
Abstract
Introduction:
Actions of physical violence, harassment, or other threatening and intimidating behavior characterize workplace violence, often subsequently followed by seclusion to maintain safety in emergency department (ED) and psychiatric settings. Though there is no universally identified benchmark of acceptable rates of seclusion, April to September 2023 preintervention rate of seclusion hours on a psychiatric ED unit at a public state hospital in the southeast was 5.57/1,000 patient care hours, exceeding current comparison data from Centers for Medicare and Medicaid Services (CMS) for calendar year 2022 with a state average, 0.26/1,000 patient care hours and national average, 0.35/1,000 patient care hours.
Aim:
This project aimed to reduce seclusion rates through the implementation of a violence risk identification and management protocol.
Methods:
Interventions included brief training and implementation of a violence risk protocol using the Violence Assessment Tool (VAT) and seclusion debriefing.
Results:
Reports of workplace violence decreased by 25% in the psychiatric ED and 17% across the adult psychiatric inpatient units, and there was a cumulative decrease in Inpatient Psychiatric Facility Quality Reporting seclusion rates by 5% across the adult psychiatric inpatient units where the components of the VAT were communicated in report from the psychiatric ED.
Conclusion:
Early identification of violence risk, patient-specific agitation factors, and de-escalation preferences in the ED setting may have the potential to improve safety through reduced seclusion and workplace violence events. Future research could study patient perspectives of the VAT as a patient-centered tool in de-escalation to reduce seclusion.
Introduction
Workplace violence impacts the United States by approximately $151 billion annually, averaging roughly $250,000 an incident (Chapin & Koller, 2022). Occupational Safety and Health Administration (n.d.) defines workplace violence as “any act or threat of physical violence, harassment, intimidation, or other threatening behavior that occurs at the work site.” In emergency department (ED) and psychiatric mental health inpatient (IP) settings, when patient behavioral emergencies present an imminent risk of harm to self, staff, or others, qualified staff are trained and authorized to initiate locked door seclusion (American Psychiatric Nurses Association, 2022). The Joint Commission defines seclusion as involuntarily confining a patient in a room alone and preventing the person from physically leaving the room (2020). Seclusion may be necessary when less restrictive measures would present a greater threat to the safety of the patient or others and should be discontinued as soon as possible (Centers for Medicare and Medicaid Services, 2020).
The current project focuses on the seclusion hours reported on a psychiatric ED unit from April through September 2023, 5.57 seclusion hours/1,000 patient care hours. Though there is no universally identified benchmark of acceptable rates of seclusion (Staggs, 2020), limited data are available for comparison rates in psychiatric ED settings, and the pre-intervention rate exceeds current Inpatient Psychiatric Facility Quality Reporting (IPFQR) CMS data for calendar year 2022 with a state average, 0.26/1,000 patient care hours and national average, 0.35/1,000 patient care hours (Medicare, n.d.). The comparison IPFQR data may appear lower as patients are being stabilized with treatment during their hospitalization, whereas patients presenting at the ED may be at the height of an acute crisis. The Joint Commission includes seclusion as a quality-of-care indicator, and rather than a form of treatment, the use of seclusion or restraint is considered treatment failure with high rates as evidence reflective of this failure (Du et al., 2017; Recupero et al., 2011). Following national standards of care to prevent seclusion to the greatest extent possible (APNA, 2022), staff must first attempt alternatives such as therapeutic communication, proactively recognizing triggers of agitation and aggression, de-escalation, and treating illness through pharmacological means (Gaynes et al., 2017). Following national standards to prevent seclusion to the greatest extent possible (APNA, 2022), staff must first attempt alternatives such as therapeutic communication, proactively recognizing potential triggers of agitation and aggression, de-escalation, and treatment through pharmacological means (Gaynes et al., 2017). Studies focusing on the effects of seclusion notice an increased length of stay with patients who experienced seclusion during their hospitalization (Chieze et al., 2019), and patients may experience loss of trust in mental healthcare and emotional distress with feelings ranging from anger, sadness, fear, anxiety, injustice, self-blame, and rejection (Hawsawi et al., 2020). Strengthening competencies in patient-centeredness and relationship-based care that fortify the therapeutic relationship may improve patient safety (Svensson, 2022).
A systematic review by Gaynes et al. (2017) included randomized controlled trials, cluster-randomized control trials (CRTs), nonrandomized control trials, and retrospective cohort studies to evaluate violence prevention and de-escalation strategies’ effectiveness in adult acute psychiatric care settings, such as seclusion reduction interventions. Two of the CRTs provided evidence supporting risk assessment protocols decreasing aggressive incidents, whereas multimodal strategies, such as six core strategies (6CS), and risk assessment may reduce initial or subsequent use of seclusion or restraint incidents (Gaynes et al., 2017). Evidence supports the use of a multicomponent intervention to reduce seclusion rates, including debriefing and assessment tools, leadership engagement, and protocols incorporating safety initiative programs such as 6CS and Safewards (Bowers et al., 2015; Fletcher et al., 2017; Gaynes et al., 2017; Huckshorn & LeBel, 2024; Putkonen et al., 2013; Wieman et al., 2014). At the practice site, there is a policy for seclusion of patients presenting imminent risk of harm, but there was no standardized preventative screening process for all patients. The aim of this quality improvement project was to reduce seclusion and workplace violence rates through the implementation of a comprehensive protocol that assesses violence risk upon admission to the unit and identifies patient-specified agitation factors and de-escalation preferences, and the use of a seclusion debriefing tool. Exploring alternatives to seclusion is vital, as seclusion can be traumatizing for patients and staff (Sacks & Walton, 2014). Efforts to improve the therapeutic alliance through patient-centered approaches that identify specific triggers, antecedents, and effective de-escalation may optimize quality and safety.
Methods
Context
The project setting was a psychiatric ED at a large academic medical center in the southeast United States. The unit is a 12-bay area of the ED that cares for patients awaiting psychiatric consults and boards patients waiting on bed placement in an IP facility. Staff include social workers, physician assistants, psychiatrists, registered nurses, therapeutic assistants, patient care technicians, and patient safety companions. Patients present with various diagnoses and mental health complaints. Some patients present voluntarily, and others present involuntarily. Pre-intervention comprised April to September 2023, followed by post-intervention months from October 2023 through February 2024.
Interventions and Procedures
Brief Training
The Nursing Professional Development Expert collaborated with the nurse manager in preparing the brief training that was delivered for the September monthly staff meetings in the psychiatric emergency unit and the three adult IP psychiatry units (geriatric, general adult psychiatry, and acute care). One month prior to the intervention initiation, during the monthly staff meeting, a brief 5- to 10-min training was provided on the violence screening protocol and the staff debriefing tool, including an example case scenario to engage staff in the training process. Education was reinforced monthly during staff meetings, shared governance meetings, and with unit-based staff leader champions.
Implementation of an Evidence-Based Screening Protocol for Violence Assessment and De-Escalation and Coping Strategies
The main intervention was a comprehensive screening protocol, the Emergency Medical Services Violence Assessment Tool (VAT), a copyrighted tool used with permission that includes a violence risk assessment and identification of patient-specified agitation factors and de-escalation preferences (Public Services Health and Safety Association [PSHSA], 2017). Further testing is needed to determine the reliability and validity of the tool. Section A of the VAT, completed by the charge nurse, measures violence risk and contains nine items, eight observable behaviors, and if a patient has a known history of violence. Each item is worth one point for a score range from 0 to 9. Observable behavior items include “confused; irritable; boisterous; verbal threats; physical threats; attacking objects; agitate/impulsive; paranoid/suspicious; substance intoxication/withdrawal; socially inappropriate/disruptive behavior; body language” (PSHSA, 2017). Section B includes actions to consider based on the stratified risk score (low 0, moderate 1–3, high 4–5, very high 6+). If the patient was noted to be at moderate or greater risk, staff responded accordingly to address known triggers using therapeutic communication techniques while implementing safety measures in alignment with the organizational policy that were most appropriate given the patient’s presentation. Section C includes check boxes for agitation factors and de-escalation preferences specified by the patient followed by space for free text for the patient to elaborate (PSHSA, 2017). The VAT assessment was documented by the nurse receiving the patient and inputted the score on the transfer tracker, a log tracking throughput within the ED, and patient assignments. The score, agitation factors, and de-escalation techniques were noted on the nurse report sheet to be communicated at handoff at shift change to the next nurse and in report to the IP nurse. As patients were admitted, the communication of this information to the IP nurses was tracked with a charge nurse checklist tracking if each of the VAT components were communicated in report: score, agitation factors, and de-escalation preferences.
Post-incident Debriefs
Post-incident debriefs were also included in the intervention as they can be therapeutic for staff and patients alike after behavioral escalation occurs that may or may not result in the seclusion of a patient. During the implementation phase of this project, an evidence-based staff debriefing tool (Table 1) adapted with permission from Huckshorn and LeBel (2024) assisted in the identification of antecedent behaviors, triggers, and improved awareness for the staff and patient in what may have been beneficial in preventing further escalation episodes. The charge nurse led the debriefs, documenting triggers, effective de-escalation strategies, and what the patient said could have been helpful. An incident report was completed in the organizational safety incident reporting system, and debriefs were uploaded in the report. Debriefs occurred immediately postincident with the charge nurse and other care team members who witnessed or were involved in the encounter such as other nurses and therapeutic assistants. The debrief with the patient occurred separately with the charge nurse and the patient following discontinuation of seclusion.
De-Escalation Debriefing Tool.
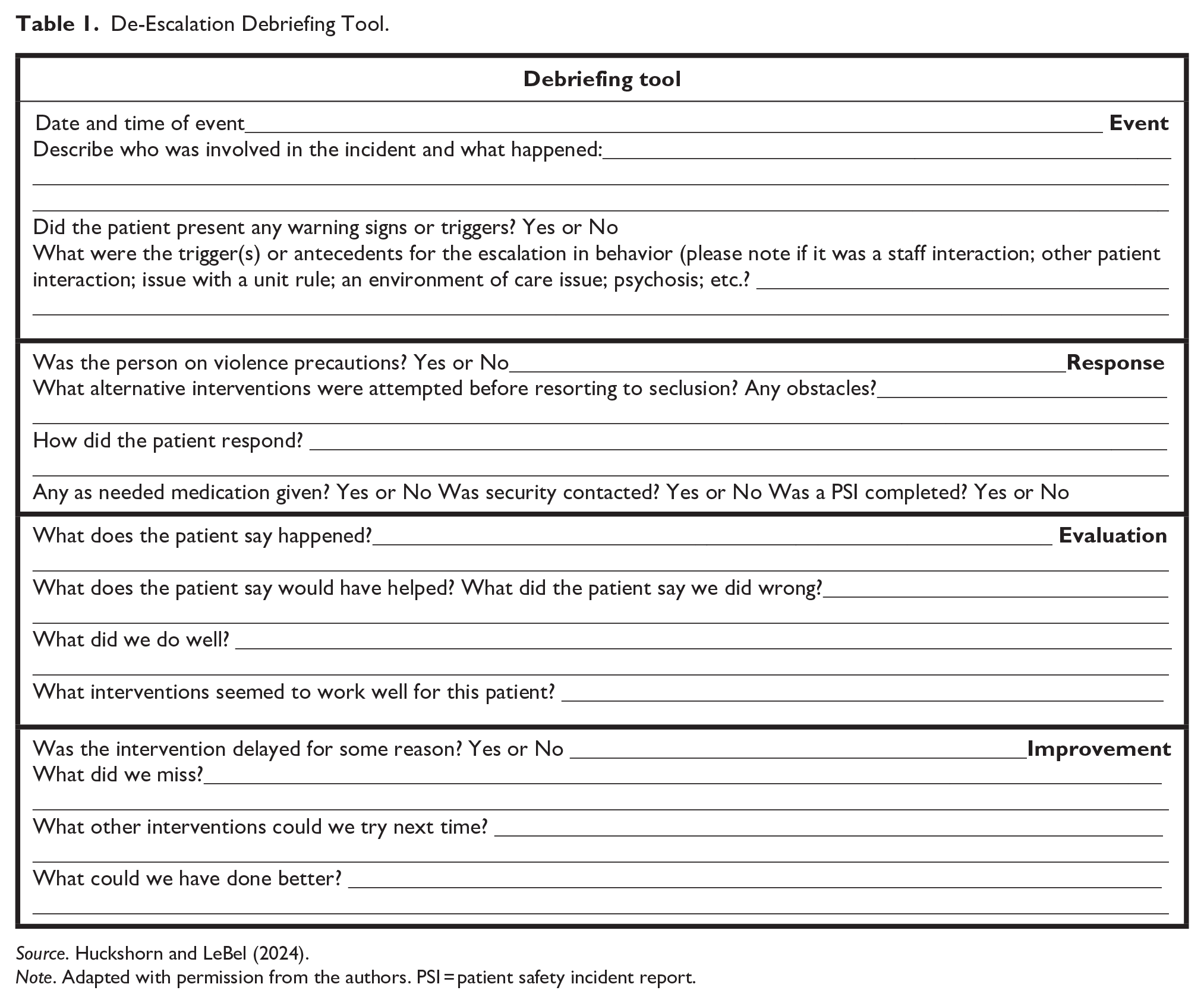
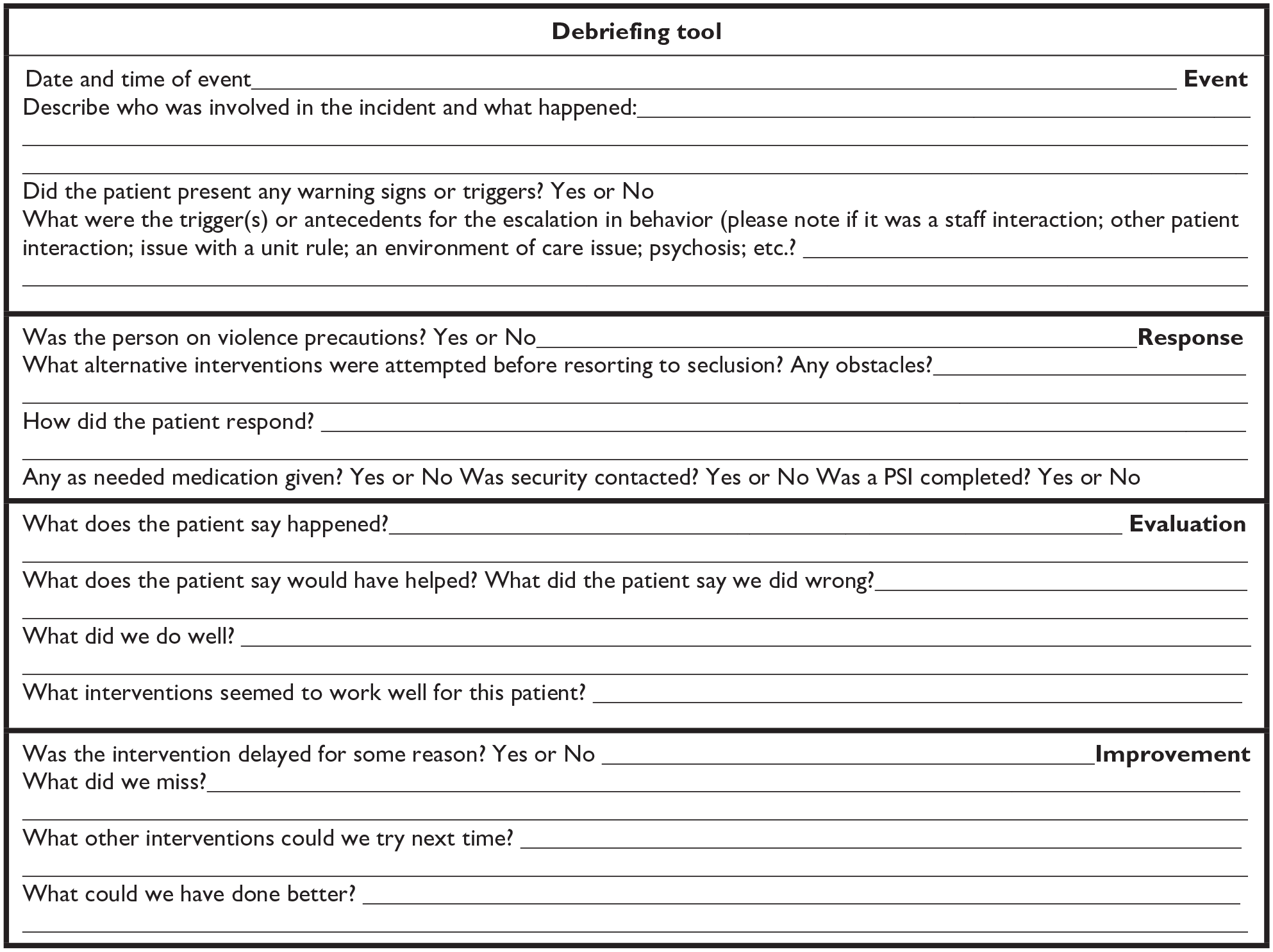
Source. Huckshorn and LeBel (2024).
Note. Adapted with permission from the authors. PSI = patient safety incident report.
Measures
Process Measures
Process measures for this project included the percentage of patients screened with the VAT tool, the percentage of patients who screened high-risk on the VAT tool, the percentage of patients whose VAT score, escalation factors, and de-escalation techniques were communicated in report handoff to the admitting IP nurse, the percentage of patients with seclusion events who have a debrief, and the percentage of staff trained. The percentage of staff trained was determined through attendance of initial staff meetings on each of the units.
Outcome Measures
The outcome measures for this project included the number of seclusion hours per thousand patient care hours each month and the total number of workplace violence reports during the post-implementation period. IPFQR is a quality-of-care indicator metric reported to CMS. In the psychiatric ED, the measurement of the seclusion incidence rate divides length of stay hours by seclusion hours multiplied by 1,000. The safety incident reporting platform includes a selection for workplace violence used to report any acts of violence or aggression toward a care team member.
Analysis
Data were analyzed using descriptive statistics for frequencies and proportions pre- and post-implementation of the intervention.
Ethical Considerations
Prior to the initiation of this quality improvement project, a detailed project description was submitted through the university’s automated quality improvement certification tool and deemed exempt from further institutional review board review as the project intended to improve the practice process in the setting.
Results
Process Measures
During the implementation phase from October 2023 through February 2024, 1,043 patients arrived into the psychiatric ED: 78.72% (821/1043) had a documented VAT score and 10.11% (82/821) scored high-risk on the VAT screening tool. Other process results during the implementation phase included 52.63% (20/38) of seclusion events had a debriefing form completed, 49.64% (274/552) of admitted patients had the VAT score communicated in report to the receiving IP nurse, 48.01% (265/552) of the admitted patients had agitation factors communicated in report, and 48.19% (266/552) of the admitted patients had de-escalation preferences communicated in report. Adherence to the interventions was calculated biweekly throughout the implementation phase and reinforced monthly in staff and shared governance meetings and in-person with unit staff shift leaders. Prior to implementing the intervention, 61.54% (8/13) of the psychiatric ED nurses and 62.74% (32/51) of the psychiatric IP nurses received brief training on the VAT and debriefing tool during the staff meetings (Figure 1).
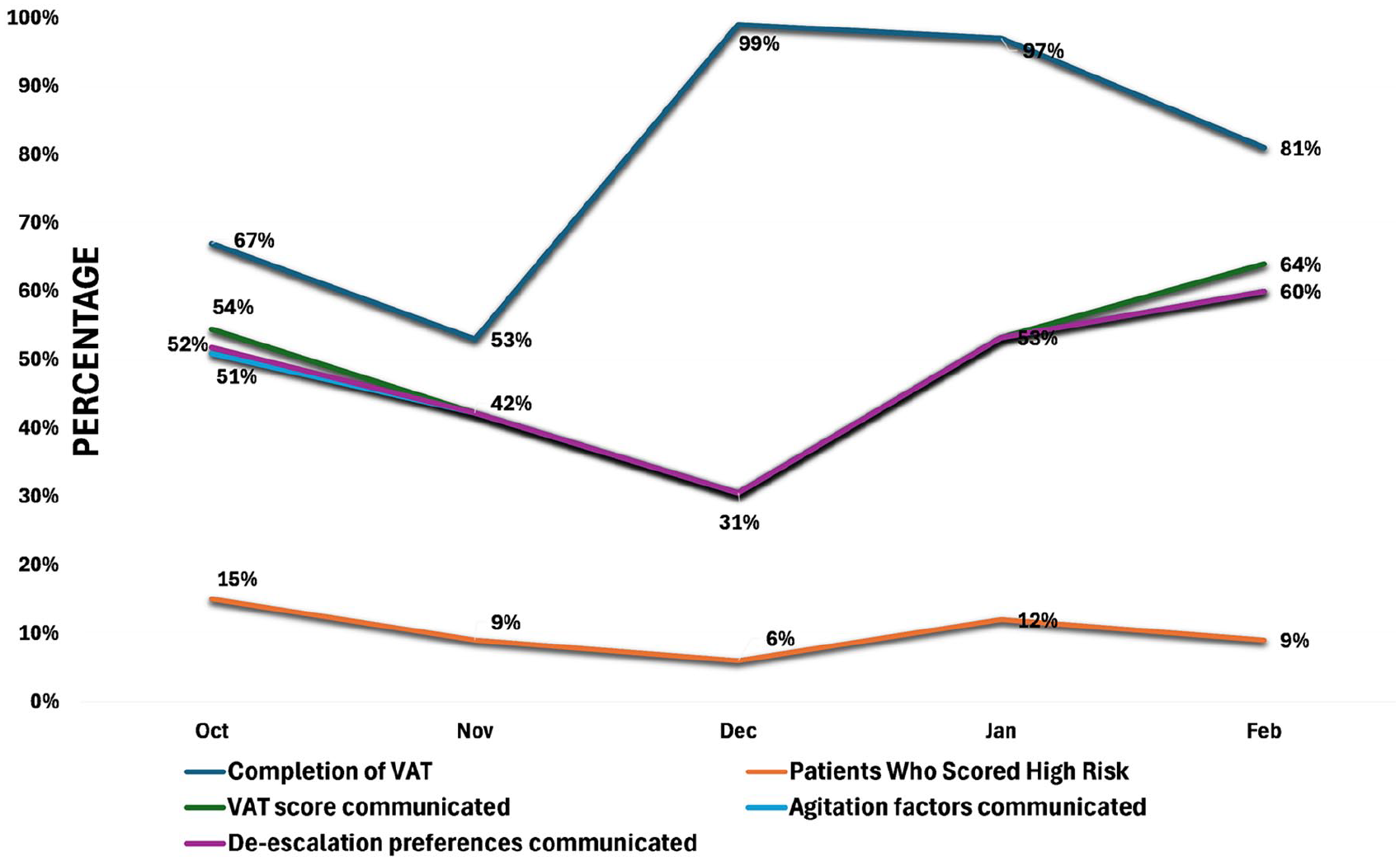
Percent compliance of process measures.
Adherence to utilization of the seclusion debriefing tool varied across the implementation phase with 67% compliance in October to 100% in November and January and 50% in February, despite a drop in compliance for December at 0% which illustrated the importance of reinforcing the tool to improve staff buy-in. The greatest percentage of patients scoring high-risk at 15% arrived in October compared to the lowest percentage of patients scoring high-risk risk at 6% that arrived in December.
Outcome Measures
As shown in Figure 2, the average seclusion rate pre-intervention was 5.56 seclusion hours per 1,000 length of stay hours compared to the post-intervention rate of 3.73 seclusion hours per 1,000 length of stay hours, an overall 33% decrease from pre- to post-intervention less the outlier month of November. In November, while seclusion was implemented for nine patients, three of these patients represented 76% of the total seclusion time for this month. There was a decrease in workplace violence reports in the psychiatric ED by 25%, with four reports during the preintervention period and three reports during the post-implementation period.
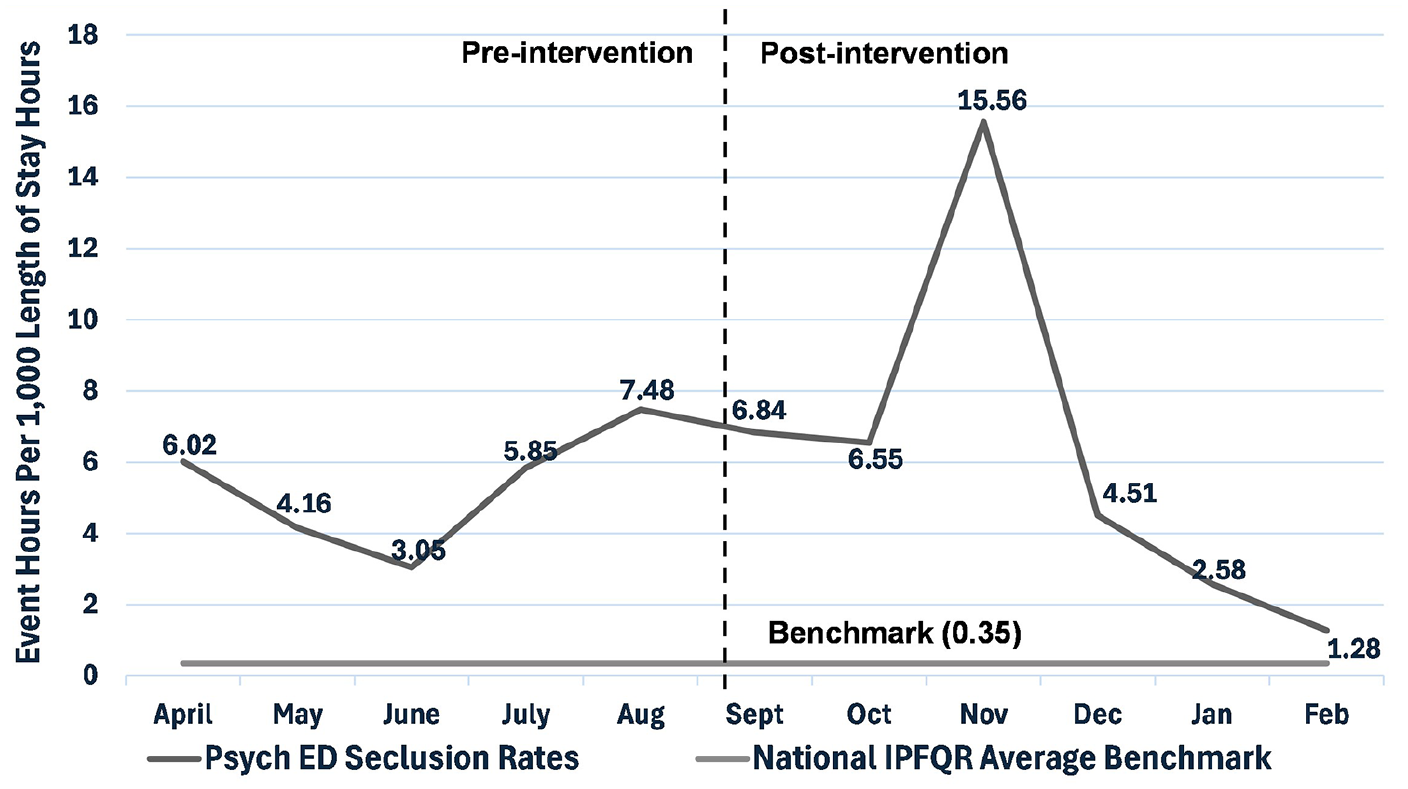
Event hours per 1,000 length of stay hours.
Discussion
The purpose of this project was to implement an evidence-based intervention to decrease seclusion and workplace violence rates. Incorporation of a violence risk assessment as part of a multimodal approach may reduce initial and subsequent seclusion incidents (Gaynes et al., 2017). Overall, the findings demonstrated that implementing this intervention was feasible and may reduce seclusion rates in a psychiatric ED. This aligns with evidence in the literature recommending assessment tools such as violence risk assessment and debriefing methods to reduce and prevent seclusion use (Huckshorn & LeBel, 2024). Furthermore, communicating the identified information from violence risk assessment to the IP setting may improve quality reporting metrics on seclusion as there was a cumulative decrease in seclusion rates by 5% across the adult psychiatric IP units where the components of the VAT were communicated. The findings support risk assessment protocols decreasing aggressive incidents and incorporation of multimodal strategies such as debriefing with risk assessments in decreasing initial and subsequent seclusion events (Gaynes et al., 2017). There may be an opportunity to study the impact of these interventions across ED and IP settings as workplace violence reports also decreased by 17% on the adult psychiatric IP units at this practice site.
These findings should be considered in the context of limitations. Race and culture of the patients were not measured, and rates of seclusion may possibly be influenced by implicit bias (Vandamme et al., 2021). Nurse and provider experiences based on race, background, and expertise may have an impact on the consistency of the findings. Another limitation was not measuring acuity, which could potentially provide greater insight into the outlier month of November with a seclusion rate of 15.56 hr per 1,000 length of stay hours. Looking forward, educating more staff prior to implementation may increase process measures and compliance rates, and a longer project timeline may strengthen the data to further demonstrate correlations among the interventions and outcomes.
Future recommendations include integrating the VAT into the electronic health record system to improve sustainability. Integration of the debriefing tool within the organizational safety incident reporting system may help improve adherence of formal debriefing. Future research could study patient perspectives of the VAT as a patient-centered tool, proactively informing care through identifying patient-specified agitation factors and de-escalation preferences.
Conclusion
Overall, implementation of an evidence-based protocol that includes assessment of violence risk using a validated tool, identifying de-escalation and coping techniques, and postincident debriefs may reduce seclusion rates and instances of workplace violence in psychiatric EDs. Implications for practice include early identification of violence risk, patient-specific agitation factors, and de-escalation preferences in the ED setting that may have the potential to improve patient and healthcare worker safety through decreased use of seclusion and reduced workplace violence events in both the ED and IP settings.
Footnotes
Acknowledgements
The authors would like to thank our director of nursing and nursing leaders at the hospital where the data were collected for their support and for all the care team members for their efforts in improving safety and quality of care. This project has also been submitted for podium and/or poster presentations at the APNA Annual Conference, the Lowcountry Nursing Research Conference, and the National Association for Healthcare Quality Next Conference.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.