
Abstract
Clinical pharmacists are important contributors to the care of patients with cancer; it is therefore critical for oncology clinical pharmacists to stay current with new anticancer therapies. This review summarizes the epidemiology and pathogenesis of non-small cell lung cancer, including the most common genetic alterations, as well as the mechanism of action, clinical development, pharmacodynamics and pharmacokinetics of the anaplastic lymphoma kinase inhibitor ceritinib for the treatment of patients with anaplastic lymphoma kinase-positive non-small cell lung cancer. Targeted therapies based on the presence of specific mutations are an important development in the treatment of non-small cell lung cancer. However, acquired resistance to the first anaplastic lymphoma kinase-inhibitor approved by the U.S. Food and Drug Administration, crizotinib, is observed in almost half of patients treated with it. Ceritinib is an oral anaplastic lymphoma kinase-inhibitor that has demonstrated more potent antitumor activity than crizotinib in preclinical models. It was granted accelerated approval in 2014 to treat anaplastic lymphoma kinase-positive metastatic non-small cell lung cancer patients who have progressed on or are intolerant to crizotinib. Ceritinib represents an important alternative second-line therapy for patients with metastatic non-small cell lung cancer who have traditionally limited treatment options.
Introduction
In today’s oncology practice, the clinical pharmacist has an active role in patient care by providing expertise regarding drug therapies. Therefore, staying current with new anticancer treatments is a priority. The oncology clinical pharmacist recommends cancer therapies, monitors toxicities, modifies doses, and educates patients and other healthcare professionals about new treatments or new indications for existing treatments.1,2 This review is intended to facilitate the oncology clinical pharmacist in his or her daily work, specifically with the use of anaplastic lymphoma kinase (ALK) inhibitor ceritinib for treatment of patients with ALK-positive metastatic non-small cell lung cancer (NSCLC). A comparison with alectinib is also included. In addition, this review aims to be of value to pharmacists who work in specialty pharmacies that dispense oral cancer therapy.
Lung cancer
Epidemiology
Lung cancer is the second most common cancer in the USA 3 and the leading cause of cancer-related deaths in the USA and worldwide.3,4 In the USA in 2016, there will be an estimated 224,000 new cases and 158,000 deaths attributed to lung cancer. 5 The median age of diagnosis is 70 years and median age at death is 72 years (range for both, 65–74 years), 5 which reflects a highly aggressive disease course. African American men have a disproportionally higher incidence (≈50%) of lung cancer than whites. 6 Cigarette smoking remains the most important risk factor for lung cancer, despite a decrease in smoking rates. A dose–response relationship exists, where quantity and duration of smoking increase risk. 3 Other significant risk factors include exposure to radon gas or asbestos and genetic predisposition. 3
Overall, the current decline in lung cancer is largely due to decreased exposure to tobacco smoking, changes in composition of cigarettes and use of more efficient cigarette filters.5,7,8
The Centers for Disease Control and Prevention continue to support comprehensive efforts to prevent initiation of tobacco use, promote smoking cessation and ensure smoke-free environments. 7 As of December 2013, the U.S. Preventative Services Task Force recommends widespread adoption of lung cancer screening with low-dose computed tomography in adults aged 55 to 80 years who have a 30 pack-year smoking history and currently smoke or have quit within the past 15 years. 9 This is anticipated to shift the epidemiology of lung cancer.6,9 Screening appears particularly effective in early detection of adenocarcinoma, thus the reported incidence of adenocarcinoma is anticipated to increase. 6
Non-small cell lung cancer
With a five-year survival of 50% at best for early stage disease and as low as 1% for advanced stage disease, NSCLC is typically associated with bleak outcomes. 10 It accounts for more than 85% of lung cancer cases 11 and is described as a group of distinct diseases with genetic and cellular heterogeneity. The two most common phenotypes are adenocarcinoma (40%) and squamous cell carcinoma (29%).11,12 The relationship with smoking is not as strong with NSCLC adenocarcinoma as it is with NSCLC squamous cell carcinoma or small cell lung cancer.6,12 Non-small cell lung cancer is characterized by a low response rate to chemotherapy; one study reported a 19% response rate with a median survival of 7.9 months among patients randomized to treatment with cisplatin/paclitaxel, cisplatin/gemcitabine, cisplatin/docetaxel, or carboplatin/paclitaxel. 13
Diagnosis and staging
For suspicion of lung cancer, a lung biopsy when possible should be performed to help establish a diagnosis. For locoregional disease, chest X-ray and chest computed tomography (CT) are recommended. For metastatic disease, the following are recommended: biopsy of mediastinal lymph nodes, optional bone scan with evidence of bone metastases, head CT or magnetic resonance imaging for symptomatic central nervous system disease, and gold-standard biopsy of radiographically confirmed isolated adrenal or lung mass, if possible. 14 NSCLC is staged with the TNM staging system. We refer the reader to the TNM Classification of Malignant Tumors and the National Comprehensive Cancer Network guidelines for a more detailed review of histology and work-up.15,16
Molecular pathogenesis
The underlying molecular abnormalities that drive lung cancer are well established and varied. During the 1980s through the 2000s, research focused on mutations in Kirsten rat sarcoma viral oncogene homolog (KRAS) and P53, loss of specific alleles, and DNA methylation of tumor suppressor genes. 17 More recently, there is interest in activating mutations in epidermal growth factor receptor (EGFR), first described in 2004, 18 and the echinoderm microtubule-associated protein-like 4 (EML4)–ALK fusion gene, first described in NSCLC in 2007. 19 Mutations in KRAS are common in NCSLC adenocarcinoma and are associated with cigarette smoking, asbestos exposure, and female sex. 20 KRAS mutation accounts for 90% of RAS mutations in lung adenocarcinomas (uncommon in SCLC). 21 Approximately 97% of KRAS mutations in NSCLC involve codons 12 or 13. 21
Mutations in EGFR occur more commonly in light or never smokers, females, and Asians. 22 Prevalence of EGFR mutation has been reported to be 45–52% among Asians. 23 They are present in approximately 15% of primary lung adenocarcinomas and are generally mutually exclusive of KRAS mutations. 22 The majority of EGFR mutations involve a deletion in exon 19 and missense mutation in exon 21. 22 ROS proto-oncogene 1, receptor tyrosine kinase (ROS1) gene rearrangements have been identified in 2% of lung adenocarcinomas and tend to appear in patients who are a younger age at diagnosis and light or never smokers. 22 The underlying mechanism for constitutive activation of ROS1 that leads to downstream signaling of several oncogenic pathways is unknown. 22 Mutations of RAF murine sarcoma viral oncogene homolog B1 (BRAF) are found in 1–3% of patients with NSCLC and are most common among former or current smokers with lung adenocarcinoma. The point mutation V600E is the most common BRAF mutation in NSCLC, accounting for roughly half of all NSCLC cases with a BRAF mutation. 24
ALK gene rearrangements are oncogenic driver mutations in 2–5% of lung adenocarcinoma with higher predominance in males.22,25,26 Similar to EGFR mutation, ALK gene rearrangements are commonly found in younger, light or never smokers.22,26 The most common ALK gene rearrangement in lung cancer is inversion of chromosome 2, resulting in the EML4–ALK fusion.19,22,26 ALK gene rearrangements are largely independent of mutations of EGFR, KRAS, and BRAF. 27
Prognosis
The overall predicted five-year survival for patients with lung cancer is 17.4%. 5 Tumor stage has a strong influence on survival. The five-year relative survival by stage at diagnosis is 54.8% for localized disease, 27.4% for regional disease, and 4.2% for distant disease. 5 Chemotherapy yields modest survival improvement for advanced NSCLC when compared with best supportive care 28 and remains a treatment option for patients with lung cancer with good performance status. 16 However, advances in our understanding of the molecular basis of disease have led to targeted approaches for certain patients in whom an actionable genetic alteration is discovered and have been associated with improved prognosis. 27 For patients with an activating EGFR mutation, EGFR tyrosine kinase inhibitors demonstrated a survival advantage over chemotherapy.16,27 Similarly, in patients in whom an ALK rearrangement is discovered, targeted therapy with an ALK inhibitor can confer improved outcomes.16,27 More recently, approaches to enhance the immune response against cancer have also become a therapeutic option for patients with progressive disease. 29
Role of ALK in human cancer
ALK constitutes a subfamily within the insulin receptor superfamily. 30 The precise, native physiological role of ALK in mammals has not been characterized; therefore, it is unclear whether adverse reactions seen with ALK inhibitors are ALK-specific effects or off-target effects.30,31 ALK-fusion proteins resulting from the rearrangement of the gene were first described in anaplastic large-cell non-Hodgkin lymphoma. 32 ALK mutations have since been found to play a role in initiation and progression of lymphomas, neuroblastomas, renal cell carcinoma, colorectal cancer, breast cancer and thyroid cancer.30,31 The discovery of EML4–ALK in NSCLC by analysis of mouse fibroblasts infected with lung cancer specimens was published in 2007. 19 Researchers found that a small inversion within chromosome 2p results in the EML4–ALK fusion in a subset of Japanese patients with NSCLC. 19 The EML4–ALK fusion transcript was detected in 6.7% (5/75) of NSCLC patients. The patient population harboring the EML4–ALK fusion gene did not overlap with those harboring EGFR or KRAS mutations,19,26 which showed that EML4–ALK-positive cancer is a novel and unique subclass within NSCLC.
ALK rearrangements, such as the EML4-ALK fusion, lead to “oncogenic addiction,” the dependency on continued ALK signaling for survival and proliferation. 33 The EML4–ALK fusion protein constitutively activates the ALK kinase domain, 30 auto-phosphorylates and activates the mitogen-activated protein kinase (MAPK)/MEK/extracellular regulated kinase (ERK), phosphoinositide 3-kinase (PI3K)/V-Akt murine thymoma viral oncogene homolog (AKT), and RAS/signal transducer and activator of transcription 3 (STAT3) pathways.22,26 These pathways promote initiation, progression and survival of NSCLC cells. 33 However, it is not clear which pathway(s) are critical to pathogenesis of NSCLC.26,34 There are a reported 27 ALK fusion variants, including 21 EML4–ALK isoforms, in NSCLC that result in proteins with differences in signaling, tumorigenic potential and sensitivities to ALK inhibitors.26,31
Crizotinib (Xalkori, Pfizer Inc, New York, NY, USA) was the first ALK-inhibitor approved by the U.S. Food and Drug Administration (FDA) after it demonstrated high objective response rates and progression-free survival (PFS) in ALK-positive NSCLC.25,26,35 While crizotinib is effective initially, patients ultimately develop resistance.25–27,31,33–35 In addition, spread of disease into the central nervous system (CNS) has been observed in patients whose disease progressed after treatment with crizotinib.3,34 Clinical characterization of ALK-positive NSCLC patients who were treated with crizotinib beyond disease progression revealed that the brain was the most common single organ site for new lesions.36,37 The pathophysiology for CNS metastasis is attributed to poor cerebrospinal fluid penetration of crizotinib despite good systemic control.3,33,34 Reports of patients who developed CNS metastasis and continued treatment with crizotinib without further disease progression suggest that some patients may be able to continue crizotinib after local radiotherapy to the CNS.33,36,37 Second-generation ALK inhibitors, such as ceritinib, have shown significant activity in the brain,31,38 providing an alternative to CNS radiotherapy. 16 Alectinib, another second-generation ALK inhibitor, has also been demonstrated to have significant activity in the brain. 39
ALK testing
ALK testing using an FDA-approved test was a requirement for FDA approval of crizotinib. 40 The break-apart fluorescence in situ hybridization (FISH) assay was the first companion diagnostic approved along with crizotinib; more recently, an immunohistochemistry (IHC) companion diagnostic was approved by the FDA.40,41 The National Comprehensive Cancer Network (NCCN) has released recommendations regarding testing for ALK mutations. 16 The NCCN Panel recommends mutation testing in all patients with nonsquamous NSCLC and NSCLC not otherwise specified; patients should not be excluded from testing on the basis of clinical characteristics. ALK testing may also be considered in patients with squamous cell histology if the patient never smoked or if mixed histology was reported or small biopsy specimens were used for testing. The FISH assay is recommended; IHC testing may be considered for rapid prescreening, and cases that have positive findings can be verified using the FISH assay. Reverse transcriptase-polymerase chain reaction testing is not recommended for ALK testing. Broad molecular profiling systems, such as next generation sequencing, may also be used if designed and validated to detect ALK rearrangements. This has been strongly endorsed by the NCCN Panel (Category 1 recommendation) as it may be used to detect rare driver mutations that may aid in guiding therapy or patient inclusion in a clinical trial. 16
Resistance mutations
As seen with EGFR-mutant NSCLC treated with EGFR inhibitors and breakpoint cluster region (BCR)–Abelson murine leukemia viral oncogene homolog (ABL) mutant chronic myelogenous leukemia treated with ABL inhibitors, intrinsic resistance to ALK inhibitors has been observed in approximately 40% of ALK-positive patients.31,33 Crizotinib-induced secondary mutations in the ALK kinase domain, such as L1196M and G1296A, have been reported. Testing for secondary ALK mutations associated with acquired resistance to ALK inhibitors is not currently required for clinical management. 16 To date, seven acquired resistance mutations have been identified among patients treated with crizotinib. 42 ALK-L1196M is the equivalent gatekeeper mutation as seen with EGFR-T790M and ABL1-T315I. ALK-L1196M interferes with the binding of crizotinib to ALK by steric hindrance and allows for continued activation of ALK in the presence of crizotinib. 30 ALK-G1269A has also been reported in crizotinib-resistant NSCLC and may reduce crizotinib binding to ALK either by steric hindrance (similar to ALK-L1196M) or enhanced affinity for adenosine triphosphate. 30 Other mechanisms of resistance have not been fully elucidated, but include ALK amplification/alteration, v-kit Hardy-Zuckerman 4 feline sarcoma viral oncogene homolog (c-KIT) amplification, KRAS mutation, and EGFR mutation.30,33 Identification of resistance phenomena and the observation that the majority of patients treated with crizotinib relapse within the first year of treatment laid the groundwork for development of new, more potent ALK inhibitors that can overcome crizotinib-associated resistance.31,33
Ceritinib
For patients with ALK-positive NSCLC, treatment options after failure of crizotinib previously included only cytotoxic chemotherapy, palliative radiotherapy, or best supportive care. 31 Ceritinib (formerly LDK378; Zykadia, Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA) is an oral ALK inhibitor that also targets insulin-like growth factor receptor, insulin receptor, and ROS1.43–45 It demonstrates more potent antitumor activity than crizotinib in preclinical models 42 and was granted accelerated approval in 2014 to treat ALK-positive metastatic NSCLC patients who have progressed on or are intolerant to crizotinib based on tumor response rate and duration of response in a phase I clinical study. 45 Ceritinib is the first second-generation ALK inhibitor approved by the FDA through an accelerated approval process. 45 More recently, alectinib (Alecensa, Genentech, Inc., South San Francisco, CA, USA) was also granted accelerated FDA approval in December 2015. 46 These second-generation ALK inhibitors represent an important alternative for patients with ALK-positive NSCLC.
Preclinical studies
Preclinical studies of ceritinib indicate that it is highly potent and selective against ALK. At the cellular level, it was the only compound to inhibit EML4–ALK with 50% the inhibitory concentration of 200 pM. 43 In enzymatic assays, it was 20 times as potent as crizotinib. 42 It was also active against crizotinib-naïve and crizotinib-resistant (with or without ALK resistance mutations) NSCLC cell lines and patient-derived cells. 42 In vitro animal studies showed that ceritinib inhibited EML4–ALK-positive NSCLC growth in a dose-dependent manner, including in crizotinib-resistant mice xenografts. 43 Ceritinib was studied in mice, rats, dogs, and monkeys to elucidate its pharmacokinetic (PK) profile. It demonstrated low plasma clearance, half-life range of 6.2–26 h, good bioavailability with slow oral absorption, and a consistent PK profile across these animal studies. 43 In rat studies, ceritinib induced dose-dependent tumor regression and was well tolerated. Complete regression was seen at a dose of 25 mg/kg. 43 These compelling preclinical results led to pursuit of clinical studies in humans.
Clinical development
First in human phase I
ASCEND-1 (NCT01283516), the first-in-human phase I single-arm study of ceritinib, was performed primarily to determine the maximum tolerated dose (MTD) in ALK-positive malignancies; safety and antitumor activity were key secondary objectives. 31 Eligible patients were aged at least 18 years, had an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 2 or less, and had a life expectancy of at least 12 weeks. Patients enrolled into the dose-escalation phase initially received ceritinib at 50 mg daily continuously for a 21-day cycle. Although the logistic regression model allowed for escalation to 900 mg daily, the MTD was set at 750 mg daily due to persistent grade 2 gastrointestinal adverse events (AEs) and grade 3 alanine transaminase (ALT) elevations. 31 Patients enrolled in the expansion phase received ceritinib at 750 mg daily until development of disease progression or unacceptable toxicities or study withdrawal. In cases of isolated CNS metastases despite disease progression, continued treatment with ceritinib was allowed.
Response of ALK-positive NSCLC patients treated with ceritinib 750 mg once daily. 38
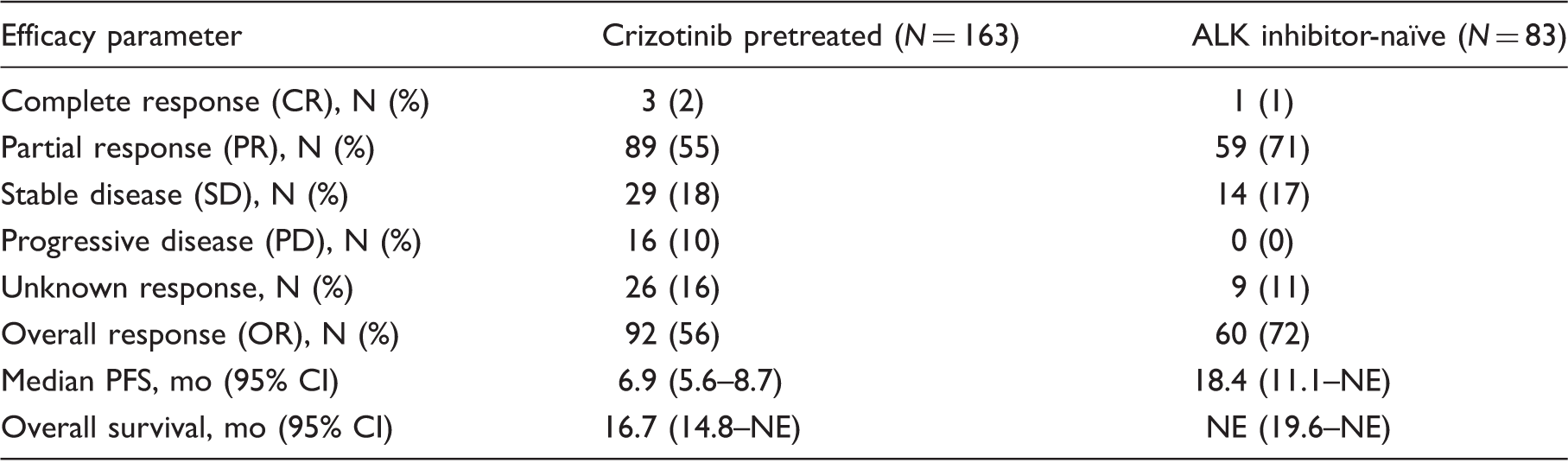
Note: CR defined as disappearance of target lesions, disappearance of nontarget lesions, and no new lesions. PR defined as CR or PR in target lesions, SD or no PD in nontarget lesions, and no new lesions. SD defined as SD in target lesions, no PD in nontarget lesions, and no new lesions. PD defined as PD in target lesions and any response in nontarget lesions independent of new lesions, any response in target lesions and PD in nontarget lesions independent of new lesions, any response in target lesions and any response in nontarget lesions and new lesions. Unknown defined as unknown response due to early study discontinuation. OR defined as combined CR and PR. ALK: anaplastic lymphoma kinase; CI: confidence interval; NE: non-estimable; NSCLC: non-small cell lung cancer; PFS: progression-free survival.
Phase II
Results from ASCEND-2 (NCT01685060), a single-arm, open-label, multicenter phase II study of ceritinib in patients with ALK-positive NSCLC previously treated with at least two lines of therapy including crizotinib, were recently published and are highlighted here.47,48 Because the phase I ASCEND-1 study showed responses in patients with brain metastases, intracranial and whole-body responses were assessed. In an analysis of 140 patients who were predominantly of White or Asian ethnicity, 100 patients (71.4%) had brain metastases and 20 patients (14%) had investigator-assessed measurable brain lesions at baseline.47,48 In this third-line population, the whole-body overall response rate was 38.6% in all patients, 33.0% in patients with brain metastases and 52.5% in patients with no brain metastases. The disease control rate was 77.1% in all patients, 74.0% in patients with brain metastases, and 85.0% in patients with no brain metastases. Median PFS was 5.7 months in all patients, 5.4 months in patients with brain metastases and 11.3 months in patients with no brain metastases. In the 20 patients with measurable brain lesions, the intracranial disease control rate was 80.0%.47,48 These data showed promising benefits of ceritinib in heavily pretreated patients with or without brain metastases. Overall, the study researchers concluded that ceritinib produced a significant, durable clinical response with a tolerable safety profile. 48
ASCEND-3 (NCT01685138) is an ongoing single-arm, open-label, multicenter phase II study of ceritinib in ALK-inhibitor-naïve patients with ALK-positive NSCLC. Patients who had received prior chemotherapy were allowed if they had received fewer than four lines. In an analysis of 124 patients with a June 2014 data cutoff, 50 had brain metastases and 10 had investigator-assessed measurable brain lesions at baseline. 49 The whole-body overall response rate was 63.7% in all patients, 58.0% in patients with brain metastases, and 67.6% in patients without brain metastases. The disease control rate was 89.5% in all patients, 86.0% in patients with brain metastases, and 91.9% in patients without brain metastases. Median PFS was 11.1 months in all patients, 10.8 months in patients with brain metastases, and 11.1 months in patients with no brain metastases. The intracranial disease control rate in patients with measurable brain lesions was 80.0%. These data also show a robust antitumor activity with ceritinib in ALK-inhibitor-naïve patients with or without brain metastases. 49
Dosing and administration
Ceritinib is available as a 150 mg strength capsule. Five capsules should be taken for the recommended dose of 750 mg once daily.31,45 In a clinical trial, approximately 62% of patients initiating treatment at the recommended dose required at least one dose reduction; the median time to first dose reduction was approximately seven weeks. 38 Discontinuation is recommended for patients who cannot tolerate 300 mg daily. 44 Ceritinib should be taken on an empty stomach and not within 2 h of a meal. A missed dose can be made up unless the next dose is due within 12 h. Ceritinib is considered a hazardous drug; healthcare professionals who handle ceritinib are advised to wear gloves. 50 Ceritinib should not be crushed.
There is currently an active phase I trial examining the MTD of ceritinib in pediatric patients for whom the contents of the capsule may be mixed with water and given via a nasogastric or gastric tube (NCT01742286). 51 Although the FDA labeling does not indicate whether ceritinib may be given through a nasogastric or gastric tube, the manufacturer is able to provide specific preparation instructions for enteral tube administration.
Clinical pharmacology in humans
Absorption, distribution, metabolism, excretion
Peak plasma level of ceritinib is achieved 4–6 h after administration. Maximum drug concentration total drug exposure increases proportionally with doses from 50 mg to 750 mg. Steady state was reached in approximately 15 days with 750 mg once daily dosing. 45 Absolute bioavailability has not been determined.31,44,45 Absorption of ceritinib is affected by food, and it should be taken on an empty stomach ideally 2 h after a meal.31,45,52 A ceritinib dose of 600 mg or greater taken with a meal is expected to result in systemic exposure exceeding the 750 mg recommended dose taken under fasting conditions.32,45,52 Ceritinib is 97% bound to plasma proteins. After a single dose of 750 mg, the volume of distribution is 4230 L. The half-life of ceritinib is 41 h. After a single 750 mg dose of ceritinib, 82% of the parent compound remained in human plasma, and 92.3% and 1.3% of ceritinib were recovered in feces and urine, respectively. 44
Drug–drug interactions
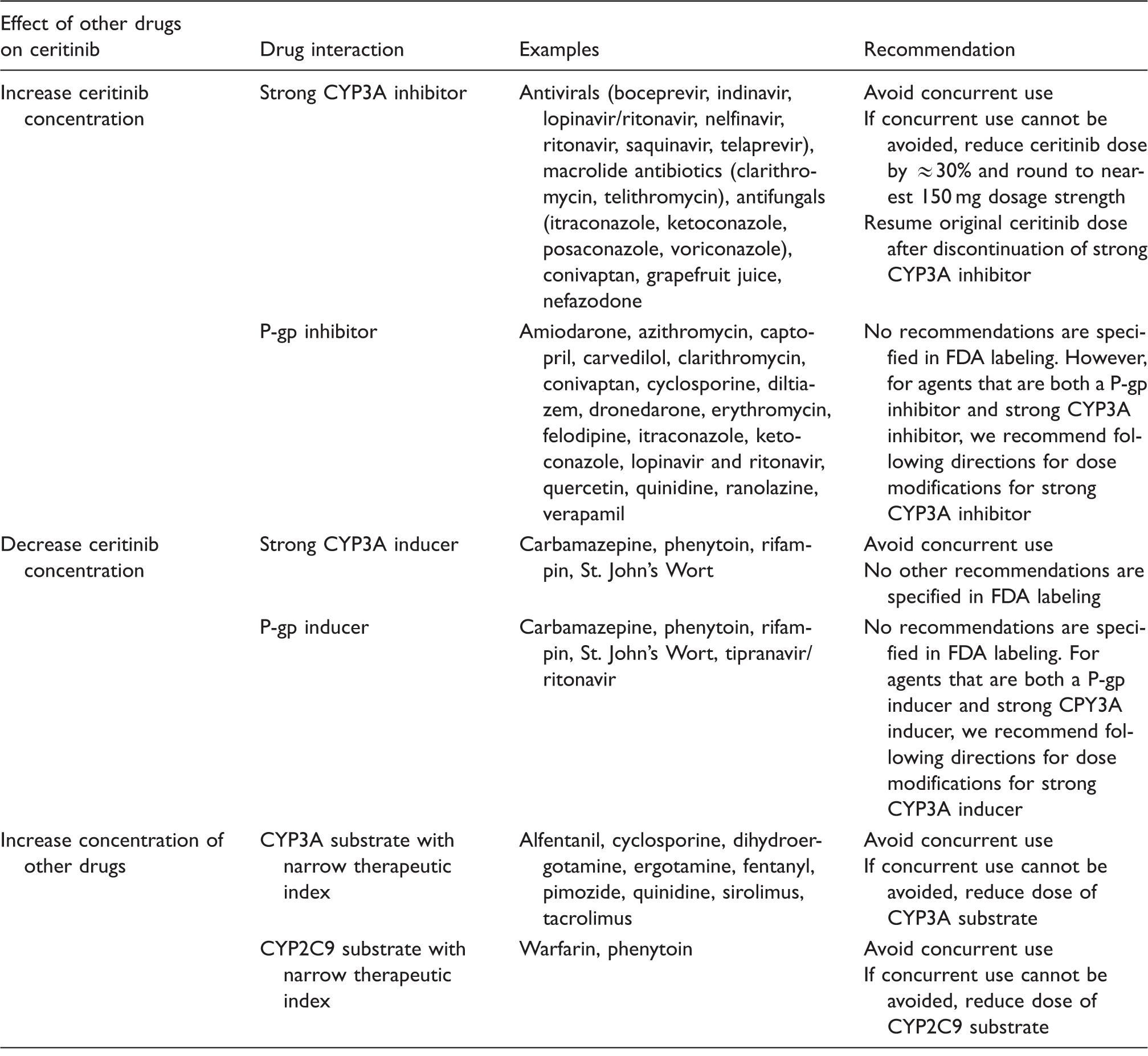
CYP: cytochrome P450; FDA: U.S. Food and Drug Administration; P-gp: P-glycoprotein.
Safety
Diarrhea, nausea, vomiting, fatigue, and abdominal pain are the most common adverse reactions in patients treated with ceritinib.31,38,47,48 These adverse reactions may be effectively managed with antidiarrheals, antiemetics, and fluid replacement. A recent report of a small case series showed that proactive management of gastrointestinal AEs prevented the need for ceritinib dose modification due to gastrointestinal toxicity in eight of nine patients. 54 Food effect studies in healthy subjects who received a single dose of ceritinib 500 mg found a reduction in gastrointestinal toxicities when ceritinib was administered with food, although similar improvements were not observed in subjects who received a single dose of ceritinib 750 mg with a light snack. 52 Because administration with food increases the concentration of ceritinib and subsequent risk for nongastrointestinal ceritinib toxicities, it is important that administration with food be avoided.31,45,52 The safety of using lower doses of ceritinib (450 mg and 600 mg) with food compared with 750 mg on an empty stomach is currently being evaluated in a randomized, open-label study (NCT02299505). 55
In the dose-escalation phase of the registry study, dose-limiting toxicities (DLTs) occurred with ceritinib daily doses as follows: with 400 mg, elevated ALT and hypophosphatemia; with 600 mg, dehydration; with 600 mg or greater, diarrhea; and with 750 mg, vomiting and nausea. All DLTs resolved with discontinuation of ceritinib. 31
In the updated results of ASCEND-1, all 246 patients with ALK-rearranged NSCLC treated with ceritinib 750 mg daily had at least one AE. 38 At least one grade 3 or 4 AE was reported in 81% of patients, and at least one serious AE was reported in 48% of patients.
Recommendations for dose modifications for ceritinib-related adverse events. 44
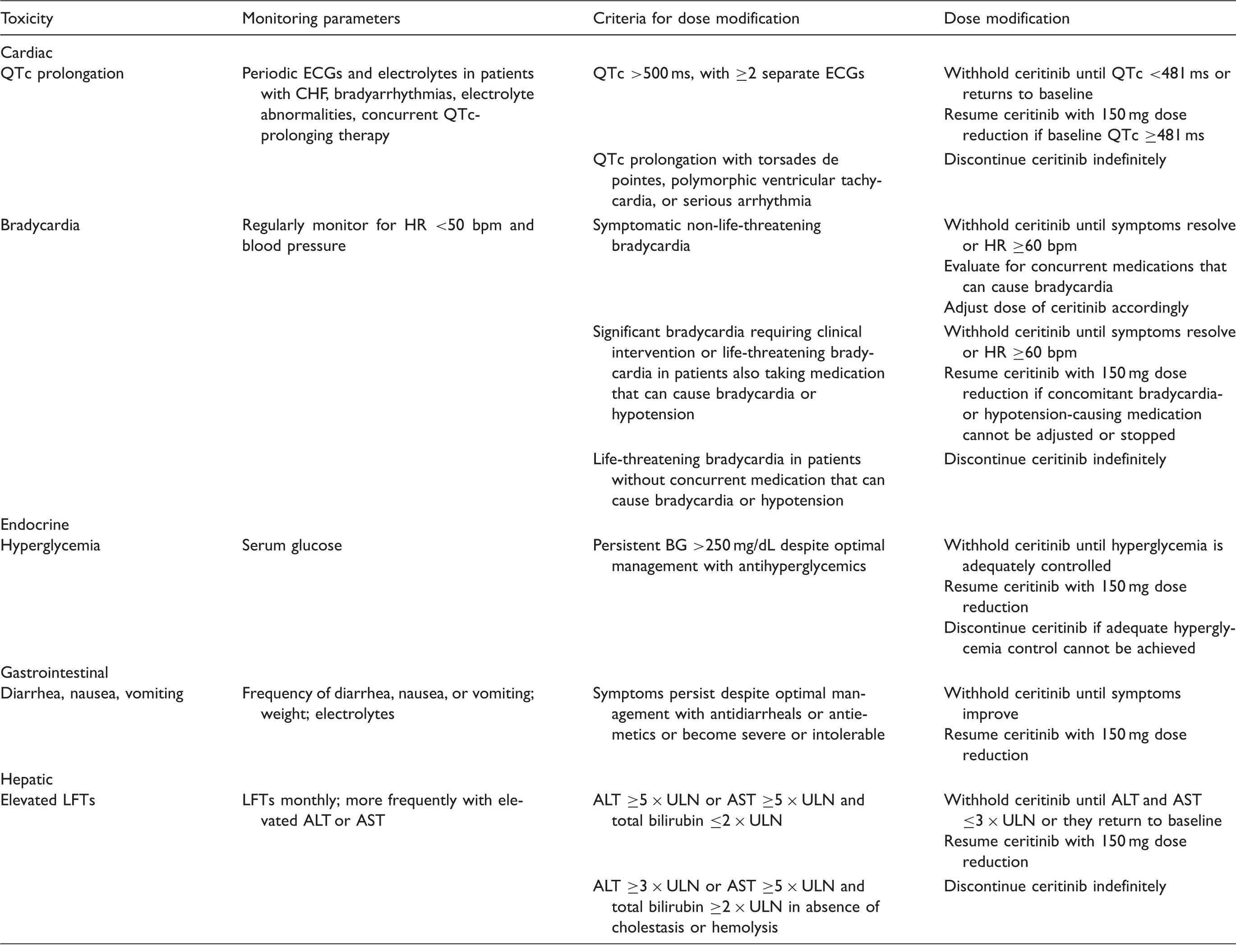
ALT: alanine transaminase; AST: aspartate transaminase; BG: blood glucose; bpm: beats per minute; CHF: congestive heart failure; ECG: electrocardiogram; HR: heart rate; LFTs: liver function test; QTc: corrected QT interval; ULN: upper limit of normal.
Ceritinib may cause hyperglycemia, and this effect is perhaps due to its inhibitory effect on insulin-like growth factor receptor and insulin receptor. 45 Grade 3 or 4 hyperglycemia was reported in 6% of patients and was reported as a serious AE in 2% of patients in the update of the ASCEND-1 study. 38 Of note, patients with uncontrolled diabetes were excluded from the study.34,38 A six-fold increase in the risk of grade 3 or 4 hyperglycemia in patients with diabetes or glucose intolerance and a two-fold increase in the risk of grade 3 or 4 hyperglycemia in patients taking corticosteroids have been noted with ceritinib treatment.32,46
Interstitial lung disease (ILD) or pneumonitis developed in 4% of patients (grade 3 or 4 in 3% of patients) in the update of the ASCEND-1 study. 38 Treatment-related AEs leading to discontinuation included increased blood alkaline phosphatase, decreased appetite, pneumonitis, increased ALT, increased aspartate transaminase, corneal infiltrates, hepatitis cholestatic, ILD, nausea, pain in extremity, pleural effusion, pleuritic pain, and acute renal failure; these each occurred in one patient and pneumonitis in two patients. 38 One case of ILD was fatal and was considered treatment-related. One other death that was considered to be treatment-related occurred in the context of infection and ischemic hepatitis. 39
Other safety considerations with ceritinib include increases from baseline of the corrected QT interval greater than 60 msec, which occurred in 3% of patients; of note, patients with impaired cardiac function or clinically significant cardiac disease were excluded from the study.31,38 It is advised that ceritinib be avoided in patients with congenital long QT syndrome. 44 During its development, bradycardia and sinus bradycardia have also been reported rarely; when possible, it is recommended to avoid concomitant use of agents known to cause bradycardia, such as beta-blockers, non-dihydropyridine calcium channel blockers, clonidine, and digoxin. 45 Serious AEs that have been reported in the phase I study of ceritinib include convulsion, pneumonia, ILD/pneumonitis, dyspnea, dehydration, hyperglycemia, and nausea. 44
Counseling points
Pharmacists are well positioned to inform patients of and discuss with them what they can expect with ceritinib therapy, particularly adverse reactions. Patients new to ceritinib therapy should be counseled. Ceritinib capsules should be taken whole on an empty stomach. 44 Patients should be reinforced to take all the capsules of their dose at once. Ceritinib can be stored at room temperature. With respect to adverse reactions, patients should be advised to contact a healthcare provider if symptoms develop, persist, or become severe or intolerable. Diarrhea, nausea, vomiting, fatigue, and abdominal pain are the most commonly reported adverse reactions. 38 Patients should receive proper counseling on the use of supportive care medications, particularly antidiarrheals. Patients should be advised to report persistent or severe gastrointestinal symptoms, and not build a tolerance to the diarrhea, and that dose modifications are often necessary for intolerable diarrhea not controlled with supportive care medications. 38
Liver injury is possible with ceritinib. 38 Signs and symptoms of hepatotoxicity include yellowing of skin or eyes, abdominal pain or swelling, loss of appetite, or fatigue. Ceritinib can cause severe or life-threatening inflammation of the lungs. 38 Patients are advised to report any new onset cough, shortness of breath, trouble breathing or chest pain. Cardiac adverse reactions, including abnormal heart rhythms and slowing of heart rate, have been reported with ceritinib. 45 Signs and symptoms include changes in heartbeat, palpitations, lightheadedness or modifications to heart or blood pressure medications. Hyperglycemia may occur with ceritinib. 38 Patients should be aware of development of frequent urination, increased thirst, headache and fatigue. In more serious cases, there may be blurred vision. Because ceritinib can cause fetal harm, females of child-bearing age should use effective contraception while being treated with ceritinib and for at least two weeks following discontinuation. The effect of ceritinib on human milk is unknown, and breastfeeding during treatment with ceritinib is not recommended. 44
In ASCEND-2, all patients experienced at least one adverse event, likely related to ceritinib in 96.4% of cases. 48 Gastrointestinal adverse reactions were most common with greater than 75% of patients having drug-related nausea or diarrhea. Approximately two% of patients discontinued ceritinib due to gastrointestinal adverse reactions. Grade 3 to 4 adverse events were reported in 71.4% of treated patients, with elevated liver enzymes being the most common. Among serious adverse events, 17.1% were suspected to be related to ceritinib. On the whole, ceritinib exhibited a safety profile that was consistent with the ASCEND-1 study and no new adverse events were noted. In addition to the observed antitumor activity, patients reported improvement in lung cancer-related symptoms. 48
Place in therapy
Non-small cell lung cancer is an aggressive lung cancer with limited treatment options. The enhanced potency of ceritinib against ALK-positive NSCLC and its demonstrated efficacy in crizotinib-naïve and crizotinib-resistant patients suggest that it may be a reasonable therapy for patients who are unable to tolerate or no longer benefit from crizotinib.31,38 This suggests that ceritinib activity may be independent of mechanisms of crizotinib-acquired resistance. The demonstrated antitumor activity of ceritinib in crizotinib-naïve patients31,38 suggests that with further evaluation, it may become a first-line option for ALK-positive NSCLC. A phase III study in previously untreated patients with ALK rearranged NSCLC is ongoing (NCT01828099).
With all new drugs, cost plays a role in determining place in therapy. The monthly cost of ceritinib is approximately $13,500. 56 Actual out-of-pocket costs will vary based on the patient’s prescription insurance coverage. The manufacturers of ceritinib, alectinib and crizotinib offer financial assistance programs for those patients who are uninsured or whose copayments are excessive. Pharmacists can often counsel both prescribing providers and patients regarding these programs. Cost-effectiveness studies have demonstrated that ceritinib may be considered a cost-effective option compared with current chemotherapies, including docetaxel or premetrexed.57,58
A review of approved second-line ALK inhibitors in NSCLC would not be complete without a summary of alectinib, and in this setting, how it compares with ceritinib. Similar to ceritinib, alectinib is a small molecule tyrosine kinase inhibitor of ALK and is indicated for patients with advanced ALK-positive NSCLC who have progressed on crizotinib. Results from two phase II trials that led to the approval of alectinib showed that it is highly clinically active, including CNS metastases, with durable response approximating 12 months.59,60 For both agents, case reports have demonstrated their activity in carcinomatous meningitis.61,62 Patients treated with alectinib experienced primarily grade 1 or 2 adverse reactions (like ceritinib) with less incidence of nausea, vomiting, and diarrhea. Instead, constipation (∼35%), fatigue (∼30%), and peripheral edema (∼24%) were the most common adverse reactions.59,60 Myalgia was also reported among approximately 20% of patients. According to FDA labeling, warnings and precautions for alectinib include hepatotoxicity, ILD, bradycardia, myalgia, and embryo-fetal toxicity. 63 These adverse effects are also seen with ceritinib, except for myalgia, and also include gastrointestinal toxicity, QTc prolongation, hyperglycemia, and pancreatitis. 44 Dose modifications are reasonably based on the respective adverse reactions.44,63 In contrast to ceritinib, alectinib requires twice daily dosing with food and confers a higher pill burden (600 mg is the recommended dose and it comes as a 150 mg strength capsule). 63
The selection of initial treatment of an ALK inhibitor after failure with crizotinib will be dependent on the patient’s pattern of disease progression, medical history, anticipated tolerance of adverse reactions, preference for dosing schedule and pill burden, and pharmacogenomics. More recently, there was a first patient report of ALK F1174V mutation conferring sensitivity to alectinib, and at the same time confirmation that acquired ALK I1171 mutation confers resistance to alectinib. 64 This suggests that acquired resistant ALK mutations produce differential sensitivities to ALK inhibitors and genomic profiling post-crizotinib may be beneficial in developing treatment sequences beyond first-line treatment.
Summary
Ceritinib represents a potent new generation of targeted therapies and offers ALK-positive NSCLC patients a much needed additional treatment option. Ceritinib was studied over a three-year period and approved by the FDA within four months of submission of New Drug Approval request. 45 Given the speed at which ceritinib was approved and became available in the clinical arena, it may also be the first example of how the new breakthrough therapy approval process is transforming the drug approval process. 45 Ceritinib’s approval was based on its efficacy, duration of response, and favorable toxicity profile (diarrhea, nausea, vomiting, increased transaminases, and hyperglycemia among the most common adverse reactions and laboratory abnormalities). 45 The rapidity of its debut from discovery to FDA approval provided an alternative therapy to ALK-positive NSCLC patients who historically have had limited options. 45 However, the complete side effect profile of ceritinib may not be fully known. Phase II studies are currently ongoing to confirm the efficacy results and further study the safety profile.
Footnotes
Acknowledgment
Medical writing and editorial assistance were provided by Michelle Yochum, PhD, and Shannon Davis of QXV Communications (Haddam, Connecticut).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for writing and editorial assistance was provided by Novartis.