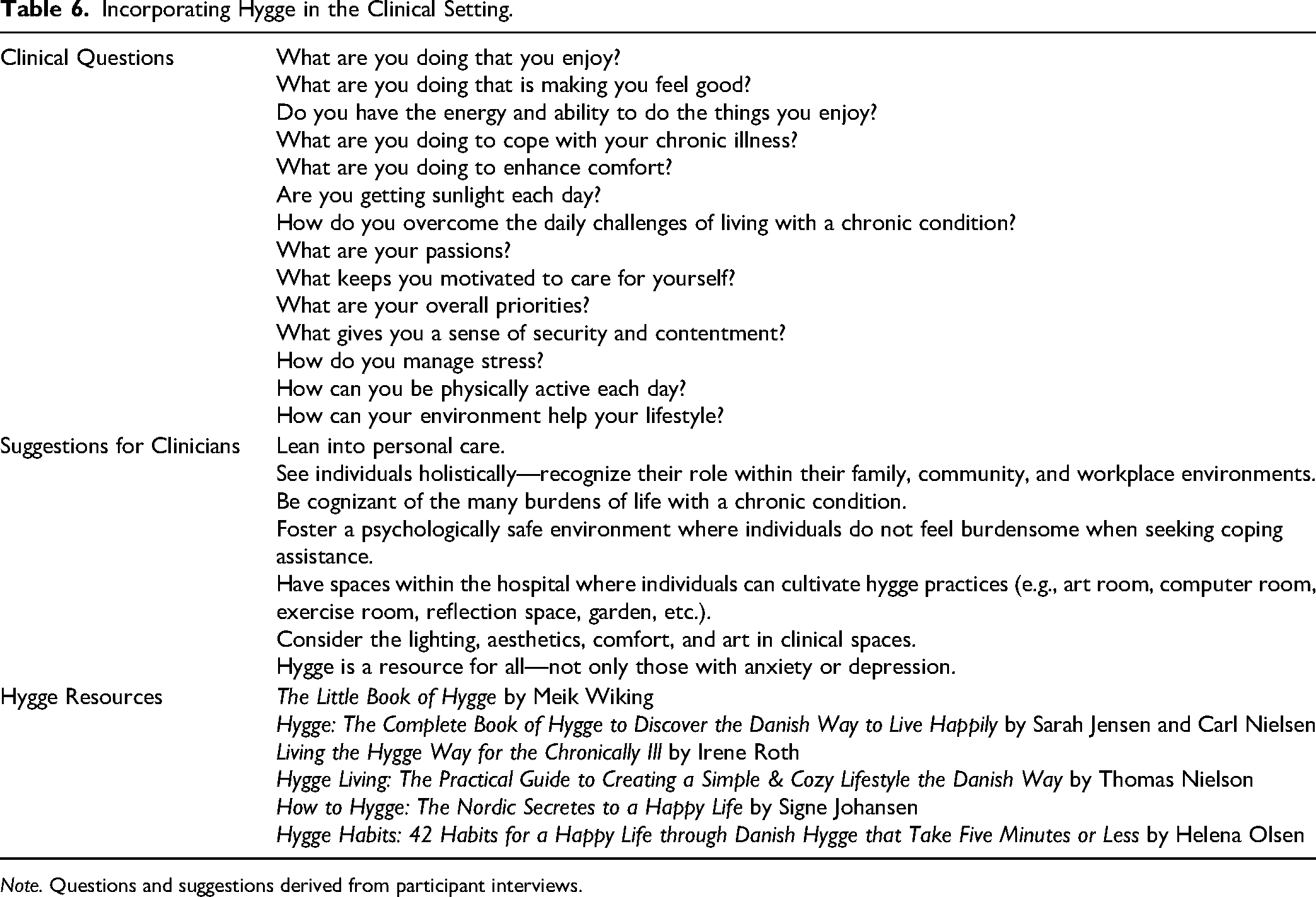
Note. Questions and suggestions derived from participant interviews.
Conclusions
Hygge practices can bring peace and comfort in various environments and circumstances, offering a holistic approach to well-being that transcends the care burdens of life with CF. Through simple, intentional practices, hygge offers individuals with CF the opportunity to experience hope and joy despite daily stressors. Disseminating knowledge of how hygge can be incorporated into CF care may provide a mechanism to improve psychological well-being and quality of life for this community.
Footnotes
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclose receipt of the following financial support for this article's research, authorship, and/or publication: This work was supported by the Alabama Friends of Cystic Fibrosis and the University of Alabama at Birmingham Blazer Graduate Research Fellowship.
Author Biographies