
Abstract
Purpose
To describe the outcomes of a pharmacist-led multi-center, collaborative patient education and proactive adverse event management program in a community-based oncology setting.
Methods
Patients with EGFR mutation-positive (EGFRm+) non-small cell lung cancer, newly prescribed with oral afatinib, and monitored as part of the Florida Cancer Specialists patient management program, were included in a retrospective, observational analysis. During follow-up, data were collected on adverse event frequency, and changes in afatinib dosing. Data analyses were descriptive and exploratory in nature.
Results
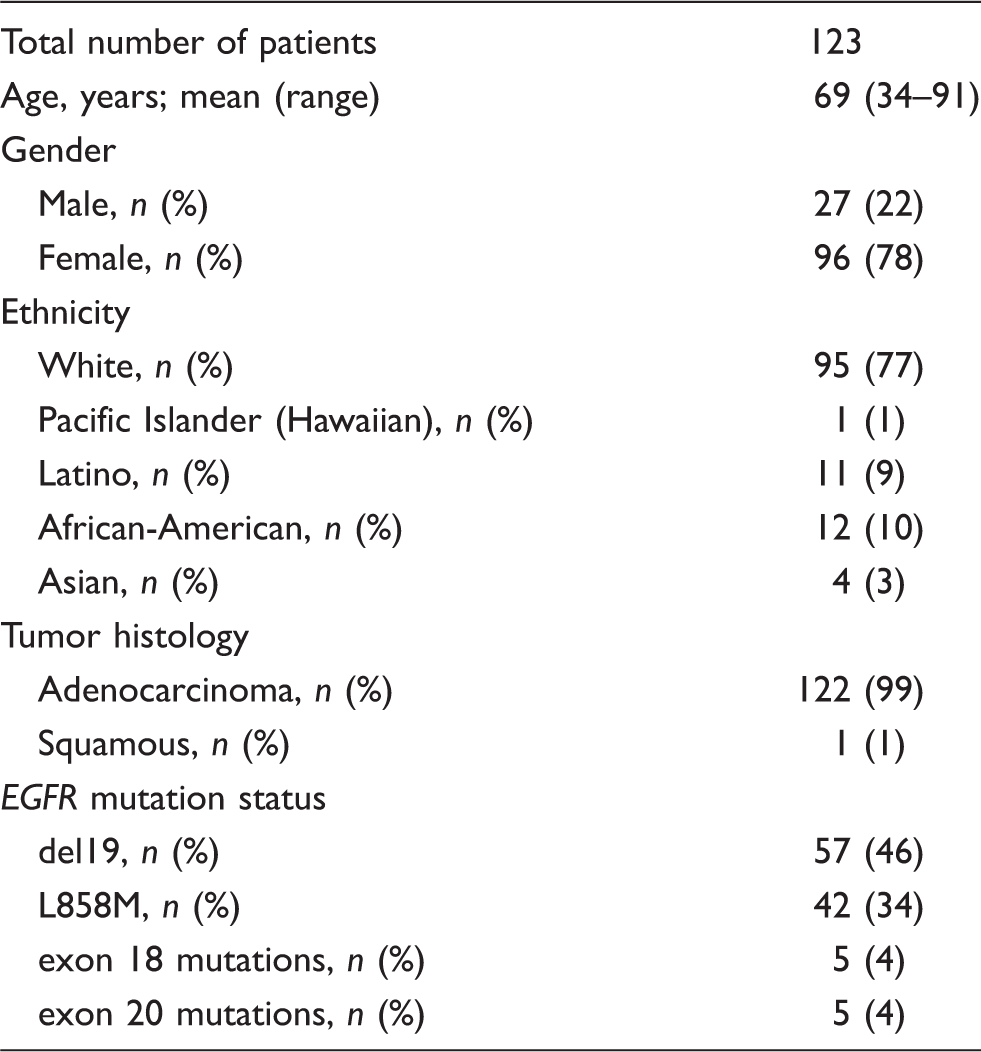
The mean age of the 123 patients included in the analysis was 69 years, and 78% were female. At the time of the analysis, 3 patients had discontinued before receiving treatment, 89 patients had discontinued afatinib treatment, and 31 patients were continuing to receive afatinib treatment. The most common afatinib-related adverse events were diarrhea (85%), rash/skin reactions (58%), stomatitis/mucositis (19%), and paronychia (16%). Overall, 13% of patients discontinued due to afatinib-related adverse events. The median duration of treatment was 4 months in patients who discontinued due to adverse events, 6 months in those who discontinued for other reasons, and 18 months in those who were continuing to receive therapy. Afatinib dose-reductions were more frequent in patients continuing treatment versus those who discontinued due to adverse events (77% vs. 42%, respectively).
Conclusions
Findings suggest that adverse events in patients with EGFRm + non-small cell lung cancer receiving afatinib can be successfully managed in a community-based, real-world setting with the help of collaborative pharmacist-led patient education, adverse event monitoring, and continuous support.
Introduction
Oral anticancer agents are increasingly used in the treatment of cancer, including non-small cell lung cancer (NSCLC). The first-generation oral epidermal growth factor receptor (EGFR) tyrosine-kinase inhibitors (TKIs), erlotinib and gefitinib, the second-generation TKI, afatinib, and the third-generation TKI, osimertinib, are approved treatment options for patients with EGFR mutation-positive (EGFRm+) metastatic NSCLC. EGFRm+ is typically seen in patients with adenocarcinoma histology. Afatinib is an irreversible ErbB family blocker that inhibits signaling from all ErbB family members (EGFR [ErbB1], HER2 [ErbB2], ErbB3, and ErbB4).1,2 The approval of afatinib in nonresistant EGFRm + metastatic NSCLC is based on significant progression-free survival (PFS) benefit versus chemotherapy in the phase 3 LUX-Lung 3 and LUX-Lung 6 studies.3,4 Pre-specified analyses of overall survival (OS) according to specific EGFR mutations showed improved OS among patients with the most common type of EGFR mutation, exon 19 deletions (del19), in each of these studies. 5 In the same treatment setting, first-line afatinib demonstrated significantly improved PFS and time-to-treatment failure (TTF) versus gefitinib in the phase 2b LUX-Lung 7 study. 6 Based on significant improvements in PFS and OS versus erlotinib in the phase 3 LUX-Lung 8 study, 7 afatinib has also been approved for patients with advanced squamous NSCLC whose disease had progressed after platinum-based chemotherapy.
EGFR TKIs have a favorable safety profile compared with chemotherapy. In the LUX-Lung clinical studies, the most common treatment-related AEs (any grade) with afatinib were diarrhea (88–95%), papulopustular (acneiform) rash (81–89%), stomatitis (52–72%), paronychia (33–57%) dry skin (29–33%), and decreased appetite (10–20%);3,4,6 despite these relatively high AE frequencies, discontinuation rates due to treatment-related AEs were relatively low (6–8%).3,4,6 The authors concluded that the use of proactive AE management approaches and the availability of a well-established and pre-defined tolerability-guided dose adjustment protocol for afatinib8,9 provide a strategy that can achieve successful management of the expected class effects of EGFR inhibition, thereby allowing patients to remain on treatment.3,4 The use of dose reductions (in 28–52% of patients)3,4,6 reduced the incidence and severity of AEs without negatively impacting progression-free survival in patients taking afatinib.10,11
Patients treated with oral chemotherapy agents have less frequent contact with medical providers, and consequently, patient safety, adherence, medication therapy monitoring, and timely follow-up can be compromised. 12 Outside the controlled environment of a clinical trial, patients and caregivers are responsible for ensuring adherence to treatment, and managing AEs between clinic visits, 13 but there is a need for patient education, close monitoring, and effective AE management strategies for patients receiving oral anticancer agents.14–18
Oncology pharmacists have the training and expertise to provide evidence-based care to cancer patients, including initial treatment decisions and subsequent therapeutic management, supportive care, and survivorship. 19 They often work with other health care providers to select the most appropriate therapy, evaluate the effects of drugs, monitor drug interactions, and manage adverse effects. 19 Because of their expert knowledge of anti-cancer medications and their adverse effects, they have a major role to play in educating other health care providers (nononcology pharmacists; nursing, pharmacy, and medical trainees; nurses and mid-level providers), 19 and are well placed to provide intervention and counseling to both patients and health care providers. 20 They are often involved in the development of clinical guidelines and other aspects of safe medication use and oncology practice. 19 Community-based oncology pharmacists play key roles within multidisciplinary teams involving nurses, oncologists, and primary care physicians, in delivering patient education and AE monitoring and management programs aimed at improving the management of AEs.13,17,19,21–23
Routine implementation of pharmacist-led drug monitoring programs has been shown to have a significant impact on clinical outcomes and health care costs of a number of chronic diseases.24,25 In oncology, a retrospective observational cohort study of a pharmacist-managed oral chemotherapy management clinic that provided services (including education on oral chemotherapy agents, concurrent medications, symptom management, and insurance assistance) to cancer patients for up to three months found that the program led to reductions in rates of adverse effects, non-adherence, drug interactions, and medication errors over time, as well as potential cost avoidance or cost savings. 26 In another study, pharmacist-mediated education and follow-up led to improvements in understanding of blood pressure monitoring among patients with metastatic renal cell carcinoma taking sunitinib, allowing a high relative dose intensity to be achieved. 27 Patients also appear to value pharmacist-led interventions in the oncology setting. Based on a survey of outpatients, 86% felt it important to discuss their initial treatment with a pharmacist, while 76% requested pharmacy follow-up at future visits; patients were interested in visiting a pharmacist regularly while receiving chemotherapy, and may be willing to pay for pharmacy counseling services. 28
Here we report the results of a retrospective, observational analysis of patients with EGFRm+ NSCLC treated with afatinib in community oncology clinics of the Florida Cancer Specialists (FCS) group, which comprises more than 95 clinics in the state of Florida. The FCS patient management program was developed to support patients' who are prescribed oral anticancer treatment, including oral afatinib. The objective of our analysis was to assess the outcomes of pharmacist-led patient education, AE monitoring and a proactive AE-management program.
Real-world studies of oral anticancer agents show that substantial numbers of patients (20–47%) are nonadherent,14,15,29,30 mainly due to AEs, and a lack of understanding by patients of the importance of taking their medication as prescribed.14–16,29,30 The FCS program addresses both of these issues by promoting a collaborative approach to AE education and management, and facilitating co-operation and teamwork between pharmacists, physicians, nurses, and patients themselves.
Methods
The Florida Cancer Specialists patient management program
The FCS patient management program was developed to support patients' prescribed oral anticancer treatment, including oral afatinib. All patients who began treatment with afatinib at FCS centers were asked if they wished to participate in the program, and to join weekly follow-up calls for up to eight weeks (Figure 1).This is a pharmacist-led program, in which patients beginning treatment with a new oral anticancer agent receive guidance on recommended dosing, administration and safe handling of the medication at home, as well as potential AEs. All patients received initial counseling from the pharmacists on dosing and AE management. In the case of afatinib, key AEs such as diarrhea, stomatitis/mucositis, rash/skin reactions, and paronychia were discussed with patients, including the expected time to onset (e.g. likelihood of diarrhea occurring during the first treatment cycle, paronychia after 2–3 cycles) and actions required for effective AE management.
Overview of the FCS patient management program, for patients newly prescribed with oral afatinib.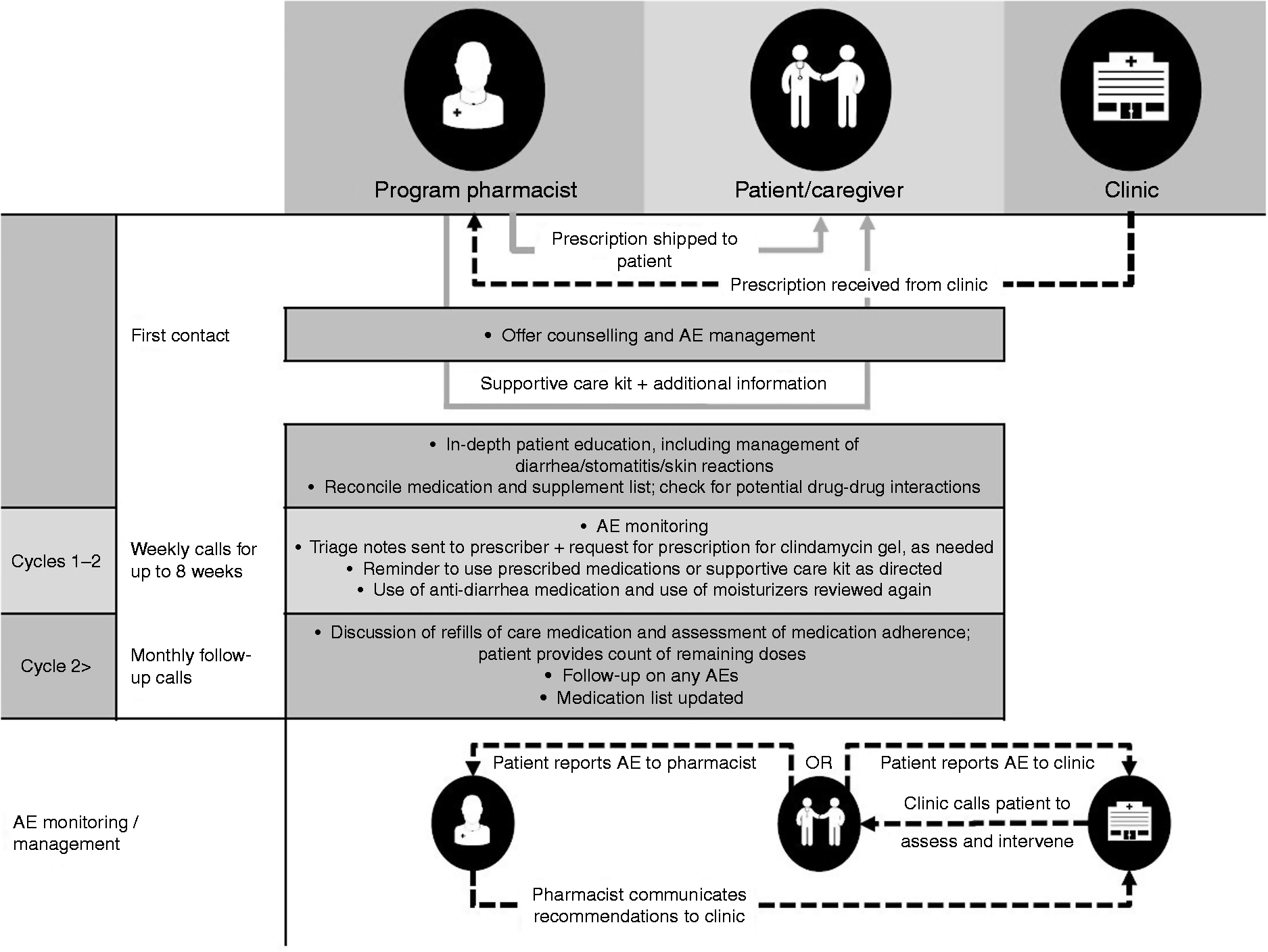
All recommendations made by the program pharmacists regarding adjusting or suspending the dose of afatinib were communicated to the prescribers' offices, and all decisions on such dose adjustments were made by the prescribers. When the pharmacists considered that a dose adjustment was required due to the occurrence of AEs, they also provided the prescriber with information on the use of tolerability-guided dose adjustments with afatinib, as described by Yang et al. 10 All decisions to discontinue treatment (due to the presence of an intolerable AE or another clinical outcome) were taken by the treating physician.
Use of supportive care kit and other medications
On joining the program, all patients received a complimentary supportive care kit from the pharmacy, containing: a moisturizing facial lotion for treatment/ prophylaxis of skin reactions; loperamide (Imodium®) tablets for diarrhea, together with verbal advice on the management of diarrhea. 31 The kits were supplied by Boehringer Ingelheim at no cost to the patients or to the program (a collaborative practice agreement was not required).
Weekly follow-up telephone calls with program pharmacists
As part of the FCS program, patients and caregivers are offered weekly follow-up telephone calls with a pharmacist for up to eight weeks from entering the program (Figure 1), in order to assess the patients' adherence to therapy, to monitor AEs, and to review the patient's current medication lists. During the calls, patients are reminded to use prescribed medications and/or the supportive care kit as directed, to help manage treatment-related AEs. After the first two treatment cycles, patients are contacted by the pharmacist on a monthly basis regarding care medication refills and further follow-up.
When the pharmacist felt that another OTC medication was needed, they advised the patient about the availability of the product for purchase from the local drug store. When they considered that a prescription medication was needed, they contacted the prescriber's office and made a recommendation for a prescription to be written.
Management of side-effects with afatinib: Role of the program pharmacists
In the event of AEs during use of afatinib, the program pharmacists provided specific recommendations on side-effect management (in accordance with the product label and the published literature), together with further follow-up (Figure 1). When prescription medications were required (e.g. clindamycin gel, doxycycline, minocycline, diphenoxylate and atropine, topical steroids), the pharmacist informed the clinic nurses and the prescribers and recommended a new prescription. When OTC medications such as loperamide or a skin moisturizer were required, the pharmacist provided the recommendation to the patient directly.
Diarrhea
The frequency of diarrhea was assessed routinely. When the pharmacist judged that the diarrhea was not adequately controlled, they would assess whether the patient had been using loperamide correctly. If they suspected that the patient had not been taking it as directed, they would repeat the advice to take the usual dose after each loose stool (this is a common challenge, as patients often fail to properly follow directions for taking loperamide). They might also provide a recommendation to the prescriber to add a prescription medication (diphenoxylate/ atropine). When a patient complained of severe diarrhea (i.e. occurring frequently; resistant to loperamide, diphenoxylate/atropine, and nonprescription medications) the pharmacist would refer them to the clinic for a follow-up visit, for hydration and further evaluation by their prescriber.
Rash
When a patient complained of rash, the pharmacist would encourage them to apply daily moisturizer and sunscreen. They may also refer them to their prescriber to be evaluated further and/or they would recommend a prescription for clindamycin gel and/or oral minocycline or doxycycline.
Stomatitis and paronychia
All patients were educated on the use of baking soda/salt rinses in the event of stomatitis and mucositis, 32 and on skin, hair, and nail care while using EGFR-targeted therapies, including the use of vinegar soaks and OTC topical steroids for paronychia. 33
When patients described having stomatitis, the pharmacist may recommend a prescription for an oral mucoadhesive or a specialized mouthwash (“magic mouthwash” (MMW)).
When patients complained of paronychia, the pharmacist would encourage them to apply a moisturizer daily. They would refer the patient to their prescriber or a dermatologist, and might recommend a prescription for topical silver nitrate, topical antibiotic, or topical steroids. Program pharmacists also provided information on the management of paronychia to the treating physicians, who were responsible for follow-up care.
Data collection and analysis
Data were collected from 1 May 2014 to 31 December 2016. Data for patients who had received a new prescription for afatinib and who had been monitored as part of the FCS patient management program were included in this retrospective, observational analysis.
Data collected at the start of afatinib treatment included age, gender, start date, starting dose, mutation type, and the number of previous lines of anticancer therapy.
During the follow-up calls, the frequency of AEs and any related treatments, and changes in afatinib dosing were recorded. Electronic medical records were also reviewed monthly for any relevant changes. Data collection continued until the medication was discontinued, at which point the reason for discontinuation was recorded. Data analyses were descriptive and exploratory in nature.
Assessing our internal practice, patient education, supportive care education, pharmacist interventions, plus general pharmacist to clinic communications is standard practice in this setting. As such, this observational study was Institutional Review Board exempt. Patient data handling was in line with data protection guidelines, so individual patient consent was not required.
Results
Patient population
Demographic and clinical characteristics of patients included in the analysis.
Management of adverse events
Management of afatinib-related AEs in patients involved in the FCS patient management program. a
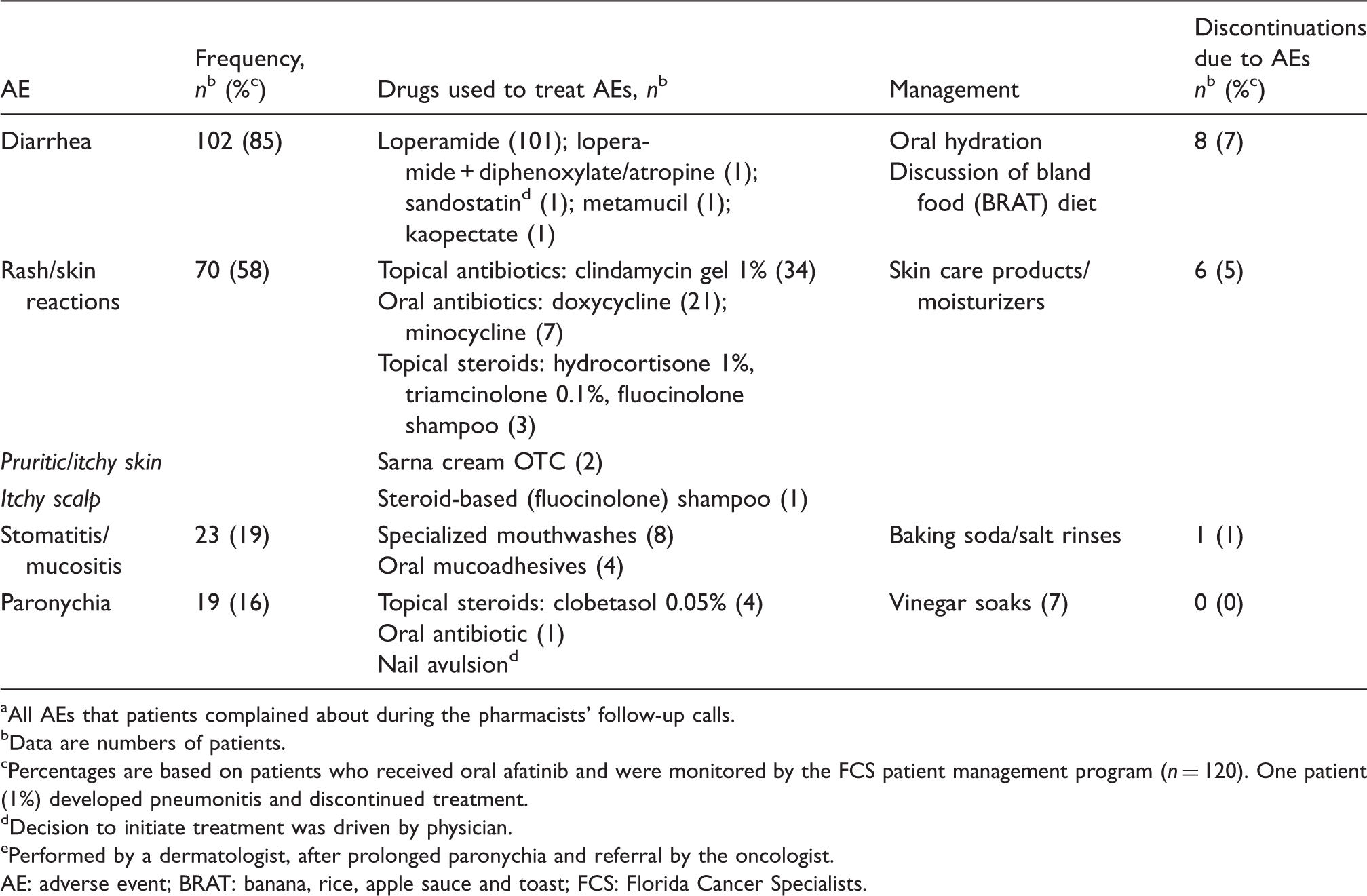
All AEs that patients complained about during the pharmacists' follow-up calls.
Data are numbers of patients.
Percentages are based on patients who received oral afatinib and were monitored by the FCS patient management program (n = 120). One patient (1%) developed pneumonitis and discontinued treatment.
Decision to initiate treatment was driven by physician.
Performed by a dermatologist, after prolonged paronychia and referral by the oncologist.
AE: adverse event; BRAT: banana, rice, apple sauce and toast; FCS: Florida Cancer Specialists.
The following examples show how specific AE management strategies were implemented by the pharmacists, for individuals with NSCLC who were treated within the program.
Patient 1: Rash/skin reaction
A 71-year-old man had been taking afatinib 40 mg/day p.o. for three weeks. At that time, during his follow-up call with the pharmacist, he mentioned that he had developed acne on his face, his nose being the most affected area. He stated that he had been using a moisturizer when he remembered to do so. The pharmacist discussed with the patient the importance of moisturizing daily, and of using a sunscreen. At the recommendation of the pharmacist, the oncologist sent a prescription of topical clindamycin gel to the patient's local pharmacy.
During the next follow-up call the patient complained that, although he had been using the clindamycin gel as directed, the rash had not resolved, and his nose was unbearably painful and swollen, with “too many pimples to count”. A triage note was sent to the physician's office with a recommendation to contact the patient and suspend afatinib dosing for seven days, or until the patient was able to tolerate the rash, and then to resume afatinib at 30 mg/day p.o., and at the same time to begin treatment with minocycline 100 mg b.i.d. p.o.. The physician agreed, and advised the patient accordingly. He was also advised to continue using moisturizer and sunscreen, and topical clindamycin b.i.d. as needed. During the follow-up call two weeks later, the patient told the pharmacist that the rash had resolved after he stopped taking afatinib. He subsequently resumed treatment at the lower dose of 30 mg/day, which he was able to tolerate. The pharmacist advised him to use the oral and topical antibiotics that had been provided to treat flare-ups of the rash. He continued to take afatinib until disease progression occurred two years later.
Patient 2: Paronychia
A 63-year-old man had been taking afatinib 30 mg/day for seven months. He called the pharmacy and complained that he had a problem with his fingers. He told the pharmacist that his cuticles were red, swollen, and irritated and complained that they were sensitive, and that his fingers cracked and bled easily. He had been using an OTC topical triple antibiotic cream. The pharmacist recommended that he soak his cuticles with equal parts of vinegar and water for 15 min to prevent infection. An appointment was scheduled for him to see his oncologist, who then prescribed an oral antibiotic.
Discontinuations from treatment
Table 2 also shows the numbers and percentages of patients who discontinued afatinib therapy. Overall, sixteen patients (13%) discontinued afatinib treatment due to an AE thought to be related to afatinib, the most common being diarrhea (n = 8; 7%) and rash/skin reactions (n = 6; 5%); other AEs that led to discontinuation were stomatitis and pneumonitis (both n = 1; 1%).
Pharmacist interventions (recommended/accepted) for afatinib-related AEs in patients who remained on treatment (“ongoing”), versus those who had discontinued due to an AE.
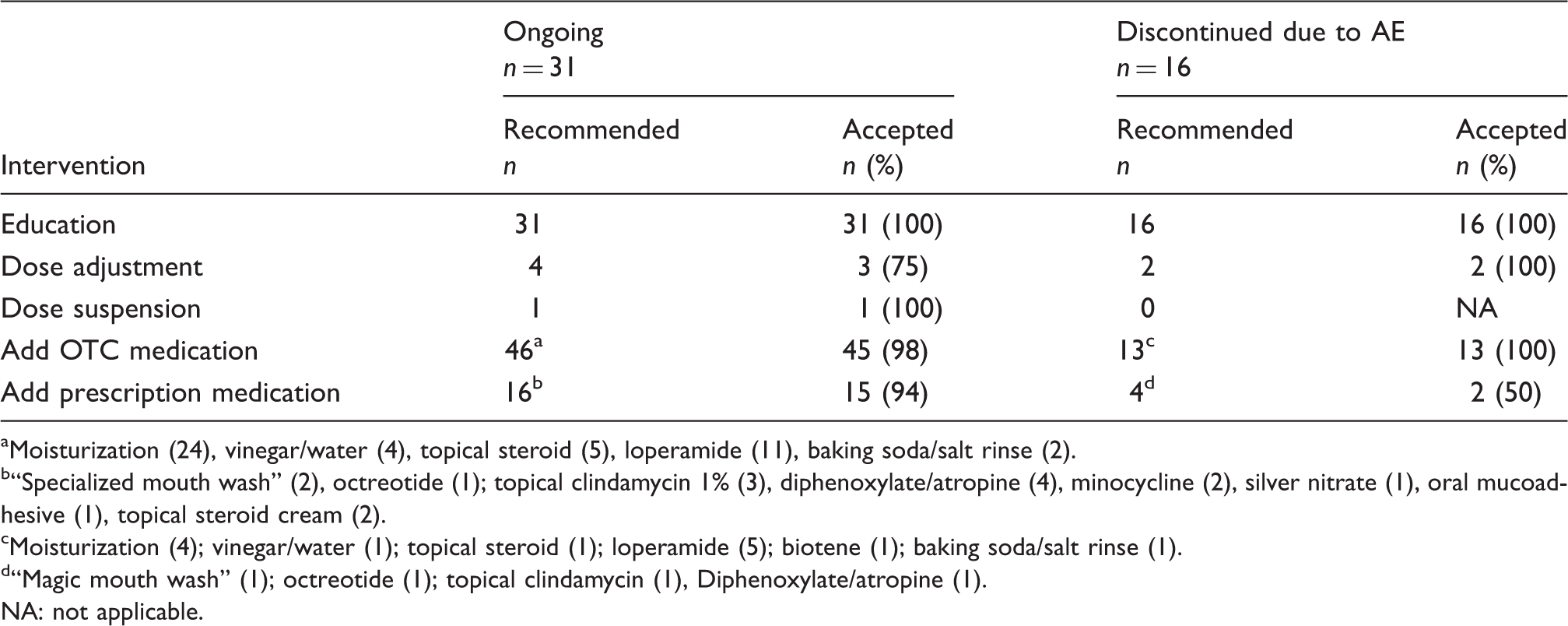
Moisturization (24), vinegar/water (4), topical steroid (5), loperamide (11), baking soda/salt rinse (2).
“Specialized mouth wash” (2), octreotide (1); topical clindamycin 1% (3), diphenoxylate/atropine (4), minocycline (2), silver nitrate (1), oral mucoadhesive (1), topical steroid cream (2).
Moisturization (4); vinegar/water (1); topical steroid (1); loperamide (5); biotene (1); baking soda/salt rinse (1).
“Magic mouth wash” (1); octreotide (1); topical clindamycin (1), Diphenoxylate/atropine (1).
NA: not applicable.
The median duration of treatment in the group that discontinued treatment due to afatinib-related AEs was 4 months (range: 1–13 months), compared with 6 months (range: 1–31 months) in the group that had discontinued afatinib due to reasons other than AEs (n = 73), and 18 months (range: 8−37 months) in the “ongoing” patients who remained on therapy at the time of the analysis.
The most common reason for discontinuation overall was disease progression (n = 45/120; 38%). Another 23 patients (19%) died during the follow-up period (all due to progressive disease) and five patients (4%) discontinued for administrative reasons.
Dose reductions
Final afatinib dose in “ongoing” patients continuing treatment versus patients who discontinued due to AEs.
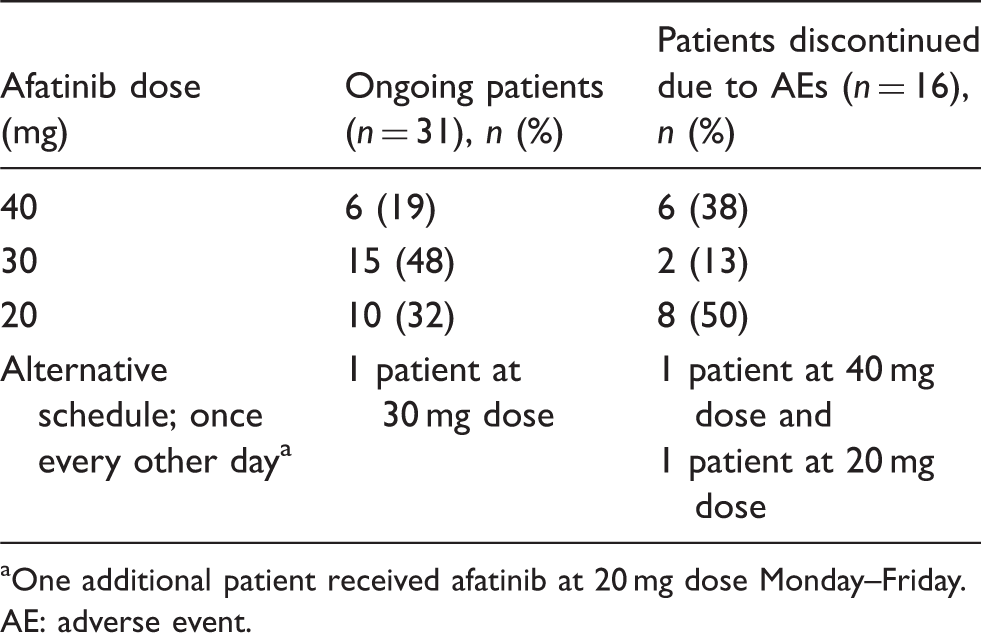
One additional patient received afatinib at 20 mg dose Monday–Friday.
AE: adverse event.
Discussion
In this real-world analysis, the AEs that patients taking afatinib mentioned to the program pharmacists were diarrhea (85%), rash/skin reactions (58%), stomatitis/mucositis (19%), and paronychia (16%). In general, these AEs were managed successfully, as indicated by the relatively low proportion of patients that discontinued afatinib due to an AE (13% overall). Although this is higher than the rates previously reported for afatinib in randomized clinical trials (6−8%),3,4,6 it shows that among patients who developed an afatinib-related AE, the large majority were able to remain on treatment for the duration of the analysis, which indicates that such AEs can be effectively managed outside of the controlled setting of the clinical trial.
The FCS program relies on pharmacist-led patient education, close monitoring and a proactive management approach that includes appropriate dose adjustments in response to the specific AEs experienced by individual patients. The value of the program to patients is indicated by the high acceptance rates for most of the interventions offered. In particular, patient education was generally welcomed and well received. Recommendations for OTC products were also well received and incorporated into the patients' care plans (pharmacists are well accustomed to making recommendations about OTC products based on the published literature or supportive care guidelines). Recommendations for prescription medications were also accepted by a large majority of patients (85% overall), despite the fact that such recommendations were often required after an OTC medication had been tried. Pharmacists made recommendations for dose adjustments/suspensions less often, perhaps because they expected patients to be hesitant about lowering the dose, due to concerns about a reduction in clinical benefit. In fact, previous studies have demonstrated that tolerability-guided dose adjustment can ameliorate AEs during use of afatinib without affecting therapeutic efficacy. 10 In the current analysis, only one of seven patients did not accept the pharmacists' recommendation of a dose adjustment or dose suspension (in all cases, the decision whether to implement the pharmacist’s recommendation was made by the physician). In our experience, continuous support provided by the pharmacists enabled patients to manage their AEs more successfully and to remain on treatment for longer.
Diarrhea (generally mild in intensity) is commonly experienced by patients during use of afatinib.3,4,6 In the current analysis, the relatively low rate of discontinuations attributed to diarrhea (7%) indicates that, among patients who initially complained of diarrhea, the use of anti-motility agents had been effective in reducing its severity, while the patient education and reinforcement strategies provided had enabled the patients to manage and tolerate the side-effect, and to remain on treatment. Similarly, rates of discontinuation due to rash, stomatitis /mucositis and paronychia were less than 5%. The fact that a larger proportion of patients in the “ongoing” group (74%) than the “discontinued due to AEs” group (56%) had a dose reduction also suggests that the use of tolerability-guided dose adjustments had helped patients to remain on afatinib treatment.
As shown in previous real-world studies,17,20,26,27,34–36 continuous follow-up with patients or caregivers is an essential aspect of successfully managing AEs in community settings. However, based on our interactions with patients in the FCS program, we concluded that provision of comprehensive education and support materials at the start of treatment was not sufficient for some individuals. Some patients either forgot how to manage their AEs soon after the start of treatment or remained unsure after their first meetings with the pharmacist, so needed continued support and education. For example, some patients required repeated reminders about taking antidiarrheal medications correctly and as prescribed. Patients can be overwhelmed by the amount of education and information initially provided by the clinic, and may experience significant anxiety, leading to poor retention and understanding of the advice and clinical information provided. 37 This underlines the importance of regular follow-up and reinforcement of AE reporting and management. In this regard, the follow-up phone calls that are offered as part of the FCS patient management program provide a point of contact for patients who may otherwise feel overwhelmed by their disease and the responsibilities of treatment. 13
Another observation from the FCS patient management program was that there is a clear need for a formal education platform for physicians and nurses, on the topic of supportive care in the management of AEs related to new oral anticancer agents (in particular, the management and treatment of rash/skin reactions, which is generally overseen by dermatologists). Our experience based on implementing the program and working with prescribers was that their understanding of how to successfully manage patients receiving afatinib improved over time, and with increased experience with the drug and its side-effects.
The educational efforts at FCS are an ongoing process. Current initiatives include, but are not limited to, the attendance of national oncology conferences by physicians, physician extenders, and pharmacists. Internal initiatives include: use of publications by pharmacists to inform prescribers about the management of AEs (via email or triage notes in the patient's electronic medical records); use of monthly electronic newsletters containing articles and video presentations on related topics; and presentations by nurse educators, and educational programs for nurses in the clinic and the oncology care management nursing team. In addition, the FCS is planning an internal educational website for FCS clinic use, which will include an educational supportive care section for health care providers.
The limitations of the current analysis relate to the retrospective, observational nature of the study. Because the study was conducted retrospectively, it was impossible for us to determine the information that would be collected. For example, we were unable to evaluate the impact of the program on the severity of side-effects, because the clinics did not evaluate or record AE severity in a systematic manner (in our experience, it would be unusual for this to happen in day-to-day clinical practice). Moreover, because the program was delivered via a centralized call center, it was impossible for the program pharmacists to evaluate the severity of AEs such as acneiform skin reactions, stomatitis, and paronychia (patients who complained of such adverse events were routinely referred back to the clinics for further evaluation). Although the pharmacists provided education to patients on the importance of adherence to their medication, information on adherence to afatinib were not recorded systematically in a form that could be analyzed. Finally, the lack of a comparison group limits the conclusions that can be drawn with regard to the impact of the program on patient outcomes.
A successful approach to AE management can help to maintain patients' adherence to treatment without limiting therapeutic efficacy or treatment duration. By allowing patients to remain on EGFR TKI therapy for as long as they continue to experience clinical benefit, patient outcomes may be optimized. This retrospective, observational analysis suggests that the use of pharmacist-led patient education, AE monitoring and continuous support may contribute to the management of afatinib-related AEs in a real-world, community setting.
The FCS program was designed specifically to manage AEs that occurred during use of afatinib, but many of the principles and approaches could be implemented for patients treated with other types of medication. The goals of AE management are often similar, particularly for disease states in which long-term adherence to medication is essential, but medication side-effects can have a negative effect on adherence, if not adequately managed. In such cases, ensuring that the patient continues to take their medication is likely to require regular follow-up, and the development of a collaborative, supportive relationship between the patient and their health care providers. Many practitioners can speak to the impact they have made in daily practice, by encouraging their patients to take their medications regularly and as prescribed, and by means of targeted assessment and proactive management of AEs, the aim of which is to not only treat the AEs, but also to help patients to tolerate their prescribed medication, thereby allowing them to continue on treatment for longer, at dose that provides them with clinical benefits.
Footnotes
Acknowledgements
The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors. The authors received no direct compensation related to the development of the article. The authors were fully responsible for all content and editorial decisions, were involved at all stages of the article development, and have approved the final version. Writing, editorial support, and/or formatting assistance was provided by Sarah Maloney, PhD, of GeoMed, an Ashfield company, part of UDG Healthcare plc, which was contracted and funded by Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI). BIPI was given the opportunity to review the article for medical and scientific accuracy as well as intellectual property considerations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.