
Abstract
BACKGROUND:
Adults with severe mental illnesses have mortality rates 2.5 to 3 times higher than the general population, largely due to medical illnesses. Those with the most profound mental illnesses are served by assertive community treatment (ACT) teams that provide intensive mental health care; however, there are no clearly established models to integrate physical health treatment into ACT and this is a critical gap in the literature.
AIMS:
To describe perceptions of ACT team members regarding services provided for their clients to treat physical health, how those services can be improved, and what implementation strategies would likely be needed to promote uptake and sustainability of those services on ACT teams.
METHOD:
Qualitative interviews were conducted via Zoom using a semistructured interview guide with 19 employees from three ACT teams in a southeastern state. Interview transcripts were analyzed, using manifest content analysis, a form of qualitative analysis, to identify key themes in the interview transcripts.
RESULTS:
ACT team members described limited physical health services for their clients. They reported (1) system-level barriers to improving physical health care, such as inadequate tools and training; and (2) patient-level barriers, such as limited awareness of physical care needs. ACT team members reported the need for additional medical staff and strengthened relationships with primary care providers. They also recommended changes in policy, education, and quality monitoring to implement new physical health care services.
CONCLUSIONS:
Findings suggest intervention components and implementation strategies for improving physical health care of ACT consumers.
Introduction
Approximately 11.2 million adults in the United States (4.5%) suffer from severe mental illness (SMI) (National Institute of Mental Health, 2019), which is defined as a mental, emotional, or behavioral disorder causing severe functional limitations that limit or substantially interfere with one or more major life activities (National Institute of Mental Health, 2019). Having SMI is associated with an increased risk of also having chronic medical conditions that are exacerbated by health risks that complicate the course of these chronic illnesses (Bahorik et al., 2017; Brown et al., 2010). For example, diabetes, dyslipidemia, hypertension, and obesity are 1.5 to 2 times more prevalent in those with SMI than in the general population (Mangurian et al., 2018; Newcomer & Hennekens, 2007; Scott & Happell, 2011). Moreover, these illnesses and risk factors contribute to developing cardiovascular disease (CVD), which, among persons with SMI, is associated with a two- to threefold greater risk for death than adults without SMI (Laursen, 2011).
Patients with SMI also experience several factors that reduce the effectiveness of services to detect and treat physical health problems. They receive fragmented primary care and access more limited health care services (Williams et al., 2019). They also receive preventative health care at a lower rate than the general population (McKibbin et al., 2014). Several factors contribute to these differences in physical health care access and utilization, including lower socioeconomic status (i.e., resources to pay for health care), transportation availability, and poor executive functioning (McKibbin et al., 2014).
Assertive community treatment (ACT) has emerged as a treatment modality with great potential to address the physical health needs in this population (Vanderlip et al., 2014; Vanderlip et al., 2017). ACT is one of the most widely studied evidence-based practices for individuals living with SMI and has clear eligibility criteria and fidelity metrics (Bond & Drake, 2015; NC Division of Medical Assistance [NCDMA], 2016). The definition and scope of ACT services vary by state but share many core components. In North Carolina, for example, ACT eligibility is defined as (1) the presence of a serious mental illness, such as schizophrenia, bipolar disorder, or major depression; (2) significant functional impairment, such as inability to maintain housing or employment; and (3) evidence of continuous high-service needs, such as increased use of acute psychiatric hospital (two or more admissions during the past year) or recent criminal justice involvement (NCDMA, 2016). Research demonstrates that ACT teams improve psychiatric outcomes for SMI clients, including housing stability and reduced hospitalizations; moderate improvements in subjective quality of life and psychiatric symptoms have also been found (Bond et al., 2001; Burns & Santos,1995; Phillips et al., 2001; Vanderlip et al., 2017).
Service definitions of ACT also require teams to address the physical health of individuals enrolled. The NC Department of Health and Human Services currently requires that ACT teams provide health education, counseling, medical screenings, coordination of medical and dental appointments, and assistance with transportation to appointments (NCDMA, 2016). Nurses are often expected to provide these services and their preparation for these roles can vary widely. For example, nursing roles on the ACT team in NC can be filled by registered nurses (RNs) or advance practice registered nurses (APRNs; NCDMA, 2016). Licensed practical nurses can also fill the nursing role on teams with more than one nurse, if there is a full-time RN or APRN in a nursing role on the team (NCDMA, 2016).
Recent studies also suggest that ACT services have the potential to improve physical health outcomes (e.g., hypertension) (Vanderlip et al., 2014; Vanderlip et al., 2017); however, models for integrating physical health care services on ACT teams have not been established (Henwood et al., 2018). Moreover, it is not yet known how community-based nurses and other staff monitor and help ACT consumers manage serious health conditions, such as heart failure and chronic obstructive pulmonary disease, or how they enable participation in primary and specialty medical care to control these chronic conditions. Thus, research is needed to explore opportunities and approaches to implementing physical health interventions within ACT programs; more information is needed about how physical health care services are currently provided by ACT, and the perceptions of ACT team members on how new physical health services could be added should be explored. The primary objective of this exploratory, qualitative study was to characterize the perceptions of ACT team members and administrators on providing ACT services related to physical health care of ACT consumers. The secondary objective was to describe implementation strategies needed to integrate evidence-based physical health services within ACT.
Method
Design
A descriptive qualitative study design was used to describe ACT team member perceptions of services and strategies that team members used to promote the physical health of ACT clients and the strategies to implement new physical health care services into routine practice (Hsieh & Shannon, 2005; Miles & Huberman, 1994). Approval for the study was obtained from the institutional review board (IRB) at the University of North Carolina at Chapel Hill.
Setting
Staff members of three ACT teams in a large southeastern state participated in the study. Local teams known to the lead investigator were invited to participate in the study. All of the teams met the following criteria: (1) location in the state where the study was conducted; (2) acceptable fidelity to the ACT model as evidenced by a score of 3.0 or higher on the Tool for Measurement of Assertive Community Treatment (Monroe-DeVita et al., 2011) in the most recent state evaluation; and (3) operation of the ACT team for at least 1 year, thereby ensuring time to be established in their respective communities (as determined by verbal report of ACT Team administrators). The exclusion criterion was ACT teams that served fewer than 25 clients.
In this exploratory study, a convenience sample of four ACT teams was recruited to participate in the study. The primary investigator (PI) approached team leaders on four ACT teams to discuss participating in the research. Leaders on three ACT teams agreed to participate. These included one large ACT team (more than 75 clients) and two small teams (less than 50 clients). After an agreement letter for team participation was completed for each site, the PI attended meetings via Zoom with each team to explain the study and provide a flyer for ACT employees to contact the PI and schedule interviews on an individual basis. An informed consent procedure was performed before each interview that included information about participation being completely voluntary as well as the subject’s right to withdraw consent at any time.
Sample and Procedures
The population from which participants in the qualitative interviews were selected was the group of staff working in the three participating ACT teams. The inclusion criteria were at least 1-year experience working in mental health and at least 3 months on the current ACT team. The rationale for these inclusion criteria was to ensure that participants involved in physical health care services were represented across teams. To recruit ACT team members, the PI used IRB-approved procedures, which included a presentation of the study purpose and procedures to ACT team members and an invitation to team members to send an email to the PI if they were interested in participating. On receipt of email, the PI screened potential participants for inclusion. The research was completed during the COVID-19 pandemic and face-to-face visits with study participants were not possible; thus, the PI used a telephone-based, IRB-approved, recruitment procedure to explain the study and obtain verbal consent for study participation.
A total of 19 employees from three ACT teams were recruited for participation. Interviews took place between July 19 and August 6, 2020. The sample included four nurses, one psychiatrist, two administrative staff, one peer-support specialist, three team leaders, and eight social workers. The sample was mostly female (79%, n = 15) and mostly White (84%, n = 16). On average, participants had been working on their ACT teams for 4.28 years (SD = 4.2). Owing to COVID-19 and risk mitigation strategies, face-to-face interviews were not possible. They were conducted via Zoom, digitally recorded, and professionally transcribed.
Measures
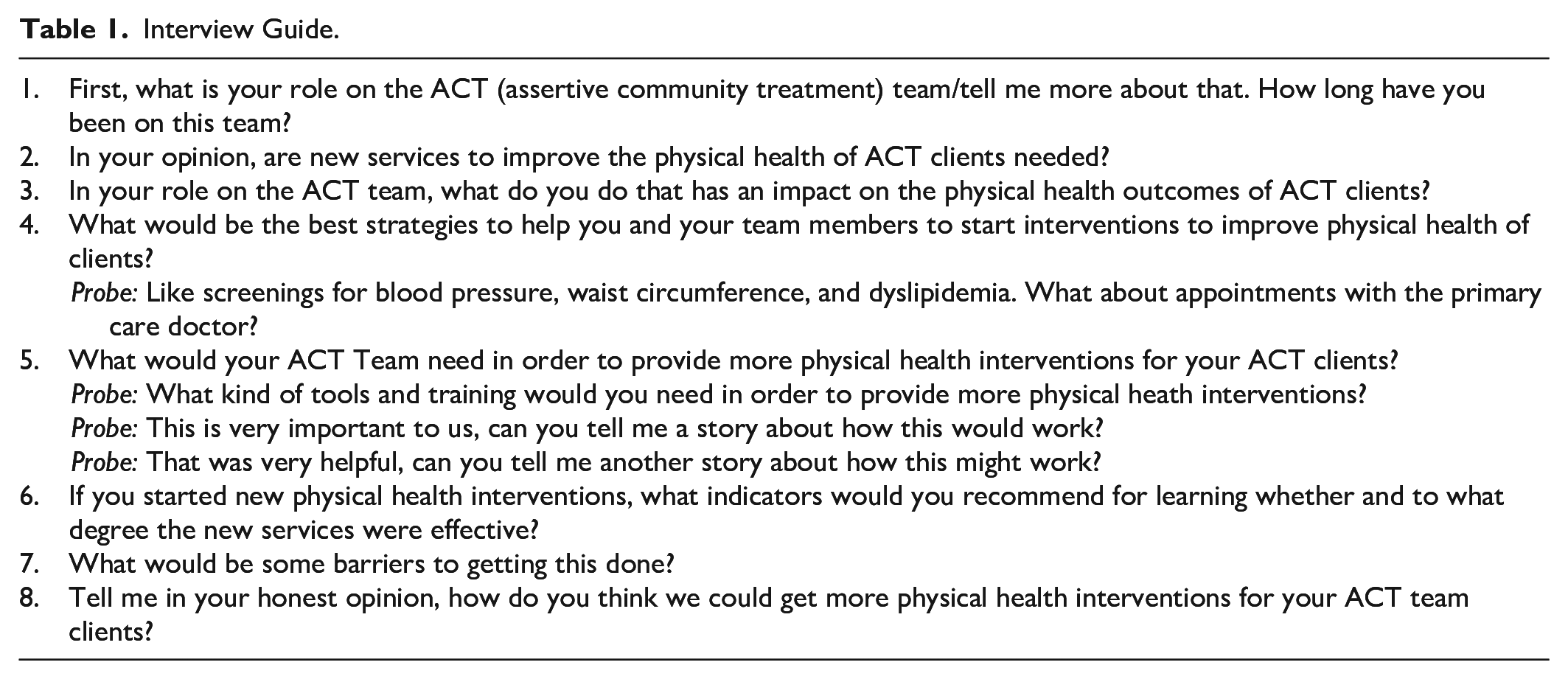
To maintain rigor in the qualitative interviews, a standardized semistructured interview guide was developed (Table 1). The interview guide was developed using the existing ACT model of care, evidence-based implementation strategies, and criteria for the care of individuals with metabolic syndrome (McEvoy et al., 2005; Powell et al., 2015; Proctor et al., 2009; Vancampfort et al., 2015; Ventriglio et al., 2019). The interview topic list included physical health care needs of ACT consumers, staff roles in providing physical health services for ACT consumers, strategies to improve the physical health of ACT consumers, barriers to providing services to improve the physical health of ACT consumers, strategies to implement interventions to improve physical health, tools needed to provide physical health interventions for ACT consumers, and realistic goals or outcomes for assessing improvement in physical health services. Data were collected, via Zoom, in one-to-one interviews with ACT team members. All interviews were less than 40 minutes in length, were digitally recorded, and professionally transcribed. Interview transcripts were checked for accuracy and managed in Atlas.ti (Scientific Software Development, 1997).
Interview Guide.
Analysis
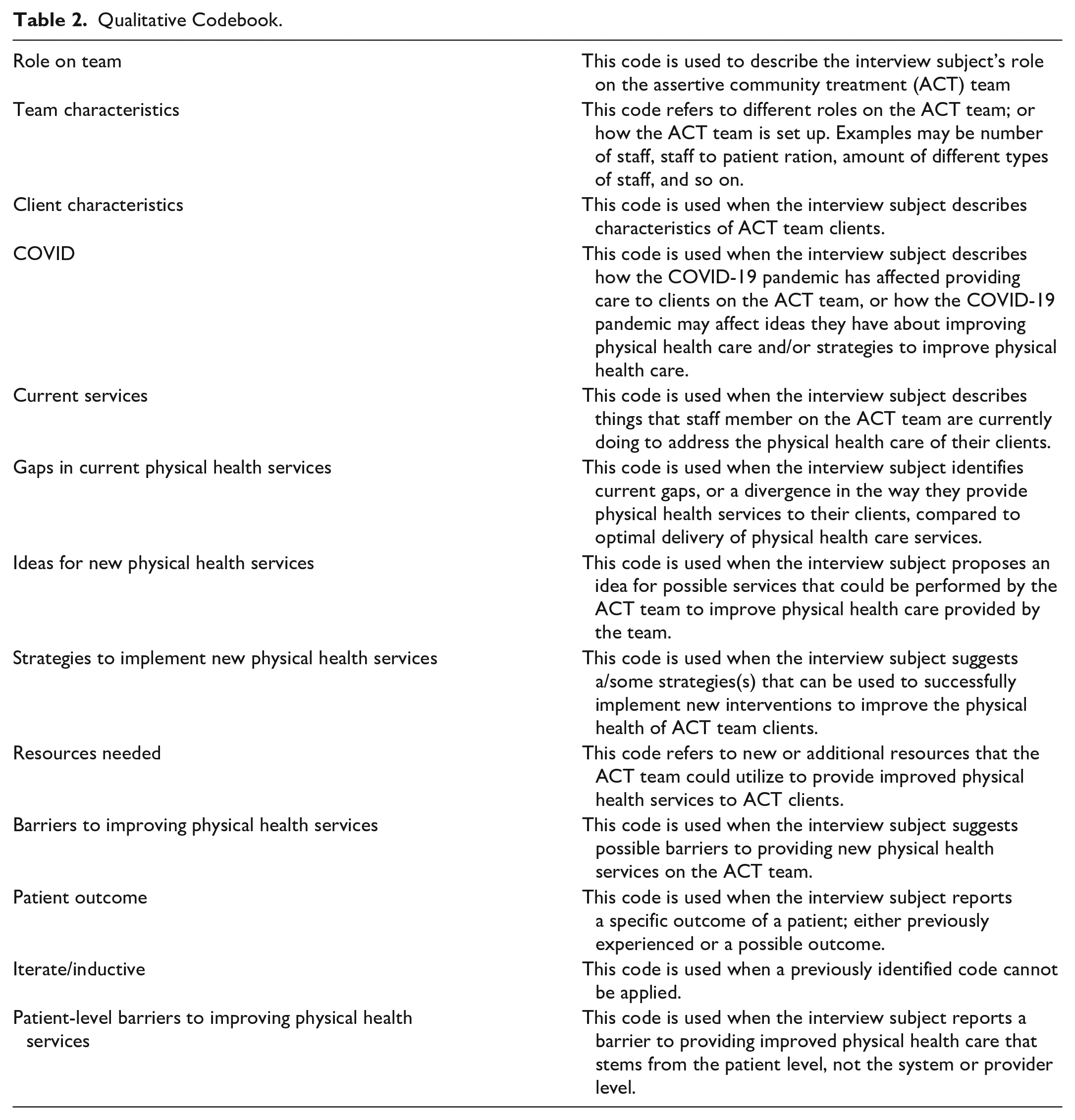
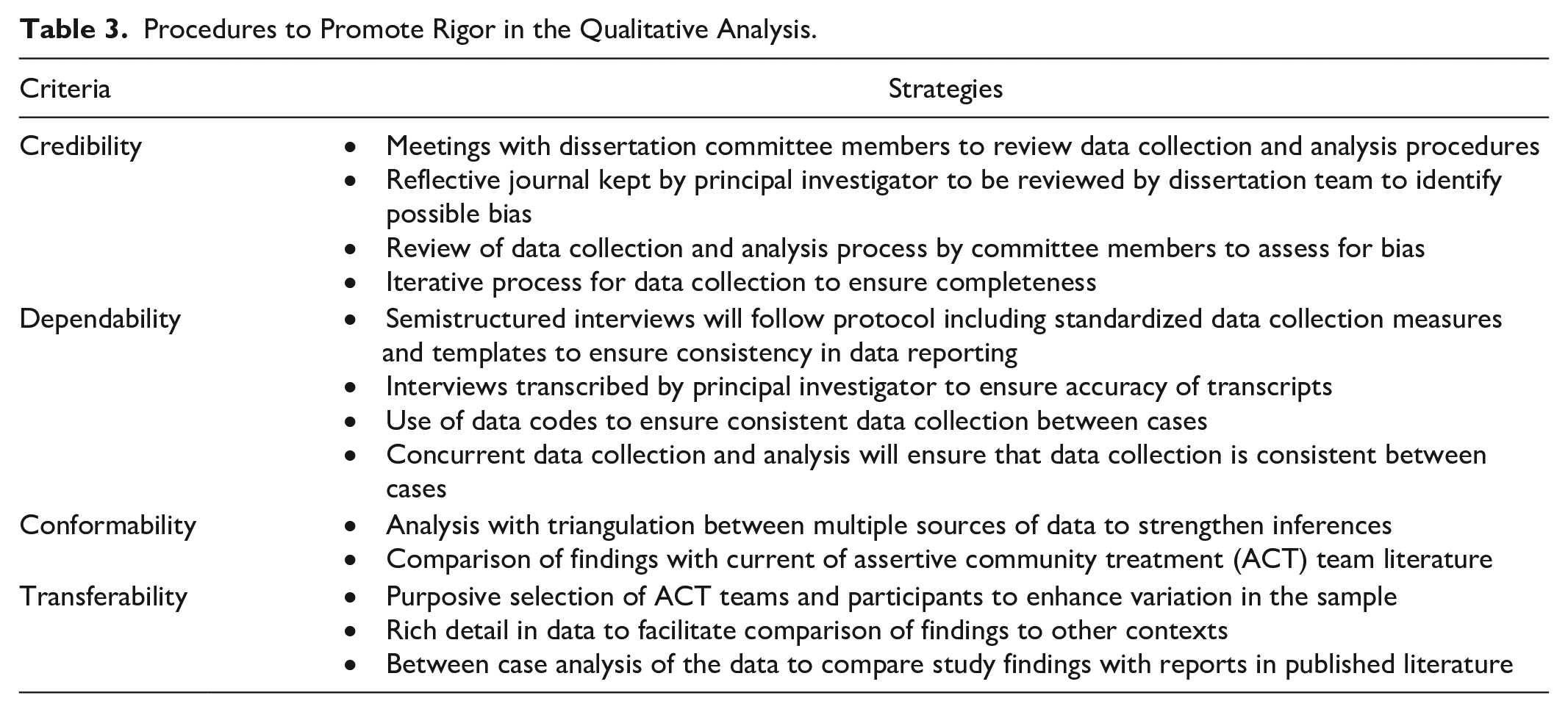
Two investigators (BR and MT) participated in the analysis of the interview transcripts (Braun & Clark, 2006; Miles & Huberman, 1994). First, all transcripts were read to gain familiarity with the full group of interviews. Investigators discussed the data and developed a codebook based on the semistructured interview guide (Table 2) with standardized codes and definitions for classifying data in the transcripts. After the codebook was developed, two investigators (BR and MT) double coded 25% of the transcripts, discussed areas of disagreement, added minor revisions to the codebook, and agreed on coding procedures; then, the PI used the final codebook to code the remainder of the transcripts. When all data were coded, the study team used thematic analysis to describe explicit patterns in the interview transcripts (Braun & Clark, 2006). Strategies that were used to ensure rigor in all study procedures are described in Table 3. Within the table, strategies that were used to promote credibility, dependability, conformability, and transferability are listed.
Qualitative Codebook.
Procedures to Promote Rigor in the Qualitative Analysis.
Results
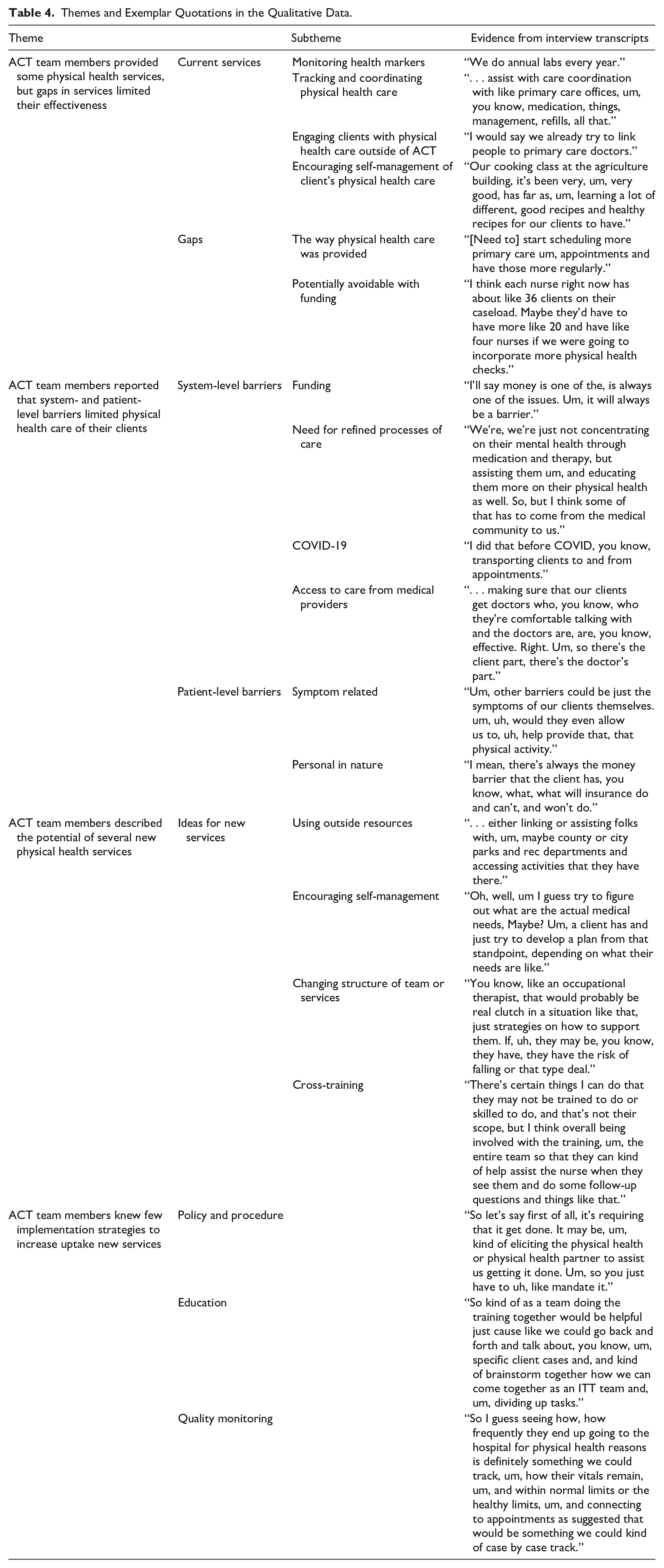
As illustrated in Table 4, four main themes were identified: (1) ACT team members provided some physical health services, but gaps in services limited their effectiveness; (2) ACT team members reported that system- and patient-level barriers limited physical health care of their clients; (3) ACT team members described several new physical health services; and (4) ACT team members were aware of few implementation strategies to increase uptake of new services.
Themes and Exemplar Quotations in the Qualitative Data.
ACT Team Members Provided Some Physical Health Services, But Gaps in Services Limited Their Effectiveness
ACT team members described current physical health services, such as monitoring health markers, tracking and coordinating physical health care, engaging clients with physical health care outside of ACT, and encouraging self-management of physical health care. ACT team members frequently reported that they assessed physical health care needs (e.g., blood pressure readings, glucose readings, and lab values). For example, one staff member reported, “I’m used to . . . our medical staff being very involved with the physical health of our clients, whether that’s blood pressure, diabetes, um, you know, back pain” (S1). A nurse reported, “When we see them, we typically do . . . some vital signs, blood pressure and we do, we actually do waist circumference sometimes as well” (S19). ACT staff members also reported services related to tracking and coordinating physical health care. One team member stated, “When we start with clients, we always get a release to talk to the primary care physician, so we can try to care coordinate” (S5).
ACT team members on all three teams reported that they coordinated care with medical providers outside of the ACT team. One ACT nurse reported, So, if they [ACT clients] have any symptoms that they’re experiencing or concerns about their physical health, um, they usually let me know. Or I can tell that that’s happening or whatever. And I can make sure that they get an appointment with their PCP. (S19)
Another ACT staff member reported, “We already try and connect all of our clients to a primary care provider” (S3). One ACT team member stated, “Our nurses for some clients have set up like calendar books to help them know when their PCP appointments are” (S1). That same staff member later reported, “Our team will help, you know, they’ll help set up whatever appointment needs . . . or make sure that clients are doing that themselves and following up” (S1).
ACT staff members also reported gaps in physical health services that limit the effectiveness of their work. One ACT team member reported that many basic services and supports are not available for her clients; she stated, They [ACT clients] don’t . . . have exercise programs or they have hard time getting to doctor’s appointments, um, following through on what they need, their meds that they may need, and that kind of stuff. And we worked with a lot with that kind of stuff, but there’s always improvements. (S2)
ACT staff reported the need for standardized tools for monitoring and recording physical health status. A staff member stated, “As far as the cholesterol and stuff and blood pressure check, that needs to be more—so, like on a screen on a daily basis—when they come in, um, just for the weekly checkup” (S12). Another team member reported that transportation to see physicians was a major barrier to achieving physical health goals for clients. She stated, “It would be helpful if you have more than one vehicle so we could, you know, have different people taking them to appointments” (S11).
ACT Team Members Reported That System- and Patient-Level Barriers Limited Physical Health Care of Their Clients
ACT staff members reported system-level barriers related to funding, the need for refined processes of care, COVID-19, and access to care from medical providers. An ACT team member stated, “Manpower, like I said, we would need another, somebody else to help out . . . 55 clients is a lot for one nurse to keep up with” (S11). Another ACT team member reported, “Shouldn’t be a cap on four contacts and that’s the maximum amount” (S12). On funding for transportation as a barrier, one ACT staff member stated, I think what would be really helpful is an expanded like public transit system, which may not seem like it’s connected to health directly. . . . I think if they had like a wider variety or better communication with the public transit system now that would actually really improve like their attendance. (S5)
ACT staff also reported the need to refine processes of care. One ACT staff member described barriers in the doctor’s office: Also, with our doctor’s offices in the town, that our office is in, they require them to go in ahead of time to fill-out the paperwork before they’ll even schedule an appointment. And that’s just, it’s a lot for our folks. (S11)
In addition to the challenges in the doctor’s office, another ACT team member reported that physical health problems tend to be forgotten the longer clients are on the team; she stated, “I think a lot of our folks have been on the team for a long time and it’s not as much our focus now” (S7).
COVID-19 has generated another set of barriers on which ACT staff reported. For example, one ACT team member stated, “Prior to COVID-19 I was able to help transport them to appointments” (S14). Another ACT staff member reported, “We aren’t supposed to touch our clients right now” (S6).
Several ACT team members described challenges related to access to care from medical providers. One stated, “Sometimes that connecting to the provider is the difficult part” (S7). Another staff member stated, We’re, we’re just not concentrating on their mental health through medication and therapy, but assisting them . . . educating them more on their physical health as well. So, but I think some of that has to come from the medical community to us. (S1)
Other system level barriers included wellness centers with no accommodations for clients with SMI, insufficient time, and the competing necessity of providing physical health services while maintaining fidelity to the ACT model.
Patient-level barriers to receiving improved physical health services that were symptom related or personal were also reported on by ACT staff members. One ACT team member described how symptoms of mental illness create a barrier to physical health care, “You know, if they’re not sort of arguing in their head and seeing . . . things around them, it’s a lot easier to say, Oh, I have a doctor’s appointment at X time. I can get there” (S16). Another ACT staff member reported, “Um, especially with the nature of diagnoses on ACT teams, they might be more paranoid around new people” (S7).
Personal barriers to physical health services included the preferences of ACT consumers, who were often afraid of or unaware of physical health services. An ACT team member stated, “Um, screening for blood pressure, for sure. If they’ll [ACT clients] allow you to do it. Sometimes they will” (S11). Other patient-level barriers that were personal in nature included poverty, client refusal, and lack of insurance.
ACT Team Members Described the Potential of Several New Physical Health Services
ACT team members recommended new services to improve care of their clients, including (1) using outside resources to provide physical health services, (2) encouraging more self-management of physical health, (3) changing structure of the team or structure of physical health services provided, and (4) cross-training nonmedical staff. One ACT team member suggested that outside personnel should provide physical health service, “I believe that there should be a medical service where they can meet them at their homes” (S13). Another ACT staff member stated, “Like if we had a group, if they could come and allow us to bring our clients to get checked out, that would be super helpful. Same thing with like the dentists that would be super helpful” (S11).
Some ACT team members had ideas that involved encouraging self-management of physical health. For example, one ACT staff member stated, I was thinking we should start a, like a physical training group, where clients can get together to, you know, socialize of course, since most of our clients isolate, but then also exercise more as well to improve their health and then like provide incentives at the end of the classes to keep them coming back. (S10)
ACT staff members also offered ideas for changing the structure of the team to be able to provide more physical health services. One team member emphasized the importance of trusting relationships that already exist on ACT teams. She stated, If we [ACT team staff] could just do all his physical health checks, that’d be perfect. He trusts us, he meets with us. Um, so I think for someone like him, this kind of thing would be perfect . . . if we could kind of be a wraparound service and do it all in one, um, that’d be awesome. (S4)
A nurse suggested that teams should add a clinical nurse with primary care training. She explained, That to me is sort of the point of maybe having a new, like a nursing person to sort of implement uh new programs like someone centralized within the whole system . . . someone to really coordinate it for not just our team, but all the teams in the company. (S16)
Finally, ACT team members recommended cross-training for nonmedical staff to provide more manpower to help clients manage a wide array of physical health symptoms and treatments. One ACT team member reported, “Our nurse does a lot and to ask of her to do more is, is a lot, but I guess we could be trained in how to take a blood pressure” (S6). Another ACT nurse stated, . . . and then education for nonmedical staff . . . the blood pressure monitor for those that are not, don’t have medical background is, is not a manual, it’s automatic. So I could show them how to properly put it on their arm and they just hit start and they could record it. They don’t have to really interpret it. They can bring it back to me and I could interpret it and decide like, you know, this is a problem, or this is normal. (S14)
ACT Team Members Knew Few Implementation Strategies to Increase Uptake New Services
ACT team members’ perceptions of strategies to increase uptake and sustainability of new physical health services included (1) added policies and procedures, (2) new education strategies, and (3) improved quality management strategies. When describing the need for new procedures for assessing the needs of clients and creating process evaluation tools, one nurse reported, A lot of it is just sort of taking a look at what you have in terms of who your patient load is. Who’s their doctor, how often do they go? Do they take their meds? Really just kind of assessing what you have and seeing where the needs are. (S16)
Another staff member suggested that new policies were needed to establish physical health care services; she said, “Well to me, it’s just making it required, then you have to do it . . . and then follow up on it . . . so that’s all it would take” (S1). Another ACT team member stated, “Just hold mandatory trainings . . . unlike other trainings that we have on the ACT team that are voluntary, go ahead and just hold mandatory ones” (S10).
ACT team members also suggested care would be improved with new educational opportunities. For example, one team member stated, “The whole team could benefit from having more training about physical health” (S15). Another ACT team member reported, Maybe more training on how the physical health is impacted when you do have a mental health diagnosis, because I know folks with schizophrenia die on like an average of 25 years earlier than other folks. So maybe more training on how those two intersect each other and how we need to pay more attention to that. (S10)
Specialized training was also suggested to learn how to engage ACT clients in medical care. One ACT team member spoke at length about this key point; he stated, One of the barriers might be some pushback from the clients themselves, um, not really being interested in exercise or increasing their fitness. So, in those cases, we would need to do a fair amount of motivational interviewing just to explore people’s, um, motivation that we could use to leverage, um, and helping them see that in even small changes . . . can make an impact. So, it would just be figuring out where, where the individual is currently with their health, health and wellness, or fitness and, where they might like to be. (S9)
ACT staff also described quality management as an implementation strategy to improve uptake of physical health services. An ACT team member reported, [We need] more of a, I guess more organized, um, like, list of our clients and knowing that they were all like having an up to date on their mammograms. . . . Up to date on colonoscopies . . . and just keeping track better of that stuff and I think having that, um, all of that up to date would make me feel as though we were doing, you know, a good job as far as keeping up with our clients health. (S19)
With improved systems for tracking the needs of ACT clients, staff members described the potential for greater capacity to formulate plans of care. A staff person stated, You’d have to start with a baseline assessment, um, um, levels of knowledge that clients would have about certain health conditions in their current, um, ability to monitor physical things. Um, and then kind of test that throughout the treatment. You know, every, I mean it would have to be maybe just an ongoing assessment. (S8)
Discussion
Consistent with limited prior evidence, ACT team members reported that they already provide some services to manage the physical health issues of their clients (Meyer-Kalos et al., 2017; Shattell et al., 2011; Vanderlip et al., 2014). However, ACT team members recognized the need for additional health services, such as monitoring chronic illnesses and promoting health lifestyle habits. These findings align with evidence in a previous study, reporting that 80% of ACT team leaders believed more information about health screenings was required to change the way they assess physical health (Vanderlip et al., 2014).
The finding that ACT services omit key physical health services suggests the need for ACT team support to manage chronic illnesses, such as hypertension, and the sequelae of unmanaged illness, such as stroke (SHEP Cooperative Research Group, 1991; Woo et al., 2004) and myocardial infarction, heart failure, and kidney disease (Elperin et al., 2014). Moreover, additional ACT services may be needed to prevent harms of unmanaged diabetes, such as eye damage, renal damage, CVD, stroke, and peripheral artery disease (Deshpande et al., 2008), as well as obesity and related sequelae such as CVD, diabetes, dementia, and cancer (Kinlen et al., 2018). Future research in this area should be focused on interventions to improve clinical outcomes associated with these gaps in care.
In addition to developing new physical health services, research and quality improvement activities may also be needed to evaluate the completeness of ACT implementation and the degree that nurses on ACT teams receive adequate training for their complex roles. In our study, all the nurses interviewed were RNs and none were APRNs. Thus, another strategy to improve the physical health of ACT clients may be to implement ACT models using APRNs more frequently and to identify strategies for training RNs (Kane & Blank, 2004). Future research may also be necessary to examine the thoroughness of ACT model implementation and the influence implementation has on medical outcomes for ACT consumers.
Participants suggested the importance of an integrated, community approach for improving physical health services. This was evident when an interview subject emphasized that part of treating physical health care needed to come from the medical community, outside of ACT. Other ACT team members emphasized improving collaboration with primary care providers. This finding is consistent with previous research indicating that improved collaboration among medical and mental health providers was a vital tool to address the physical health needs of persons with SMI (Meyer-Kalos et al., 2017; Shattell et al., 2011).
Findings in this study included ACT team member descriptions of common barriers to providing ACT consumers with optimal physical health care. The findings accord with barriers to care identified in earlier research, such as lack of health insurance, poor funding for physical health services, few primary care doctors who are willing to work with clients with SMI, and client preference on where they receive primary care (Shattell et al., 2011). Additional barriers to physical health services include client-level barriers to care such as poverty, access to care, and transportation (Meyer-Kalos et al., 2017). Collectively, these findings suggest potential areas for improvement to create effective physical health services for adults receiving ACT care.
While findings support earlier research, this study also indicated barriers that have not previously been discussed; for example, those related to the COVID-19 pandemic. These barriers included being unable to transport clients, unable to touch clients (e.g., take vitals), the inability to have in-person trainings to improve knowledge regarding physical health, and the need for additional psychological therapy to address client frustration and isolation. Important next steps to address other barriers described in this study will be research and quality improvement activity to raise awareness of the special needs of adults with SMI and policy changes to support the work of ACT team members, such as increasing office staff to coordinate and solve administrative problems related to integrating mental health and primary care services on ACT teams. Furthermore, new staff and clinical services may be needed to increase physical health services on ACT teams, such as new health screening techniques to prevent the spread of infections and control symptoms of chronic illnesses.
Very little prior research has evaluated the impact of implementation strategies designed to increase uptake of physical health interventions in ACT teams. Findings in this study suggest the need for training ACT team members with new skills to provide physical health services. In this study, two thirds of ACT staff members reported that training would be essential to improving physical health services on their team. Furthermore, 17 of the 19 team members reported the need for quality monitoring strategies to ensure that physical health interventions were being performed effectively. These findings suggest that a combination of tools, training, and technical assistance are required to improve physical health care services on ACT teams.
Our findings also suggest implications for policy. For example, one ACT staff described a service cap of four visits per month for ACT consumers; this barrier in the reimbursement policy is a significant barrier to increasing care of the physical health needs of ACT consumers. One solution might be an ACT wraparound service, in which the ACT model is modified to provide complete medical and mental health care to their clients. Moreover, many ACT team members reported that additional nursing staff might be required to address the complex medial needs of ACT consumers. This may require changing the structure of the ACT team to include more nursing staff compared with social work staff. Social work staff are valuable in providing wrap around psychiatric services to clients, but the ACT model may need modification to provide wrap around medical and dental services.
The limitations of this study deserve comment. First, the study setting (three ACT teams) and the small sample size limits the generalizability of the findings. A strength in the sample was that participants in the interviews were from several disciplines, including four nurses, a psychiatrist, a peer support specialist, two administrative staff members, and three team leaders. A second limitation was that the sample included ACT team members and did not include ACT consumers or other community providers, such as primary care physicians or clinical nurses. Nonetheless, the study provided consistent evidence of a common set of barriers and potential solutions to provide improved physical health services to ACT consumers.
Conclusion
Adults with SMI, compared with adults in the general population, more frequently experience serious adverse health events and death related to poorly managed physical health care needs (Correll et al., 2017). Findings in this qualitative study identified a common set of challenges and potential solutions for developing and testing new physical health services for adults with SMI and ACT consumers.
Footnotes
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Nursing Research of the National Institutes of Health under Award Number T32NR007091. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Research reported in this publication was also supported in part by a Samuel B. Kellett Long Future Nursing Faculty Scholarship.