
Abstract
BACKGROUND:
Nurses and nursing students are at risk for negative mental health as a result of significant work stressors from the COVID-19 pandemic.
AIMS:
The purpose of this study was to (1) describe the mental health of nursing students during the COVID-19 pandemic, (2) investigate relationships between stressful COVID-19 experiences and mental health, and (3) examine correlates of mental health service use.
METHOD:
This observational study used a web-based survey to assess COVID-19 experiences, self-reported mental health, and mental health service utilization among nursing students in Los Angeles in spring 2021 (N = 174, 30.1% response rate). The survey used measures of stressful COVID-19 experiences (personal COVID-19 illness, hospitalization of close friends or family, and death of close friends or family), loneliness, resilience, depression, anxiety, COVID-19-related traumatic stress, and utilization of campus and noncampus mental health services.
RESULTS:
Students had high levels of depression (30%), anxiety (38%), and traumatic stress (30%). There was no relationship between stressful COVID-19 experiences and mental health, but loneliness was associated with higher odds of mental health problems and resilience with lower odds. Mental health problems were not associated with use of campus or noncampus mental health services. Students with primary caregiving responsibilities (OR = 0.22, 95% CI [0.05, 0.87]) and students who identified as Asian/Pacific Islander (OR = 0.24, 95% CI [0.09, 0.70]) had lower odds of mental health service utilization.
CONCLUSIONS:
Resilience and loneliness affect nursing student risk for negative mental health as a result of the COVID-19 pandemic. Targeted, accessible mental health support within nursing education programs may be warranted.
Introduction
As of May 2021, there have been an estimated 32 million confirmed cases of coronavirus disease 2019 (COVID-19) disease caused by the SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) coronavirus and 570,000 deaths in the United States, with several acute periods of public health strain and patient surges for health care systems (Centers for Disease Control and Prevention, 2021). Frontline health care workers have experienced significant personal and occupational stressors as a result of working in the COVID-19 pandemic, including not having enough personal protective equipment (74%), concerns about personal safety (64%), and fear of going to work (85%; Arnetz et al., 2020). Pandemic stressors have potential to harm the mental health of frontline health care workers, including physicians, nurses, therapists, and support staff. There is particular concern about the mental health of nurses, who are most often in intensive patient care roles and at risk for experiencing overwork, burnout, and stress as a result of pandemic working conditions (Chen et al., 2021; Hu et al., 2020; Murat et al., 2021). Nurses are among the health care workers most likely to test positive for COVID-19 and to die from COVID-19 (Jackson et al., 2020). There is early evidence for elevated levels of depression, anxiety, insomnia, and distress among nurses during COVID-19, as well as evidence that nurses are at elevated risk for suicide compared with the general population and with physicians (Chen et al., 2021; Davis et al., 2021; Hu et al., 2020; Murat et al., 2021).
This risk for poor mental health among nurses extends to nursing students, who are working in similar stressful pandemic conditions but also managing the stress of a rapid switch to remote learning. Recent studies of college students suggest similar elevated levels of psychological distress and a need for mental health resources (Copeland et al., 2021; Son et al., 2020; Zimmermann et al., 2020). A recent national survey of college students in the United States found that that one in five college students report a decline in their mental health during COVID-19 (Active Minds, 2020). It is evident that young adults are at high risk for mental health problems during COVID-19 and that there is a need for research on resources to support student mental health. Although studies have suggested that COVID-19 has greatly harmed the mental health of nurses and college students independently, there is limited research on the mental health of nursing students, who sit at the unique intersection of college students and health care workers.
Studies are needed to understand the mental health experiences and needs of nursing students during the pandemic, as well as what kinds of campus and community resources can support mental well-being among students entering essential worker professions like nursing. There was one survey of graduate nursing student mental health conducted in June 2020. This study found that approximately 25% of students experienced significant depression, anxiety, or stress and 24% of students experienced posttraumatic stress symptoms (Rosenthal et al., 2021). However, because the study did not assess students’ COVID-19 experiences, did not include undergraduate nursing students, and was conducted prior to the most severe wave of the COVID-19 pandemic from November 2020 to January 2021, there are still unanswered questions about nursing student mental health. Thus, the purpose of this study was to (1) describe the mental health of nursing students during the COVID-19 pandemic; (2) investigate relationships between stressful COVID-19 experiences (personal COVID-19 illness, hospitalization of close friends or family, and death of close friends or family) and mental health problems; and (3) examine relationships between mental health problems and use of campus and noncampus mental health services. We hypothesized that (1) students who reported stressful COVID-19 experiences would have worse mental health than those who did not and (2) that students who had higher levels of mental health problems (i.e., need) would have higher utilization of campus and noncampus mental health services.
Method
Design
This observational study used a onetime, web-based survey to assess COVID-19 experiences, self-reported mental health, and mental health service utilization among nursing students. We relied on the Anderson Healthcare Utilization Model as a conceptual framework for this study, where service utilization is determined by predisposing factors (e.g., gender, race, and age), enabling factors (e.g., health insurance), and need (e.g., actual or perceived need for health care; Andersen, 2008; Andersen & Newman, 2005; Babitsch et al., 2012). At the nursing school from which our sample was selected, all students are required to have health insurance and are eligible for all campus-based mental health services assessed in our survey, and thus have comparable potential ability (i.e., enabling factors) to access campus-based services. Participants were recruited from a School of Nursing at a large, research university in Los Angeles. The survey included 81 items, and participation was voluntary and anonymous. The study was reviewed and determined to be exempt from institutional review board regulation by the University of California, Los Angeles.
Sample and Survey Procedures
All actively enrolled nursing students were eligible to participate in the survey, including undergraduate, masters, and doctoral (DNP or PhD) students. The School of Nursing had approximately 604 enrolled students across all programs in 2020. Students were invited to participate in the study through a series of emails from school administration and social media recruitment by student representatives from all programs. A study description was provided on the survey landing page, including contact information for study investigators for questions related to the research. Although the study was exempt from institutional review board regulation, we required all participants to digitally indicate that they understood the study and gave consent to participate (yes/no) before proceeding with the survey. All survey participants were provided with a comprehensive list of campus and community resources for emergent and nonemergent mental health needs. The survey was administered via Qualtrics, and there were no fields for participant identifying information to ensure anonymity (Qualtrics XM, n.d.). The survey was open from March to April 2021 and was available to students via phone, computer, or tablet. There were 182 students who completed the survey for a 30.1% response rate. These respondents were representative of the nursing student population as a whole in terms of race/ethnicity and gender in chi-square goodness-of-fit tests. Eight respondents did not answer any survey items and were omitted from the sample for a final analytic N of 174.
Measures
The survey measured COVID-19 experiences, student self-reported mental health, two risk/protective factors (loneliness and resilience), use of campus and noncampus mental health services, and sociodemographics.
COVID-19 Experiences
Students were asked whether they had ever tested positive for COVID-19, whether any close friends had ever tested positive for COVID-19, and whether any family members had ever tested positive for COVID-19. For the self-COVID-19 item, they were asked to rate their illness severity on a 5-point Likert-type scale (1 = No symptoms, 5 = Severe symptoms requiring hospitalization). For the close friends and family items, students were asked whether members of each respective group had ever been hospitalized for COVID-19 and whether they had died from COVID-19.
Mental Health
Three measures were used to assess areas of student self-reported mental health, including depression, anxiety, and traumatic stress.
Depression
The two-item version of the Patient Health Questionnaire (PHQ-2) is a widely used, validated screener for clinical depression (Arroll et al., 2010; Löwe et al., 2005). The eight- or nine-item versions are used most frequently, but the two-item version has also been studied and validated as a reliable indicator of probable depression (Arroll et al., 2010). The items use 4-point Likert-type scales to assess the frequency of depressive symptoms (Not at all to Nearly every day), with scores of 3 or higher indicating probable depression. Because the PHQ-2 is not specific to COVID-19, we also included one item assessing the extent to which students attributed their responses to the COVID-19 pandemic. The COVID-19 attribution item was rated on a 5-point Likert-type scale, with higher scores representing stronger attribution of depression symptoms to the pandemic.
Anxiety
The General Anxiety Disorder–7 (GAD-7) is a validated measure of generalized anxiety that uses seven items rated on a 4-point Likert-type scale to assess the frequency of anxiety symptoms (Not at all to Nearly every day; Spitzer et al., 2006). Scores of 10 or above are considered moderate or severe anxiety. Like the PHQ-2, we included a COVID-19 attribution item for the GAD-7 rated on a 5-point Likert-type scale, with higher scores representing stronger attribution of anxiety symptoms to the pandemic.
Traumatic stress
The COVID Stress Scales is a new measure of COVID-19 related stress, developed and validated rapidly in 2020 (Taylor et al., 2020). It contains six subscales for danger, socioeconomic consequences, xenophobia, contamination, traumatic stress, and checking items specific to COVID-19 stressors. This study used the six-item traumatic stress subscale to assess COVID-19-related trauma symptoms. Items were rated on a 5-point Likert-type scale. There is not yet an established clinical-range cutoff score for this measure, so scores were examined as a continuous score variable ranging from 0 to 24, with higher scores denoting higher COVID-19-related traumatic stress.
Risk/Protective Factors
We examined loneliness as a risk factor for poor mental health and resilience as a protective factor for mental wellness.
Loneliness
We assessed loneliness with the six-item DeJong Gierveld Loneliness Scale, a brief, validated measure of emotional and social loneliness (Gierveld & Van Tilburg, 2006). Items are reported on a 3-point Likert-type scale (Yes, More or less, and No), with Yes or More or less responses counted as indicators of loneliness. Positive loneliness items are summed across items and scores range from 0 to 6.
Resilience
Student resilience, the ability to persist in the face of adversity, was measured with the Brief Resilience Scale (BRS; Smith et al., 2008). This six-item measure uses a 5-point Likert-type scale (Strongly disagree to Strongly agree), with scores then averaged across items for a range of 1 to 5. Scores less than 3 are considered low resilience; scores from 3 to 4.3 are considered normal resilience; and scores greater than 4.3 are considered high resilience.
Service Utilization
We assessed service utilization during the COVID-19 pandemic (past 12-month utilization) for 12 campus-based mental health services and nine general mental health services not specific to the university. The campus mental health services questionnaire asked whether students had heard of and actually used each service. The campus mental health services were collapsed into four categories: services for mental illness (three services), mindfulness/meditation services (three services), primary care services for mental health (two services), and resilience promotion services (three services). All service items were analyzed as binary yes/no indicators of whether the student had used at least one service in the category. For noncampus mental health services, students reported yes/no utilization of the following services for mental health outside of the university: individual psychotherapy, group/couple psychotherapy, partial hospitalization or day treatment, inpatient or residential treatment, primary care services for mental health, mindfulness/meditation programs, mobile apps for mental health, and self-help groups.
Sociodemographics
Sociodemographic measures included age (years), gender (female, male), education program level (bachelors, masters, and doctoral), relationship status (married/partnered, single/not in a committed relationship, single/in a committed relationship, and other), race/ethnicity (White/Caucasian, Black/African American, Hispanic/Latinx, Asian American/Pacific Islander, Multiracial, and other). We also assessed whether students had primary caregiving responsibilities for children or other dependents (yes/no) and whether students self-identified as having a disability (yes/no), circumstances which have potential increase stress and risk for poor mental health in the context of the pandemic.
Analysis
Data were analyzed using R, version 4.0.3(R Core Team, 2020). We conducted a power analysis and determined that a sample of at least 137 participants would be needed for 80% study power at a .05 level of statistical significance; thus, our sample size of 174 students was adequate. For the analytic sample, data were missing at a rate of 1.8%. These data were multiply imputed using chained equations. Descriptive statistics and frequencies were used to characterize the study sample. Bivariate tests (analysis of variance for continuous variables and chi-square tests for categorical variables) were used to compare students’ COVID-19-related mental health by COVID-19 experiences (personal COVID-19 illness, hospitalization of a close friend or family member, and death of a close friend or family member).
In the first set of models, multiple logistic regression models were used to identify associations between COVID-19 experiences and mental health problems attributed to COVID-19, adjusting for sociodemographic factors. The outcome variables were constructed by considering those who had clinical risk-range scores on each mental health measure (PHQ-2, GAD-7, COVID-19 Traumatic Stress) and, for the PHQ-2 and GAD-7, those who attributed their responses on each respective measure directly to the COVID-19 pandemic. The attribution items were used only for the PHQ-2 and GAD-7 because these measures are not specific to COVID-19, while the COVID Traumatic Stress scale was specific to COVID-19. Then, risk/protective variables were added to the models.
In the second set of models, multiple logistic regression models were used to identify associations between mental health problems (i.e., need) and utilization of campus and noncampus mental health services, adjusting for COVID-19 experiences and sociodemographic factors. All campus mental health service variables were collapsed into a single, binary indicator of any campus mental health service use during the COVID-19 pandemic. All noncampus mental health services were collapsed in the same manger into a single, binary indicator.
Results
Sample Description and Stressful COVID-19 Experiences
The sample was primarily masters-level students (54.6%, n = 95) who were female (89.1%) and married, partnered, or in a relationship (combined 58%, n = 101; Table 1). A majority of students identified as Asian/Pacific Islander (37.9%, n = 66), White (22.4%, n = 39), or Hispanic/Latinx (19.5%, n = 34). Approximately 40% (n = 69) were first-generation college students, and 12.6% (n = 22) had primary caregiving responsibilities. Five percent of students (n = 9) self-identified as having a disability. Students had high levels of depression (30%), anxiety (38%), and COVID-19-related traumatic stress (30%), and 85% of students with one or more of these mental health problems had used at least one on or off-campus mental health service (Figure 1). Students had statistically comparable levels of depression and anxiety when compared by education level, but masters-level students had higher proportions of COVID-19-related traumatic stress (37.9%) than undergraduate (25.0%) or doctoral (10.5%) students (p = .01).
Sample Characteristics.
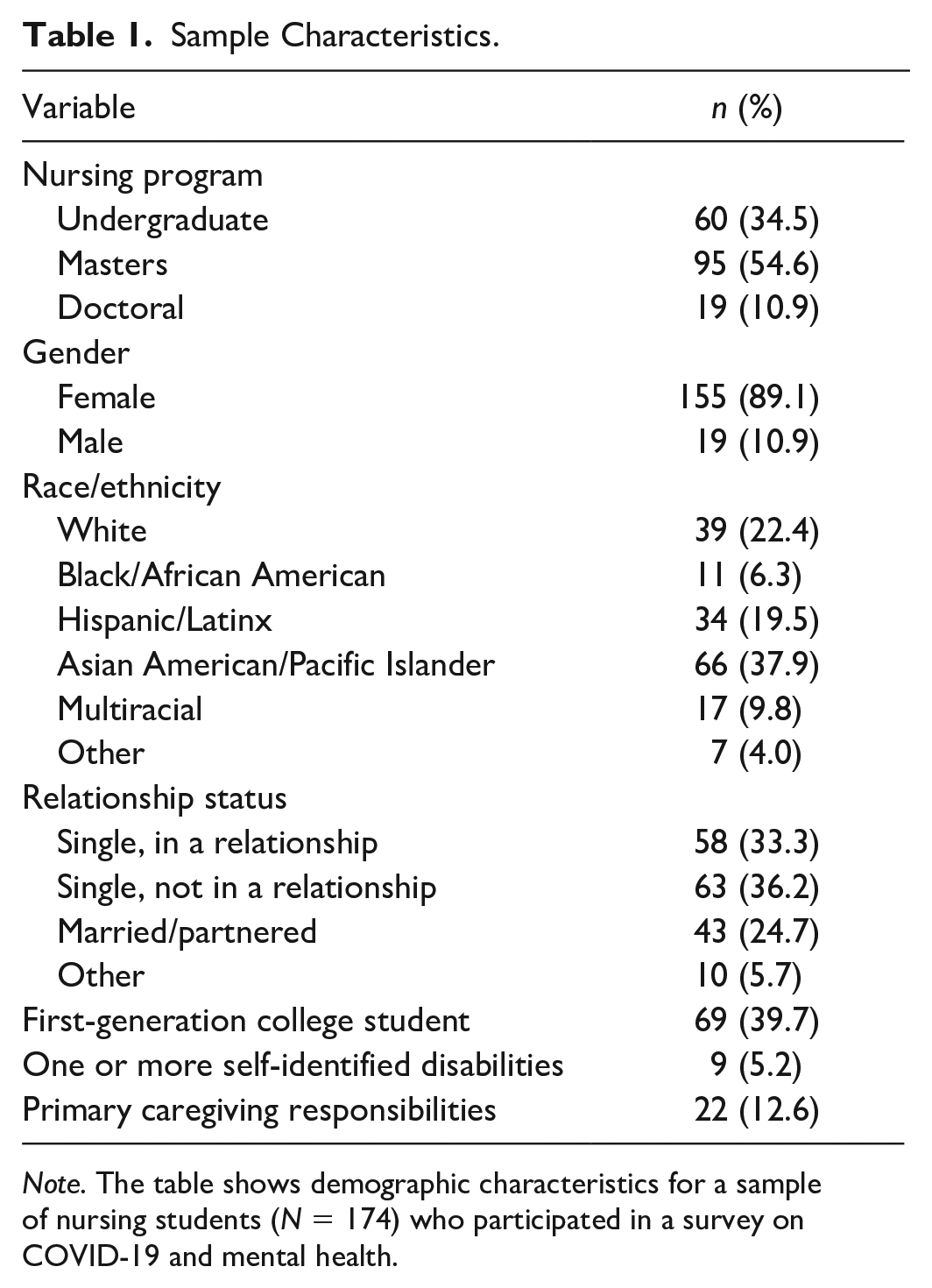
Note. The table shows demographic characteristics for a sample of nursing students (N = 174) who participated in a survey on COVID-19 and mental health.
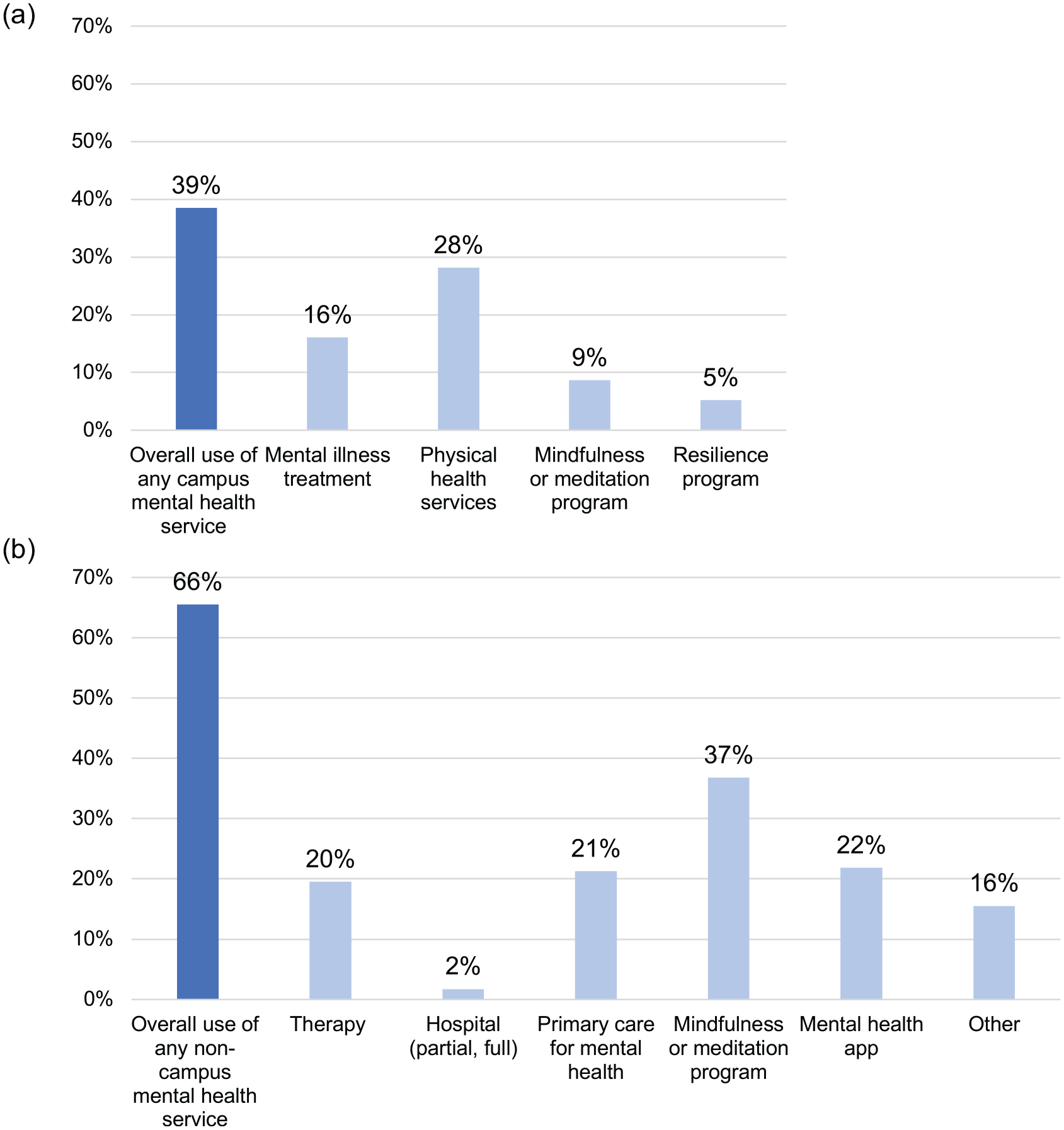
Mental health service utilization. (a) Percentage of nursing students (N = 174) who reported using each of four types of campus mental health services and overall utilization of any of the campus mental health services. (b) Percentages for six noncampus mental health services and overall utilization of any of the noncampus mental health services.
Stressful COVID-19 experiences were relatively rare among participants. Approximately 7.5% of students (n = 13) reported having tested positive for COVID-19; 17.2% (n = 30) reported hospitalization of a close friend or family member with COVID-19; and 2.9% (n = 5) reported the death of a close friend or family member from COVID-19. There were no significant differences between students who did and did not report each of these experiences for any of the mental health outcomes (depression, anxiety, and traumatic stress; Table 2).
Comparison of Mental Health by Stressful COVID-19 Experiences.
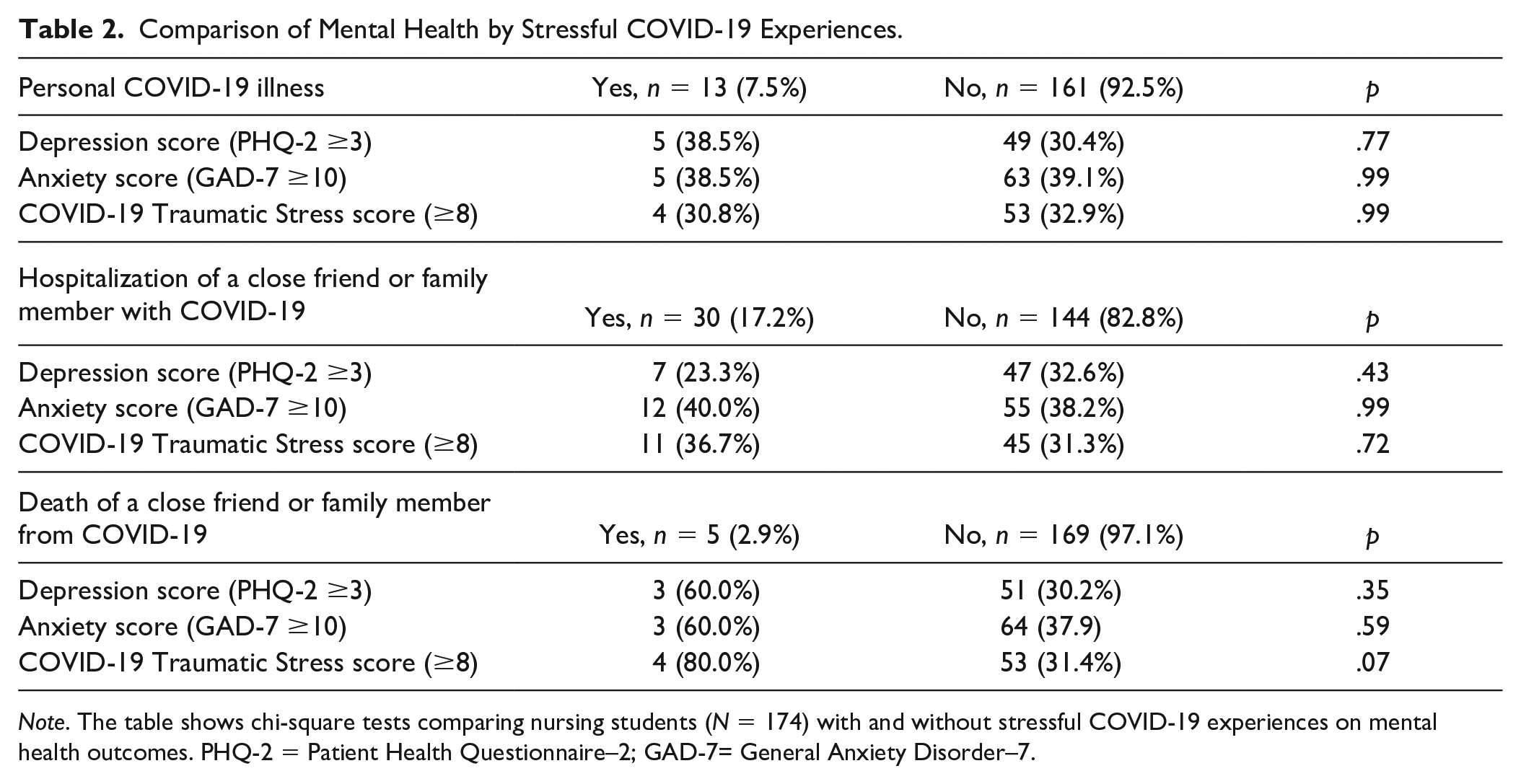
Note. The table shows chi-square tests comparing nursing students (N = 174) with and without stressful COVID-19 experiences on mental health outcomes. PHQ-2 = Patient Health Questionnaire–2; GAD-7= General Anxiety Disorder–7.
Mental Health Attributed to COVID-19
In adjusted models, there was no significant association between any stressful COVID-19 experiences (having COVID-19, hospitalization of a family member/friend, and death of a family member/friend) and having clinical-range depression risk attributed to COVID-19; having clinical-range anxiety risk attributed to COVID-19; or having high levels of COVID-19-related traumatic stress (Table 3). However, in the second set of models where risk/protective factors were added as predictors, loneliness scores and resilience scores were associated with all three outcomes. Higher loneliness scores were associated with higher odds of COVID-19-attributed depression (odds ratio [OR] = 1.64, 95% confidence interval [CI; 1.24, 2.16]); higher odds of COVID-19-attributed anxiety (OR = 1.40, 95% CI [1.10, 1.78]); and higher odds of COVID-19 traumatic stress (OR = 1.31, 95% CI [1.03, 1.67]). In contrast, higher resilience scores were associated with lower odds of COVID-19-attributed depression (OR = 0.50, 95% CI [0.26, 0.95]); lower odds of COVID-19-attributed anxiety (OR = 0.56, 95% CI [0.32, 0.98]); and lower odds of COVID-19 traumatic stress (OR = 0.55, 95% CI [0.31, 0.96]).
Associations Between Stressful COVID-19 Experiences and Mental Health.
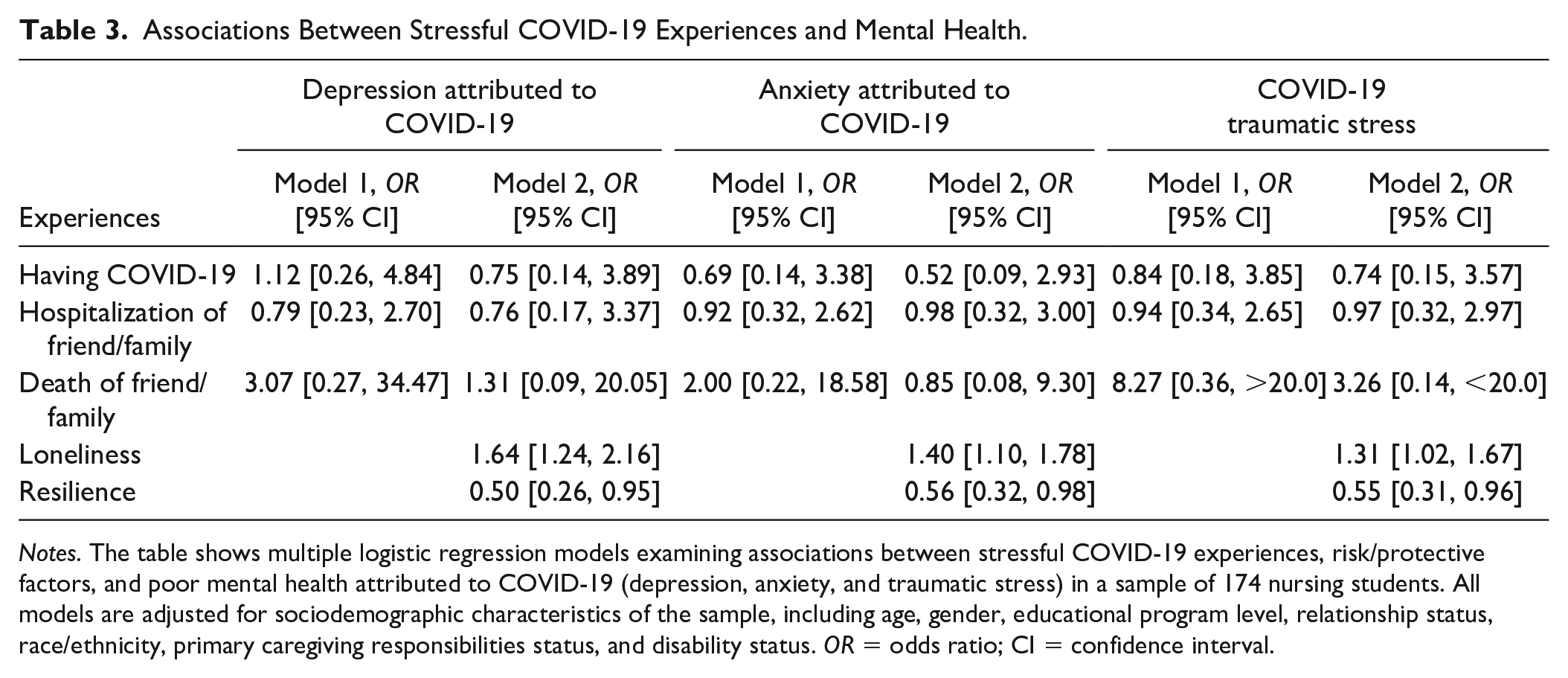
Notes. The table shows multiple logistic regression models examining associations between stressful COVID-19 experiences, risk/protective factors, and poor mental health attributed to COVID-19 (depression, anxiety, and traumatic stress) in a sample of 174 nursing students. All models are adjusted for sociodemographic characteristics of the sample, including age, gender, educational program level, relationship status, race/ethnicity, primary caregiving responsibilities status, and disability status. OR = odds ratio; CI = confidence interval.
Mental Health Service Utilization
We observed no significant relationship between any mental health variables (PHQ-2 score, GAD-7 score, and COVID-19 Traumatic Stress score) and utilization of campus mental health services in adjusted models (Table 4). There were also no relationships between these variables and utilization of noncampus mental health services. Two sociodemographic items had significant associations to service utilization outcomes. Being a primary caregiver to children or other dependents was associated with lower odds of utilization of campus mental health services (OR = 0.22, 95% CI [0.05, 0.87]). For noncampus mental health service utilization, those who identified their race/ethnicity as Asian American/Pacific Islander had lower odds of utilizing noncampus mental health services than their White/Caucasian counterparts (OR = 0.25, 95% CI [0.09, 0.70]).
Associations Between Mental Health Need and Mental Health Service Utilization.
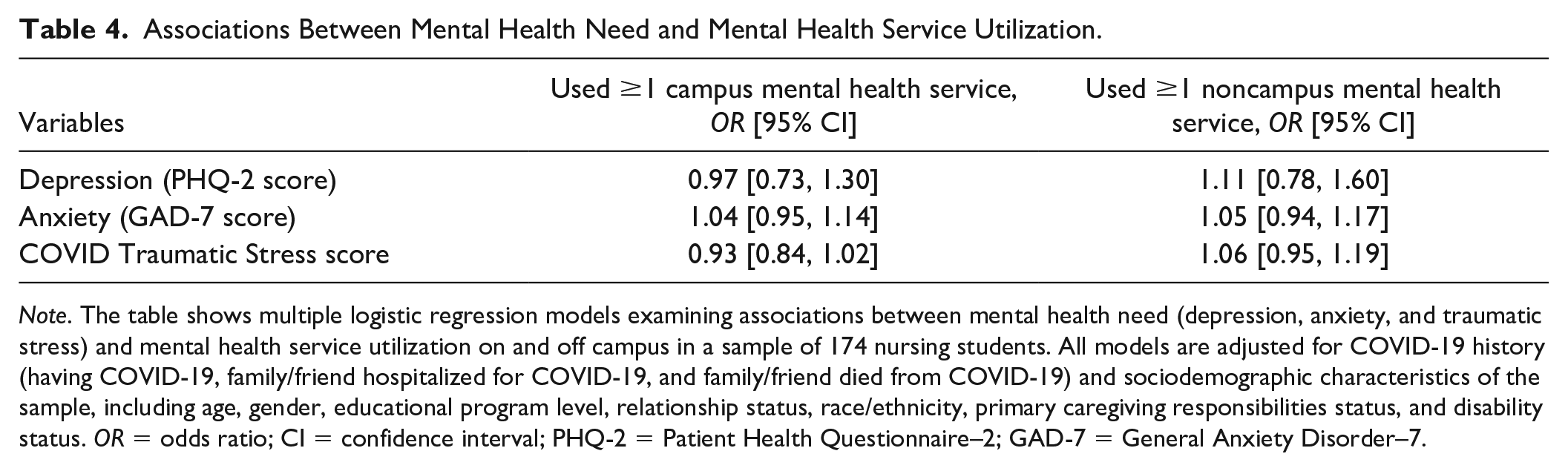
Note. The table shows multiple logistic regression models examining associations between mental health need (depression, anxiety, and traumatic stress) and mental health service utilization on and off campus in a sample of 174 nursing students. All models are adjusted for COVID-19 history (having COVID-19, family/friend hospitalized for COVID-19, and family/friend died from COVID-19) and sociodemographic characteristics of the sample, including age, gender, educational program level, relationship status, race/ethnicity, primary caregiving responsibilities status, and disability status. OR = odds ratio; CI = confidence interval; PHQ-2 = Patient Health Questionnaire–2; GAD-7 = General Anxiety Disorder–7.
Discussion
This study found elevated levels of depression, anxiety, and traumatic stress related to the COVID-19 pandemic among undergraduate and graduate nursing students in Los Angeles. Thirty percent of students had clinical-range depression scores, 37.9% of students had moderate or high anxiety, and 29.9% of students had high levels of COVID-19 traumatic stress, consistent with what has been observed with other college student samples during COVID-19 (Copeland et al., 2021; Son et al., 2020; Zimmermann et al., 2020). However, we found that stressful COVID-19 experiences did not have a relationship to mental health need. Neither testing positive for COVID-19, having a family member/friend hospitalization for COVID-19, nor having a family member/friend die from COVID-19 were associated with increased odds of any mental health problems. Higher self-reported levels of loneliness increased odds of having each mental health problem. Opposite of loneliness findings, having higher personal resilience decreased odds of each mental health problem. Our findings suggest that COVID-19 experiences, in and of themselves, may not necessarily have an association to mental distress—but that other risk/protective factors for mental health problems (e.g., loneliness and resilience) do in a pandemic context. In the stress literature, a negative subjective appraisal of potentially stressful events can be an important precursor to one’s ability to mobilize coping strategies, psychological symptoms, and psychiatric disorders (Brown et al., 2020; Thornton, 1992). Future studies should consider whether subjective appraisal of potentially stressful COVID-19 events has a relationship to mental health problems in this population.
Although many students reported having used campus and noncampus mental health services, we found no relationship between mental health need and service utilization on or off campus in adjusted models. Mental health service utilization among adults with clinical-range mental illness is known to be low in the United States (Park-Lee et al., 2012). The lack of relationship observed in this sample may suggest unmet need for mental health services, inadequate knowledge of mental health services, reliance on informal forms of mental health support (e.g., friends/family and faith), mental illness stigma, or other barriers to mental health service access among nursing students with the highest levels of need. This issue should be explored further in future research studies to identify pandemic-specific barriers and facilitators of mental health service use. For example, some pandemic circumstances like the rapid switch to telehealth may have facilitated mental health service access, while other circumstances like increased family, work, or personal responsibilities may have been barriers (Nicholas et al., 2021; Russell et al., 2020). We found that students who were primary caregivers to children or other dependents and students who identified as Asian American/Pacific Islander were less likely to use mental health services. This is consistent with recent evidence about the potential burden of caregiving/parenting during the COVID-19 pandemic as well as a large body of research indicating that Asian American/Pacific Islander populations may less likely to use mental health care than their White counterparts (Jang et al., 2019; Russell et al., 2020; Yang et al., 2020).
Our findings point to a need to provide specific support for the mental health of nursing students as well as the early careers of psychiatric nurses graduating during the COVID-19 pandemic. Universities and schools of nursing should consider targeted, accessible approaches to supporting student mental health, such as integrated student mental health services at campus health centers; information about campus mental health resources and accessibility issues (e.g., time offerings, insurance requirements, and telehealth options); and resilience-promoting programs. New graduate nurses who enter psychiatric practice settings may benefit from knowledge of occupational health support at their institutions of employment, mentorship from more experienced nurses, peer support, and provision of information on community mental health resources. Likewise, programs to bolster nurse resilience in their early practice may be useful. These individual-level supports should be accompanied by structural strategies in psychiatric practice settings to promote the mental well-being of nurses, such as safe working conditions and patient ratios, support for time off work, a trauma-informed work climate that acknowledges the potential for nurse vicarious trauma, and an organizational culture where new nurses feel valued and supported to advance their careers.
There are strengths and limitations to this study to consider in interpreting its findings. The study was cross-sectional and used a onetime, self-report survey. As such, we are unable to verify relationships over time, the direction of relationships, or objective mental health status of students sampled. Findings may not necessarily be generalizable to all nursing students in the United States, as the timing and impact of the COVID-19 pandemic differs by geographic area. We did not assess appraisal of potentially stressful COVID-19 experiences, potential barriers to mental health service utilization, remote learning experiences, student employment status, or mental health history. There were relatively few students who responded to our survey with children/dependents and with disabilities, and as such we could not perform subgroup analysis. Despite these limitations, there are also study strengths. We used a diverse sample of nursing students that was representative of the nursing student population at this university. The survey used validated measures of mental health, including a new measure of COVID-19-related traumatic stress. We assessed attribution of mental health responses to the COVID-19 pandemic and considered a variety of mental health treatment and promotion services on and off campus.
Nursing students in Los Angeles appear to have elevated rates of mental health problems during COVID-19, but mental health need was not related to use of mental health services. Strategies to promote mental health service awareness and access are especially important for nursing students who are primary caregivers to children or other dependents, and mental health services may require cultural tailoring for racial/ethnic groups that historically use fewer mental health services, such as Asian/Pacific Islander students in our survey. Given that loneliness was associated with increased risk for mental health problems and resilience with lower risk, nursing educators and administrators should also consider ways to promote social support/peer connection among students and foster resilience inside and outside of the classroom.
Footnotes
Acknowledgements
We are grateful for assistance from the UCLA School of Nursing Office of Student Affairs for their assistance in distributing our survey. Dr. Choi acknowledge K12 career development award support (K12HS26407-01) from the Agency for Healthcare Research and Quality (AHRQ) and the Patient-Centered Outcomes Research Institute (PCORI).
Author Contributions
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the UCLA School of Nursing.