
Abstract
Background:
Workplace violence is an urgent issue for psychiatric mental health nurses. While physical workplace violence is overt, microaggressions are covert. Microaggressions are brief, daily offenses that communicate negativity. An estimated 90% of healthcare providers report experiencing microaggressions. However, evidence-based strategies and interventions for mitigating microaggressions in healthcare settings are not well established.
Aims:
The purpose of the review was to identify strategies and interventions for addressing microaggressions that are applicable to nurses.
Method:
The evidence-based literature review was conducted using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Databases included Web of Science, Embase, CINAHL, and PubMed. Published articles from 2010 to 2024 were included if they: (a) discussed strategies or interventions for reducing microaggressions and (b) included health professions students, educators, healthcare workers, or first responders in the sample. After a preliminary review, deduplication and eligibility criteria screening of 102 articles, 17 articles were included in the review.
Results:
Of the 17 articles, seven reported on communication strategies and eight on interventions. Four articles highlighted microinterventions as a strategy to address microaggressions. Seven of the eight intervention studies used a descriptive, pre/post-test design. All intervention studies targeted medicine professionals and none nurses. Most interventions effectively raised awareness and the ability to recognize microaggressions, but the effectiveness to reduce microaggressions was not measured.
Conclusions:
Findings suggest further research is needed on strategies and interventions addressing microaggressions, particularly for nurses.
Background and Significance
Instances of workplace violence (WPV), defined as “any act or threat of physical violence, harassment, intimidation, or other threatening disruptive behavior that occurs at the work site,” are rising around the world (Occupational Safety and Health Administration [OSHA], 2015). Healthcare workers are particularly vulnerable to WPV, with 81.6% reporting being verbally and physically abused in 2023 (National Nurses United [NNU], 2024). Further, psychiatric mental health (PMH) nurses report experiencing WPV at even higher levels. Approximately 65% of PMH nurses report at least one type of patient aggression within the past 12 months compared to 36% of nurses working in medical and/or surgical settings (Mento et al., 2020). The underreporting of WPV is common, with only about 20% to 60% of WPV incidents being reported (Spencer et al., 2023).
Microaggressions, a form of WPV that is more covert, are experienced by almost 90% of healthcare providers (Fisher et al., 2021), yet no research on microaggressions exists among nurses. The recent American Psychiatric Nurses Association Position Paper on Diversity, Equity and Inclusion (American Psychiatric Nurses Association, 2024) calls for researchers to investigate all instances of WPV that affect PMH nurse workforce members. To begin to answer this call, we conducted a narrative review of the literature focused on strategies and interventions for reducing microaggressions in healthcare settings that can be applied to reduce microaggressions among nurses.
The term microaggression was originally coined by Pierce and colleagues in the 1970s as “proracist behaviors. . .that are subtle, stunning, often automatic and non-verbal exchanges which are put-downs” (Pierce et al., 1977, p. 65). More recently, Fisher et al. (2021, p. 3592) defined microaggressions as “verbal, behavioral, or environmental communications that convey hostility, invalidation, or insult based on an individual’s marginalized status in society.”
Microaggressions contribute to systems of inequity, feelings of burnout, and sometimes even suicidal thoughts (Wittkower et al., 2022). Further, research has established an association between microaggressions and burnout in health professionals, especially in minoritized populations (Chisholm et al., 2021). However, the majority of research on microaggressions in healthcare involves medicine professionals and trainees but not nurses (Wittkower et al., 2022). In a review of 27 studies on recommendations and education for healthcare professionals to address patient-initiated microaggressions, none of the studies included nurses (Wittkower et al., 2022). In another review, the authors investigated interactions among healthcare professionals, trainees, and students in the clinical environment, focusing on lateral microaggressions or microaggressions between healthcare providers (Archuleta et al., 2024). We add to this knowledge base by reviewing studies on microaggressions from patients to providers that nurses can implement to reduce microaggressions.
Methods
The evidence-based, narrative literature review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Sukhera, 2022; Page et al., 2021). A narrative review provides a flexible, yet rigorous framework for the authors to analyze available research (Sukhera, 2022). The authors searched the following databases: Web of Science, Embase, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and PubMed. We used terms and Boolean operators including: “burnout* or burn out*” and “microagression*” and “training* or curriculum* or educat* or workshop* or class” or course* or intervention*.” This search yielded 57 articles. When the word nurs* was included, the search decreased to two articles. Therefore, nurs* was not an inclusion requirement. Instead, the focus shifted to what might apply to nurses. Published articles from 2010 to 2024 were included if they (a) discussed strategies or interventions targeting microaggressions and (b) included health professions students, educators, healthcare workers, or first responders in the sample. Exclusion criteria included publication prior to 2010 and any article not published in English. A similar search in Embase revealed 18 articles, two of which were duplicates and only one relevant to the literature review. With the same search terms in CINAHL, there were 17 articles, none of which included interventions. Finally, the search in PubMed resulted in four articles, two of which did not fit inclusion criteria and one duplicate article, totaling one article for inclusion. Additional articles were identified from reference list searches (see Figure 1).
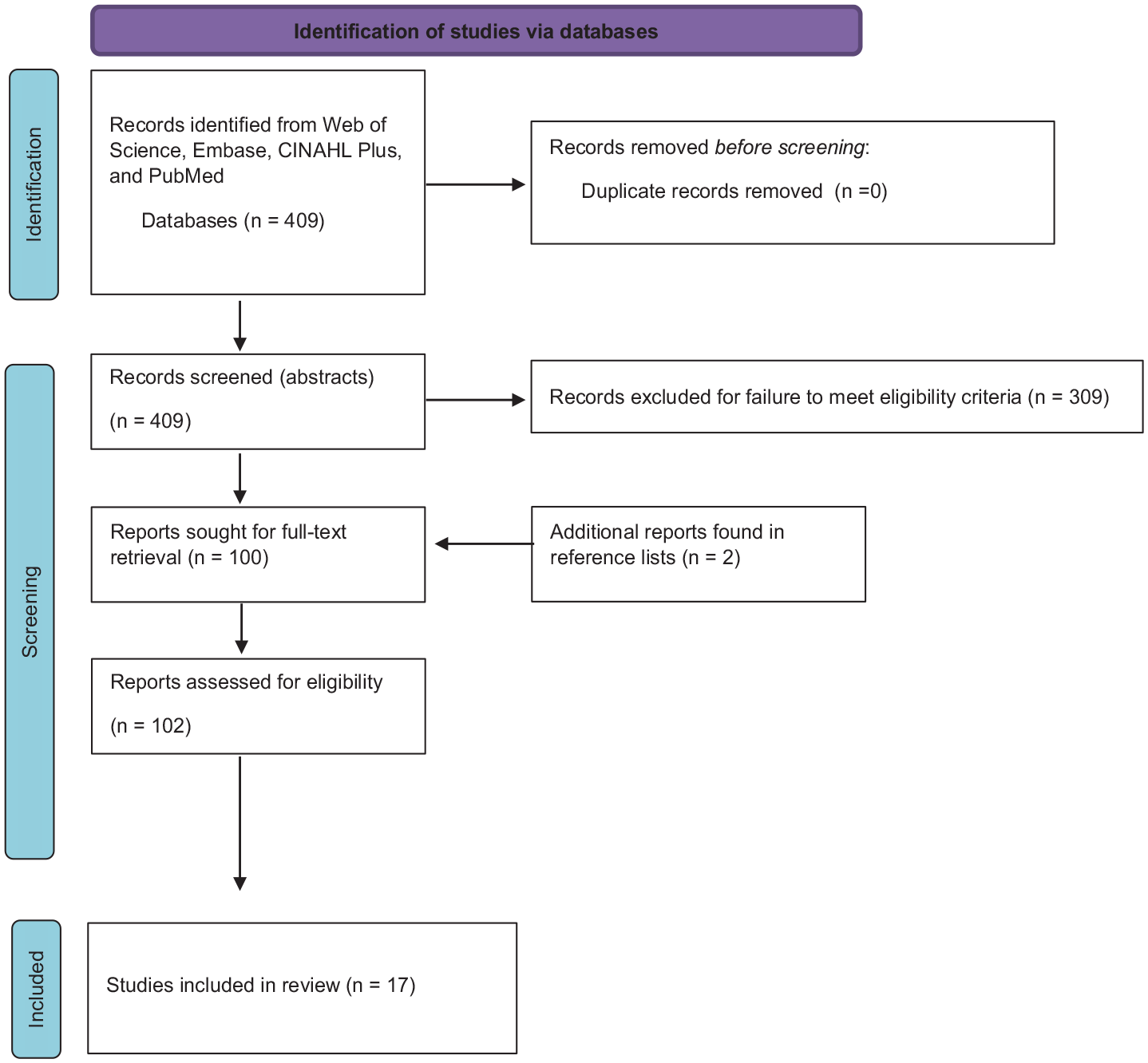
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases.
Results
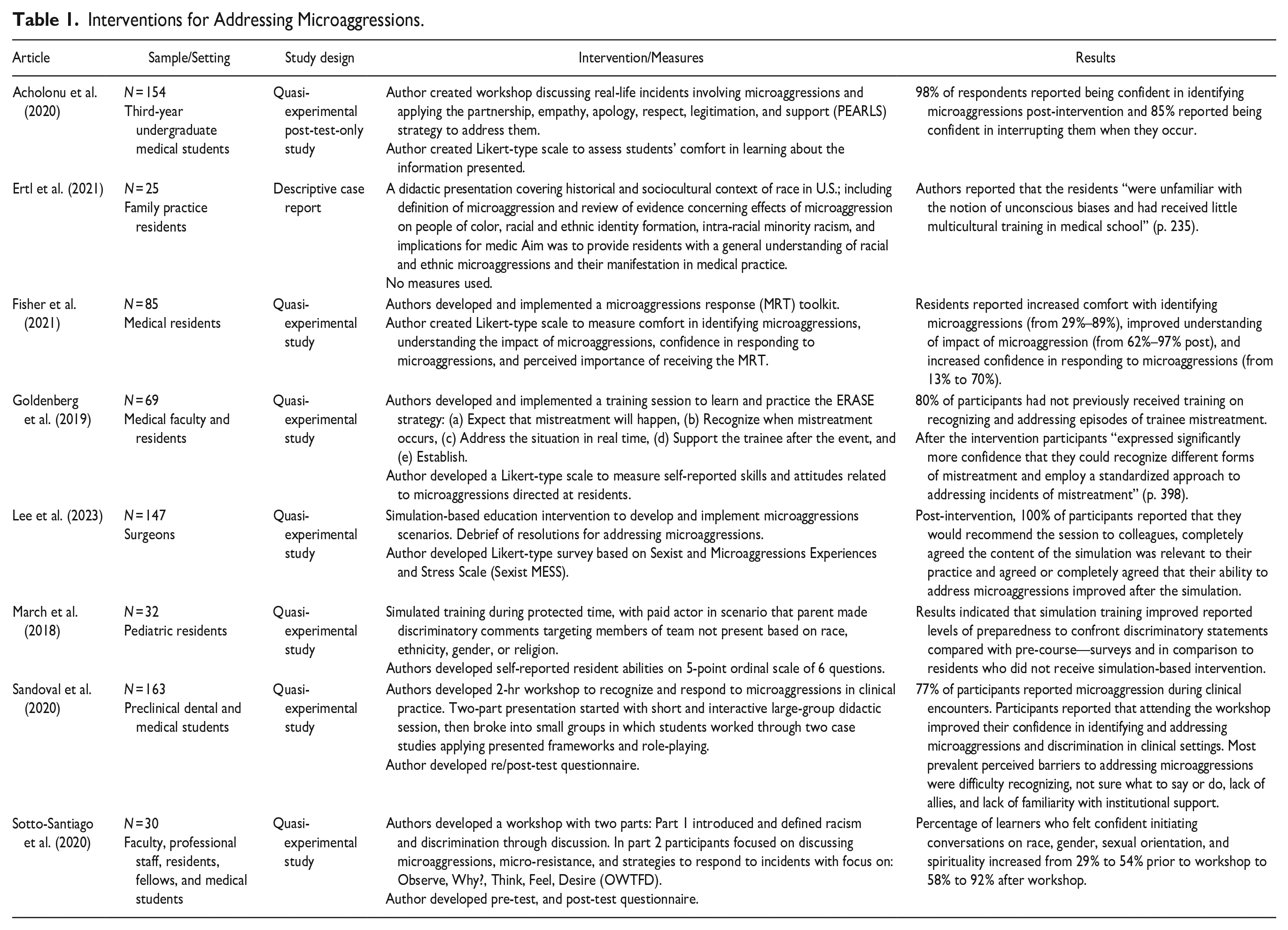
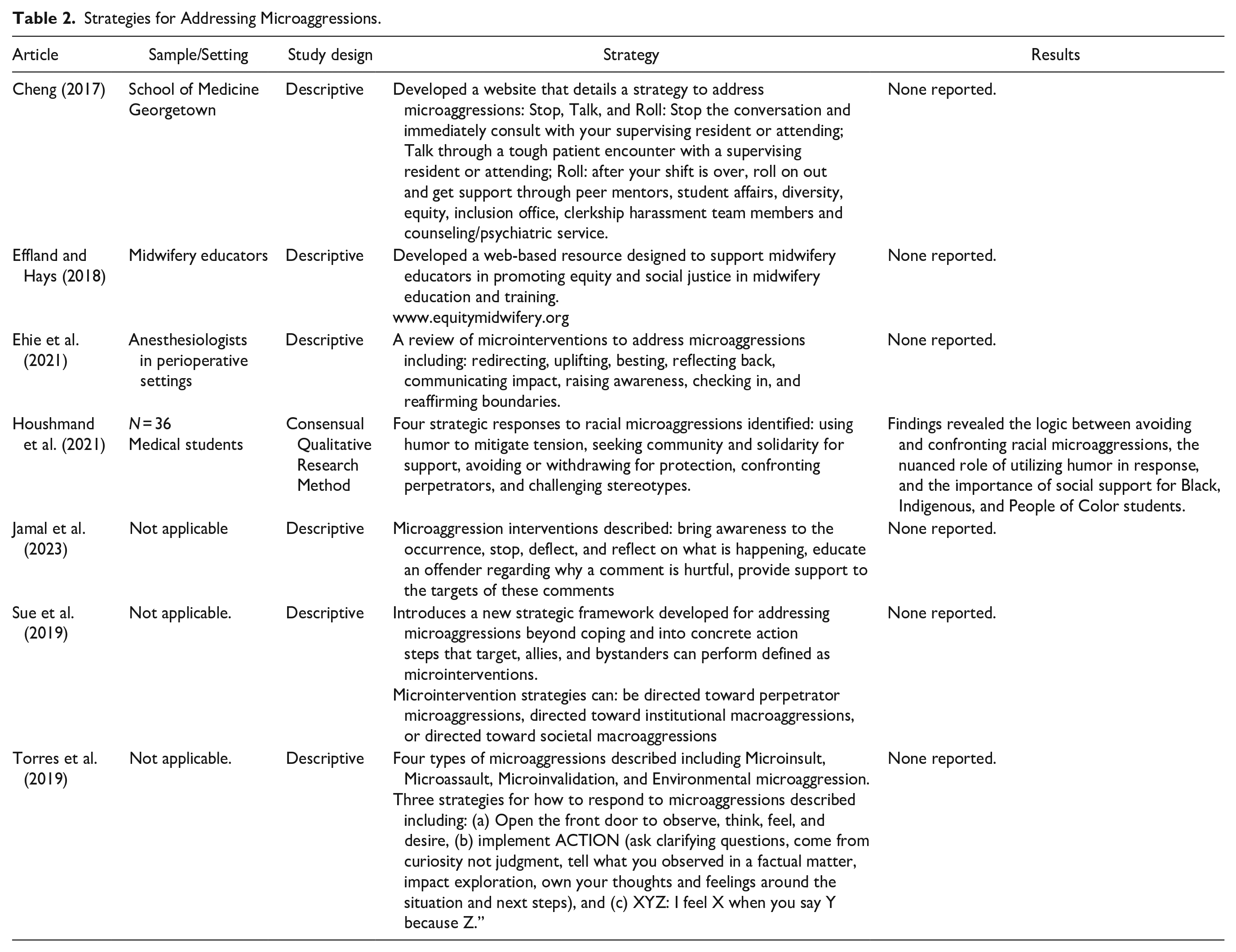
There were 102 articles reviewed for eligibility, which resulted in the inclusion of 17 articles published from 2010 to 2024 and summarized in Tables 1 and 2. The results focus on identifying, mitigating, and addressing microaggressions in healthcare. Of the 17 articles, two were reviews on microaggressions (Archuleta et al., 2024; Wittkower et al., 2022). Seven articles described strategies for explaining and addressing microaggressions (Cheng, 2017; Effland & Hays, 2018; Ehie et al., 2021; Houshmand & Spanierman, 2021; Jamal et al., 2023; Sue et al., 2019; Torres et al., 2019) and eight described interventions to mitigate and prevent microaggressions (Acholonu et al., 2020; Ertl et al., 2021; Fisher et al., 2021; Goldenberg et al., 2019; Lee et al., 2023; March et al., 2018; Sandoval et al., 2020; Sotto-Santiago et al., 2020). Of the 17 articles, none included nurses as study participants.
Interventions for Addressing Microaggressions.
Strategies for Addressing Microaggressions.
Strategies for Addressing Microaggressions
A common theme among the articles describing strategies for reducing microaggressions was the need to first acknowledge the microaggression. Specific action steps to address the microaggressions varied across the articles (Cheng, 2017; Effland & Hays, 2018; Ehie et al., 2021; Houshmand & Spanierman, 2021; Jamal et al., 2023; Sue et al., 2019; Torres et al., 2019).
Cheng (2017) developed the communication strategy “Stop, Talk and Roll.” With this strategy, the target is directed to stop the verbal conversation and immediately consult with a leader, talk through the tough encounter with a leader, and roll out to get support from program leadership or human resources. Effland and Hays (2018) created an equity-focused website that provides strategies for midwifery educators to address structural racism and microaggressions in the lives of underrepresented students. Ehie et al. (2021) reviewed existing literature on microaggressions, outlining types of microaggressions with examples, and gave examples of indirect and direct strategies to address microaggressions. They called for institutional policy and codes of conduct to include accessible ways to document microaggressions and to be clear about their frequency and approaches to address them (Ehie et al.). Torres et al. (2019, p. 869) defined four types of microaggressions: (a) microinsult (subtle, sometimes unconscious remark that demeans an aspect of the recipient’s identity. For example, a perpetrator stating someone of a certain race does not ‘look like a nurse’), (b) microassault (often conscious, discriminatory remark or behavior aimed at an individual rather than a group. For example, a perpetrator stating, “They’re letting women be executives now.”), (c) microinvalidation (often unconscious remark that invalidates the recipient’s feelings, thoughts, or experiential reality. For example, when a perpetrator claims “I do not see race,” it invalidates the individual from a minority group’s experience and leads them to question the validity of their feelings.), (d) environmental microaggression (when macro-level microaggression, microinsults, and microinvalidations are a part of the organization’s culture. For example, when all of the photos on a wall have White people as leaders and healthcare providers.). They then provided three strategies for how to respond to microaggressions: (a) open the front door (observe, think, and feel desire), (b) ACTION (ask clarifying questions, come from curiosity not judgment, tell what you observed in a factual matter, impact exploration, own your thoughts and feelings around the situation and next steps), and (c) XYZ : “I feel X when you say Y because Z” (Torres et al., 2019).
Sue et al. (2019) introduced the concept of microinterventions to combat microaggressions. A microintervention provides concrete action steps and dialogues that targets, allies, and bystanders can perform when microaggressions occur. They organized responses into four major strategic goals of microinterventions: (a) make the invisible visible, (b) disarm the microaggression, (c) educate the perpetrator, and (d) seek external reinforcement or support. The researchers also outlined the steps that witnesses of microaggressions can take to go from bystander to upstander or ally. Jamal et al. (2023) discussed the application of these microinterventions to provide psychological safety for healthcare professionals. Houshmand and Spanierman (2021) used qualitative methods to develop four microinterventions: (a) using humor to mitigate tension, (b) seeking community and solidarity for support, (c) avoiding or withdrawing for protection, and (d) confronting perpetrators and challenging stereotypes.
Interventions for Addressing Microaggressions
Of the eight intervention studies, seven used a descriptive, pre/post-test design (Acholonu et al., 2020; Fisher et al., 2021; Goldenberg et al., 2019; Lee et al., 2023; March et al., 2018; Sandoval et al., 2020; Sotto-Santiago et al., 2020) and one used a descriptive case report design (Ertl et al., 2021). All eight studies targeted medical professionals. Across the intervention studies, implementing interventions was related to improved reported awareness and ability to recognize microaggressions. However, the intervention’s effectiveness in reducing the occurrence of microaggressions was not measured.
In the one descriptive case report study, Ertl et al. (2021) presented education on microaggressions in healthcare to 25 family practice, predominantly White, medical residents in a large teaching hospital. Their education started with the historical context of racism within the medical system, at which point it became clear to the presenters that this material had not been previously covered in the participants’ medical school education. Results were only discussed from the vantage point of the presenters. The presenters noted the content of the presentation needed to be changed in real time to address the residents’ clarifying questions about systemic racism within the medical field and healthcare delivery system (Ertl et al., 2021).
Results from the remaining seven studies, which utilized pre/post-test design, revealed a significant increase in the reported knowledge on microaggressions post-intervention. However, each study measured what knowledge was gained differently. For example, Acholonu et al. (2020) utilized an intervention with 154 undergraduate medical students focused on building relationships with patients with the partnership, empathy, apology, respect, legitimation, and support (PEARLS) strategy to reduce microaggressions. After the intervention, researchers evaluated the participants’ ability to identify and interrupt microaggressions in a post-workshop survey. Ninety-eight percent of participants reported feeling confident in identifying microaggressions, and 85% reported feeling confident in interrupting when they occur.
Goldberg et al. (2019) developed a training session for medicine faculty and residents utilizing the ERASE approach to address microaggressions: (a) expect that mistreatment will happen, (b) recognize when mistreatment occurs, (c) address the situation in real time, (d) support the trainee after the event, and (e) establish a positive culture (Goldberg et al., 2019). Four one-hour sessions were delivered at various departmental meetings in an academic medical center. There were 69 total participants, including residents and faculty members from psychiatry, internal medicine, and pediatrics. Participants were asked to complete a Likert-scale questionnaire regarding their own skills and attitudes pertaining to trainee mistreatment immediately before the intervention. Then the intervention was delivered, which included a 1-hr session. Following the session, participants reflected on their skills and attitudes with the Likert-scale questionnaire again. Only about 20% of participants reported any prior training on recognizing and addressing microaggressions. Upon completion of the session, participants reported more confidence in recognizing and utilizing the standardized approach to addressing microaggressions. Fisher et al. (2021) developed the Microaggression Response Toolkit (MRT). The MRT includes strategies to respond to microaggressions as a target or a witness. The MRT was presented to 85 medical residents in a 50-min workshop that included case scenarios and role-play. In a post-workshop survey, participants reported increased comfort with identifying microaggressions (29% pre-workshop vs. 89% post-workshop), improved understanding of the impact of microaggressions (62% pre-workshop vs. 97% post-workshop), and increased confidence in responding to microaggressions (13% pre-workshop vs. 70% post-workshop).
Sotto-Santiago et al. (2020) developed a workshop to create dialogue around racism, discrimination, and microaggressions (RDM) at the Indiana University School of Medicine for institutional leaders, faculty, trainees, professional staff, and healthcare teams. The first half of the workshop introduced and defined racism with a case scenario. The second half of the workshop focused on discussing microaggressions, micro-resistance, and possible strategies to respond to these incidents, including Observe, Why?, Think, Feel, and Desire (OWTFD). Participants reported an increase in their confidence in initiating conversations related to race/ethnicity, gender identity/expression, sexual orientation, and spirituality from 29% to 54% before the workshop to 58% to 92% after the workshop.
Discussion
WPV is on the rise in healthcare and among nurses, with PMH nurses being particularly affected (Mento et al., 2020). While state laws and accreditation organizations have recently enacted mandates to combat WPV (American Nurses Association [ANA], 2021; Arnetz, 2022), current research on WPV (Marquez et al., 2020) in nursing does not explicitly address microaggressions. Therefore, we conducted a narrative review to identify the available evidence on strategies and interventions to mitigate and prevent microaggressions that apply to nurses in healthcare settings.
Previous narrative reviews focused on lateral microaggressions or microaggressions directed from one member of the healthcare team to another, whereas in this review, we also included studies focused on microaggressions directed from patients to healthcare providers. We identified only one intervention study, conducted in Britain, that involved nurses as its participants (McLaughlin et al., 2010). The study was not included in the review as it focused on verbal aggression, not specifically microaggressions.
It is imperative for nurse researchers to understand microaggressions directed at nurses, how these affect nurses, and how nurses can effectively intervene. Until more robust research with nurses is available, PMH nurses and administrators could apply strategies and interventions identified in our review in their daily practice.
The results of the review suggest that the first step in addressing microaggressions is gathering baseline data on the frequency of microaggressions. The adapted REMS could be used to gather data on nurses’ experiences of microaggressions (Chisholm et al., 2021). In the eight intervention studies, underrepresented minority students and residents reported higher levels of microaggressions than their White counterparts.
After the data on the baseline state of microaggressions are collected, PMH nurses and administrators can choose from several strategies to address microaggressions including the ERASE (Goldenberg et al., 2019), PEARLS (Acholonu et al., 2020), MRT (Fisher et al., 2021), OWTFD (Sotto-Santiago, et al., 2020) and Stop, Talk and Roll (Cheng, 2017). Common steps across these strategies include the necessity to pause or take time when the microaggression occurs, build skills to feel comfortable addressing the transgression in real time, and allow time to debrief and reflect after the encounter. Microinterventions go a step further to give instruction on how to go from bystander to upstander (Sue et al., 2019; Jamal et al., 2023).
Following the selection of a strategy to address the problem of microaggressions, PMH nurses and administrators can choose approaches to intervention implementation such as didactic learning, simulation-based learning, including role-play and small-group learning, which invites participants to share personal experiences. For example, Acholonu et al. (2020) requested the personal experiences of participants before their workshop on microaggressions. Then, the workshop consisted of an introduction, a large group discussion that included examples submitted by participants, a small-group discussion, pair role-play, and reflection (Acholonu et al., 2020). Fisher et al. (2021) used a case report and asked participants to role-play in a 50-minute workshop. Two other intervention studies employed professional actors to engage in role-play with participants (Lee et al., 2023; March et al., 2018). In these intervention studies, role-play was successfully utilized as an approach to improve recognition, mitigation, and/or prevention of future microaggressions.
Strengths and Limitations
This narrative review has several strengths and limitations. One strength of the review is that it fills an important knowledge gap by summarizing available literature on microaggressions directed from patients to providers. A limitation is that some articles might have been excluded because the search was restricted to English-language articles. Another limitation is that there is no research that included nurses, and the experiences of nurses may be unique compared to other health professionals.
Conclusion
There is an urgent need to address WPV experienced by nurses, particularly microaggressions with PMH nurses. In this review, we present systematic strategies and interventions that nurses can implement and adapt to begin to address the problem of microaggressions in nursing. Future research should focus on measuring the prevalence of microaggressions in nurses, developing rigorous intervention studies that test effectiveness for reducing microaggressions in nurses and developing validated instruments to measure microaggressions.
Footnotes
Author Contribution Statement
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.