
Abstract
Background
Granulocyte colony-stimulating factors are effective at reducing the risk and duration of neutropenia. The current meta-analysis compared the neutropenia-related efficacy and safety of lipegfilgrastim to those of pegfilgrastim and filgrastim.
Methods
Embase was searched for trials examining the efficacy/safety of lipegfilgrastim, pegfilgrastim, or filgrastim. Outcomes included febrile neutropenia, severe neutropenia, duration of severe neutropenia, time to recovery of absolute neutrophil count, and incidence of bone pain. Direct comparisons were made using random-effects models. No trials directly compared lipegfilgrastim and filgrastim. Indirect comparisons were made between lipegfilgrastim and filgrastim with pegfilgrastim as the common comparator.
Results
This meta-analysis included a total of 5769 patients from 24 studies. Over all cycles, lipegfilgrastim showed a lower, nonsignificant risk of febrile neutropenia compared with pegfilgrastim. Lipegfilgrastim has a lower risk of febrile neutropenia versus filgrastim but was also not statistically significant. The risk ratio for severe neutropenia in cycle 1 was 0.80, a 20% reduction in favor of lipegfilgrastim. For cycles 2–4, the risk ratio was 0.53 (0.35, 0.79) for lipegfilgrastim versus pegfilgrastim. The risk of severe neutropenia in cycles 2–4 was also significantly lower for lipegfilgrastim (risk ratio 0.45, 0.27, 0.75, respectively). No significant differences were found for febrile neutropenia and severe neutropenia in cycle 1. However, in cycles 2–4, lipegfilgrastim was associated with significant and clinically meaningful reductions in risk of severe neutropenia versus either pegfilgrastim or filgrastim.
Conclusions
Compared with pegfilgrastim or filgrastim, lipegfilgrastim has a statistically significantly lower absolute neutrophil count recovery time; however, differences in duration of severe neutropenia and bone pain were nonsignificant.
Introduction
Neutropenia is a common yet serious complication experienced by cancer patients treated with myelosuppressive chemotherapy. 1 Neutropenia is the primary cause for chemotherapy delays and dose reductions, potentially compromising patient outcomes, including survival and complete response rates.2–4 Of particular concern are severe neutropenia (SN; absolute neutrophil count (ANC) <0.5 × 109/L) and febrile neutropenia (FN; SN with fever), which is defined as an oral temperature of >38.3℃ or two consecutive readings of >38.0℃ for 2 h and an ANC of <0.5 × 109/L or expected to fall below 0.5 × 109/L. 5 FN is associated with prolonged hospitalization, serious infections and the use of broad-spectrum antibiotics, decreased quality of life, and increased mortality.6,7 The average mortality rate associated with episodes of FN ranges from 5% to 13.7%; however, it can reach 50% or higher in selected populations.7–9 Additionally, FN is associated with substantial economic consequences related to hospitalization and employment losses. 3
One of the primary treatment strategies to reduce the risk of SN and FN is the prophylactic use of granulocyte colony-stimulating factor (G-CSF). G-CSF is a biological growth factor that supports the proliferation, differentiation, and activation of hematopoietic cells.6,10 US and European guidelines10,11 suggest that G-CSF be used as primary prophylaxis after chemotherapy when the risk of FN is >20%. Prophylactic use of G-CSFs is associated with a reduction in the incidence, severity, and duration of SN (DSN) and FN, a reduction in FN-related hospitalizations, and a lower mortality rate due to infection.12–14 In addition, the use of G-CSFs is associated with fewer dose reductions and delays, leading to greater relative dose intensity and increasing the probability of receiving a full dose of chemotherapy within a cycle.13,15,16 The most frequent patient-reported adverse event (AE) associated with G-CSF use is mild-to-moderate bone pain. 13
Two of the most widely used G-CSFs available are short-acting filgrastim (FIL; Neupogen®; Amgen Inc., Thousand Oaks, CA) 17 and long-acting pegfilgrastim (PEG; Neulasta®; Amgen Inc.). 18 Short-acting FIL is administered subcutaneously or intravenously once daily for up to 14 days or until the ANC has reached 10,000/mm3 following its chemotherapy-induced nadir. Previous clinical trials12,13,19–21 have indicated that 8 to 14 days of FIL treatment produce the most optimal results, with 11 injections as the average.19,22 Long-acting PEG is administered once per chemotherapy cycle, 17 and previous randomized controlled trials (RCTs) and observational studies suggest that a single dose of PEG is equivalent, and in some instances superior, to a 10 - to 14-day daily course of FIL.23–26
Lipegfilgrastim (LIP) (Lonquex®; Teva Pharmaceuticals Industries Ltd, Petach Tikva, Israel) is a long-acting, once-per-cycle G-CSF that was approved by the European Medicines Agency in 2013. Phase 3 trials of chemotherapy-naïve patients with breast cancer reported that LIP was non-inferior to PEG with respect to DSN, and the incidence and duration of FN-related dose reductions, hospitalizations, and antibiotic use were similar to those of PEG.27,28 The safety profile of LIP is also similar to that of PEG and bone pain-related symptoms were similar in patients receiving LIP or PEG.27,29
This paper describes a meta-analysis of recombinant human G-CSF studies in patients receiving chemotherapy in order to assess the relative benefit of available long-acting agents (LIP versus PEG) and similarly compare LIP to the short-acting agent (FIL). Outcomes of interest were neutropenia-related efficacy and safety.
Methods
Data sources and search strategy
A systematic literature review was performed to identify trials examining the efficacy and safety of LIP, PEG, or FIL, either head-to-head or versus placebo/non-treatment (PLA/NT). Elsevier’s Embase Biomedical Answers website was used to identify published literature in the MEDLINE and Embase databases on the use of G-CSFs and/or antibiotic therapy in the prevention and treatment of chemotherapy-induced neutropenia and FN. The search crossed relevant disease and drug terms with additional terms related to epidemiology, humanistic and economic burden, and regional identifiers (see Supplemental material). The search was restricted to English-language reports published between 2005 and 2015. Additional records were identified by hand-searching other relevant sources, including product label information and the reference lists of key published studies.
Design
A direct meta-analysis comparing the efficacy of LIP versus PEG was chosen because randomized head-to-head trials have been conducted between the compounds. For the comparison of LIP versus FIL, indirect analytical techniques were employed because no head-to-head trials were identified. Potential paths of comparison and contrast of interest are outlined in Figure 1. We selected two common comparators (or links) for the indirect treatment comparison of LIP to FIL: via PEG and via PLA/NT. Refinements of the analytical methods were made based on the findings of the search and assessment of the completeness of data.
Multipath meta-analysis plan.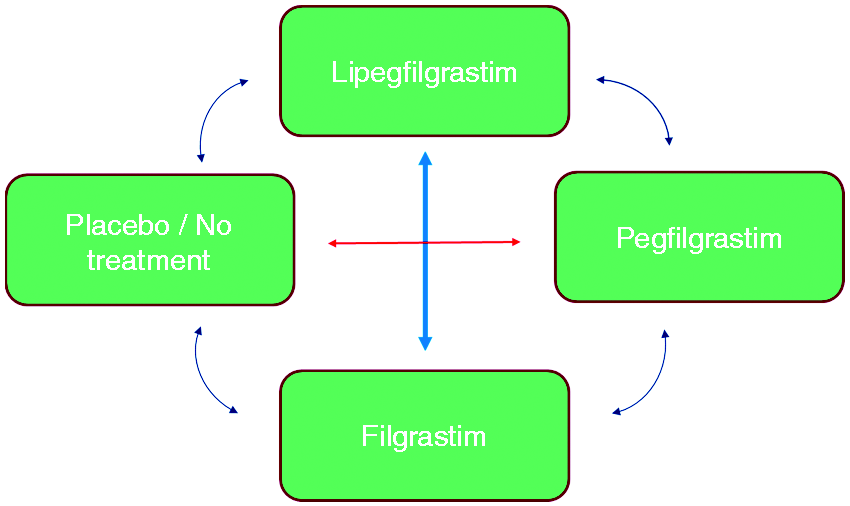
Study selection and data extraction
To be included in the analysis, studies needed to meet the following criteria: prospective design, randomized treatment assignment, double-blind design (or, at minimum, blinding of outcome assessment), pre-specified eligibility criteria, adequate sample size, report of the number of participants randomized, adequate details of treatment groups at baseline, comparable treatment groups at baseline, and similar co-interventions (that could affect results) across groups. A follow-up primary outcome assessment rate of 80% was required for the first cycle of treatment. Studies of G-CSFs for stem cell mobilization in bone marrow or peripheral blood stem cell transplantation and studies in children were excluded from consideration.
Abstracts of articles identified in the search were screened by two independent reviewers. Full reports were obtained for the studies selected in the first stage and evaluated by the two reviewers for final inclusion. Data related to the outcomes of interest were extracted independently by the reviewers into structured spreadsheets. At each step, disagreements between the reviewers were resolved by discussion or the inclusion of a third reviewer.
Data analysis
The pre-selected efficacy outcomes were incidence of FN, incidence of SN, hospitalization for FN or SN, time to recovery of ANC, and DSN. Because data on hospitalization incidence were missing in some reports and inconsistently reported in others, this outcome could not be analyzed. In addition to these pre-specified efficacy outcomes, incidence of bone pain was also examined. Random-effects meta-analysis was used to synthesize results from direct (head-to-head) trials using RevMan 5.2 software.
Meta-analysis methods for continuous outcome measures varied due to differences in the availability of reported results. Generic inverse variance methods based on estimates of mean treatment differences and standard errors were used for time to ANC recovery. Analysis of DSN employed inverse variance based on the means and standard deviations of each treatment group. Indirect estimates of treatment differences were conducted using the Bucher method 30 with two iterations: PEG as the common comparator and PLA/NT as the common comparator.
Heterogeneity was assessed using forest plots that graphically represent between-study variability alongside the ratio measures. The inconsistency index (I2) was used to quantify the percentage of variability due to heterogeneity rather than sampling error. This index can be interpreted on a scale from 0–40% (might not be important) to 75–100% (considerable heterogeneity).
Where available, intention-to-treat analyses were used instead of per-protocol (PP) analyses. No imputation for missing data was performed for binary outcome measures. For continuous outcomes, missing standard deviations were calculated from the standard error or the 95% confidence interval (CI) or vice versa. The crossover study by Shi et al. 31 was inadequately reported with statistical methods suitable for parallel-group studies. In the case of dose-finding studies, only arms with therapeutic levels of G-CSF were used in analyses (e.g., 6 mg of LIP or PEG); consequently, the Kosaka et al. 32 study was not considered in the analyses.
Results
Study characteristics
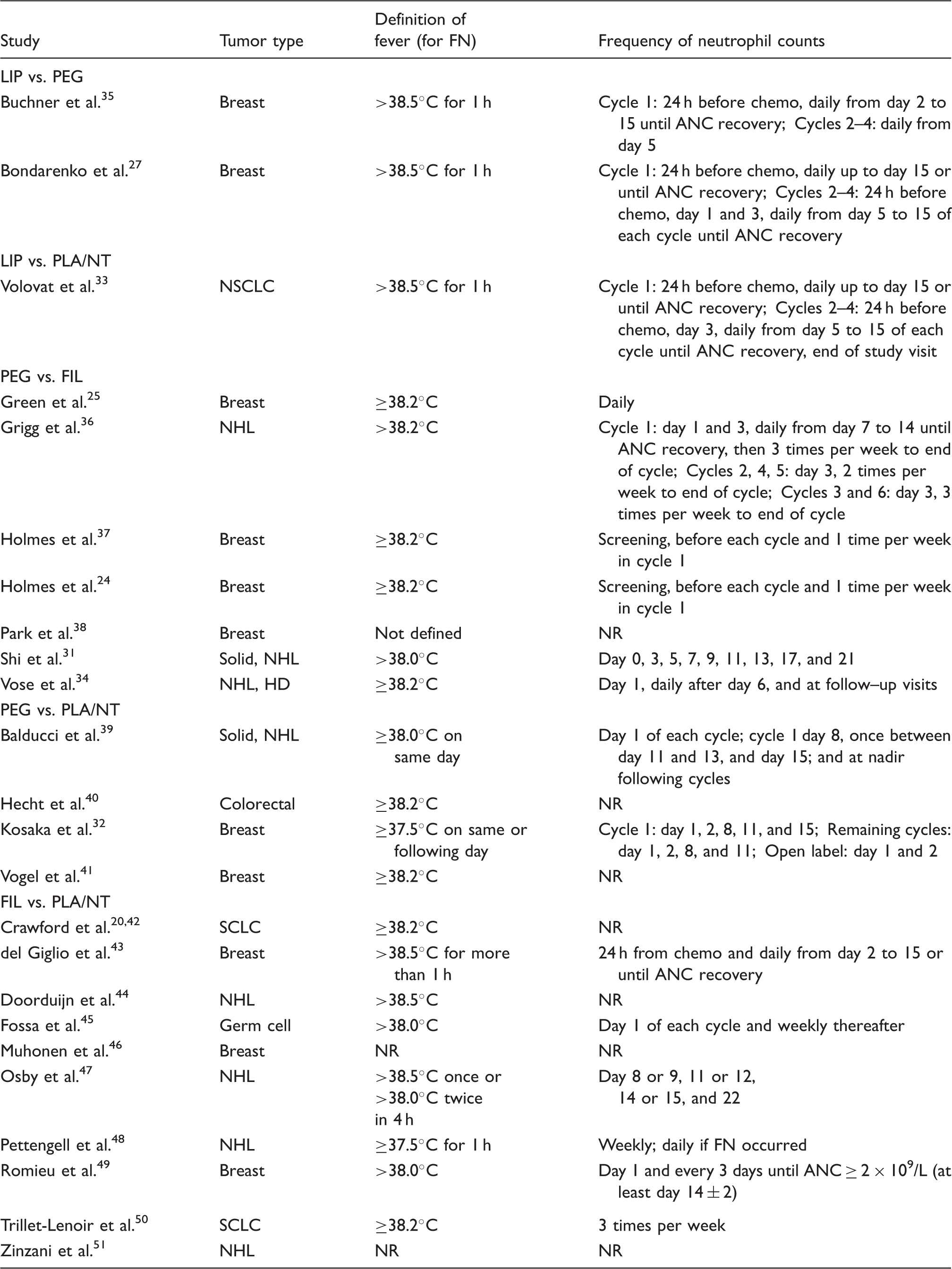
After duplicates were removed, 91 unique abstracts were identified and screened (Figure 2). Of those, 35 full-text articles were obtained and reviewed for eligibility. Ultimately 24 studies involving 5769 patients were deemed eligible for inclusion and were subjected to data extraction. Characteristics of these 24 studies are presented in Table 1.
Flow diagram of publication selection process. Study characteristics.
a
ANC: absolute neutrophil count; FIL: filgrastim; FN: febrile neutropenia; HD: Hodgkin’s disease; LIP: lipegfilgrastim; NHL: non-Hodgkin’s lymphoma; NR: not reported; NSCLC: non-small-cell lung cancer; NT: no treatment; PEG: pegfilgrastim; PLA: placebo; SCLC: small cell lung cancer; SN: severe neutropenia. Also stipulated protocol-defined SN as the administration of systemic antibiotics (not used in meta-analysis). Grade 3 neutropenia = ANC between 0.5 × 109/L and 1.0 × 109/L; Grade 4 neutropenia = ANC < 0.5 × 109/L.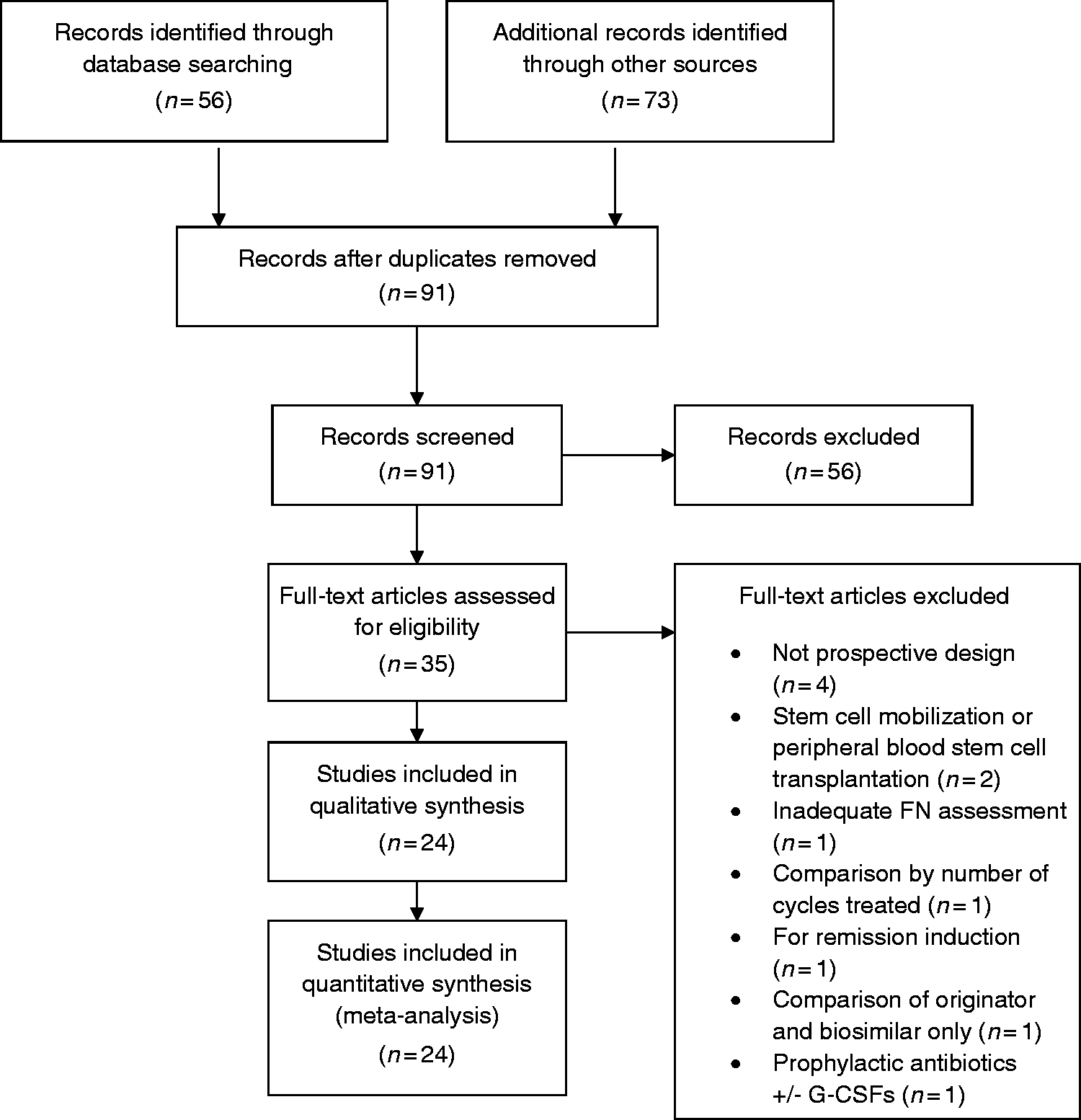
Most studies included data from phase 2 or phase 3 RCTs with a mix of double-blind and open-label trials. Parallel-group comparisons were most common, although for two studies the comparator was existing treatment protocols or physician decision versus active treatment. In both cases, the first cycle of chemotherapy was treated as a placebo-controlled period. Trials included three types of control groups: active control, placebo control, or no treatment.
Eleven reports provided data from trials of breast cancer tumors, one study involved non small-cell lung disease, two studies were for small cell lung cancer, one was for colorectal cancer, eight involved non-Hodgkin’s lymphoma, and one was for germ cell tumors. Across trials, the percentage of females ranged from 31% to 100% (in breast cancer). Three studies included patients with stage I cancer; the remainder included only more advanced cancer stages (II–IV). Full descriptions of chemotherapy regimens and definitions of the efficacy outcomes are provided in Table 1.
The inclusion criteria of one pivotal LIP study design had a significant impact on the analysis. Due to ethical considerations, the LIP versus PLA study 33 was limited to patients not at high risk for FN. As might be expected, the incidence of FN in the PLA group of this study was low (8.0%) compared to those in the PLA group of the older FIL versus PLA trials (12.5% to 59.6% per trial; 43.0% across the combined PLA population). For this reason, the older FIL versus PLA studies could not be considered “similar” to the LIP versus PLA study, and therefore the planned indirect analysis through PLA as a common comparator was deemed invalid, and only indirect analyses of LIP versus FIL through PEG are presented.
Direct and indirect comparisons
Incidence of FN
The incidence of FN was low across the two studies (see Figure 3), with only five events occurring among 306 patients. In the pooled comparison, the risk of FN was lower with LIP than PEG, but did not reach statistical significance (risk ratio (RR) = 0.34, 95% CI: 0.05, 2.14). In the FIL versus PEG head-to-head trials, the pooled comparison suggested that PEG had lower risk of FN relative to FIL (RR = 1.54, 95% CI: 1.03, 2.29). In the indirect comparison of LIP versus FIL via PEG, LIP had nonstatistically significant lower risk of FN in the overall analyses (RR = 0.22, 95% CI: 0.03, 1.51). Similar results were seen in two sensitivity analyses (LIP versus FIL via PEG): one limited to studies of breast cancer patients (RR = 0.20, 95% CI: 0.03, 1.41) and one limited to reports published in the past five years (RR = 0.18, 95% CI: 0.02, 1.51).
Forest plots of LIP versus PEG and FIL versus PEG.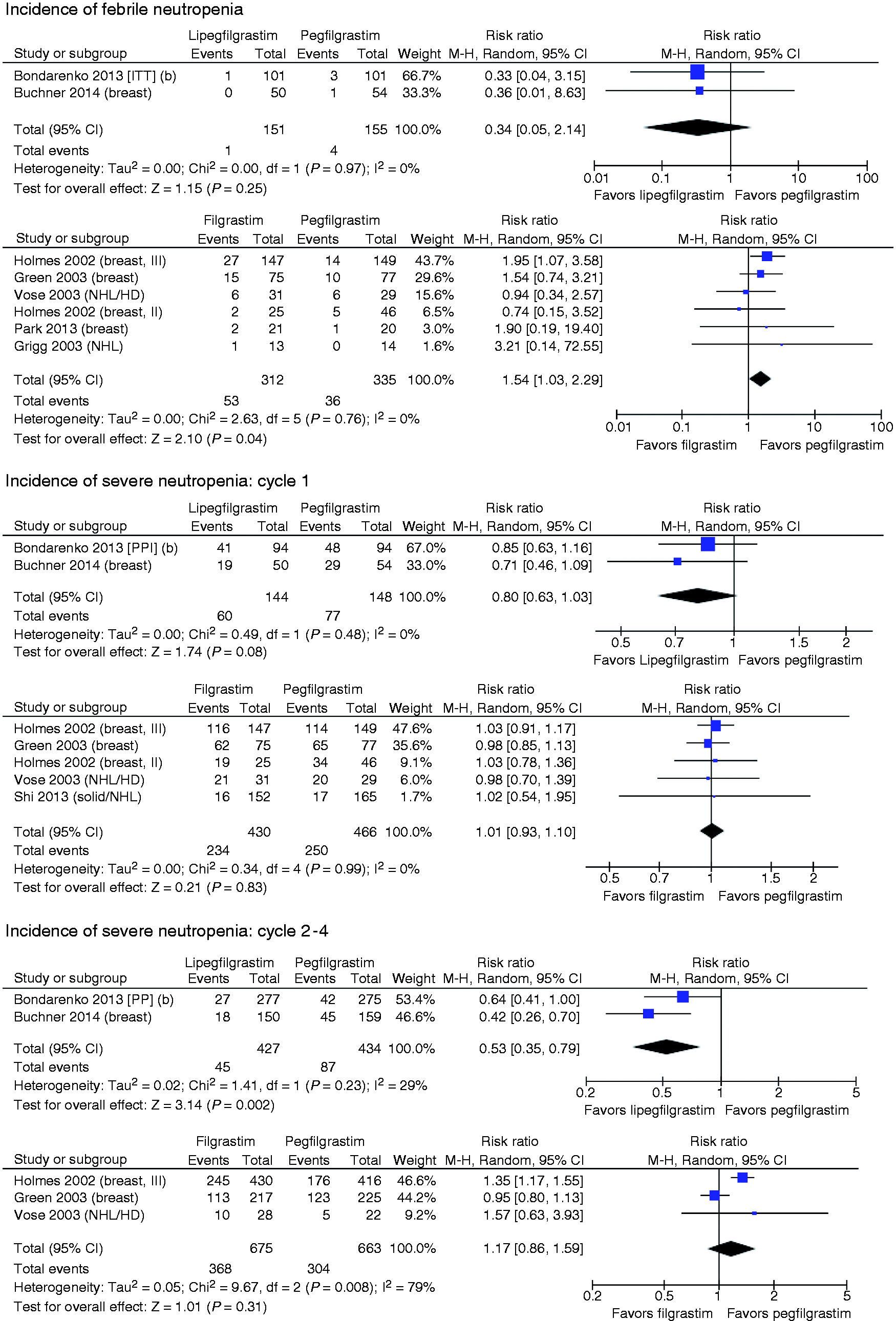
Incidence of SN
Comparison of incidence of FN and SN.

CI: confidence interval; FIL: filgrastim; FN: febrile neutropenia; LIP: lipegfilgrastim; PEG: pegfilgrastim; RR: risk ratio; SN: severe neutropenia.
SN in cycle 1
The RR for SN in cycle 1 for the LIP versus PEG trials was 0.80 (95% CI: 0.63, 1.03), a 20% relative risk reduction in favor of LIP which did not reach statistical significance (p = 0.08). In cycle 1, the incidence of SN in the PEG-treated arms of FIL versus PEG studies ranged from 51.1% to 84.4% with one outlying result at 10.3%. 31 In studies of FIL versus PEG, no appreciable difference was seen in the incidence of SN in cycle 1 of chemotherapy. (Note that the Bondarenko et al. 27 report included only PP analyses.)
The indirect comparison of LIP and FIL produced a similar RR for SN in cycle 1: 0.79 (95% CI: 0.61, 1.03). Sensitivity analyses limited to breast cancer studies or excluding the outlying Shi et al.’s study did not change the estimate for the indirect analysis.
SN in cycles 2–4
The risk of SN per cycle in cycles 2–4 was statistically significantly lower for LIP versus PEG (RR = 0.53, 95% CI: 0.35, 0.79). In studies of PEG versus FIL, the overall RR was 1.17 (95% CI: 0.86, 1.59), a nonsignificant difference in favor of PEG. In the indirect comparison, the risk of SN in cycles 2–4 was significantly lower for LIP compared to FIL (RR = 0.45, 95% CI: 0.27, 0.75). The size and significance of this association remained in a sensitivity analysis excluding the study by Vose et al. 34 (RR = 0.46, 95% CI: 0.27, 0.79), which reported only cycles 1 and 2.
Time to ANC recovery
Comparison of time to ANC recovery, duration of SN, and incidence of bone pain. a

ANC: absolute neutrophil count; CI: confidence interval; FIL: filgrastim; LIP: lipegfilgrastim; PEG: pegfilgrastim; RR: risk ratio; SN: severe neutropenia.
RR reported for bone pain.
Mean recovery time was shorter for LIP versus FIL by 1.88 days (95% CI: 0.95, 2.82). For the main indirect comparison, the Shi et al.’s crossover study 31 was excluded due to unknown intrapatient correlation in cycles 2–4. The size and direction of the difference between LIP and FIL remained in a sensitivity analyses limited to breast cancer patients, with a mean difference of 1.95 days (95% CI: 1.02, 2.88) in favor of LIP. When the Shi’s study was included with various assumptions regarding intrapatient correlation across the cycles, similar results were found (point estimates from 2.03 to 2.04 days).
Duration of severe neutropenia
For the LIP versus PEG trials, which involved daily neutrophil counts, the mean DSN did not differ significantly between LIP and PEG, with a mean difference of 0.17 days (95% CI: −0.39, 0.04) in favor of LIP (see Table 3). The differences between treatment arms within the FIL versus PEG studies were quite small: less than one day in either direction. The overall estimated effect was 0.0 days. The indirect analysis of LIP versus FIL reflects primarily the difference between LIP and PEG, with the extra comparison of FIL versus PEG not changing the estimate.
Incidence of bone pain
Combining the two studies that compared LIP with PEG, the rates of bone pain were 15.9% and 14.2%, respectively (see Table 3 and Figure 3). The direct comparison of LIP with PEG produced a RR of 1.12 (95% CI: 0.66, 1.90), indicating that the difference did not reach statistical significance. The indirect comparison of LIP versus FIL via PEG was similar to that of the direct comparison and was also nonsignificant: 1.07 (95% CI: 0.59, 1.93).
Discussion
Myeloid growth factors are critical to reduce the incidence of chemotherapy-induced neutropenia and FN and allow full dosing of chemotherapy on schedule. Commercially available agents include FIL, which is administered daily; and the long-acting, once-per-chemotherapy cycle drugs LIP and PEG. This meta-analysis applied a mixed treatment comparison approach with direct and indirect comparisons to make it possible to compare the efficacy of LIP versus PEG (through a direct meta-analysis) and LIP versus FIL (through an indirect meta-analysis with PEG as the common comparator). Four efficacy outcomes and one AE were included to provide a comprehensive comparison of these agents.
In trials that compared LIP to PEG, the risk of FN was numerically lower for LIP but not statistically significant. This may be due to the low incidence of FN in the two studies. The overall low incidence of FN in the Bondarenko et al. 27 study may be explained by the protocol-specified strict definition for FN and the use of prophylactic systemically active antibiotics for patients at high risk for infection in this non-inferiority trial, which may have reduced the FN event rate. This prophylactic treatment creates exchangeability problems for the indirect analysis of LIP versus FIL. Although FN occurred in 1.9% to 3.0% of patients in the PEG arm of the LIP versus PEG trials, the incidence among PEG-treated patients was as high as 20.7% in the PEG versus FIL trials. The myelosuppressive intensity of the chemotherapy regimens used in each study as well as the presence of other risk factors may have impacted the base rate of FN.
In chemotherapy cycles 2–4, LIP was associated with significant and clinically meaningful reductions in risk of SN versus either PEG (RR = 0.53, 95% CI: 0.35, 0.79) or FIL (RR = 0.45, 95% CI: 0.27, 0.75). In cycle 1, differences between LIP/PEG and LIP/FIL were smaller and did not reach statistical significance.
Time to ANC recovery, which has a longer duration than DSN overall, was significantly shorter for LIP than for both PEG (1.75 days, 95% CI: 0.90, 2.61) and FIL (1.88 days, 95% CI: 0.95, 2.82). Bone pain, the most commonly reported AE across trials, was numerically higher for LIP but not to a statistically significant extent.
For the outcome of FN, comparisons of LIP to PEG and FIL were hampered by the low incidence of FN in the two pivotal LIP studies: a non-inferiority study which had patients at high risk for infection use prophylactic systemically active antibiotics per protocol, 27 and the other which was limited to patients not at high risk for FN. 33 Although FN occurred in only 1.9% to 3.0% of patients in the PEG arm of the LIP versus PEG trials, the incidence among PEG-treated patients was as high as 20.7% in the PEG versus FIL trials.
The study also shares the limitations of most meta-analyses: differences in the baseline patient population (e.g., cancer type), differences in study design (e.g., crossover between groups and the timing of assessments of SN and ANC), differences in the definition of FN, and changes in concomitant treatment strategies over time (e.g., prophylactic antibiotic use).
The clinical trial data have clearly demonstrated the safety and efficacy of LIP. Unlike most of the previous studies, the current meta-analysis provided a comprehensive assessment of the efficacy and safety of LIP, PEG, and FIL by including the incidence of FN, SN, time to ANC recovery, DSN, and bone pain. Compared with either PEG or FIL, LIP was associated with lower risk of FN and SN in cycle 1, but the RRs were not statistically significant. In chemotherapy cycles 2–4, LIP was associated with significant and clinically meaningful reductions in risk of SN versus either PEG or FIL. Compared with PEG or FIL, LIP has a statistically significantly shorter ANC recovery time. Differences in DSN and bone pain were not significant. This meta-analysis supports the conclusion that LIP is more effective than either PEG or FIL for the prevention of SN in cycles 2–4 of chemotherapy and that patients treated with LIP had a shorter time to ANC recovery. More head-to-head clinical studies and real-world data analyses are suggested to validate the comparative findings.
Footnotes
Acknowledgments
All authors meet the ICMJE criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published. Editorial assistance in the preparation of this manuscript was provided by Jason Allaire, PhD of Generativity Solutions Group, Cary, NC, USA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bond received funding from Teva Pharmaceuticals to develop the meta-analysis. Dr Schwartzberg has received consulting fees from Amgen Pharmaceuticals. Dr Klastersky has nothing to disclose. The remaining authors are employees of Teva Pharmaceuticals.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Teva Pharmaceuticals.