
Abstract
Groups are a common clinical intervention for women survivors of intimate partner violence (IPV). This secondary mixed-methods analysis from a study of 567 Canadian women from the prairie provinces compared the mental health and well-being of 131 women who had attended a IPV group to 436 women who had not attended any group. Qualitatively, perspectives from 131 women (113 comments; 18 interviews) who attended some form of group treatment were analyzed. Of the 199 coded comments about the IPV groups, most were positive (157 or 78.9%), while the remaining 21.1% (42) reflected concerns or suggested changes. Clinical implications are provided.
Violence against women by intimate partners (IPV) has been recognized as a global phenomenon that leads to significant harm to women and their children (World Health Organization, 2021). Although we often focus on physical violence and its potential for lethality, thankfully, only a small proportion of women are murdered by partners (Dawson, 2016; Johnson et al., 2019). Sexual assaults by partners are relatively common, with almost one-fifth (18.3%) of American women reporting contact sexual violence by partners (Smith et al., 2018). This can result in serious mental health consequences in response to these often-serial marital rapes (Messing et al., 2014; Tutty & Nixon, 2022). While psychological or emotional abuse has long been considered a critical aspect of IPV, the term “coercive control,” which is more all-encompassing, has recently been seen as central to all forms of IPV (Sharp-Jeffs et al., 2018; Stark, 2007). Even after women separate from abusive partners, the IPV often continues through physical abuse (Brownridge et al., 2008) and coercive control (Rezey, 2020; Tutty et al., 2023).
The mental health consequences of these multiple aspects of IPV have been well-documented and can comprise significant depression, anxiety, and post traumatic stress disorder (PTSD) (Baird et al., 2021; Fedina et al., 2021; Tutty et al., 2021a), all of which indicate the need for clinical intervention. Although researchers such as Addington (2022) and Voth Schrag et al. (2021) describe the “many” women who do not engage with formal services, others identify a substantial proportion of IPV survivors who seek formal services such as counseling (Ravi et al., 2022; Tutty, 2023). The current study focuses on a service for women abused by intimate partners, support and therapy groups. We assessed potential differences between women who attended groups and those who do not from a large sample of abused women from Canada, and qualitatively examined women's impressions of their IPV group experiences.
Group Interventions for IPV
Groups are a powerful medium for counseling women abused by intimate partners (Trabold et al., 2020). IPV groups are often differentiated as offering either support or therapy. Schopler and Galinsky (1993) see group interventions as on a continuum with self-help or peer-led groups at one end, therapy groups at the other and support groups falling in the middle. The main difference between peer support groups and other support groups is their leadership (Kurtz, 1997). Whereas support groups are led by one or two professionals, self-help groups have at least one peer facilitator, who likely experienced IPV.
Support groups for abused women are an integral part of many shelters and community programs (Abel, 2000). Most are offered weekly and are relatively short (6–12 weeks), although groups in violence against women (VAW shelters) may be offered daily, as women's residence is often only about 21 days (Tutty & Rothery, 2002a). While some specify using a feminist model (i.e., Rinfret-Raynor & Cantin, 2007; Sharma, 2001; Singh & Hays, 2008), much of the teachings about IPV concepts used in support groups reflect a feminist understanding of the issue.
In 1984, Pressman described common themes in support groups for women abused by intimate partners. First, the safety of the woman is critical and, if she has not already made one, developing a safety plan is important. Denying or minimizing the IPV may become apparent and should be confronted in a supportive way or through education about the dynamics of IPV. The women may explore why they remained stayed in the abusive relationship as a mechanism to reduce their sense of self-blame. Assisting women to identify ways that they have resisted the abuse or acted to protect themselves and their children can positively impact women's self-esteem and sense of efficacy (Pressman, 1984).
Almost all IPV support groups include the opportunity for women to tell their stories to the extent to which they are comfortable (Larance & Porter, 2004; Moldon, 2002; Taylor, 2000; Tutty & Rothery, 2002b). Most offer information about IPV including concepts such as the “cycle of abuse” (Walker, 1979), red flags for abusive relationships, improving self-esteem, and generational abuse (Brandl et al., 2003; Moldon, 2002; Tutty et al., 1996, 2016). Sometimes termed “psychoeducational,” these include an interpersonal component, referring to the leaders using the group process to address psychological issues and group interaction, and teaching about IPV or behavioral skills.
More recently, IPV groups offered by psychologists have emerged, with most using Cognitive Behavior Therapy (CBT) (Crespo & Arinero, 2010; Santos et al., 2016) or Dialectical Behavior Therapy (DBT) (Iverson et al., 2009), a specific form of CBT. These tend to be highly structured around teaching skills specific to cognitions in general, not necessarily related to IPV. For example, Iverson provides a detailed list of the skills taught in each group session, including mindfulness and self-validation, with no mention of IPV.
Some IPV survivor groups are specific to the unique needs of older women (Brandl et al., 2003; Brownell & Heiser, 2006; Straka & Montminy, 2006; Wolf, 2001). Other groups focus on mothering in the context of IPV (Austin et al., 2019; Grip et al., 2011; Howell et al., 2015; Miller et al., 2014). More unusual group foci include one on group art therapy (Skop et al., 2022) and two on theatre interventions (Kumar, 2013; Wozniak, 2009), one on vocational and economic access (Chronister & Davidson, 2010) and one on Self-Defence Stress Management (Liu et al., 2013). Several (Ilardi & Kaslow, 2009; Kaslow et al., 2010; Taylor, 2000) were culturally specific to African American women, one was developed for South Asian American women (Singh & Hays, 2008) and one for immigrant women more generally (Sharma, 2001).
Peer-led groups for women abused by intimate partners have been described, although rarely studied (Fearday & Cape, 2004; Hartman, 1983; Tutty et al., 2017a, 2017b). The group leaders, themselves previously abused by partners, provide important role-models and benefit by bearing witness to other women in similar circumstances, sharing their stories and, thus, acknowledging their own healing (Tutty et al., 2017b). In addition to the group members benefitting from the role-models provided by the peer-leaders, women described benefits of participating similar to those in advocate-offered IPV support groups such as learning from the other women participants and improving self-esteem (Fearday & Cape, 2004; Hartman, 1983; Tutty et al., 2017a, 2017b).
Research on IPV Groups
A number of quantitative outcome evaluations of women's support and therapy groups for IPV have been conducted. These report statistically significant pretest/posttest improvements in areas such as self-esteem, anxiety, depression and PTSD (Allen et al., 2021; Arroyo et al., 2017; Cort et al., 2014; Crespo & Arinero, 2010; Liu et al., 2013; McWhirter, 2011; Santos et al., 2016; Trabold et al., 2020; Tutty et al., 1993, 2016).
Qualitative research that captures the voices of women who have attended IPV groups and provides information about the group process is less common. Exceptions include Matos et al. (2022), Moldon (2002), Preston (2002) Skop et al. (2022), Tutty and Rothery (2002a), Tutty et al. (2017a), and Zust (2006). As is common in qualitative research, the number of respondents is relatively small, six to ten in most studies, exceptions being Preston (2002) with 18 group completers, Matos et al. (2022) with 19 respondents and Tutty and Rothery (2002b) with 32 women from a shelter-based study, in contrast to the others which were all community-based.
The major themes from these qualitative studies include the benefits of connecting with other women (Matos et al., 2022; Moldon, 2002; Preston, 2002; Skop et al., 2022; Tutty & Rothery, 2002b; Tutty et al., 2017a; Zust, 2006), positive connections with the group leaders (Moldon, 2002; Skop et al., 2022; Tutty & Rothery, 2002b; Tutty et al., 2017a; Zust, 2006), improvements in self-esteem and resilience (Matos et al., 2022; Moldon, 2002; Skop et al., 2022; Tutty et al., 2017a; Tutty & Rothery, 2002b; Zust, 2006), knowledge about IPV dynamics (Matos et al., 2022; Moldon, 2002; Preston, 2002; Tutty et al., 2017a; Tutty & Rothery, 2002b) and generally positive reactions to groups (Moldon, 2002; Preston, 2002; Skop et al., 2022; Tutty et al., 2017a; Tutty & Rothery, 2002b; Zust, 2006).
Groupwork Issues With Women Survivors of IPV
The benefits of offering support in groups include the fact that groups reduce social isolation, a significant effect of being in an abusive relationship (Matheson et al., 2015). Group members encourage each other, allowing women to see that their reactions to the abuse are not unique. Group members may be at different stages in acknowledging that their partners have abused them and deciding how to respond. For example, some may have separated from their partners while others are in the process of deciding whether to do so. Learning from each other's experiences is a prime benefit of the group process, as mentioned previously.
Several studies have compared group models or group process issues. Liu et al. (2013) compared a support group for IPV survivors and a self-defence group, concluding that women with depression symptoms and self-esteem issues benefitted from either group. Mancoske et al. (1994) compared groups using a feminist model to a grief model, unexpectedly finding more significant improvements in self-esteem, self-efficacy, and positive attitudes to feminist beliefs in the grief groups. Tutty et al. (1996) found no program outcomes that could be attributed to group characteristics, although there were some advantages of two-leader groups over time. In this study, of all the benefits of group intervention, the sense of commonality, the “all being in the same boat phenomenon” (Yalom, 1995) relieved the guilt that many of the women had expressed.
Few articles discuss the group process in IPV support groups, exceptions being Chronister and Davidson (2010), Larance and Porter (2004) and Singh and Hays (2008). Chronister and Davidson described six group processes in detail, clarifying that the role of the group leader is to facilitate interaction between the women, rather than being an educator. Larance and Porter (2004) and Singh and Hays (2008) described the importance of engaging the women at intake, through building trust and supporting women's interactions. Discussing group process is important since, in many instances, the fact that the intervention was in a group appears to be irrelevant. This is especially so in structured groups promoting CBT or DBT in which, as mentioned, the therapeutic interventions (individual skill-training) are the major focus rather than group interactions, similar to conducting individual therapy in a group setting.
Rationale for the Current Study
As mentioned, while groups constitute a major counseling intervention for women abused by intimate partners, few studies have captured the women's impressions of their group experiences, and these are all qualitative (Matos et al., 2022; Moldon, 2002; Preston, 2002; Skop et al., 2022; Tutty et al., 2017a; Tutty & Rothery, 2002b; Zust, 2006). With unique access to a large study of Canadian women abused by intimate partners from three Western Canadian provinces, the goal of the current secondary data analysis was to examine the group counseling experiences of 567 women who had engaged with IPV programs, including groups, in terms of their demographic locations, IPV, and mental health severity to determine any important differences between group members and nongroup members.
There is a paucity of studies on the counseling experiences of Indigenous women abused by intimate partners (exceptions being Ogden & Tutty, 2024; Riel et al., 2014). Given that over half of the women in the current study were Indigenous, we considered this an important focus. In Canada, Indigenous women experience more severe IPV (Brownridge, 2008; Romans et al., 2007). In the General Social Survey (GSS) on Victimization in Canada (Statistics Canada, 2011), with data collected in 2009 (closest to that in the current study), Canada's three prairie provinces (sites of the current study) had the country's highest rates of self-reported spousal violence (national average = 6%; Saskatchewan = 8.2%; Alberta = 7.6%; Manitoba = 7.4%). Indigenous people in the prairie provinces constitute 39.2% of the First Nations population and 50.4% of the Métis population in Canada. As such, the current study may add important context to questions about Indigenous women's participation in IPV groups.
Method
This exploratory secondary analysis used a mixed-methods approach (Long-Sutehall et al., 2010; Sandelowski, 2000), including both quantitative and qualitative components. The data were from the “The Healing Journey,” a longitudinal, Canadian study with a convenience sample of 665 women who had experienced IPV in the three prairie provinces of Alberta, Saskatchewan, and Manitoba. The original study aimed to assess the characteristics of women abused by intimate partners including their mental health and general well-being (Tutty et al., 2021a), experiences of mothering (Ateah et al., 2019; Nixon et al., 2017), and following the women over 2.5 years (Tutty et al., 2021b). Data were collected in seven waves between 2005 and 2009, with one wave specific to an economic analysis (DeRiviere, 2014). In addition, to provide the women the opportunity to share their own stories, in-depth interviews were conducted with 90 women from the original 665 in 2005–6.
The current study used mixed methods, including standardized measures, to quantitatively assess potential differences between women who did and did not access group services. The women were asked whether they had ever participated in a counseling program, the type of program, and comments about the programs. The current analysis focuses on comments specific to having participated in a group. These were generally short, ranging from one-word to up to five sentences.
Study Participants
The research protocols were approved by the Research Ethics Boards of the six associated universities (Universities of Manitoba, Calgary, Regina, Brandon, Winnipeg, and Lethbridge). Each province conducted an environmental scan of agencies (i.e., women's shelters and counseling agencies) to cover urban, rural, and northern sites from which to recruit, so most women were engaged through IPV-specific services. The criteria for inclusion were as follows: minimum 18 years of age, the most recent incident of IPV no sooner than three months and no longer than five years prior, commitment to stay in the study for the full four years, and no debilitating mental health issues. Honoraria ($50 CAN) were given to participants at each wave.
Research Procedures: Quantitative Component
Data in the original study were collected with respect to four major areas: demographic background and history of abuse, general functioning and service utilization, health, and mothering over four years. The surveys included standardized measures as well as open- and closed-ended questions developed specifically for the study (all administered verbally by trained research assistants). The current mixed-methods secondary analysis used data from the first two waves of the Healing Journey study. The core demographics, including the severity of IPV of the total sample, and women's comments with respect to the counseling they received were obtained in Wave 1. The mental health measures were collected in Wave 2.
Intimate Partner Violence. The nature of the IPV was assessed by the Composite Abuse Scale (CAS) (Hegarty et al., 2005). This screening measure consists of 30 items rated for frequency in the past 12 months on a six-point scale from never to daily, with a possible total of 150. The four subscales are as follows: Severe Combined Abuse (8 items; range of scores 0–40; suggested cut-off of 1), Physical Abuse (7 items; range of scores 0–35; cut-off of 1), Emotional Abuse (11 items; range of scores 0–55; cut-off of 3), and Harassment (4 items; range of scores 0–20; cut-off of 2). The suggested clinical cut-off for the Total CAS score is 3 or 7 to minimize false positives. The scale has demonstrated convergent and discriminant validity (Hegarty et al., 2005). Cronbach's alpha for the CAS in the current study is .93.
Child Abuse. Child abuse history was collected via structured questions (yes/no answers): “Were you abused as a child or adolescent? (a) physical, (b) sexual, (c) emotional/psychological, (d) witnessing abuse among family members” (consistent with Elias et al., 2012) (Elias et al., 2012).
Mental Health and Well-Being. The Symptom Checklist Short Form (SCL-10) (Nguyen et al., 1983) is a screening tool to assess global mental health functioning and psychological distress in the previous week. Items (e.g., “In the past week, how much were you distressed by feeling lonely?”) are endorsed with a 0 to 4 Likert scale (0 = not at all; 4 = extremely). Higher scores indicate more distress. Published clinical cut-offs for the 10-item version were not found. However, since clinical cut-off scores are one standard deviation above the mean (Jacobson et al. 1984), we used Müller's data (Müller et al., 2010) reporting a mean score of 7.8 (SD of 6.3), resulting in a clinical cut-off score of 14.2. Cronbach's alpha in the current study is .89.
The CES-D-10 (Centre for Epidemiological Studies—Depression) is a short form of the CES-D-20 (Radloff, 1977) used to document depression symptoms in the previous week (Andresen et al., 1994). Ten items (e.g., “In the past week I was bothered by things that usually don’t bother me?”) are rated on a 0 to 3 Likert scale, with zero as rarely or none of the time (less than 1 day)” and three as all of the time (5–7 days). Internal consistency and test-retest reliability are good (Björgvinsson, et al., 2013). Cronbach's alpha in the current study is .84. Björgvinsson et al. suggest that a cut-off of 15 has the best sensitivity and specificity.
The PTSD Checklist (PCL) (Blanchard et al., 1996) is a 17-item self-report questionnaire that measures PTSD symptoms in the past month. Items (e.g., “In the past month how much have you been bothered by repeated, disturbing memories, thoughts or images of abuse or violence?”) are endorsed with a 0 to 4 Likert scale with zero meaning not at all and 4 meaning extremely. Blanchard et al. recommend a clinical cut-off of 44. The scale has good psychometric properties (Cronbach's alpha = .94; Blanchard et al., 1996). Cronbach's alpha in the current study is .92.
The original 25-item Quality of Life Questionnaire (Andrews & Withey, 1976) was shortened by Sullivan and Bybee (1999) to nine items (QoL-9) measuring satisfaction with her overall quality of life (e.g., “How do you feel about life as a whole”) and satisfaction with particular areas (e.g., “How do you feel about yourself?; your personal safety?; the amount of fun and enjoyment you have?”). Items are rated on a 7-point scale (1 = extremely pleased, 7 = terrible) and are summed with a range of 0 to 63. Higher scale scores indicate better QoL. Cronbach's alpha in the Healing Journey study is .84.
Quantitative Data Analysis
The demographic characteristics of the women and their scores on the CAS and mental health measures are presented descriptively. Demographic characteristics of the women and the perceived helpfulness of the counseling are compared using Pearson's chi-square analysis based on whether they had sought counseling, with effect sizes calculated with Phi or Cramer's V. Standardized residuals were calculated to identify the category differences responsible for the statistically significant chi-square analysis (Field, 2009). Effect sizes were interpreted using Rea and Parker’s (1992) suggested benchmarks of under .10 as a “negligible” association; between .10 and under .20 as a “weak”; between .20 and under .40 as a “moderate”, and between .40 and under .60 as a relatively “strong” association (p. 203). The mean scores on the standardized measures were compared with independent t-test based on whether or not they had sought counseling for IPV. Cohen's d (Cohen, 1988) is used to interpret statistically significant t-tests with a d between 0.2 and 0.3 considered as a ‘small’ effect size, 0.5 representing a ‘medium’ effect size, and 0.8 a ‘large’ effect size.
Research Procedures: Qualitative Component
In addition to the quantitative focus, two qualitative components were investigated for the current analysis. First, in Wave 1, the women were asked to describe and to comment on any IPV counseling they had accessed. Secondly, 90 women from the original sample were randomly chosen to be interviewed to allow the women to tell their stories from their own perspectives. The semistructured interviews were designed by a subgroup of Healing Journey team members, to add depth and context to the respondents’ experiences. Each woman was asked to begin where they thought their journey/story of IPV began, where that journey/story is at today, and where they think it is taking them in the future. Notably, no interview question was specific to any form of counseling. Honoraria of $50 CAN were provided to participants at each wave and for the one-time qualitative interviews.
The qualitative interviews were conducted in 2007 and 2008, about halfway through the longitudinal study. The interviews took approximately 2 to 2½ hours, scheduled at times and locations convenient to the participants. The research assistants who had administered the quantitative component at each wave were trained to conduct qualitative interviews. The interviews were audiotaped and transcribed verbatim. The research protocols for both the original and the qualitative interview component were approved by the Ethical Review Boards of the six associated universities (blinded for review).
Qualitative Data Analysis
We used descriptive qualitative health research to analyze the women's comments about their counseling. This method is particularly appropriate for mixed-methods research (Neergaard et al., 2009) and for “assessing, developing and refining interventions with vulnerable populations” (Sullivan-Bolyai et al., 2005, p. 127). Descriptive qualitative methods use the practicality of the research question as the guiding principle, rather than epistemological confines of qualitative traditions such as grounded theory or phenomenology (Neergaard et al., 2009).
Secondary qualitative analysis entails a re-analysis of already-available narratives (Heaton, 2008). The 113 comments and sections of any of the 18 interviews that described participating in an IPV group were analyzed together. The qualitative analysis followed established qualitative content analysis processes. We identified the major themes, subthemes, and categories (Graneheim & Lundman, 2004; Neergaard et al., 2009). First-level coding entailed word-by-word scrutiny of the comments to identify prominent themes and subthemes (Braun & Clarke, 2006). Second-level coding involved looking within the themes and subthemes to identify similarities, differences, and gaps using the constant comparative method (Thorne, 2000).
Some typical mechanisms to establish trustworthiness in qualitative research, such as member-checking, are not possible in secondary qualitative analysis (Yardley et al., 2014). However, consistent with Lincoln and Guba (1985), the quotes were triangulated by source (more than one respondent raising similar issues), analyst, and negative case analysis and this triangulation was used to establish dependability.
Results
Demographics of the Study Participants
The 567 women respondents (85.3% of the total 665) who had attended at least one IPV program had an average age of 36.9 years (SD = 10.9), while their partner/ex-partners had an average of 39.2 years (SD = 11.2). The women's racial backgrounds were 47.5% Indigenous, 46.1% White, and 6.4% Visible Minority, while the partner/ex-partners were White (51%), Indigenous (41.4%), and 7.7% Visible Minority. The majority of the women (90.7%) had children.
The women primarily lived in large urban centers (73.4%) with populations of more than 100,000, with 13.2% in smaller urban centers (30,000 to 99999) and 13.4% in rural centers (less than 29,000). With respect to their highest level of education, 39.8% of the women had not completed high school, 21.6% had completed high school, while 38.7% had some postsecondary education, either in technical institutes (18.4%) or universities (20.3%).
Their average total income in the past year was $23,500 (SD = $25,787); about half of the women's incomes fall below the poverty line for that time in the three Canadian provinces (DeRiviere, 2014). This low yearly income is partly explained by the fact that the majority of women (59.4%) were not currently working, another 18.5% worked casually or part-time, and only 22.1% worked full-time. With respect to their own history of child maltreatment, 21.4% reported none, 23.7% reported child abuse not including child sexual abuse, and over half (54.9%) had been sexually abused as children. A little less than two-thirds of the women (65%) had stayed in a VAW shelter at least once.
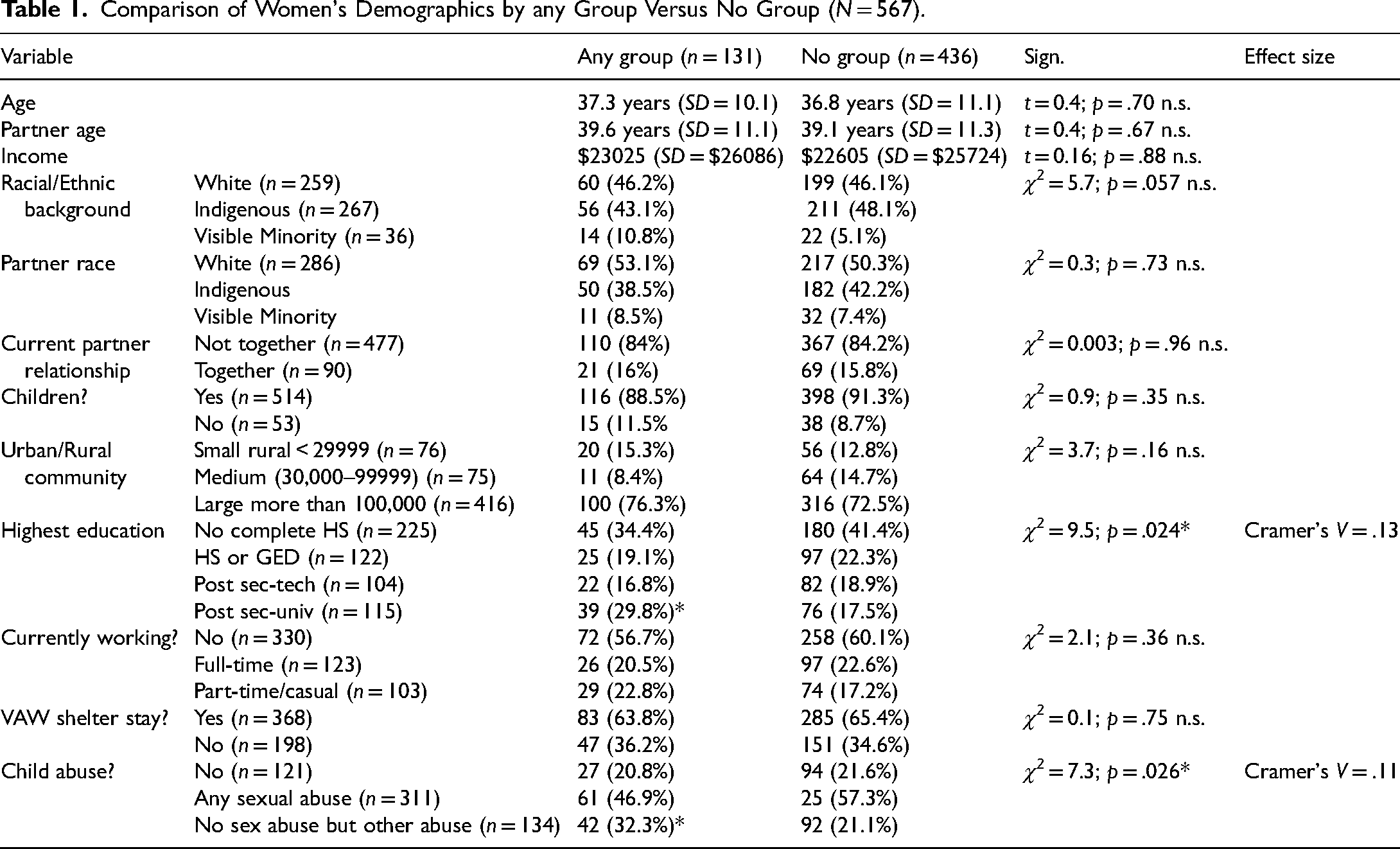
Differences Based on Any Group Counseling Versus None
The demographics of the women who had attended groups were compared to those who had not (see Table 1). Only two demographic characteristics differentiated women who had as compared to women who had not attended any group. More women who had group experience had attended university or college and more had been abused as children but not sexually abused.
Comparison of Women's Demographics by any Group Versus No Group (N = 567).
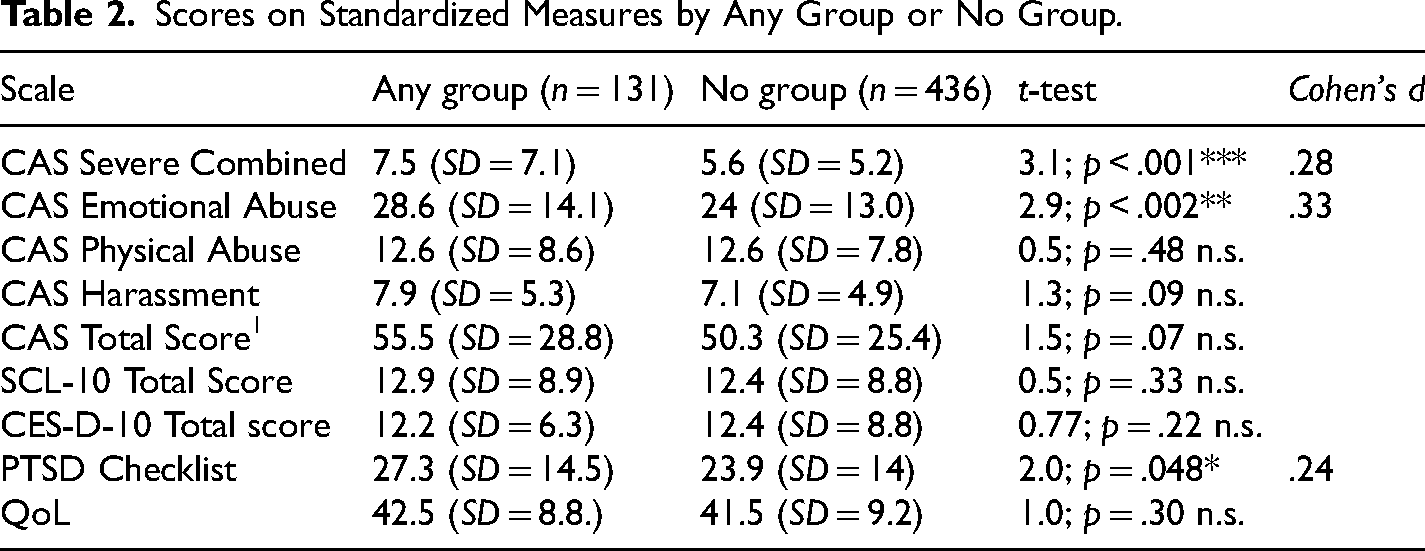
As can be seen in Table 2, average scores on the CAS subscales for all the women were well above the suggested clinical cut-off scores. None of the average scores on the measures of mental health functioning were in the clinical range. Women who attended any form of group had significantly more serious IPV on the CAS Severe Combined and Emotional Abuse subscales and on the PTC.
Scores on Standardized Measures by Any Group or No Group.
Qualitative Themes
The qualitative secondary analysis is based on 113 comments and 18 in-depth interviews with women who mentioned having participated in an IPV survivor group (a total of 131). As mentioned, the comments and interview sections that noted any IPV group membership were qualitatively analyzed together. The comments and interviews were relatively evenly spread across the three provinces (Manitoba: 39 comments, 6 interviews; Saskatchewan: 32 comments, 4 interviews; Alberta: 42 comments, 8 interviews). Twenty-nine comments and 10 interviews were with respect to groups offered in VAW shelters, and twenty comments and five interviews were about groups offered by community agencies. As many of the women's qualitative responses referenced more than one issue, these were coded into different categories. Of the total of 199 coded issues, two major themes emerged: 1. comments about group benefits and 2. comments about the group process or design. To provide additional context for the comments, the racial background of the women's comments was added to any direct quotes.
Comments About Group Benefits. A total of 148 comments (74.4% of 199) fit this first major theme. The categories were as follows: 1. hearing other women's stories (47 comments); 2. generally positive about group (45 comments); 3. information about IPV (35 comments); 4. self-reflection/self-esteem (16 comments); and 5. the importance of referrals (5 comments).
The importance of hearing other women's stories was the most mentioned comment about the groups (42 comments), including for example: “It helps me realize I am not alone. It helps me heal when I hear others talk of their problems and I share mine. People share their ideas of healing and that helps (Indigenous)” and “It was one of the most revealing experiences of my life (White).” More comprehensive descriptions are from in-depth interviews with two other women: Gloria tells her story, then Charity. We’re all sitting at that table [saying,] “That's what happened to me.” “Oh, that happened to me, too.” I heard all those stories from those women, and I said, “Oh my.” I’m not even in the worst situation. It's like one big family. I’m not embarrassed any more. They (partners) should be the ones who are ashamed. They are the ones who are doing this on us. We are just the victims. (Visible Minority) I heard the women, and it was like they were repeating my story. For months I never talked: I just listened. Finally, I shared my story. I remember crying and feeling a huge relief and the women looked back at me like they understood. I didn’t feel judged. I didn’t feel foolish. I had never told anyone about the abuse. (Visible Minority)
Others commented in more depth about why they liked the groups, including “I liked the structure—that every week I had someone to talk to. This anchored me (White);” “The recent group experience was good because I was at point where I was opening up and it was comforting to be in a group setting (White);” and “felt respected, encouraged to keep going, nonjudgmental, networks and they believe your situation (White).” The sharing circle is both spiritual and peer driven. Women from different backgrounds, not all abuse victims, but all have the desire to improve our lives for our children. (White) It's a structured fourteen-week support group for IPV. They focus more on positive healing than on the abuse itself, which is cool. It does bring up stuff but it's really positive. I’m going take it again when I’m in the right mind space. (White) Remember the cycle of change, where you have escalation then the abuse, then the honeymoon period and that same cycle starting again with the put downs and the verbal abuse and leading up to the intensity and the provocation. I got to recognize that volcanic period, that intense period before the abuse started again. (White) I understand more about verbal and emotional abuse, abuse in my childhood that I never thought of as abuse. I discovered that adult children (of alcoholics) can be abusive. I thought of abuse as physical and sexual but discovered verbal abuse can be a vicious cycle. (White) Because of them, I was able to get my self-esteem back. I see it as a life-long journey; You probably never get to where you want to be but at least you could proceed without feeling that you’re not living up to somebody else's expectations. And to give you confidence that you could make the changes. (White) Helped me realize that I was a fairly intelligent human being and had done good things with my life. I brought up three children who have done extremely well. I have wonderful grandchildren. They taught me to accept myself; helped with my self-esteem. (White)
Comments About Group Process or Design. A total of 51 comments were about group process issues and leadership. The categories were as follows: 1. length, timing and access to group (11 comments); 2. not liking group (11 comments); 3. problems with other group members (10 comments); 4. safety/relevance issues (8 comments); 5. positive group leadership (9 comments); 6. readiness for group (6 comments); and 7. negative group leadership (5 comments).
Eleven women commented on group structure issues such as length (5), timing (4) and access to the group programs (2). With respect to program length, all five comments expressed a wish for longer groups; “They put restrictions on how long you can attend group sessions. This is not helpful. A lot of women don’t have outside support. One falls back to the abuser because he is still haunting you (Indigenous);” “I need more time with the Wednesday evening group. One year was not good enough as things take me a little longer (Indigenous);” and “None of the counseling around here is long term. I’ve had enough short term. And it's the same issues; I don’t want to discuss it again. This is the problem, let's get this worked out (Indigenous).”
Of the eleven comments about group structure, four women mentioned the timing of the group sessions: “It's important to start within six months of leaving because women get stuck, and the feelings will always come up, even in future relationships (White).” And “I couldn’t go anymore because after this there were afternoon sessions. One time per week and I couldn’t get childcare (White).” The final two comments were about difficulties accessing the groups: “It took me a long time to get into Klinic [community agency]. [Child welfare] wanted me to go there, and when I met with them, they were like, ‘You can probably teach the training, so we can’t really help you (Indigenous)’” and “The only downfall was accessing the service. I basically stumbled upon Family Services not knowing what was available to whom (Indigenous).”
Eleven comments were with respect to not liking groups, including “I didn’t really like it. It's hard to communicate in a group setting (White);” “I’m scared to say some things due to them phoning [child] welfare on me (Indigenous);” “Not helpful because you were forced to participate (this was in a VAW shelter) (Indigenous);” “As much as I’m trying to get out there, I’m not comfortable with groups (Indigenous);” and “Telling my story was difficult. Not helpful and left me wondering what good it did (White).” Four comments indicated a preference for one-to-one counseling “Used to one-on-one, not group counseling (Indigenous)” and “I would be more comfortable with one-on-one. Someone I could talk too. But they wouldn’t give that to me (Indigenous).”
Nine comments raised concerns about the behaviors of some other group participants, including “Some women were very self-involved whereas I’m very private and not trusting of other people (Visible Minority);” “Other participants not particularly helpful (White);” “Clicky groups. Women very battered here (White);” and “At that time, I had 3.5 years sobriety. It wasn’t helpful to be with other girls with addictions (White).”
An additional nine comments were about positive behaviors of the group leaders, including “The people who work here are fantastic. I found it hard to trust them at first, but now I know I won’t have to pay for their kindness in other ways. I am more trusting of their kindness now (White);” “Counsellor is very caring—very gentle, soft spoken, I feel safe with her (White);” “counselor—good listener, very nonjudgmental, good connection (White);” and “The few I like to talk to listen with their hearts and that makes me feel good (Indigenous).”
In contrast, six comments described negative characteristics of the group leaders, including “Didn’t find counseling to be helpful—tried to tell me what to do and were judgmental (Indigenous)” and “Control of group could have been better (moving along the women who were holding up the discussion) (White).” Support groups are helpful depending on which counselors I talk to. I expected not to be judged, to vent my frustrations without being told how to think, do and behave. My expectations were not met with some counsellors. Two of them I avoid. They make me feel stupid and I am not a stupid person. Sometimes I walk out more stressed than when I walk in. They like to push buttons. (Indigenous) Family Counseling had two sixteen-week sessions, once a week all day. The first 16 weeks I just went there to cry. I completed that course, but I didn’t really learn anything. But the next winter they had the same class and the counsellor said she wanted me to take it again. So, I went again, and I learned a lot of things. (White) (Interviewer: You said you weren’t ready for a program.) I wasn’t. I was still in this relationship, and I think that I needed out of the relationship in order to explore the grief around that whole experience and my own loss of self. (White)
Discussion
There were few demographic differences between the women who attended IPV groups versus those who did not. More group attendees had postsecondary university education and more reported child abuse histories that did not include child sexual abuse. On the IPV and mental health measures, group attendees reported significantly more IPV on the Severe Combined and Emotional Abuse subscales of the CAS and more PTSD symptoms. There were no differences between group participants and nongroup participants with respect to how many had resided in VAW shelters (about 64%), so this does not explain the differences in group treatment engagement. It may be that the severity of the IPV and the PTSD symptoms prompted these women to attend an IPV group, but this would need further study. Notably, most evaluations of IPV groups do not have a comparison group of nongroup attendees, a strength of the current analysis.
The combined sample size of 131 women (113 comments; 18 interviews) is considerably larger than most previously published qualitative studies of IPV group counseling for abused women. The qualitative analysis identified most of the themes that previously emerged in other qualitative studies of IPV groups such as the benefits of connecting with other women (Matos et al., 2022; Moldon, 2002; Preston, 2002; Skop et al., 2022; Tutty & Rothery, 2002b; Tutty et al., 2017a; Zust, 2006), generally positive reactions to groups (Moldon, 2002; Preston, 2002; Skop et al., 2022; Tutty et al.,2017a; Tutty & Rothery, 2002b; Zust, 2006), knowledge about IPV dynamics (Matos et al., 2022; Moldon, 2002; Preston, 2002; Tutty et al.,2017a; Tutty & Rothery, 2002b), improvements in self-esteem and resilience (Matos et al., 2022; Moldon, 2002; Skop et al., 2022; Tutty et al.,2017a; Tutty & Rothery, 2002b; Zust, 2006), and positive connections with the group leaders (Moldon, 2002; Skop et al., 2022; Tutty & Rothery, 2002b; Tutty et al.,2017a; Zust, 2006).
Negative comments about the groups or the group process were seldom highlighted in other qualitative studies. Similar to the current qualitative analysis, there were concerns that the groups were too short (Matos et al., 2022; Preston, 2002) or needed a follow-up group program (Tutty et al. (2017a). Few other studies mentioned concerns about the behavior of other group members, exceptions being Preston (2002) and Tutty et al. (2017a), or noted concerns about some group leaders (Tutty et al., 2017a). The readiness to attend a group, whether because of trauma or the stage in the relationship with the abusive partner, is an important aspect to discuss with referred women clients.
Implications for Groupwork With Women Survivors of IPV
According to the majority of the women in our study, attending groups for women survivors of IPV was generally valuable. Considering the women's comments describing the groups they had attended, all seem to be support groups rather than more therapeutically focused groups such as CBT or DBT. Given that the interviews were conducted in 2005/2006, this makes sense, since research about CBT, DBT, theatre or arts-based group formats mostly emerged after this date, examples being Santos et al. (2016), Crespo and Arinero (2010), Iverson et al. (2009) and Skop et al. (2022). The availability of some of these more recent but somewhat esoteric group programs is unknown.
The most common positive theme was with respect to connecting with the other women group members. Leaders with an understanding of the group process are more likely to identify and support conversations among the group members to facilitate learning from each other. In contrast, group leaders need to respond appropriately to group members who present difficult behaviors such as monopolizing the group or behaving disrespectfully to other members (i.e., Moldon, 2002).
The negative comments largely represented concerns about the women's readiness, groups length/availability and concerns about the participation of some group members, consistent with several group program evaluations that mentioned similar concerns, such as needing a longer group, a follow-up group and scheduling (Fearday & Cape, 2004; Preston, 2002). Some of these issues could be dealt with using in-depth screening mechanisms to ensure the appropriateness of the group model for potential members. The mandated program mentioned was in a VAW shelter where women were given no choice about participating. Forcing women to attend programs is not common and not recommended.
A more pressing concern is the availability of quality programs that address the needs of multiple clients. Virtually all of the groups mentioned by the women in the study were offered by nonprofit agencies that often struggle to fund their programs, giving them little flexibility in providing more comprehensive or follow-up programming as some women wished for.
The extent to which groupwork skills are taught in clinical professions such as social work and psychology is either diminishing or has always been limited (Drumm, 2006; Simon & Kilbane, 2014). Agencies or shelters offering groups for IPV survivors could provide in-house groupwork training to educate the leaders to encourage more interpersonal interactions. While IPV concepts provided in the groups were often seen as valuable by the current study informants, rather than becoming the central focus of the groups, these concepts can be introduced briefly with a subsequent discussion among group members, or when the ideas fit with the experiences of a group member.
Limitations and Strengths of the Current Study
With secondary analyses, one is limited by the nature of the original study, which, in this case, relied on a convenience sample of women from VAW shelters or counseling agencies. The current results are not generalizable to other women abused by intimate partners from Canada's prairie provinces, as most were engaged through IPV-specific services, which increases the likelihood that they had received some form of counseling for IPV. The women were not asked specific questions about any group experiences, either in the quantitative comments or qualitative interview components of the Healing Journey study. As such, they may simply not have remembered or chose not to mention IPV groups.
The fact that the data for the original study was collected in 2004–2008 is a limitation, although secondary analyses may be conducted on data that is decades older (i.e., see the study by Brownridge et al. [2011] that used data from 1993). Further, although the recent published literature is more focused on therapeutic models offered by professionals such as CBT and DBT, VAW shelters and community agencies continue to offer support that mirror those described by the women in the current study (i.e., Liu et al., 2013; Rinfret-Raynor & Cantin, 2007; Singh & Hays, 2008; Tutty et al., 2016).
Most research on IPV groups, whether quantitative (Allen et al., 2021; Arroyo et al., 2017; Cort et al., 2014; Crespo & Arinero, 2010; Liu et al., 2013; McWhirter, 2011; Santos et al., 2016; Trabold et al., 2020; Tutty et al., 1993, 2016) or qualitative (Matos et al., 2022; Moldon, 2002; Preston, 2002; Skop et al., 2022; Tutty et al., 2017a; Tutty & Rothery, 2002b; Zust, 2006), focuses on one or two specific group programs. The current analysis provides the opportunity to assess strengths and weaknesses of various programs from a large group of counseling seeking women, to examine similarities or differences.
A strength of the current study is that the women constitute a large sample of intimate partner violence survivors from the Canadian prairies, with more than half of Indigenous background, a group whose well-being is particularly important in Canada but who may not be included in IPV research. Although we did not compare the Indigenous women's comments in group counselling to non-Indigenous women, no obvious differences emerged. It should be noted that “talking circles” are an Indigenous culturally appropriate strategy similar to what occurs in mainstream support groups (Ogden & Tutty, 2024; Sabri et al., 2019). The women's candor with respect to their opinions about the group counseling for the abuse from their partners adds important considerations to agencies that assist women abused by intimate partners.
Conclusions
The negative impacts of IPV on women's mental health and well-being are well-established (Baird et al., 2021; Fedina et al., 2021; Tutty et al., 2021a), and IPV often continues after women leave abusive intimate partners (Brownridge et al., 2008; Rezey, 2020; Tutty et al., 2023). The comments from the 131 women group participants in the Healing Journey study add context to the clinical literature on what is most helpful to IPV survivors, confirming some of the major benefits of group intervention, such as support from other group members and raising questions about group process considerations such as length, readiness to attend, leadership and accessibility.
The IPV groups in the current study were offered by VAW shelters and small nonprofit community agencies. Funding initiatives such as the IPV groups can be difficult, and such small agencies are unlikely to have the resources to evaluate their programs. The women's comments from the current study primarily validate the efficacy of the groups from the perspectives of the group members, supporting their being offered.
Encouraging women to attend groups can be challenging, especially when potential group members may have mental health issues or be traumatized, as is often the case with survivors of IPV. Acknowledging that it can be scary to attend an IPV group but promoting the group's strengths by, for example, using qualitative comments from other IPV survivors, such as in the current analysis, may encourage women to allay their fears and take the risk to attend at least the first session. Attending an initial group session may reassure women about the safety, support and value in meeting other women from similar circumstances and providing the opportunity to reflect on one's own circumstances.
Footnotes
Acknowledgments
The CURA team: Dr. E. Jane Ursel and Marlene Bertrand (Manitoba Department of Family Services and Housing, MB) are the Co-Principal Investigators; Dr. Kendra L. Nixon; Dr. Christine Ateah; Dr. Janice Ristock; Dr. Lori Wilkinson; Colin Bonnycastle; Dr. Jocelyn Proulx (University of Manitoba); Dr. Johanna Leseho; Dr. Roberta Graham (Brandon University); Dr. Linda DeRiviere; Dr. Michelle Owen (University of Winnipeg); Anna Pazdzierski (Nova House, Selkirk, MB); Karen Peto (YWCA Brandon); Margaret Marin & Darlene Sutherland (Osborne House, Winnipeg); Dr. Mary R. Hampton; Dr. Bonnie Jeffery; Dr. Darlene Juschka; Dr. Wendee Kubik (University of Regina); Dr. Stephanie Martin (University of Saskatchewan); Carol Soles (Prince Albert Emergency Shelter for Women); Debra George (Family Services Regina); Dr. Karen Wood (Tamara's House, Saskatoon); Maria Hendrika (Provincial Association of Transition Houses Saskatchewan); Angela Wells (Family Support Centre, Saskatchewan); Dr. Leslie M. Tutty; Dr. H. L. Radtke; Dr. Wilfreda Thurston; Dr. Erin Gibbs Van Brunschot (University of Calgary); Dr. Caroline McDonald-Harker (University of Alberta); Dr. Ruth Grant Kalischuk (University of Lethbridge); Jan Reiner & Carolyn Goard (Alberta Council of Women's Shelters); Brenda Brochu (Peace River Regional Women's Shelter); Kristine Cassie (YWCA Lethbridge); Pat Garrett (WINGS of Providence, Edmonton).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Social Sciences and Humanities Research Council (SSHRC) Community University Research Alliance (CURA); Alberta Centre for Child, Family, & Community Research; Alberta Heritage Fund for Medical Research; the Prairieaction Foundation; and TransCanada Pipelines.