
Abstract
Background
Patients with cancer have an elevated risk of venous thromboembolism. Importantly, patients with cancer, who have metastatic disease, renal insufficiency, or are receiving anticancer therapy, have an even higher risk of a recurrent event. Similarly, the risk of recurrent venous thromboembolism is higher than the risk of an initial event. To reduce the risk, extended duration of prophylaxis for up to six months with low-molecular-weight heparins such as dalteparin, enoxaparin, nadroparin, and tinzaparin is recommended by international guidelines. In this paper, the clinical and economic literature is reviewed to provide evidenced based recommendations based on clinical benefit and economic value.
Methods
A systematic review of major databases was conducted from January 1996 to October 2016 for randomized controlled trials evaluating the four distinct low-molecular-weight heparins against a vitamin K antagonists control group for the prevention of recurrent venous thromboembolism in patients with active cancer. This was then followed by the application of the National Institute of Health and Clinical Excellence guidance to assess the quality of all trials that met the inclusion criteria. Finally, the cost-effectiveness literature supporting the value proposition of each product was reviewed.
Results
Six randomized trials met the inclusion criteria. There were one, two, and three trials that compared dalteparin, tinzaparin, and enoxaparin to a vitamin K antagonists control group. However, there were no trials for nadroparin in the setting of secondary venous thromboembolism prevention. In addition, only the dalteparin and one of the tinzaparin trials were of high quality and adequately powered. Of the two studies, only the dalteparin trial reported a statistically significant benefit in terms of venous thromboembolism absolute risk reduction when compared to a vitamin K antagonists control group (HR = 0.48; p = 0.002). In addition, there was robust pharmacoeconomic data from Canada, the Netherlands, France, and Austria supporting the cost-effectiveness of dalteparin for this indication. There were no such studies for any of the other agents.
Conclusions
The totality of high-quality clinical and cost-effectiveness data supports the use of dalteparin over other low-molecular-weight heparins for preventing recurrent venous thromboembolism in patients with cancer.
Introduction
Low-molecular-weight heparins (LMWHs), which include nadroparin, dalteparin, enoxaparin, and tinzaparin, have been used in the prevention and treatment of venous thromboembolism (VTE) for over 20 years. 1 These unique drugs have a long history in terms of safety and efficacy in a broad range of indications including VTE prophylaxis after orthopedic surgery, other elective surgeries, and in acutely ill medical patients with restricted mobility.2–4 Some LMWHs have also been shown to be cost-effective alternatives to unfractionated heparin and vitamin K antagonists (VKA) across the approved indications.5–7
One patient population that is particularly vulnerable to the development of deep vein thrombosis (DVT) and subsequent pulmonary embolism (PE) are patients with an active cancer. 8 From one epidemiologic study, it was estimated that approximately 15% of all patients with cancer will develop VTE during their disease period. 9 Notably, patients with cancer who have metastatic disease, renal insufficiency, or are receiving antineoplastic medication or radiotherapy demonstrate an even higher risk of suffering a thrombotic event. 10 Once an initial VTE develops and is adequately managed, patients with cancer are at an increased risk for a secondary event. Therefore, the American College of Chest Physicians advocates secondary prophylaxis in outpatients with cancer. 11 Of the available agents, international guidelines recommended the LMWH over VKA based on a lower risk of VTE recurrence,12,13 which was suggested by one large randomized trial evaluating dalteparin and a meta-analysis.14,15 However, the guidelines made no distinction between dalteparin, enoxaparin, nadroparin, and tinzaparin, the primary agents that are available in the United States and Europe. In this paper, the clinical and economic literature was reviewed to develop an evidence base for making recommendations for secondary VTE prophylaxis in cancer patients based on clinical benefit and economic value. The paper will then review the available data in patients with moderate to severe renal impairment, a patient subgroup that is of clinical concern to practicing oncologists.
Methods
Systematic review of the literature
A computer literature search of PubMed, Embase, the Cochrane Database, and Google Scholar was conducted from 1 January 1996 to 31 October 2016 for published randomized trials evaluating the extended duration of dalteparin, enoxaparin, nadroparin, or tinzaparin against a VKA control group for secondary VTE prevention in cancer patients. Search terms consisted of “{VTE} OR {DVT} OR {PE} AND {cancer} OR {metastatic cancer} OR {dalteparin} OR {enoxaparin} OR {tinzaparin} OR {nadroparin} AND {VKA} AND {randomized clinical trial} AND {extended duration} AND {recurrent} OR {secondary prophylaxis}”. The new oral factor Xa inhibitors were not included in the comparison, because these agents are still investigational in cancer patients.
Eligibility criteria regarding the validity of trial design and analysis were used to identify potential studies. To be eligible, studies must have used a randomized design with at least 25 patients enrolled into each group. Patients must have been adults, 18 years of age or older, with cancer and a newly diagnosed initial VTE. One of the trial arms must have been between extended dalteparin, enoxaparin, or tinzaparin, with a VKA as the control arm. Extended duration must have been at least three months of therapy. Unpublished randomized trials presented in abstract form at professional meetings were not eligible unless access to full study reports was available. Care was taken to avoid inclusion of duplicate publications.
Once trials meeting the inclusion criteria were identified, the following data were extracted: sample size, year of publication, drug regimen, dosage, definition of primary and secondary endpoints, trial duration, planned treatment duration, number of major bleeding events, number of withdrawals from the study, all-cause mortality, and all relevant clinical outcomes.
Assessment of study quality
The checklist for randomized trials developed by the National Institute of Health and Clinical Excellence (NICE) was used to assess the quality of all trials that met the inclusion criteria. 16 The NICE checklist consists of seven questions related to study quality and is considered reliable and valid. Randomized trials that did not meet at least four of the seven quality criteria were excluded from the analysis.
Review of published economic evaluations
A second literature review for published economic evaluations of dalteparin, enoxaparin, nadroparin, or tinzaparin for the secondary prevention of VTE in cancer patients was also undertaken. The review was limited to English language studies that used either a cost-effectiveness or cost-utility design and reported the primary outcome as an incremental cost per VTE avoided or quality-adjusted life year (QALY). The review focused on these endpoints because they would allow the economic value to be compared across the four agents.
Results
A total of 361 citations were identified and reviewed. A total of six randomized trials meeting the inclusion criteria were appropriate for closer examination. Reasons for study rejection included other indications evaluated, duplicate publications or review articles, did not evaluate secondary VTE prophylaxis, evaluated other agents under investigation, or trial was not relevant to the current analysis (Figure 1). VKA were the control group in all six trials and the treatment duration ranged from three to six months (Table 1). There was one, two, and three trials with dalteparin, tinzaparin, and enoxaparin in the experimental arm, respectively.14,17–21 There were no trials for nadroparin in the setting of secondary VTE prevention. Patients enrolled into each trial were comparable with respect to mean age and in at least three of the trials, patients were diagnosed with an active cancer or were receiving treatment within six months of enrollment (Table 1). However, the status of the cancer was unclear in three of the trials.
Consort diagram of study selection. Randomized trials of secondary VTE prophylaxis in cancer patients. VTE: venous thromboembolism; VKA: vitamin K antagonists; D: dalteparin; E: enoxaparin; T: tinzaparin; D/C: discontinuation; Dx: diagnosis; Tx: treatment; NR: not reported. These data were from a cancer patient subgroup, which was part of a larger study population.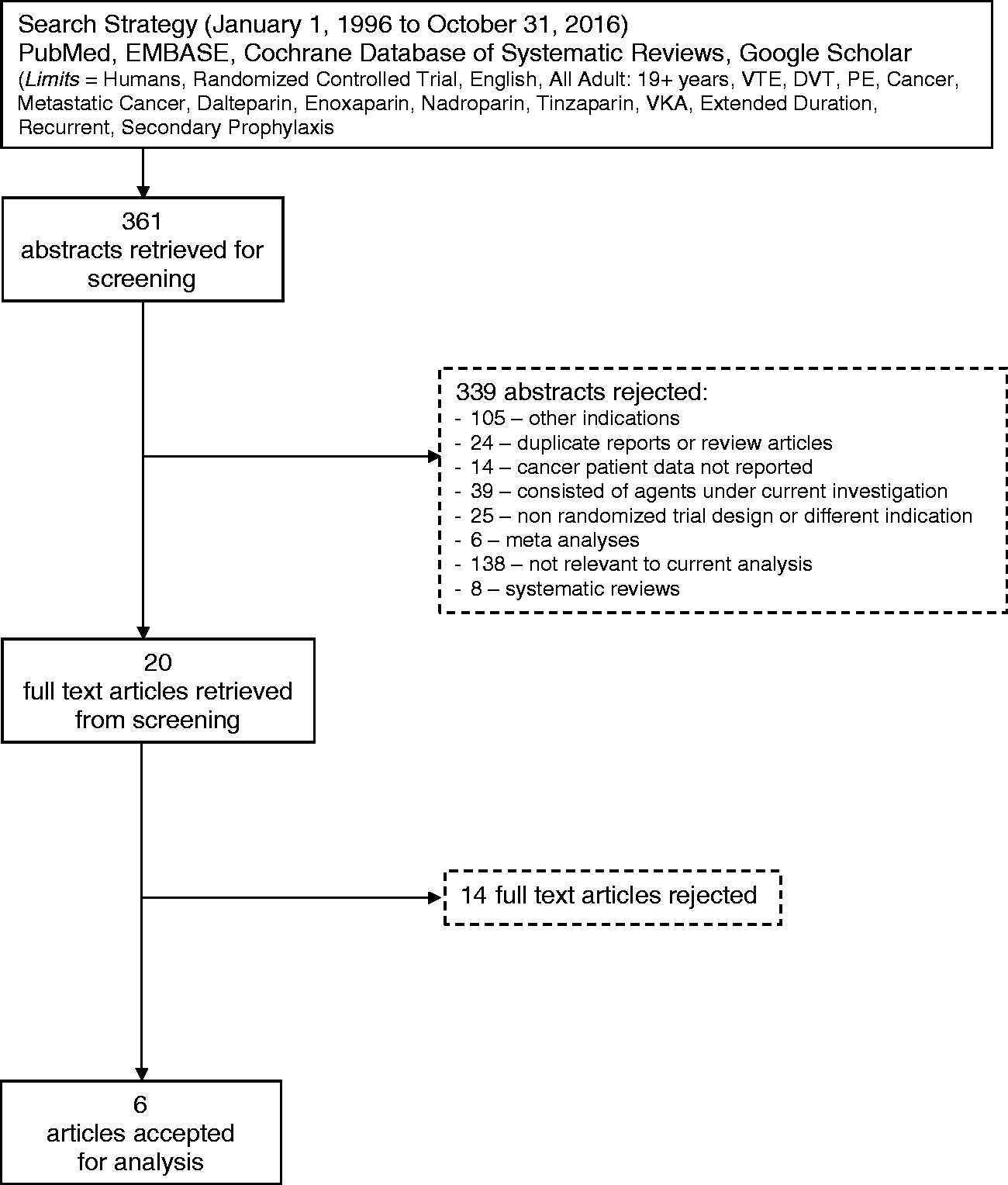
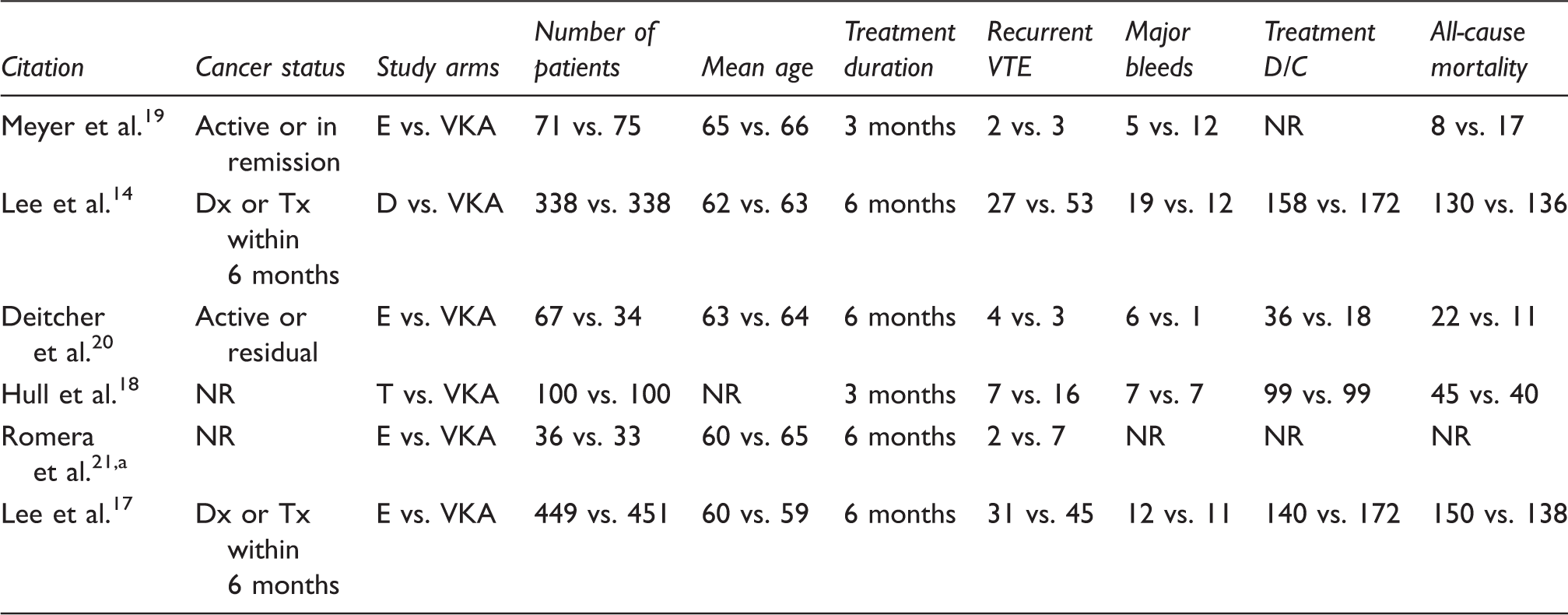
The study quality ranged from moderate to high quality (Appendix 1). Except for the multinational trials that evaluated dalteparin and tinzaparin,14,17 most of the studies were small and underpowered to adequately evaluate the primary endpoint. Furthermore, the data reported by Romera et al. were from a cancer-patient subgroup that was part of a larger study population. 21
The trial evaluating dalteparin was the multinational (Comparison of Low-Molecular-Weight Heparin versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer) CLOT study. Patients were randomized to receive dalteparin (200 IU/kg SC once daily in the first month, then 150 IU/kg SC once daily from months 2 to 6) or 5–7 days of dalteparin (200 IU/kg SC once daily) overlapped with and followed by an oral VKA for six months. Over the course of the study, 676 cancer patients with newly diagnosed VTE were enrolled. The trial met its primary endpoint. By the end of the study, 27 of 336 (8.0%) patients in the dalteparin group developed recurrent VTE compared to 53 of 336 (15.8%) in the VKA control group (HR = 0.48; 95% CI: 0.30–0.77; p = 0.002). Safety was comparable between groups with no significant differences in major bleeding events (dalteparin = 6% vs. VKA = 4%; p = 0.27). 14
Patients with renal insufficiency are a subpopulation of special interest to the practicing oncologist because of increased risks for VTE recurrent and major bleeding events. In a post hoc subgroup analysis of the CLOT trial, Woodruff et al. evaluated patients who had moderate (CrCl 30–59 mL/min) to severe (CrCl 15–29 mL/min) renal impairment at randomization. 22 The findings revealed that patients treated with dalteparin had lower absolute rates of recurrent VTE than those in the VKA group (3% vs. 17%; p = 0.011), while the frequency of major bleeding was similar between subgroups (2.0% vs. 2.4%; p = 0.46). 22
The second adequately powered study compared extended duration of tinzaparin, an LMWH that differs from dalteparin to VKA for the secondary prevention of VTE in patients with cancer. In that trial, 900 patients were randomized 1 to 1 to receive tinzaparin once daily for six months or to a warfarin (overlapping with tinzaparin, 175 IU/kg, once daily for the first 5 to 10 days) for the same duration of time. 17 The trial did not meet its primary endpoint, even though the high initial dose of tinzaparin was specifically maintained in the experimental group over the six-month course of the study.
Overall, 31 of 449 patients in the tinzaparin group developed a recurrent VTE compared to 45 of 451 patients in the warfarin group (HR = 0.65; 95% CI: 0.41–1.03; p = 0.07). Differences in major bleeding were not significantly different between groups (HR = 0.89; 95% CI: 0.40–1.99; p = 0.77). 17 It was also interesting to note than in a subgroup analysis in patients with renal impairment (representing 15% of study population), there were no statistically significant differences in reported VTE between the tinzaparin and warfarin groups (RR = 0.93; 95% CI: 0.39–2.18). 23 Therefore, based on the available data, it appears that dalteparin is the only LMWH to have demonstrated superior efficacy in terms of VTE recurrence in patients with cancer and especially in those with moderate to severe renal impairment.
The older VKA required routine monitoring of international normalized ratio (INR) levels. LMWH do not affect INR. Therefore, there is no clinical benefit from INR monitoring. Anti-Xa monitoring on the other hand may have clinical utility when used in patient subgroups who are at risk. 24 These include patients with renal impairment (creatinine clearance = 30–50 mL/min) and in patients who are at extremes of weight (less than 45 kg or greater than 130 or 150 kg). Of note, the routine use of such monitoring remains controversial and there are no published guidelines to guide pharmacotherapy.24,25 Therefore, monitoring anti-Xa is generally not necessary but should be considered for specific patient populations.
Studies evaluating the economic value of LMWH in cancer patients
The review of the economic literature did not find any economic evaluations of enoxaparin, nadroparin, or tinzaparin for secondary VTE prevention in cancer patients. However, five cost-effectiveness analyses were identified for dalteparin.7,26–28 All the economic analyses were patient-level cost-effectiveness and cost-utility studies using resource-use data that was collected during the CLOT randomized trial.
Summary of economic evaluations of dalteparin for the prevention of secondary VTE in patients with cancer.

QALY: quality-adjusted life year; VTE: venous thromboembolic event; NR: not reported.
Using the CLOT trial database, similar analyses were recently conducted from the health care system perspectives of the Netherlands, France, and Austria for all patients and for patients with renal impairment. Considering the cost per VTE as an endpoint, dalteparin had incremental costs that ranged from €8400 in the case of the Netherlands to €11,800 for France.7,26 Using the alternative endpoint, dalteparin had an incremental cost per QALY gained that ranged from €4700 to €6600 (Table 2). The main driver behind these inter-country differences was the cost of both drugs and DVT/PE management patterns in the individual countries.
Evaluations were also conducted in patients with moderate to severe renal impairment that were treated within the CLOT trial (which was not conducted in the original 2005 Canadian analysis). The findings revealed that for all country-specific analyses, the incremental cost per VTE avoided and QALY gained was reduced, suggesting enhanced economic value in the renal subgroup (Table 2). The primary factor responsible for this improvement was the enhanced efficacy of dalteparin in terms of VTE risk reduction compared to VKA.
Discussion
LMWHs have been used based on evidence, or empirically, for over 10 years in the acute treatment and secondary prevention of VTE in patients with cancer. The recommendation by American Society of Clinical Oncology (ASCO) and European Society of Medical Oncology (ESMO) is for an LMWH for the initial 5–10 days of treatment of an established DVT and PE, followed by long-term secondary prophylaxis for at least six months.11,12 The guidelines do not distinguish between agents and assume comparative safety and efficacy. But the LMWH are not alike, with differences in chemical characteristics and pharmacodynamic properties. 29 Therefore, in the absence of direct head-to-head data from randomized trials, the findings from individual trials must be used to select the agent with the best data to support efficacy, safety, and cost-effectiveness for optimal patient care.
There were only two well-designed and adequately powered randomized trials of LMWH that were identified in the systematic literature review.14,17 Of the two studies, the CLOT trial was the only one to report a statistically significant benefit in terms of VTE absolute risk reduction when compared to a VKA control group (dalteparin = 8% vs. VKA = 15.8%; p = 0.27). 14 In contrast, the recent tinzaparin study failed to find statistically significant difference between tinzaparin and the VKA control. 15 Differences in efficacy between dalteparin and tinzaparin were also suggested by subgroup analyses in patients with renal impairment.22,23 It is unclear what caused these observed disparities, but it could be related differences in patients, disease characteristics, concurrent anticancer therapy, or even modest efficacy or safety differences between dalteparin and tinzaparin.
The current review of the literature was also extended to supporting economic evaluations of the LMWH in patients with cancer-related VTE. There was a paucity of data for enoxaparin, nadroparin, and tinzaparin. In contrast, there were robust patient-level economic evaluations of dalteparin that were conducted in four countries, with costs per QALY being less than three times the per capita gross domestic product (GDP) of the respective countries.7,26–28 This observation is relevant from the health-policy perspective, because the World Health Organization (WHO) has suggested that drugs with costs per QALY less than three times the per capita GDP would be considered cost-effective.30,31 Based on the WHO criteria, secondary prophylaxis dalteparin is a cost-effective alternative to VKA for the prevention of recurrent VTE in patients with cancer and especially in patients with moderate to severe renal impairment. In addition, it is tempting to speculate that the economic value of dalteparin may also be extended to other populations of special interest such as patients with metastatic disease.
There are several limitations in this review that need to be acknowledged. All systematic reviews are affected by the quality of the studies analyzed. For that reason, the analysis was limited to prospective randomized trials with at least 25 patients per arm. Given the nature of the intervention (oral vs. subcutaneous injections), the trials were not double blinded, which could have introduced observer bias into the final assessment of recurrent VTE. Since there were only six randomized trials identified with slight differences in patient characteristics, an indirect analysis was not conducted because of limited statistical power to find differences between agents and the inherent heterogeneity between trials. Even though there are ongoing randomized trials, the oral factor Xa inhibitors were not included in the current review because data have not been reported from these studies. 32
Conclusions
This new literature review revealed that the best quality clinical and cost-effectiveness evidence supporting the use of an LMWH for acute treatment and secondary prophylaxis of VTE in patients with cancer supports the use of dalteparin and tinzaparin. However, compared with VKA, only dalteparin demonstrated a statistically and clinically relevant reduction in the occurrences of VTE in all patients and in patients with moderate to severe renal impairment. The totality of high-quality clinical and cost-effectiveness evidence specifically supports the use of dalteparin over different LMWHs (tinzaparin, nadroparin, and enoxaparin) for the acute treatment and prevention of recurrent VTE in patients with cancer, and especially in those with renal insufficiency.
Footnotes
Authors’ contribution
All authors confirm they were involved in study design, data analysis and interpretation, drafting of the paper, and final approval of the current version to be published. The corresponding author had full access to the data, designed the study, conducted the analysis, interpreted the results, and had the final responsibility for the decision to submit the paper for peer-reviewed publication.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LS and SW are employees of the sponsor (Pfizer Inc.).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by Pfizer Inc.