
Abstract
BACKGROUND:
Sexual assault (SA) is a serious crime that is a prevalent mental and public health problem.
AIMS:
Addressing the needs of SA victims and providing appropriate treatment are essential to reduce potential adverse short- and long-term outcomes.
METHODS:
Our team undertook an extensive systematic literature review (published between January 2006 and July 2021) to provide evidence-based mental health intervention recommendations for adolescent and adult victims of SA. Where SA-specific research was limited, the literature and clinical practice guidelines on treatments for trauma-induced post-traumatic stress disorder (PTSD) were reviewed to provide additional information to formulate recommendations.
RESULTS:
Findings strongly support several primary psychotherapy treatments: cognitive behavioral therapy, cognitive processing therapy, eye movement desensitization and reprocessing, narrative exposure therapy, and prolonged exposure therapy. Complementary (aerobic exercise, art, drama, and music therapy) and pharmacological treatments were explored.
CONCLUSIONS:
Mental health nurses who provide services for victims of SA can utilize this overview to guide recommendations for treatment of SA trauma and related PTSD symptoms to mitigate the short- and long-term negative impacts after a traumatic event. When victims of SA receive optimal mental health treatments, our communities benefit as victims heal and recover.
Keywords
Background
Globally, one in three women will experience sexual violence in their lifetime, with wide variations in rates due to definitions, measurement tools, cultures, and reporting norms (Borumandnia et al., 2020). Sexual assault (SA) is a form of sexual violence where touching occurs without consent. Available statistics do not unveil the true prevalence of SA. Only 25% of SA victims in the United States report to law enforcement (Morgan & Ouderkerk, 2019). The World Health Organization (WHO, 2021) acknowledges that SA is vastly underreported. Tragically, sexual violence results in health, economic, and social burdens for survivors and society (Borumandnia et al., 2020; WHO, 2021). SA is prevalent in our local, national, and international communities and is a public health issue.
SA trauma can often result in many negative short- and long-term physical and psychological outcomes (Valentine et al., 2019). Increased severity and frequency of adverse cardio-respiratory, gastrointestinal, and pain symptoms are some of the common physiological responses to trauma (Pacella et al., 2013). Life-changing psychological signs can include acute stress disorder (ASD) and post-traumatic stress disorder (PTSD) symptoms: intrusion, avoidance of stimuli, negative alterations in cognitions and mood, and marked alterations in arousal and reactivity (American Psychological Association [APA], 2013). Other potential negative consequences linked to SA trauma include social adjustment, anxiety, and depression symptoms, as well as increased substance abuse, self-harm behaviors, disordered eating behaviors, and interpersonal relationship difficulties (Combs et al., 2014; Valentine et al., 2019).
Besides common PTSD symptoms, there are several other adverse outcomes: earlier onset of mental illness, physical medical conditions, role performance impairment, substance abuse, and suicidal ideation (Angelone et al., 2018; Brooker & Tocque, 2016; Carey et al., 2018; Dworkin et al., 2017; Jeon et al., 2014; Miles et al., 2020; Sachs-Ericsson et al., 2014; Santaularia et al., 2014). Several studies found an increased lifetime risk of suicide attempts in SA victims (Brooker & Tocque, 2016; Dworkin et al., 2017; Jeon et al., 2014; Miles et al., 2020). With an increased risk for suicide, SA victims should be carefully monitored for not only suicidality but struggles with mental health.
A survey of older women who were victims of SA discovered that decades after the assault, they struggled with anxiety, depression, and substance abuse symptoms throughout their lifespan (Sachs-Ericsson et al., 2014). A beneficial approach to mitigate ongoing mental health consequences following SA is to offer effective mental health treatments early to SA victims to reduce lifelong dysfunction (Miles et al., 2020).
In a review of the literature, Miles and colleagues (2020) found that women who were victims of SA or intimate partner violence were more likely to become unemployed, divorced, suffer serious illness, and fall into poverty (Byrne et al., 1999; Costa et al., 2019; Monnier et al., 2002). The impact of SA is not just exclusive to individuals but impacts our communities.
SA is a criminal offense. Investigating and prosecuting SA crimes and providing treatment and resources to SA victims are a community financial burden (Miles et al., 2020). The lifetime cost of rape in the United States is $122,462 per victim, with a $3.1 trillion economic burden (Peterson et al., 2017). Sexual violence against women costs our global economy 2% of its gross domestic product, about $1.5 trillion (Puri, 2016). SA is not just a U.S. issue but a global one.
Implementing evidence-based mental health treatments post SA is necessary to improve SA victims’ psychological and physical health. In the United States, SA victims may receive funding for mental health treatments through government crime compensation programs. The impetus for this review was a request from a state government crime compensation program for guidance on recommended evidence-based mental health treatments for SA trauma. The program receives multiple requests for varying post-SA mental health therapy options and desired an updated literature review to inform best practice recommendations and disbursement of funds for adolescent and adult SA victims. Providing funding for evidence-based mental health therapies aims to reduce individual and societal consequences and costs of SA by preventing adverse long-term psychological outcomes (Miles et al., 2020).
Objective
This systematic review aimed to evaluate evidence-based interventions to decrease psychological and functional symptoms in adolescent and adult SA victims. Regehr and colleagues (2013) completed a similar literature review, citing articles from 1991 to 2005, and found eye movement desensitization and reprocessing (EMDR), cognitive processing therapy (CPT), and prolonged exposure (PE) therapy had statistically significant reductions in PTSD and depression symptoms. This review augments Regehr et al.’s (2013) systematic review findings, which only included studies through 2005. The objective of this systematic review was to conduct a comprehensive search of treatment modalities for adolescents (>14 years of age) and adult victims of SA to provide best practice treatment recommendations for adolescent and adult SA victims. The authors included victims 14 years or older to align with the Protocol for Sexual Assault Medical Forensic Examinations: Adolescents/Adults (U.S. Department of Justice, Office on Violence Against Women, 2013).
Methods
Search Strategy
This systematic literature review was undertaken to summarize and describe research findings in detail on evidence-based mental health treatments for adolescent and adult SA victims (Miles et al., 2020). The Cochrane Handbook for Systematic Reviews of Interventions (Higgins & Thomas, 2019) guided the literature review process and structure (Miles et al., 2020).
Records from January 2006 to July 2021 were included in the search using the following search engines: CINAHL Complete, Academic Search Ultimate, PsycINFO, Med-line, Women’s Studies International, EMBASE, WoS, Cochrane, Scopus, Gender Watch, and selections from Social Science Premium Collection (Criminology Coll-ection, Education Database, ERIC, IBSS, PAIS Index, Policy File Index, Political Science Database, Worldwide Political Science Abstracts, Social Science Database, Applied Social Sciences Index and Abstracts, Sociological Abstracts, Sociology Database, Social Services Abstracts, and Sociological Abstracts). The following search terms were used: (sexual assault* “OR rape OR rapes OR” sexual violence) AND ( adolescen* OR teen* OR youth* OR adult*) AND (trauma* OR “post trauma*” OR posttrauma*) AND (treat* OR therap* OR intervention* OR emdr OR “eye movement desensitization and reprocessing” OR “eye movement desensitization and reprogramming” OR cbt OR “cognitive behavioral therapy” OR cpt OR “cognitive processing therapy” OR psychotherap* OR prolonged exposure; Miles et al., 2020). The MeSH terms compromised “Sexual Assault,” “Adolescents,” “Trauma,” and “Treatment,” including interventions such as “EMDR,” “Cognitive Behavioral Therapy,” “Cognitive Processing Therapy,” “Psychotherapy,” and “Prolonged Exposure” to explore the therapeutic approaches for individuals affected by SA.
Inclusion/Exclusion Criteria
Included studies met the following five criteria: (1) studied therapeutic interventions (including pharmacotherapy) following SA; (2) included a sample in which victims were adolescents (age 14 years or older) or adults when SA occurred; (3) included standardized measures or instruments for outcomes measuring PTSD symptoms, anxiety, depression, functioning, and so on; (4) included pre- and post-treatment comparisons; and (5) from a peer-reviewed journal in the English language (Miles et al., 2020). Preferred Reporting Items for Systematic Reviews and Meta-Analysis was utilized for our selection and review processes (Moher et al., 2009; Figure 1). Exclusion criteria included: (1) child sexual abuse; (2) participants without SA trauma; (3) below age 14 at the time of SA; (4) lack of standardized measurement tools; (5) duplicate datasets without original findings; (6) focus on policy or program interventions; (7) not available in the English language; and (8) dissertations or conference presentations.
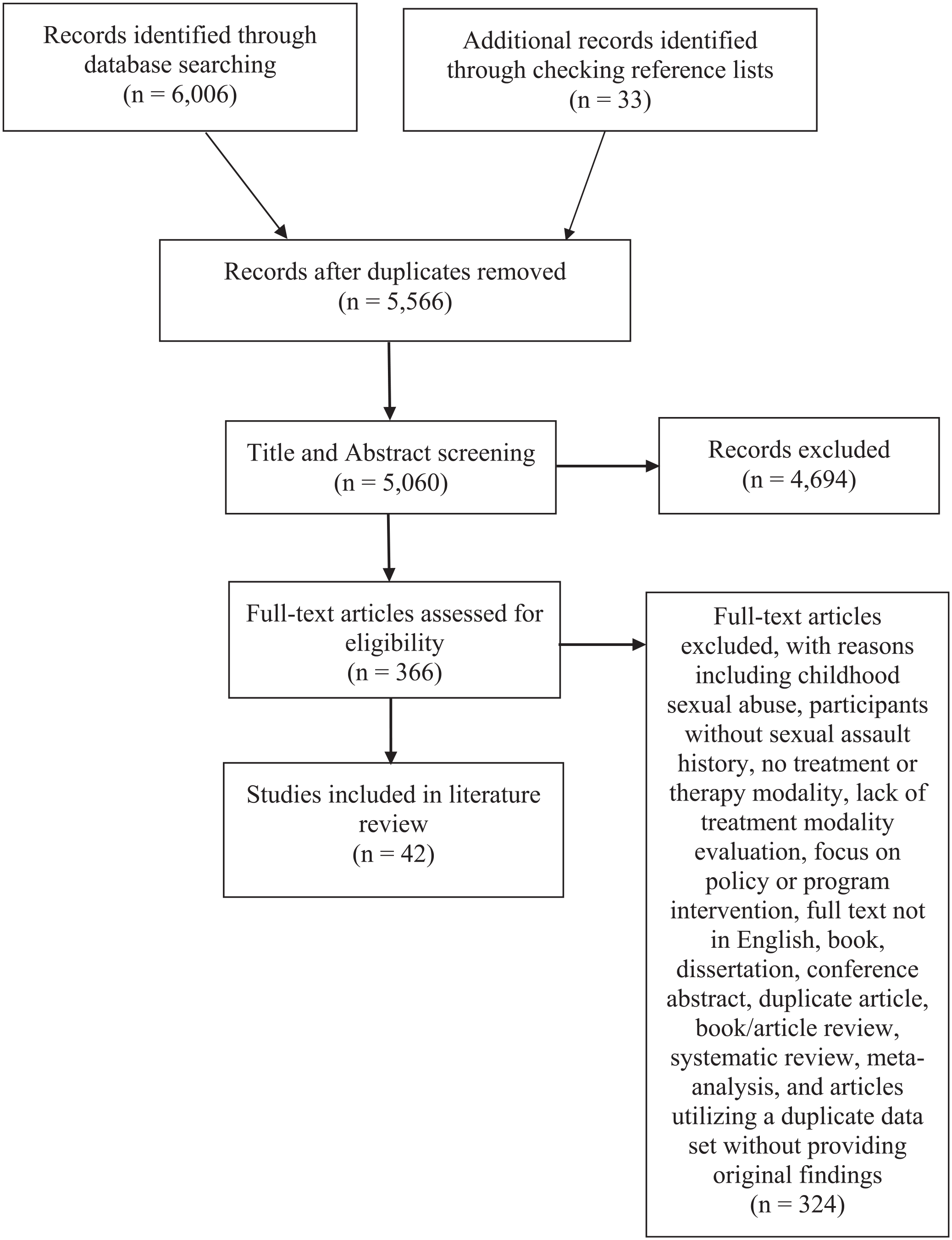
Preferred Reporting Items for Systematic Reviews and Meta-Analysis Flow Diagram
Assessment of Methodological Quality
The research team utilized the Covidence review management software to evaluate all potential research citations, titles, and abstracts retrieved from the database and manual searching to identify relevant literature. The design protocol dictated two or more team members independently evaluate each study for inclusion or exclusion in every review step, following Covidence guidelines. The full texts of all potentially relevant studies were retrieved in their entirety. Conflicts were resolved with discussion and consensus with the primary researchers. The discussion included an evaluation of methodological quality to include in the review.
Results of Literature Review
A total of 42 relevant studies were identified: 11 randomized controlled trials (RCTs), 11 quasi-experimental (QE) studies, and 20 case studies (Miles et al., 2020). See Table 1 for results of RCT and QE-reviewed studies. To align with our purpose of providing an overview of all possible treatment recommendations for SA victims, lower levels of evidence studies were included in our results. See Table 2 for a list of SA intervention studies.
Results of RCT and QE-Reviewed Studies.
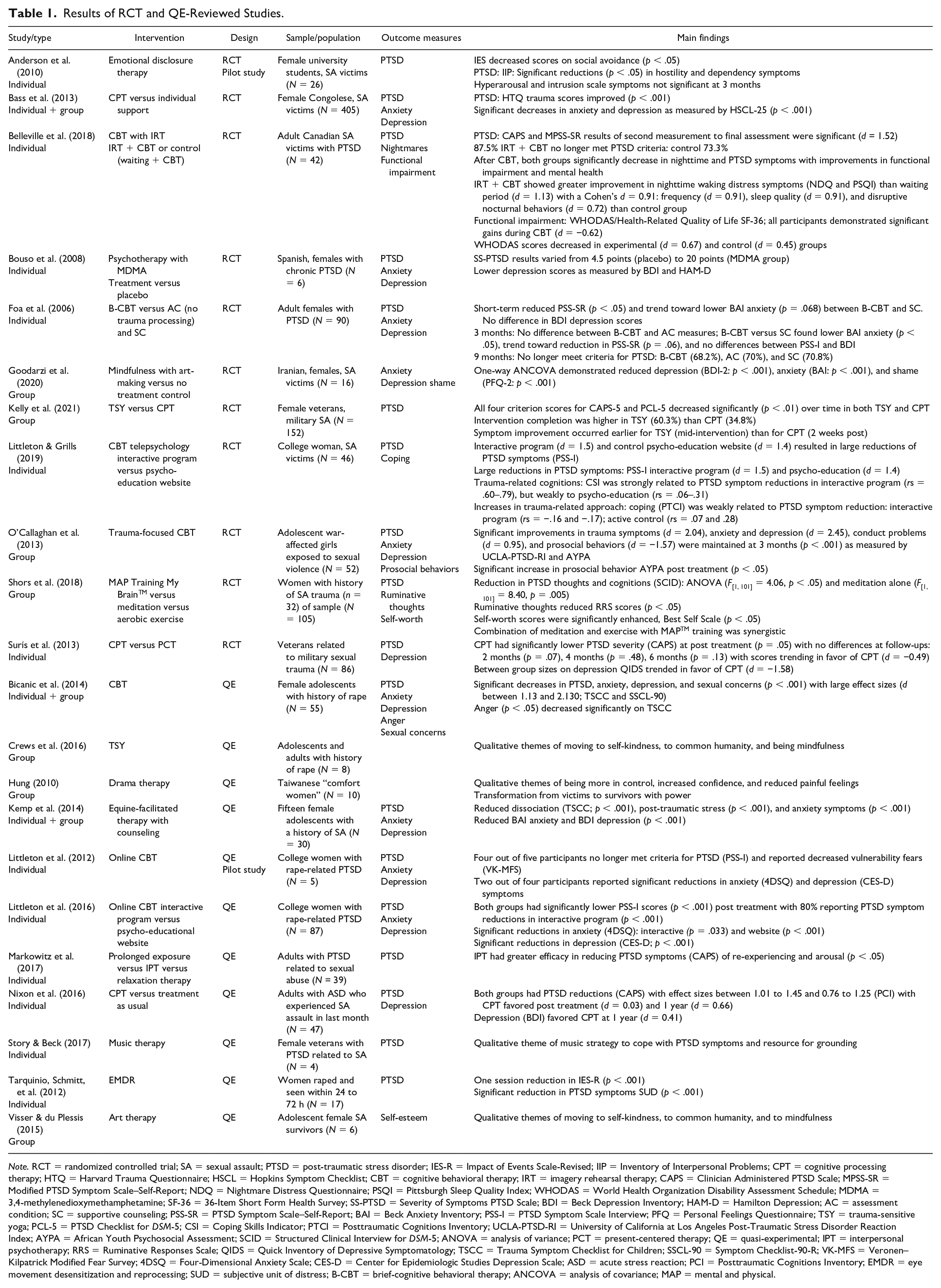
Note. RCT = randomized controlled trial; SA = sexual assault; PTSD = post-traumatic stress disorder; IES-R = Impact of Events Scale-Revised; IIP = Inventory of Interpersonal Problems; CPT = cognitive processing therapy; HTQ = Harvard Trauma Questionnaire; HSCL = Hopkins Symptom Checklist; CBT = cognitive behavioral therapy; IRT = imagery rehearsal therapy; CAPS = Clinician Administered PTSD Scale; MPSS-SR = Modified PTSD Symptom Scale–Self-Report; NDQ = Nightmare Distress Questionnaire; PSQI = Pittsburgh Sleep Quality Index; WHODAS = World Health Organization Disability Assessment Schedule; MDMA = 3,4-methylenedioxymethamphetamine; SF-36 = 36-Item Short Form Health Survey; SS-PTSD = Severity of Symptoms PTSD Scale; BDI = Beck Depression Inventory; HAM-D = Hamilton Depression; AC = assessment condition; SC = supportive counseling; PSS-SR = PTSD Symptom Scale–Self-Report; BAI = Beck Anxiety Inventory; PSS-I = PTSD Symptom Scale Interview; PFQ = Personal Feelings Questionnaire; TSY = trauma-sensitive yoga; PCL-5 = PTSD Checklist for DSM-5; CSI = Coping Skills Indicator; PTCI = Posttraumatic Cognitions Inventory; UCLA-PTSD-RI = University of California at Los Angeles Post-Traumatic Stress Disorder Reaction Index; AYPA = African Youth Psychosocial Assessment; SCID = Structured Clinical Interview for DSM-5; ANOVA = analysis of variance; PCT = present-centered therapy; QE = quasi-experimental; IPT = interpersonal psychotherapy; RRS = Ruminative Responses Scale; QIDS = Quick Inventory of Depressive Symptomatology; TSCC = Trauma Symptom Checklist for Children; SSCL-90 = Symptom Checklist-90-R; VK-MFS = Veronen–Kilpatrick Modified Fear Survey; 4DSQ = Four-Dimensional Anxiety Scale; CES-D = Center for Epidemiologic Studies Depression Scale; ASD = acute stress reaction; PCI = Posttraumatic Cognitions Inventory; EMDR = eye movement desensitization and reprocessing; SUD = subjective unit of distress; B-CBT = brief-cognitive behavioral therapy; ANCOVA = analysis of covariance; MAP = mental and physical.
Intervention Studies on Sexual Assault Trauma, Other Trauma With Recommendations.
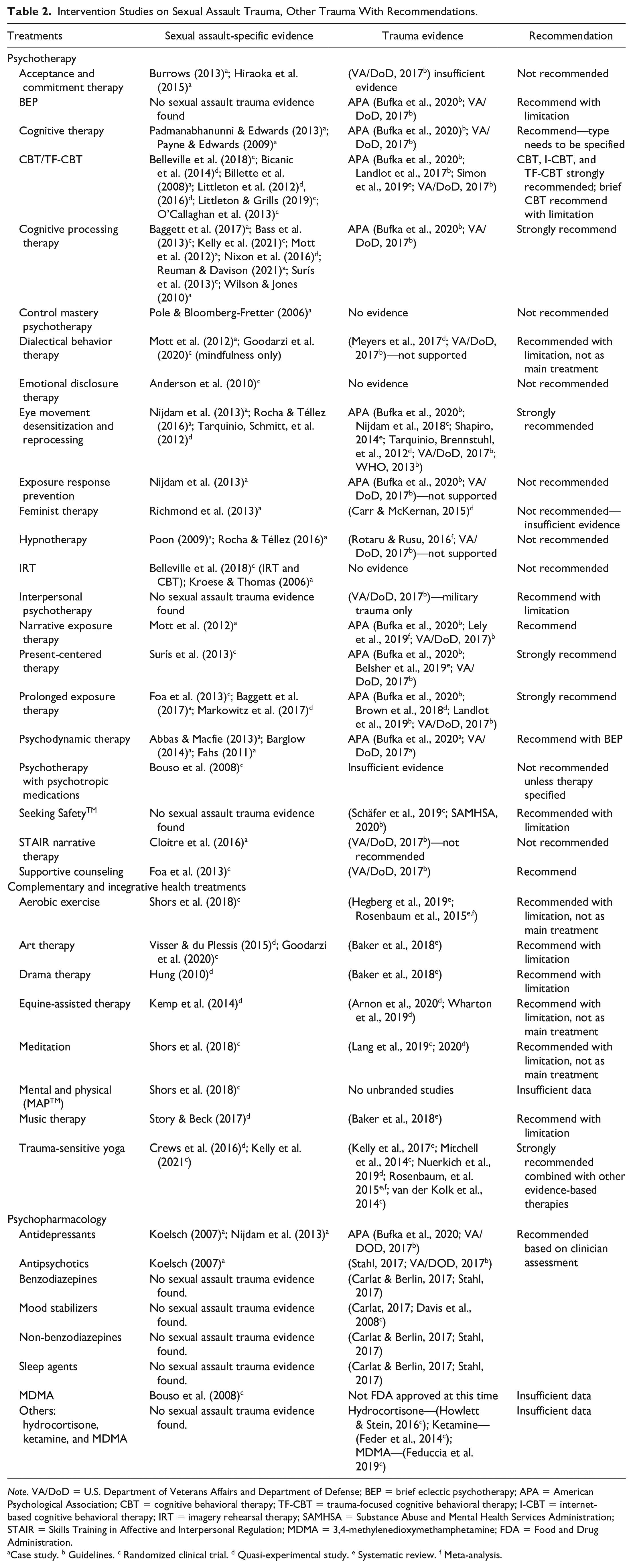
Note. VA/DoD = U.S. Department of Veterans Affairs and Department of Defense; BEP = brief eclectic psychotherapy; APA = American Psychological Association; CBT = cognitive behavioral therapy; TF-CBT = trauma-focused cognitive behavioral therapy; I-CBT = internet-based cognitive behavioral therapy; IRT = imagery rehearsal therapy; SAMHSA = Substance Abuse and Mental Health Services Administration; STAIR = Skills Training in Affective and Interpersonal Regulation; MDMA = 3,4-methylenedioxymethamphetamine; FDA = Food and Drug Administration.
Case study. b Guidelines. c Randomized clinical trial. d Quasi-experimental study. e Systematic review. f Meta-analysis.
The majority of the studies (N = 22) were conducted in the United States, with research from 14 countries (n = 20): South Africa (n = 3), Australia (n = 2), Democratic Republic of Congo (n = 2), Netherlands (n = 2), Spain (n = 2), and Canada, Denmark, France, Germany, Hong Kong, Iran, Mexico, Taiwan, and the United Kingdom each contributing one study to the body of evidence about SA treatment modalities (Miles et al., 2020).
Characteristics of Participants
Ages ranged from 14 to 90 years (N = 1,035), with a preponderance of women (97.4%) and a low representation of men (2.6%). No studies identified lesbian, gay, bisexual, transgender, or questioning (LGBTQ) subjects. There was a large representation of U.S. ethnic minorities. U.S.-based studies that delineated race indicated: Black/African American (34.92%), White (26.79%), Hispanic (10.5%) with ethic minority (9.56%). One study (n = 87) indicated most were ethnic minorities (Littleton et al., 2016). Six military veterans and four university-specific population studies were included. Adolescent population-focused studies were limited to six: two RCTs (Foa et al., 2013; O’Callaghan et al., 2013); three QE studies (Bicanic et al., 2013; Kemp et al., 2014; Visser & du Plessis, 2015); and one case study (Payne & Edwards, 2009). The time frame from SA to interventions ranged from 24 h to years.
Characteristics of Therapeutic Interventions
Therapeutic interventions were separated into three main categories: psychotherapies, complementary and integrative health (CIH), and pharmacological treatments. Psychotherapy included: acceptance and commitment therapy (ACT; two case studies), cognitive behavioral therapy (CBT; n = 7; RCT = 3; QE = 3; case study), CPT (n = 4; RCT = 3; QE = 1), control mastery psychotherapy (case study), dialectical behavioral therapy (DBT; case study), emotional disclosure therapy (EDT; n = 1, RCT = 1), exposure response prevention (ERP; case study), EMDR (n = 3; QE = 1; two case studies), feminist therapy (one case study), hypnotherapy (two case studies), imagery rehearsal therapy (IRT; n = 2; RCT = 1; case study), narrative exposure therapy (NET; case study), present-centered therapy (PCT; RCT = 1), PE therapy (n = 3; RCT = 1; QE = 1; case study), psychodynamic therapy (three case studies), Skills Training in Affective and Interpersonal Regulation
Mode of Therapy Delivery
In RCT and QE studies, therapy was provided individually (n = 12), in group (n = 7), and combined (n = 3) as their modality. Littleton and colleagues (2012, 2016; Littleton & Grills, 2019) provided individual CBT with an online interactive format. Treatments in case studies were also delivered individually. The timing, frequency, and duration of sessions varied widely across studies.
Characteristics of Outcome Measures
Reviewed studies utilized various outcomes and assessment instruments (n = 89) measuring PTSD symptoms (n = 25). Measurement tools included: anxiety and depression (n = 14), treatment evaluation (n = 8), adolescent age-specific (n = 8), intimacy and sexual satisfaction (n = 5), life quality (n = 4), past events (n = 4), social support (n = 4), self-esteem and worth (n = 2), stress perception (n = 2), and miscellaneous instruments. The variety of measurement tools made it impossible to compare results between studies (refer to Supplemental Appendix).
All RCT studies found statistically significant reductions in PTSD outcome measures. There was improvement in anxiety and depression measures (Bass et al., 2013; Bouso et al., 2008; Goodarzi et al., 2020; Nijdam et al., 2013; O’Callaghan et al., 2013; Surís et al., 2013) and functional impairments (Belleville et al., 2018). Studies that measured nightmares (Belleville et al., 2018) and shame (Belleville et al., 2018; Littleton & Grills, 2019) showed a reduction in symptoms.
Methodological Quality
The methodological quality of RCT studies was evaluated using the Center for Evidence-Based Medicine (2023) therapy study checklist and found to range from moderate to high quality (see Table 3). Randomization and comparable groups were described in all studies, with a few exceptions where it was unclear. Full blinding of therapeutic interventions was unclear. All studies had treatment and control groups for comparison. The use of assessment scales and tools made the outcome measures objective for all studies. Statistical measures of effect size were limited. Studies provided p values to demonstrate a statistical effect difference between groups and Cohen’s d values as measures of effect size between groups. Confidence intervals, which provide the magnitude of the size of the effect between groups, were provided.
Critical Appraisal of Randomized Controlled Trials.
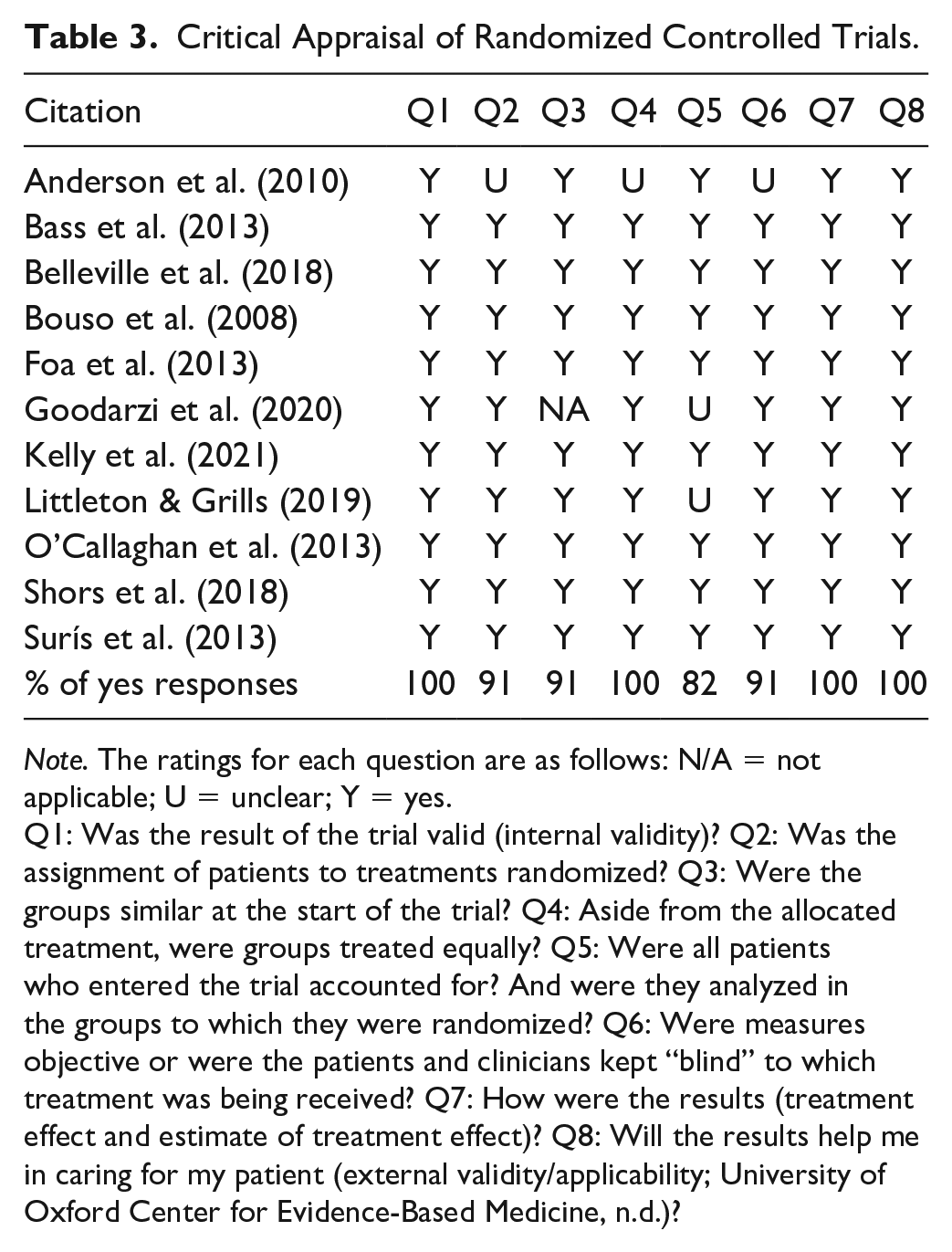
Note. The ratings for each question are as follows: N/A = not applicable; U = unclear; Y = yes.
Q1: Was the result of the trial valid (internal validity)? Q2: Was the assignment of patients to treatments randomized? Q3: Were the groups similar at the start of the trial? Q4: Aside from the allocated treatment, were groups treated equally? Q5: Were all patients who entered the trial accounted for? And were they analyzed in the groups to which they were randomized? Q6: Were measures objective or were the patients and clinicians kept “blind” to which treatment was being received? Q7: How were the results (treatment effect and estimate of treatment effect)? Q8: Will the results help me in caring for my patient (external validity/applicability; University of Oxford Center for Evidence-Based Medicine, n.d.)?
QE studies were important to include as they provided some causal evidence when RCTs were not possible, possessed a high degree of external validity, generated causal evidence on long-term outcomes of an intervention, and produced evidence faster and at a lower cost than intervention studies (Bärnighausen et al., 2017). A systematic assessment was not conducted on these lower quality studies.
Characteristics of Interventions
Our initial review (Miles et al., 2020) found 11 RCTs: EDT (Anderson et al., 2010), CPT (Bass et al., 2013; Surís et al., 2013), CBT (Belleville et al., 2018; Littleton & Grills, 2019; O’Callaghan et al., 2013), PE therapy (Foa et al., 2013), TSY (Kelly et al., 2021), art therapy (Goodarzi et al., 2020), and psychotherapy with MMDA (Bouso et al., 2008). Shors and colleagues’ (2018) study on aerobic exercise combined with meditation was the only CIH that met with inclusion criteria.
Eleven QE studies with inherently less scientific validity and more potential for bias were identified. CBT was the most frequent therapy modality in these QE studies (Bicanic et al., 2014; Littleton et al., 2012, 2016). EMDR for SA trauma treatment was studied by Tarquinio, Brennstuhl, and colleagues (2012; Tarquinio, Schmitt, et al., 2012). CPT (Nixon et al., 2016) and PE therapy (Markowitz et al., 2017) were other researched psychotherapy modalities.
Several QE studies found that paired CIH therapies can be effective but not as primary treatment for SA trauma: art therapy, drama therapy, EAT, guided imagery with music, and yoga (Crews et al., 2016; Hung, 2010; Kemp et al., 2014; Miles et al., 2020; Story & Beck, 2017; Visser & du Plessis, 2015).
While 20 case studies were included to explore the feasibility of possible treatments for SA trauma, the evidence on specific treatments was low quality (Abbas & Macfie, 2013; Baggett et al., 2017; Barglow, 2014; Billette et al., 2008; Burrows, 2013; Cloitre et al., 2016; Fahs, 2011; Hiraoka et al., 2015; Koelsch, 2007; Kroese & Thomas, 2006; Mott et al., 2012; Nijdam et al., 2013; Padmanabhanunni & Edwards, 2013; Payne & Edwards, 2009; Pole & Bloomberg-Fretter, 2006; Poon, 2009; Reuman & Davison, 2021; Richmond et al., 2013; Rocha & Téllez, 2016; Wilson & Jones, 2010). A summary of treatment recommendations for SA trauma is contained in Tables 2 and 5.
Psychotherapy
CBT in various forms was utilized in seven studies with three RCTs and three QE studies and one case study (see Tables 1 and 2). Two studies were with adolescent-specific populations (Bicanic et al., 2014; O’Callaghan et al., 2013). There were improvements in several measures in RCTs: PTSD symptoms reduction ranged from p = .06 to p < .001 with large effect sizes d = 1.13 (Belleville et al., 2018; Littleton & Grills, 2019; O’Callaghan et al., 2013); anxiety and depression (d = 2.45; O’Callaghan et al., 2013); trauma-related coping being weakly related to PTSD symptom reduction (rs = −.16; O’Callaghan et al., 2013); prosocial behavior (p < .05; O’Callaghan et al., 2013); and decrease in nightmare frequency and improved sleep quality (d = 0.91; Belleville et al., 2018; see Table 1). Significant functional improvements in quality of life were found in CBT versus control groups (Belleville et al., 2018). Two QE studies (Littleton et al., 2012, 2016) explored online CBT interventions and found statistically significant lower measures on anxiety (p < .001), depression (p < .001), and PTSD symptoms (p < .001). Bicanic and colleagues’ (2014) QE study found significant symptom decreases in anxiety, depression, PTSD, and sexual concerns with large effect sizes (d = 1.13–2.13) with significant decrease in anger (p < .05).
Three RCTs, one QE study, and several case studies (see Tables 1 and 2) utilized CPT. Reductions in PTSD symptoms post evaluations compared between groups were statistically significant (Bass et al., 2013; p > .001; Kelly et al., 2021; p < .01; Surís et al., 2013; p = .05). There was no significant difference between TSY and CPT interventions (Kelly et al., 2021). Anxiety and depression scores improved (p < .001; Bass et al., 2013) with Surís et al. (2013) demonstrating a large effect size (d = 1.58) in favor of CPT. One pilot QE study (Nixon et al., 2016) found medium effect size reductions (d = 0.66) in PTSD symptoms and small effect size (d = 0.41) with depression at 1 year.
DBT following SA was limited to only one case study (Mott et al., 2012), where CPT and PE therapy were also utilized, which confounded the true impact of DBT. Goodarzi and colleagues (2020) utilized the DBT component of mindfulness with art therapy in a small RCT group and found significant decreases in anxiety (p < .001), depression (p < .001), and shame (p < .001) symptoms.
Anderson et al.’s (2010) EDT pilot study found significant reductions (p < .05) in hostility and dependency symptoms and improved social avoidance (p < .05). Unfortunately, reductions of PTSD symptoms of hyperarousal and intrusion were not significant, and researchers concluded that EDT may be useful, but needs further study.
Only one small (n = 6) QE study (Tarquinio, Schmitt, et al., 2012) and two case studies (Nijdam et al., 2018; Rocha & Téllez, 2016) evaluated the impact of EMDR following SA trauma. Tarquinio, Schmitt, and colleagues (2012) conducted statistical analysis using Wilcoxon’s nonparametric matched pairs signed-rank test and found significant decreases between sessions in anxiety, depression, distress (9–0; scale 0–10) and PTSD symptom measures (p < .05) in their small sample size.
IRT was limited to one RCT that combined IRT with CBT and found large effect size reductions in PTSD (d = 1.52) and nightmare frequency (d = 0.91) compared to controls (Belleville et al., 2018). Additionally, there were moderate effect sizes with improvements in disruptive nocturnal behaviors (d = 0.72) and individual functioning levels in multiple domains (d = 0.67). Interestingly, functioning levels had a small effect size improvement in the control group (d = 0.45; Belleville et al., 2018). A small case study (n = 2) demonstrated reduction in trauma-related nightmares in persons with intellectual disabilities (Kroese & Thomas, 2006).
Surís et al.’s (2013) RCT compared PCT to CPT for victims of military sexual trauma and found veterans who received CPT had a significantly greater reduction in self-reported PTSD symptoms (p = .05) but not on clinician assessment measures. Pre- and post-treatment effect sizes were moderate to large (d = 0.30–1.02) and trended in favor of CPT on two PTSD (d = −0.49) and depression (d = −1.58) measures (Surís et al., 2013).
Foa and colleagues’ (2013) RCT study compared PE therapy to supportive counseling (SC) and found significant reductions in PTSD diagnosis rates (p = .01) with over 78% losing PTSD diagnosis (p<.01), improved depression rates (p = .008), and greater functional improvement (74.3%) compared to SC (65.5%: p = .008). Markowitz and colleagues’ (2017) QE study compared PE therapy to interpersonal therapy (IPT) and relaxation therapy and found that PE therapy produced less positive outcomes in PTSD symptoms, except for avoidance symptoms. One case study combined CPT, PE therapy with senate focus therapy and demonstrated positive outcomes for the patient (Baggett et al., 2017).
The following case studies explored various psychotherapies yielding insufficient evidence: ACT (Burrows, 2013; Hiraoka et al., 2015), cognitive therapy (CT)—unspecified (Padmanabhanunni & Edwards, 2013; Payne & Edwards, 2009), control mastery therapy (Pole & Bloomberg-Fretter, 2006), ERP ( Nijdam et al., 2013), feminist therapy (Richmond et al., 2013), hypnotherapy (Poon, 2009; Rocha & Téllez, 2016), NET (Mott et al., 2012), psychodynamic psychotherapy (Abbas & Macfie, 2013; Barglow, 2014; Fahs, 2011), and STAIR narrative therapy (Cloitre et al., 2016).
Complementary Interventions
Several complementary modalities were utilized with SA trauma victims with five RCT studies. Shors and colleagues (2018) compared mental and physical (MAPTM) with aerobic exercise and meditation and found reductions in PTSD thoughts (p < .05) and ruminative thoughts (p < .05), and enhanced self-worth (p < .05). They concluded that combining the modalities had a positive synergistic effect. Art therapy combined with mindfulness yielded significant decreases in measures of anxiety, depression, and shame (p < .001; Goodarzi et al., 2020). A QE study with adolescents found improved positive self-esteem and interpersonal closeness (Visser & du Plessis, 2015). Kemp et al.’s (2014) QE adolescent study evaluated EAT with adolescents and found reduced anxiety (p < .001, effect size .798), depression (p < .001, effect size .784), and externalized behaviors (p < .001, effect size .698).
Kelly and colleagues’ (2021) RCT compared TSY to CPT and found a higher completion rate with TSY (60%) compared to CPT (34.8%) with symptom improvement occurring earlier with TSY (mid-intervention) than CPT (2 weeks post). In addition, two PTSD measures decreased significantly (p < .01) in both groups (Kelly et al., 2021). A QE adolescent-focused TSY group study found increased self-esteem components (Crews et al., 2016).
There were several QE studies with positive outcomes: drama therapy (Hung, 2010), EAT (Kemp et al., 2014), and music therapy (Story & Beck, 2017).
Pharmacological Interventions
Limited studies were found on pharmacological interventions for SA trauma. Only one small RCT (n = 6) combined psychotherapy with MDMA (3,4-methylenedioxymethamphetamine), and found lower depression scores and PTSD severity (Bouso et al., 2008). The use of MMDA with psychotherapy lacked strong evidence to support it as the study suddenly ended. There were low-quality case studies that utilized antidepressants (Koelsch, 2007; Nijdam et al., 2013) and antipsychotics (Koelsch, 2007).
Discussion
The negative physical and psychological impacts of SA are well-documented for adolescents and adults. If SA victims receive evidence-based therapeutic treatment, the data indicate that many long-term adverse mental and physical health outcomes can be reduced, and individuals can experience healing from their trauma. The objective of this systematic review was to evaluate the research and clinical guidelines on methods to reduce the morbidity associated with SA trauma. This review found many psychotherapies, CIH, and pharmacological treatments that can effectively reduce the negative sequelae from SA trauma. Although therapeutic guidelines specific for SA victims have not been established, this review is the first step in providing strategies for SA trauma treatment.
Consideration should also be given to therapies in the early stages of development that have shown some promise in preliminary studies. As Neukirch and colleagues (2019) have noted, additional treatments will be developed and refined as our knowledge expands regarding the effects of trauma on the brain and body. Although many therapies lack strong evidence to recommend, one must remember that individuals are unique, and several treatment modalities, even combined ones, may benefit victims.
Inclusion of PTSD Treatment Evidence
Evidence on PTSD treatments was included in this review because of its prominence as a negative consequence of SA. Dworkin and colleagues (2023) found that 1 week following SA, 81% of survivors experienced symptoms of ASD, a precursor to PTSD. One month later, when PTSD can be diagnosed, 75% met the Diagnostic and Statistical Manual criteria for PTSD (APA, 2013). The majority of SA survivors experience PTSD symptoms (Dworkin et al., 2023), with 41% still meeting PTSD criteria 1 year after SA (Dworkin et al., 2017). The inclusion of systematically developed PTSD clinical practice guidelines enhances our development of recommendations to assist practitioners and patient decisions about their care.
The U.S. Department of Veterans Affairs and Dep-artment of Defense (VA/DoD, 2017) Clinical Practice Guidelines for Management of PTSD and ASD analyzed different types of therapies and recommended the following: strongest evidence PE therapy, CPT, and EMDR; sufficient evidence CBT, brief eclectic psychotherapy (BEP), NET, and narrative exposure—written. The VA/DoD (2017) guidelines found that trauma-focused psychotherapies positively impact core PTSD symptoms more than pharmacotherapies. If victims voiced a preference for treatment not focused on their trauma, the VA/DoD (2017) recommended individualized psychotherapy, including stress inoculation training, PCT, and IPT.
Clinical practice guidelines for adult PTSD symptoms from APA strongly recommend psychotherapy, CBT, CPT, CT, PE therapy, and antidepressants and conditionally recommend BEP, EMDR, and NET (Bufka et al., 2020). The APA found insufficient evidence to support Seeking SafetyTM (Bufka et al., 2020)
Recommendations
In the United States, the best-practices protocol for SA medical forensic examinations combines adolescents (14 years and older) with adult victims (US Department of Justice, Office on Violence Against Women, 2013). Mental health practitioners should evaluate the developmental levels of their patients and their sexual trauma history to determine which mental health therapies would be appropriate. The recommendations in this review are for adolescents and adults who experienced SA after the age of 14 years and not for past childhood sexual abuse.
SA-specific trauma treatment recommendations merge findings from this systematic review with the VA/DoD (2017) and APA clinical practice guidelines (Bufka et al., 2020) along with relevant PTSD studies in Table 3. The authors developed recommendation criteria to categorize treatment modalities: strongly recommend, recommend with limitations, and not recommended at this time due to insufficient evidence for the main treatment (Table 4). These recommendations can serve as a guide for informing nurses, health care providers, and SA victims about evidence-based trauma treatment options (see Table 5). Notably, therapeutic approaches to treating SA trauma can vary widely between adolescents and adults due to differences in developmental stages, cognitive capacities, emotional needs, communication style, and family involvement. These treatment recommendations should not supersede a mental health nurse’s judgment to customize individual treatment.
Criteria for Recommendation Levels for Therapies.
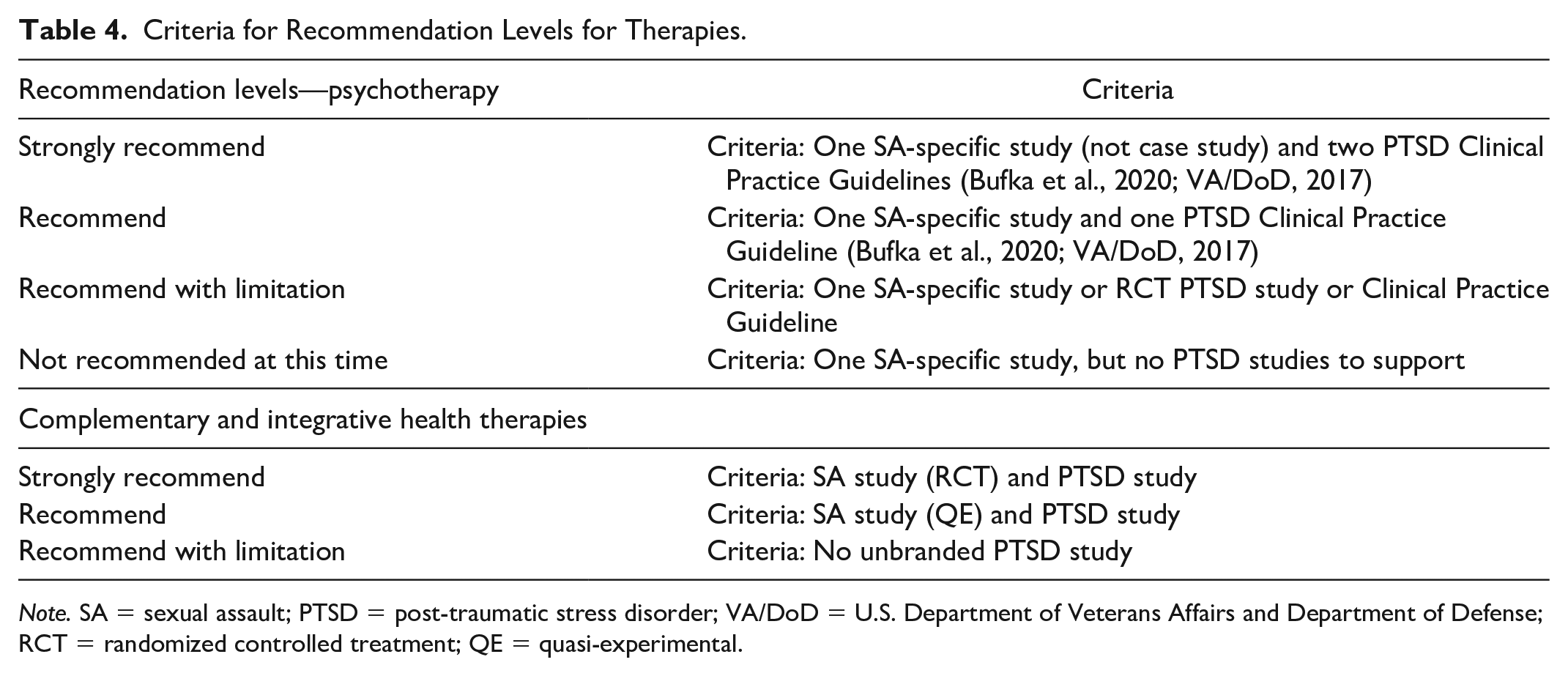
Note. SA = sexual assault; PTSD = post-traumatic stress disorder; VA/DoD = U.S. Department of Veterans Affairs and Department of Defense; RCT = randomized controlled treatment; QE = quasi-experimental.
Summary of Recommendations for Psychotherapy and Complementary Therapies Post Sexual Assault.
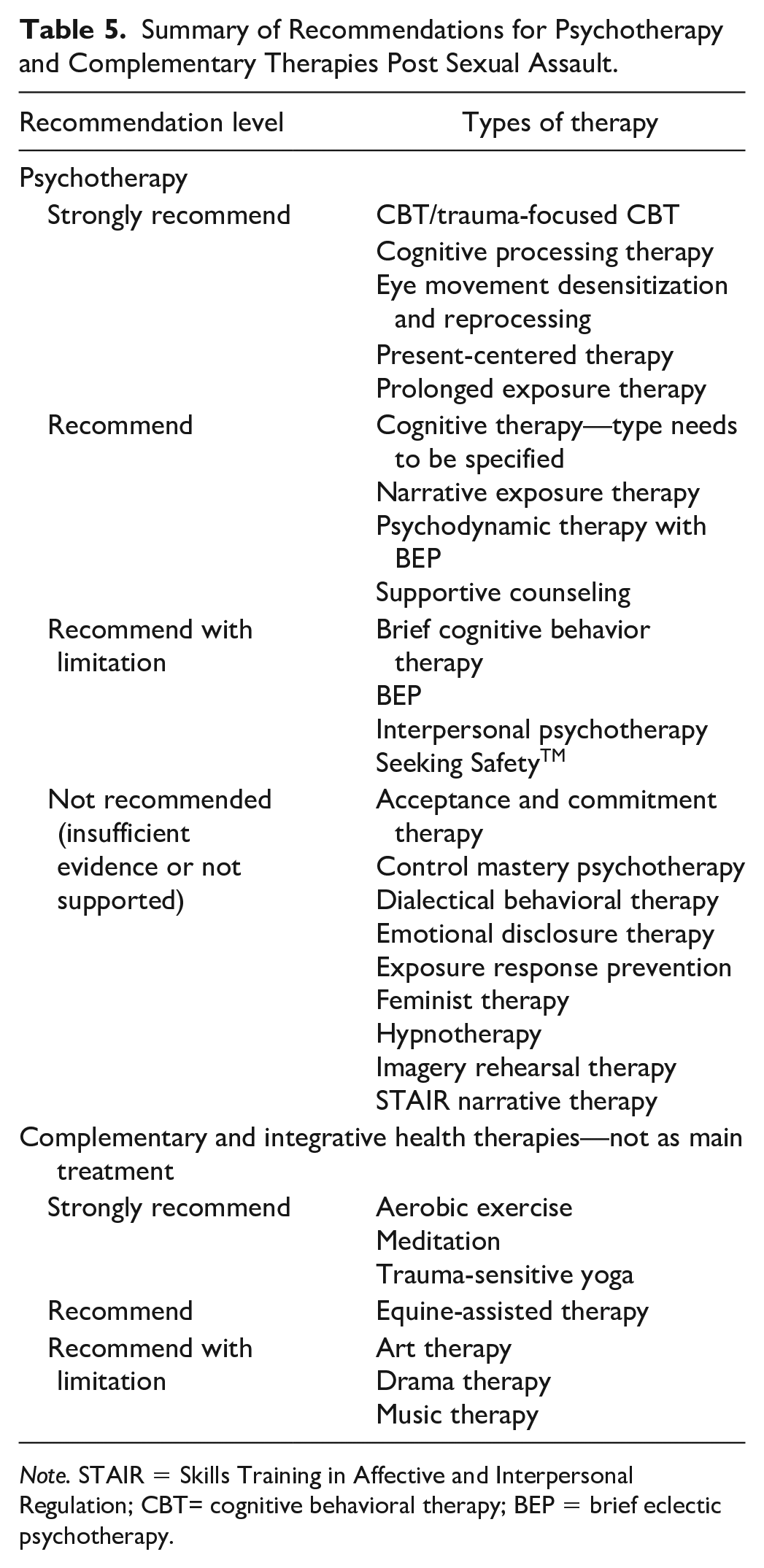
Note. STAIR = Skills Training in Affective and Interpersonal Regulation; CBT= cognitive behavioral therapy; BEP = brief eclectic psychotherapy.
Psychotherapy Options (Listed Alphabetically)
Psychotherapy is the well-respected gold standard for treating trauma (Bufka et al., 2020). There were a wide variety of long-standing and newer methodologies utilized and reviewed. Generally, psychotherapy performed better than control groups in addressing ASD and PTSD.
ACT uniquely utilizes behavioral commitments with a blend of acceptance and mindfulness strategies to target PTSD symptoms. The authors of this review found only two case studies (Burrows, 2013; Hiraoka et al., 2015) on ACT. The VA/DoD (2017) review found insufficient evidence for ACT as a trauma-specific treatment. ACT could be an option if a victim is unable to tolerate other evidence-based therapies (not recommended at this time).
This review found no BEP studies for SA victims. BEP for PTSD combines CBT with a psychodynamic approach that focuses on changing specific shame and guilt emotions. The APA (Bufka et al., 2020) and VA/DoD (2017) support BEP as an evidence-based treatment modality for PTSD trauma. Even though no studies utilized BEP with SA victims, there is still significant evidence to recommend with limitations for PTSD symptoms.
CBT: Brief-CBT (B-CBT), Internet-Based CBT (I-CBT), and Trauma-Focused CBT (TF-CBT)
CBT therapy focuses on recognizing dysfunctional beliefs and thoughts, followed by the cognitive actions of challenging and replacing them with more realistic thoughts or ideas that result in behavioral change. Seven studies from this review supported CBT in adolescent and adult victims of SA with lowered anxiety, depression, and PTSD symptoms and improved functional and social impairments (see Tables 1 and 2). CBT is a standard recommended trauma treatment to improve daily functioning in adults (WHO, 2013). For adolescents with PTSD, Landolt et al.’s (2017) clinical guidelines found substantial evidence to support CBT.
Littleton and Grills (2019) utilized a telepsychology-interactive program and psycho-education online TF-CBT that significantly reduced PTSD symptoms, demonstrating that therapy does not have to be in person. A systematic review of I-CBT RCTs found this PTSD therapy modality was acceptable for anyone over age 16 (Simon et al., 2019). However, Simon and colleagues (2019) found no difference in dropout rates between I-CBT and other non-CBT treatments but a greater dropout rate from I-CBT compared to waitlist persons not receiving treatment. B-CBT was not studied with SA victims. The VA/DoD (2017) and APA (Bufka et al., 2020) recommended cognitive behavioral therapies, but did not specifically review B-CBT, resulting in limited evidence to recommend.
TF-CBT is a respected first-line trauma treatment and a researched therapy for adolescents. Numerous RCTs have demonstrated that TF-CBT effectively reduces symptoms of anxiety, depression, dissociation, PTSD, sexual dysfunction, and feelings of shame from the SA (Landolt et al., 2017). In summary, CBT, I-CBT, and TF-CBT are strongly recommended, but B-CBT is recommended with limitation.
Cognitive Processing Therapy
Similar to CBT, CPT focuses on cognitive strategies to alter erroneous thinking. Two RCTs (Kelly et al., 2021; Surís et al., 2013) and several case studies (Table 2) utilized CPT and found the interventions reduced PTSD symptoms related to SA at post-evaluations. The VA/DoD (2017) guidelines noted that the strongest evidence supporting CPT as a PTSD treatment. Across racially diverse populations and in telehealth, CPT has solid empirical support (Bufka et al., 2020). CPT is strongly recommended.
Control Mastery Therapy
Pole and Bloomberg-Fretter’s (2006) case study utilized this integrative form of psychotherapy that combined cognitive, humanistic, and psychodynamic therapy into treatment for SA (insufficient data—not recommended at this time).
Dialectical Behavioral Therapy
DBT is CBT for compl-ex disorders focusing on emotion regulation, distress tolerance, and mindfulness (Dimeff & Linehan, 2001). Although positive outcomes were demonstrated with the use of one of the components of DBT, mindfulness (Goodarzi et al., 2020), not using full DBT was combined is a major limitation. DBT was combined with PE in persons (n=22) with borderline personality disorder, including suicidal ideation Meyers et al. (2017). The researchers found moderate effect size reductions in PTSD symptoms and suicidal ideation. Citing a lack of sufficient evidence, the VA/DoD (2017) did not endorse DBT as a primary treatment (not recommended at this time as main treatment).
Emotional Disclosure Therapy
EDT is a type of psychotherapy in which emotions are expressed in a therapeutic environment to regulate emotions. Anderson et al.’s (2010) lacked sufficient evidence to recommend EDT for SA victims to reduce PTSD symptoms. A review of the literature did not discover any other studies examining EDT with PTSD or trauma (not recommended at this time).
Eye movement Desensitization and Reprocessing
EMDR is one of two therapy approaches endorsed by the WHO (2013) for PTSD treatment in adults and adolescents. Therapy reduces the emotional impact of trauma-based symptoms by simultaneously visualizing the traumatic event while concentrating on external stimuli (Bufka et al., 2020; VADoD, 2017). Three SA-specific lower evidence quality studies were evaluated in this review (Nijdam et al., 2018; Rocha & Téllez, 2016; Tarquinio, Schmitt, et al., 2012). Tarquinio, Brennstuhl, and colleagues (2012) investigated the use of EMDR with SA victims shortly following a SA (24–72 h). They found decreased intrusive and avoidance symptoms, indicators of PTSD, as well as a reduction in anxiety and depression. PTSD symptoms following EMDR treatment were reduced by 84% to 100% in those with single incident trauma after 5 h of treatment (Shapiro, 2014). Tarquinio, Brennstuhl, et al. (2012) went further to recommend EMDR as part of an emergency room protocol for SA victims. Nijdam et al.’s (2018) RCT reported reduced PTSD symptoms and improved post-traumatic growth. Even though EMDR had limited SA-specific trauma studies, the across-the-board endorsement from the VA/DoD (2017) and APA guidelines (Bufka et al., 2020) leads the authors to strongly recommend.
Exposure Response Prevention
ERP is an intensive form of behavior therapy where specific techniques are utilized to help clients refrain from undesired behaviors. A single case study combining EMDR and ERP with antidepressant treatment had low results on several measures (Nijdam et al., 2013). Rauch and Rothbaum (2016) suggested that ERP and exposure-based therapies could be considered for PTSD for individuals who do not wish to participate in evidence-based treatments. ERP was not endorsed by the APA (Bufka et al., 2020) and VA/ DoD (2017) guidelines (not recommended at this time).
Feminist Therapy
Female empowerment is an essential component of feminist therapy. A single case study of a female SA victim explored the use of feminist therapy treatment to reduce depression and anxiety symptoms (Richmond et al., 2013). In a unique approach, Carr and McKernan (2015) adapted feminist theory, combined with CPT and PE therapy, to address men’s barriers (masculinity and mental illness stigma) in treating PTSD symptoms in veterans. They concluded that the inclusion of feminist therapy improved engagement in therapeutic processes. Integrating feminist strategies into psychotherapy could meet individuals’ needs as they process their trauma (not recommended at this time for main treatment).
Hypnotherapy
Studies on the use of hypnotherapy to decrease PTSD and trauma symptoms were limited to two case studies (Poon, 2009; Rocha & Téllez, 2016). While these results were positive, there was low supporting PTSD treatment evidence, resulting in the VA/DoD (2017) conclusion not to support. A small meta-analysis (Rotaru & Rusu, 2016) combined hypnosis with other therapies found hypnotherapy could be additionally helpful in mitigating PTSD symptoms (not recommended at this time as main treatment due to insufficient evidence).
Image Rehearsal Therapy
This short-term CBT therapy focuses on reducing nightmares by instructing individuals to write about nightmares and edit them to more positive images. IRT studies are limited to Belleville et al.’s (2018) study that combined IRT with CBT, which confounded findings specific to IRT. Women with learning disabilities were included in two small case studies that demonstrated IRT could be effective with significant reductions in stress related to trauma-related nightmares (Kroese & Thomas, 2006). APA (Bufka et al., 2020) and VA/DoD (2017) did not evaluate IRT (not recommended at this time for reducing PTSD symptoms), but could be beneficial to reduce trauma-related nightmares.
Interpersonal Psychotherapy
Interpersonal interactions with others, including exploring current and past experiences with their antecedent thoughts and resulting behaviors, are the focus of IPT. No studies were found on treating SA trauma. VA/DoD (2017) recommended IPT for PTSD treatment in veterans (recommend with limitations as only studied in military trauma).
Narrative Exposure Therapy
NET is a form of psychotherapy utilized for multiple or complex traumas in which individuals tell their stories and challenge their perceptions. APA clinical guidelines (Bufka et al., 2020) state that NET is an evidence-based intervention for PTSD in adolescents and young adults. Likewise, VA/DoD (2017) recommended NET to treat trauma and PTSD. Lely and colleagues (2019) undertook a meta-analysis of NET and found NET outperformed comparative treatments and improved PTSD and depression symptoms. Mott et al.’s (2012) study was the only SA-specific case study that utilized NET. Even though there are no RCT or QE studies with SA victims, there is strong evidence for PTSD trauma treatment (Recommend).
Present-Centered Therapy
PCT focuses on increasing adaptive coping skills to life stressors and difficulties related to trauma or PTSD symptoms. Surís et al.’s (2013) study and VA/DoD (2017) recommended PCT in combination with other therapies. APA recommends a PCT focus at the beginning of CBT sessions (Bufka et al., 2020). A recent Cochrane review found moderate-quality evidence that PCT effectively reduced PTSD severity compared to controls (Belsher et al., 2019). PCT was not as effective for reducing PTSD symptoms severity as TF-CBT, but PCT had a lower dropout rate (Belsher et al., 2019). When TF-CBT is not available, PCT is a treatment option (strongly recommend).
PE Therapy
PE therapy is a form of CBT, a brief treatment where individuals relive their traumatic experiences by describing them aloud, listening to the recording, and confronting triggers to habituate to the event to decrease anxiety, fear, and other distressing emotions. Landolt et al.’s (2017) clinical guidelines recommended PE therapy for adolescents. A study specific to adolescents who received PE therapy reported reduced PTSD and depression symptoms with improved functioning (Foa et al., 2013). Brown et al. (2018) found a transactional relationship between PTSD and depression where a reduction in one symptom cluster resulted in a decrease in the other with PE therapy. Markowitz and colleagues (2017) included, but did not separate in their analysis, SA victims from those who experienced other types of trauma, limiting conclusions about the effectiveness of PE in the SA victim population. Support in the literature for PE for adults with PTSD is extensive. Many studies have demonstrated that symptoms of PTSD, depression, anger, guilt, and anxiety, as well as improved social function, can extend to at least 10 years past the completion of treatment (Bufka et al., 2020; VADoD, 2017; strongly recommend).
Psychodynamic Psychotherapy
This form of psychotherapy focuses on dealing with unconscious forces and self-understanding. Although initially promising, case studies published by Abbas and Macfie (2013), Barglow (2014), and Fahs (2011) provided a low level of evidence to support psychodynamic psychotherapy for trauma and PTSD. APA clinical guidelines (Bufka et al., 2020) support psychodynamic psychotherapy as part of BEP but not as a stand-alone therapy approach. The VA/DoD (2017) review agreed with this conclusion (strongly recommend with BEP).
Psychotherapy Unspecified With Psychotropic Medications
Many types of psychotherapy treat dysfunctional behavioral and thinking patterns and emotional reactions. Two psychotherapy case studies examined combining psychotherapy with pharmacological therapy: MMDA, antidepressant, and antipsychotic medications (Bouso et al., 2008; Koelsch, 2007). However, neither of these case studies indicated what type of psychotherapies were utilized (therapy needs to be specified to recommend).
Seeking SafetyTM
Seeking SafetyTM is a manualized treatment for individuals with substance abuse in addition to trauma and PTSD. This review found no studies specific to SA victims utilizing this treatment approach. Schäfer and colleagues’ (2019) meta-analysis of Seeking SafetyTM found decreased PTSD symptoms (medium effect size) and substance abuse (modest effect size) with treatment. APA found insufficient evidence to support this treatment (Bufka et al., 2020). Seeking SafetyTM for persons with substance abuse issues with comorbid PTSD and trauma is supported by the Substance Abuse and Mental Health Services Administration (2020; recommend with limitations).
STAIR Narrative Therapy
STAIR combines skills training with narrative therapy to address trauma symptoms. This review found one small study of SA victims (n = 3) demonstrating improved PTSD symptoms but provided low-quality evidence of effectiveness (Cloitre et al., 2016). The VA/DoD (2017) review did not recommend STAIR based on insufficient data (
Supportive Counseling
This modality relies on the therapeutic alliance with the therapist to improve emotional well-being and functional capacity without probing into the source of stress. Many studies utilized this approach as a comparison group. Although response to PE therapy was more robust, SC was effective to reduce PTSD and depression symptoms as well as improve global functioning (Foa et al., 2013). The VA/DoD (2017) concluded that counseling was not as effective as a stand-alone treatment for PTSD and trauma, although a supportive relationship is fundamental to the success of any therapy endeavor (recommend with limitations).
Adolescent Population Specifics
TF-CBT adolescent-specific findings mirrored adult measurements of reduction in anxiety, depression, and PTSD symptoms with a reduction in conduct problems and an increase in prosocial behaviors (O’Callaghan et al., 2013). In addition, a reduction in anger and sexual concerns was found (Bicanic et al., 2013). PE therapy findings in the adolescent population were similar with decreased depression and PTSD symptoms in the adult population (Foa et al., 2013; Markowitz et al., 2017). This underscores the efficacy of both TF-CBT and PE therapy in addressing psychological challenges in adolescents, suggesting promising avenues for therapeutic interventions in this population.
Complementary Treatments as Adjunctive Options
Complementary treatments include many modalities, such as mindfulness and physical therapies. Although many are safe and may be helpful adjunctively in the treatment of PTSD, none have demonstrated by research to be a primary treatment for PTSD (Rosenbaum et al., 2015; Wahbeh et al., 2014). The VA/DoD (2017) also found the majority of complementary treatments had insufficient evidence to recommend them as primary treatments for PTSD.
Aerobic Exercise
Physical activity, typically prolonged and moderate intensity, strengthens the cardiovascular and respiratory systems and decreases anxiety and depression (Shors et al., 2018). Shors and colleagues (2018) compared MAPTM training, which combines specific mental training with meditation and exercise, to meditation plus exercise groups with SA victims. Exercise or meditation alone was not effective in reducing trauma-related cognitions and ruminations, but MAPTM training with meditation and exercise was effective. A systematic review and meta-analysis undertaken by Rosenbaum et al. (2015) found that aerobic exercise, physical activity, and trauma-informed yoga were more efficacious than treatment-as-usual in improving depressive and PTSD symptoms. Hegberg and colleagues’ (2019) literature review (n = 19) found that aerobic exercise as a primary treatment or adjunctive may reduce PTSD symptoms.
Smith-Marek and colleagues’ (2018) qualitative study with focus group discussions and interviews (n = 8) with SA victims found exercise choices were impacted by the recovery stage of the individual. Further studies are needed to determine the most effective strategies for implementing these therapies. Currently, evidence supports aerobic exercise as adjunctive treatment in combination with best-practice PTSD treatments (strongly recommend).
Art, Drama, and Music Therapy
Art, drama, and music therapies utilize artistic modalities to increase self-awareness and self-expression. Visser and du Plessis’ (2015) art therapy (n = 6), Hung’s (2010) drama therapy (n = 10), and Story and Beck’s (2017) music therapy with guided imagery studies (n = 4) were too small to derive sufficient evidence to support their use as a primary treatment for PTSD. An interesting study by Goodarzi et al. (2020) combined mindfulness with art therapy principles (n = 16) and found reductions in anxiety, depression, and shame. However, further research with a larger pool of participants is necessary to validate the effectiveness of this approach. Creative art therapies were examined in a systematic review by Baker et al. (2018). The researchers concluded that the trials evaluated were of poor quality (recommend with limitation).
Equine-Assisted Therapy
EAT is a pet therapy utilized to enhance an individual’s cognitive, emotional, physical, and social functioning. Kemp and colleagues’ (2014) lower quality adolescent QE study was the only specific study for SA victims. EAT with veterans was investigated by Arnon et al. (2020) and was found to provide short-term reductions in PTSD symptoms and improve quality of life while eliciting high participant satisfaction. Wharton and colleagues (2019) utilized a manualized approach combining EAT with CPT in men veterans with PTSD (n = 27) and demonstrated that PTSD and trauma-related symptoms improved significantly. There is a lack of sufficient research to support EAT as a primary treatment modality, although there has been a high degree of interest in this approach. EAT may be helpful for those more interested in non-traditional therapy and as an adjunct to evidence-based treatment (recommend).
Meditation/MAPTM
Meditation or self-contemplation has been successfully utilized in various forms, including combined with aerobic exercise (Shors et al., 2018), yoga (Crews et al., 2016; Kelly et al., 2018, 2021; Lang et al., 2019, 2020; Mitchell et al., 2014; Neukirch et al., 2019; van der Kolk et al., 2014; Wahbeh et al., 2014), and music therapy (Story & Beck, 2017).
Compassion meditation (CM) focuses on cultivating compassion toward self and others. Lang et al. (2020) found CM reduced PTSD symptoms. Researchers developed a manualized group training, cognitively based compassion training (CBCT®), that reduced depression and PTSD symptoms in two veteran populations (Lang et al., 2019, 2020). Although the VA/DoD (2017) and APA (Bufka et al., 2020) did not review, other PTSD studies support (strongly recommend).
Yoga and TSY
Yoga is purported to improve participants’ well-being by increasing tolerance for the sensory and physical experiences accompanying helplessness and fear, as well as raising emotional awareness and affect tolerance (Kelly et al., 2018; Quiñones et al., 2015; van der Kolk et al., 2014). Crews et al.’s (2016) qualitative study found that TSY was an effective healing modality for SA adolescent survivors. van der Kolk and colleagues’ (2014) investigation of women with chronic PTSD (n = 64) utilizing TSY found that 52% of the yoga intervention group no longer met PTSD criteria, compared to 21% of the control group. Relapse was also more prevalent in the control group. A larger RCT study (n = 152) found a significant decrease in PTSD symptoms and higher retention rates than CPT with sustained positive effects in women veterans (Kelly et al., 2018).
In a small mixed methods case series examining the effects of TSY on the psychological sequela of sexual trauma, Neukirch et al. (2019) found TSY decreased PTSD, anxiety, depression, and stress symptoms while increasing interoceptive awareness. Davis et al. (2020) undertook an RCT comparing holistic yoga to a wellness lifestyle program. Davis et al.’s study did not utilize TSY, which could have influenced the re-emergence of symptoms at 7 months to follow-up, despite initial improvement. In a Kripalu-based yoga RCT investigation with women, Mitchell et al. (2014) found decreases in both re-experiencing and hyperarousal symptoms, with small to moderate between group effect sizes. These results support TSY as an effective adjunct for PTSD treatment in combination with evidence-based standard treatments (strongly recommend).
Adolescent Population Specifics
Art therapy (Visser & du Plessis, 2015), EAT (Kemp et al., 2014), and TSY (Crews et al., 2016) were studied in this population, underscoring the need to utilize other therapeutic modalities than just psychotherapy to address the unique needs of developing adolescents to heal from their trauma.
Pharmacological Therapies
PTSD symptoms can be treated by several psychotropic medication classes, including antianxiety medications, mood stabilizers, antidepressants, atypical antipsychotics, and others (Stahl, 2017). Only three studies utilized medications to treat SA trauma in this review specifically: antidepressants (Koelsch, 2007; Nijdam et al., 2018), atypical antipsychotics (Koelsch, 2007), and mood stabilizers (Davis et al., 2008).
Because of the lack of psychopharmacology studies specific to SA trauma, the literature was reviewed for medication studies for PTSD symptoms related to trauma. The VA/DoD (2017) concluded that gains from psychotherapy are more long lasting than those from medications. A systematic review and meta-analyses of trauma-focused psychotherapy versus pharmacotherapy found that trauma-focused psychotherapy was more effective as a first-line treatment (Lee et al., 2016). A common treatment plan for PTSD symptoms is a combination of therapy with psychotropic medications to alleviate PTSD symptoms (Berlin, 2017).
One small RCT with SA victims utilized MDMA, a synthetic mood and perception-altering drug, in combination with exposure therapy that had improved PTSD symptoms (Bouso et al., 2008). Positive results from a study using MDMA with exposure therapy conducted by Mithoefer et al. (2013) led to the U.S. Food and Drug Administration giving MDMA a breakthrough therapy designation for trauma treatment (Feduccia et al., 2019).
To treat depression symptoms from trauma, Feder et al.’s (2014) study (n = 14) utilized ketamine to treat depression and PTSD symptoms. They found a rapid reduction in symptoms without the persistence of dissociative symptoms. Howlett and Stein (2016) explored using hydrocortisone administration immediately after a traumatic event to reduce PTSD symptoms with some favorable preliminary results. While MDMA, ketamine, and hydrocortisone treatment for PTSD might hold promise in the future, other psychotropic agents can be helpful, based on years of experience of demonstrated effectiveness in treating mental health symptoms. MDMA, ketamine, and hydrocortisone are not recommended at this time due to insufficient data. Psychotropic medications are recommended based on clinician assessment of symptom benefit.
The expertise of mental health practitioners, with input from trauma survivors and evidence-based practice, should inform the decisions on therapeutic modalities for SA victims. As each victim has a distinctive background and trauma history, practitioners should thoroughly evaluate and optimize the most effective treatment for that individual. These guidelines are not meant to prescribe a one-size-fits-all approach; rather, they are intended to synthesize current research and practice recommendations addressing SA trauma.
Limitations
There are several limitations in this review. The authors did not compare effect sizes between studies. Effect estimates were not calculated for individual studies, though some studies did include effect estimates in their analyses. Studies and clinical guidelines were also not compared against each other regarding their respective quality of evidence due to the wide variety of assessment tools and outcome scales utilized (see Supplemental Appendix). A limitation of this review is that some studies possibly contained SA victims under age 14 although the majority of victims were 14 years or older. These studies were included because the authors felt that the studies added more knowledge about SA treatment. An important limitation to the generalizability of findings is the inclusion of QE studies and case studies to supplement RCTs.
Unfortunately, the majority of studies on the effects of SA trauma primarily include white heterosexual women participants, indicating substantial gaps in research on men, minorities, and LGBTQ populations. The SA of men is a pervasive problem, yet men might be less likely than women victims to report rape and seek help (Miles et al., 2020). The lower rates of males reporting SA and seeking treatment may be associated with sociocultural norms related to men’s sexuality and self-identity (Valentine et al., 2019). Additional studies on men SA victims are needed. Even though women are at a 10 times higher risk of being raped compared to men, the PTSD risk post SA is higher for men compared to women (65% vs 46%; Mithoefer et al., 2013).
While many studies reported racial demographics, few explored treatment implications related to gender identity and cultural or racial issues. No studies were found specific to the LGBTQ population, thus a limitation of this review is the generalizability of findings to other populations because of the low representation of men, minorities, and LGBTQ victims.
Despite these limitations, this literature review specific for SA victims and synthesis with evidence-based trauma research contributes to our knowledge about effective treatments for SA trauma. Given the increase in sexual violence in our communities, the small number of high-quality SA-specific treatment studies is distressing. In an effort to provide some treatment recommendations, PTSD clinical practice guidelines were utilized, which may confound our recommendations. We strongly propose a call for high-quality clinical studies with rigorous designs that explicitly focus on evidence-based trauma interventions for SA victims.
Conclusion
The impetus for this literature review was a request from a U.S. state government crime compensation program for guidance on recommended evidence-based treatments for SA trauma in adolescent and adult victims because they lacked the resources to undertake a literature review. Providing adequate government and private funding for evidence-based treatments for SA victims is of the utmost importance for recovery. Evidence-based therapeutic interventions for adolescent and adult SA victims should be a priority in our communities to promote individual recovery, reduce societal burdens, and improve public health (Miles et al., 2020). Mental health nurses, funding stakeholders, SA survivor services, and SA victims should be informed of available treatment options to guide funding, practice, and individual decisions. Evidence-based therapeutic interventions for SA victims can positively impact healing and recovery, leading to healthier individuals, families, and communities.
Supplemental Material
sj-pdf-1-jap-10.1177_10783903231216138 – Supplemental material for A Systematic Review of Evidence-Based Treatments for Adolescent and Adult Sexual Assault Victims
Supplemental material, sj-pdf-1-jap-10.1177_10783903231216138 for A Systematic Review of Evidence-Based Treatments for Adolescent and Adult Sexual Assault Victims by Leslie W. Miles, Julie L. Valentine, Linda J. Mabey, Elizabeth S. Hopkins, Paige J. Stodtmeister, Reilly B. Rockwood and Alyssa N. H. Moxley in Journal of the American Psychiatric Nurses Association
Footnotes
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The College of Nursing at Brigham Young University in Provo, Utah, supported our research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.