
Abstract
This mixed-methods secondary analysis examined VAW shelter use by 662 Canadian women abused by partners (50.5% Indigenous, 43.4% White, and 6.1% visible minority). Women who had never resided in shelters (n = 242) had less Severe Combined and Total IPV on the Composite Abuse Scale and fewer PTSD symptoms. More nonresidents worked full time and had higher incomes and no children. The 420 women residents mentioned strengths (70.4%) such as supportive staff and safety, and concerns (29.6%) about unsupportive staff and the shelter rules or facility. Some Indigenous women reported racist attitudes by shelter staff and child apprehensions. Practice implications are presented.
While concerns about the serious impact of intimate partner violence (IPV) are global (World Health Organization, 2021), services to assist women to respond to being physically, sexually, or emotionally abused by their intimate partners are not necessarily easily accessible. Emergency shelters or “violence against women” (VAW) shelters are often seen as society's major resource to address IPV. Although shelters are commonly used to access women to study the nature and consequences of IPV, little research has focused holistically on women's experiences in shelters. Some Canadian evaluations support the importance of VAW shelters in providing safety and assisting the transition to a life separate from an assaultive partner (Tutty, 2006, 2015). Similarly, American and European studies conclude that shelters are helpful (Allen et al., 2021; Bennett et al., 2004; Chanley et al., 2001; Grossman & Lundy, 2011; Ham-Rowbottom et al., 2005; Jonker et al., 2014; Sullivan et al., 2008; Voth Schrag et al., 2020).
Most women abused by partners do not use VAW shelters. According to Statistics Canada (Brzozowski, 2004), 11% of women abused in the past five years had used a shelter, with only 7% as residents. In a Canadian study of 309 women, only 16% had stayed in a shelter in the first six months after leaving an abusive partner (Ford-Gilboe et al., 2015). One US study of 113 women (Galano et al., 2013) concluded that those most likely to use shelters had lower income, were racialized (more African American women), and had PTSD but not depression. A 30-year-old comment that still holds true is that shelters provide “options for women who have few options” (Weisz et al., 1994). Given shelters’ centrality in the efforts to address IPV, additional research on women's experiences while residing there is recommended and is the focus of the current study.
VAW Shelter Organization and Services
According to a study of 112 Canadian shelter directors and frontline staff (Harris et al., 2014), the four most important shelter services are: (1) safety in times of crisis; 2) material support in shelter; (3) information and referral; and (4) education about IPV and counseling. In Canada in 2006, closest to the data collection in the current study, 553 shelters provided residential services to women and children fleeing abusive situations, according to the 2005/2006 Transition Home Survey (THS) (Taylor-Butts, 2007). While most are clustered in urban areas, in 2010, 39 shelters were on rural Indigenous reserves; however, 64% of all shelters reportedly offer culturally sensitive programs for Indigenous women and their children (Burczycka & Cotter, 2011). Many VAW shelters provide additional services such as crisis-phone-lines, outreach for women who are not shelter residents, and follow-up programs for former residents who have moved into the community (Burczycka & Cotter, 2011; Tutty, 1996; Wathen et al., 2015).
Shelters tend to be complex organizations and coping with the rules and structures needed to function within a communal setting can be challenging for both residents (Dewey & St. Germain, 2014; Glenn & Goodman, 2015; Tutty et al., 1999; Tutty, 2015; Voth Schrag et al., 2020; Wood et al., 2020) and staff (Burnett et al., 2016). Shelter staff must face the complex nature of the residents’ needs, including of those with mental health concerns (Burnett et al., 2016; Helfrich et al., 2008; Hughes et al., 2011; Mantler et al., 2020; Tutty, 1998) and/or substance use (Hovey et al., 2020; Schumacher & Holt, 2012). Support services are often lacking; structural issues such as poverty (Burnett et al., 2016; Goodman et al., 2009) and discrimination, and the short timeframe within which to assist women are challenging. VAW shelter workers have also been designated as mandated reporters of potential child abuse, which, can be seen as a betrayal of their role of supporting all women (Burnett et al., 2015; Fauci & Goodman, 2020; Goodman et al., 2020; Pajak et al., 2014; Thomas et al., 2015). Working with such traumatized and vulnerable populations, shelter staff may be at risk of vicarious traumatization or secondary traumatic stress (Bishop & Schmidt, 2011; Frey et al., 2017) caused by repeatedly hearing traumatic stories from clients in one's professional capacity (McCann & Pearlman, 1990).
In early research (Aguirre, 1985; Cannon & Sparks, 1989), women whose partners abused them were described as returning to those partners an average of about eight times and as returning to the VAW shelters repeatedly. In a recent Canadian THS (Beattie & Hutchins, 2015), one-quarter of the residents had stayed in the same shelter before. Whether or not the number of shelter stays is a proper indicator of success in outcomes remains of interest. Given the structural issues identified, indicators of success may vary. Although primarily positive about their shelter experiences, some residents raise concerns about the behaviors of a few other residents, some staff not being helpful, feeling under surveillance by staff, and not receiving sufficient help to access housing or other basic needs (Dewey & St. Germain, 2014; Tutty, 2006, 2017). Glenn and Goodman (2015) posit that PSTD may affect a resident's reading of other people's intentions and behaviors. As one would expect, length of stay is related to women's needs (Sullivan & Virden, 2017b); however, in Canada, length of stay is typically mandated by the provincial governments and is usually limited to three to four weeks, which may account for some readmissions.
VAW shelters for women offer many services, including providing information about IPV and crisis counseling (referred to as advocacy in the United States), as well as helping women access housing, jobs, or schooling for their children (Hughes, 2020). Nevertheless, previous studies have shown that shelter residents refer to crisis counseling from shelter staff as vital to assisting them (Sullivan & Virden, 2017a; Sullivan & Virden, 2017b; Tutty, 2017). Shelter staff often make referrals to external resources, such as legal information (Wright & Bertrand, 2017) and financial support (Harris et al., 2014). Housing referrals have become another essential role in VAW shelters, as abused women may be at risk of homelessness (Harris et al., 2014; Tutty et al., 2013).
Rationale for the Current Study
Considering the structural complications and limitations of VAW shelters and given their central place in society's response to IPV, it is important to understand how women perceive shelter services, which is the focus of this research. With unique access to a large study of Canadian women abused by intimate partners from three western provinces, the goal of the current secondary data analysis was to examine the VAW shelter experiences of 662 women in terms of their demographic locations, IPV experiences, and mental health concerns. Further, there is a paucity of studies on women who do not seek VAW shelters: about one-third of the women in the current study had not resided in VAW shelters.
Given that over half of the women in the current study were Indigenous, this was an important opportunity to learn about their VAW shelter use. While constituting only 4% of Canadian women, 10% of Indigenous women (First Nations, Métis, and Inuit) report IPV compared to 3% of non-Indigenous women (Statistics Canada, 2016). The Truth and Reconciliation Commission of Canada (2015) highlighted the legacy of colonization, residential schools, and the “Sixties Scoop” (child welfare apprehension of Indigenous children) that contributes to violence, including IPV, among Indigenous peoples. These structural issues also include poverty, lack of services, the loss of traditional lifestyles, and parental role models (Brownridge, 2008; Burnett et al., 2015). Moreover, a higher proportion of Canadian shelter residents are Indigenous compared to not being Indigenous: According to Maxwell (2022), in a recent one-day snapshot of Canadian shelters, “60% of women and 65% of accompanying children were identified as Indigenous persons” (p. 3). However, beyond this we could find little research specific to Indigenous women's perceptions of their shelters stays, exceptions being Ogden and Tutty (2024). Racism on the part of some shelter staff was raised by Indigenous women in several studies (Baskin, 2012; Tutty, 2015).
Method
This exploratory secondary analysis used a mixed-methods approach (Sandelowski, 2000), including both quantitative and qualitative components. The data were from the “The Healing Journey,” a longitudinal, Canadian study with a convenience sample of 662 women who had experienced IPV in the three prairie provinces of Alberta, Saskatchewan, and Manitoba. The original study aimed to assess characteristics of women abused by intimate partners, including mental health and general wellbeing (Tutty et al., 2021a), mothering in the context of IPV (Ateah et al., 2019; Nixon et al., 2017) and following women over 2.5 years (Tutty et al., 2021b). Both academics and community agency research team members designed the research and recruited participants. Data were collected in seven waves between 2005 and 2009, with one wave specific to an economic analysis (DeRiviere, 2014).
Study Participants
The research protocols were approved by the Ethical Review Boards of the six associated universities (Universities of Calgary, Manitoba, Regina, Brandon, Lethbridge, and Winnipeg). Each province conducted an environmental scan of agencies (i.e., women's shelters and counseling agencies) to cover urban, rural, and northern sites from which to recruit. The criteria for inclusion were minimum 18 years of age; the most recent incident of IPV no sooner than three months and no longer than five years prior; commitment to stay in the study for the full four years; and no debilitating mental health issues. Honoraria (CAN$50) were given to participants at each wave.
Research Measures
The current study used quantitative methodology, including standardized measures, to assess potential differences between women who did and did not access counseling services. Data in the original study were collected with respect to four major areas over 2.5 years: demographics and history of abuse; general functioning and service utilization; health status; and mothering experiences. The surveys included standardized measures as well as open- and closed-ended questions developed specifically for the study, all administered verbally by trained research assistants. The current mixed-methods secondary analysis used data from the first two waves of the study: core demographics, including the severity of IPV of the total sample and women's comments with respect to the shelters in which they resided were gathered in Wave 1. Mental health measures were collected in Wave 2.
Intimate Partner Violence
The nature of the IPV was assessed by the Composite Abuse Scale (CAS) (Hegarty et al., 2005). This screening measure consists of 30 items rated for frequency in the past 12 months on a six-point scale from never to daily, with a possible total of 150. The four subscales are Severe Combined Abuse (8 items; range of scores 0–40; suggested cutoff of 1), Physical Abuse (7 items; range of scores 0–35; cutoff of 1), Emotional Abuse (11 items; range of scores 0–55; cutoff of 3), and Harassment (4 items; range of scores 0–20; cutoff of 2). The suggested clinical cutoff for the Total CAS score is 3 or 7 to minimize false positives. The scale has demonstrated convergent and discriminant validity (Hegarty et al., 2005). Cronbach's alpha for the CAS in the current study is .93.
Child Abuse and Disability
Child abuse history was collected via structured questions (yes/no answers): “Were you abused as a child or adolescent?” (a) physical, (b) sexual, (c) emotional/psychological, and (d) witnessing abuse among family members (consistent with Elias et al., 2012). We asked the women to self-report physical and mental health conditions (whether or not diagnosed by medical personnel) and to assess disability, we asked whether these conditions affected their employability or the number and types of daily activities.
Mental Health and Well-Being
The Symptom Checklist Short Form (SCL-10) (Nguyen et al., 1983) is a screening tool to assess global mental health functioning and psychological distress in the previous week. Items (e.g., “In the past week, how much were you distressed by feeling lonely?”) are endorsed with a 0–4 Likert scale (0 = “not at all;” 4 = “extremely”). Higher scores indicate more distress. Published clinical cutoffs for the 10-item version were not found. However, as clinical cutoff scores are one standard deviation above the mean (Jacobson, et al. 1984), we used Müller's data (2010) reporting a mean score of 7.8 (SD of 6.3), resulting in a clinical cutoff score of 14.2. Cronbach's alpha in the current study is .89.
The Centre for Epidemiological Studies–Depression-10 (CES-D-10) is a shorter form of CES-D-20 (Radloff, 1977) used to document depression symptoms in the previous week (Andresen et al., 1994). Ten items (e.g., “In the past week I was bothered by things that usually don't bother me?”) are rated on a 0–3 Likert scale, with 0 as “rarely or none of the time (less than 1 day)” and 3 as “all of the time (5–7 days).” Internal consistency and test-retest reliability are good (Björgvinsson et al., 2013). Cronbach's alpha in the current study is .84. Björgvinsson et al. (2013) suggest that a cut-off of 15 has the best “sensitivity” and “specificity.”
The PTSD Checklist (PCL) (Blanchard et al., 1996) is a 17-item self-report questionnaire that measures PTSD symptoms in the past month. Items (e.g., “In the past month how much have you been bothered by repeated, disturbing memories, thoughts or images of abuse or violence?”) are endorsed with a 0–4 Likert scale with 0 meaning “not at all” and 4 meaning “extremely.” Blanchard et al. (1996) recommend a clinical cutoff of 44. The scale has good psychometric properties (Cronbach's alpha = .94; Blanchard et al., 1996). Cronbach's alpha in the current study is .92.
The original 25-item Quality of Life Questionnaire (Andrews & Withey, 1976) was shortened by Sullivan and Bybee (1999) to nine items (QoL-9) measuring satisfaction with her overall quality of life (e.g., “How do you feel about life as a whole”) and satisfaction with particular areas (e.g., “How do you feel about yourself; your personal safety; the amount of fun and enjoyment you have”). Items are rated on a 7-point scale (1 = extremely pleased, 7 = terrible). Higher scale scores indicate poorer QoL. Cronbach's alpha in the current study is .84.
Quantitative Data Analysis
The demographic characteristics of the women and their scores on the CAS are presented descriptively. Demographic characteristics of the women are compared statistically using Pearson's chi-square analysis based on whether they had resided in a VAW shelter, with effect sizes calculated with Phi or Cramer's V. Standardized residuals were calculated to identify the category differences responsible for the statistically significant chi-square analysis (Field, 2009). Effect sizes were interpreted using Rea and Parker's (1992) suggested benchmarks of under .10 as a “negligible” association; between .10 and under .20 as a “weak” association; between .20 and under .40 as a “moderate” association, and between .40 and under .60 as a relatively “strong” association (p. 203). The mean scores on the standardized measure were compared with independent t-test based on whether they had resided in a VAW shelter. Cohen's d (Cohen, 1988) is used to interpret statistically significant t-tests with a d between 0.2 and 0.3 considered a “small” effect size, 0.5 represents a “medium” effect size and 0.8 a “large” effect size.
Research Procedures: Qualitative Component
Qualitatively, the women were asked whether they had ever resided in a shelter and if so, how helpful was it? They were given an open-ended opportunity to comment, which is the focus of the current analysis. The interviewers read the questions and wrote down the women's responses.
We used descriptive qualitative health research to analyze these comments about their shelter, a method that is particularly appropriate for mixed-methods research (Neergaard et al., 2009) and for “assessing, developing and refining interventions with vulnerable populations” (Sullivan-Bolyai et al., 2005, p. 127). The descriptive analysis followed established inductive content analysis processes (the meaning emerges from the quotes) (Elo & Kyngäs, 2008; Sandelowski, 2000). We identified the major themes and subthemes (Graneheim & Lundman, 2004; Neergaard et al., 2009). Given the large number of comments available for analysis, we deemed it appropriate to examine the positive and negative themes by calculating the proportions of each, as suggested by (Nassaji, 2015) who writes, “data collected qualitatively can also be analyzed quantitatively. This happens when the researcher first examines the qualitative data thoroughly to find the relevant themes and ideas and then converts them into numerical data for further comparison and evaluation” (p. 130).
Results
Demographics of the Study Participants
The 662 women respondents were an average age of 36.4 years, while their partner/ex-partners were an average 38.7 years (see Table 1). The women's racial backgrounds were 50.5% Indigenous, 43.4% White, and 6.1% visible minority, with the partner/ex-partners being White (47.3%), Indigenous (44.9%), and 7.8% visible minority. Most women (90.8%) had children.
Comparison of Women's Demographics by VAW Shelter Stay Ever or Not (N = 662).
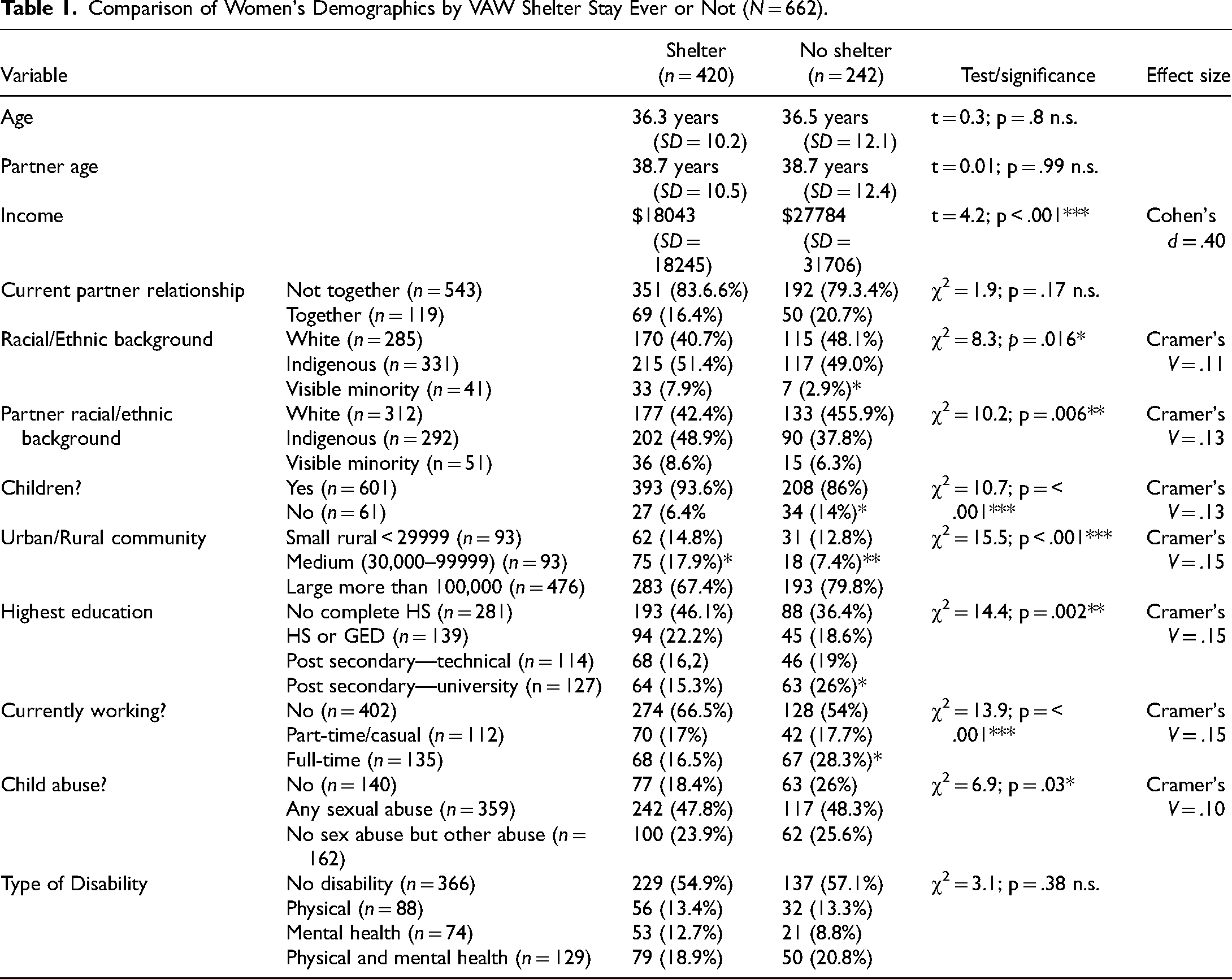
The women primarily lived in large urban centers (71.9%) with populations of more than 100,000, with 14% in smaller urban centers (30,000–99999) and 14% in rural centers (less than 29,000). With respect to their highest level of education, 42.5% of the women had not completed high school and 21% had completed high school, while 36.4% had some post-secondary education, either in technical institutes (17.2%) or universities (19.2%). Their average total income in the past year was $21,694; about half of the women's incomes fall below the poverty-line for that time in the three Canadian provinces (DeRiviere, 2014). This low yearly income is partly explained by the fact that the majority of the women (61.9%) were not currently working, 17.3% worked casually or part-time, and 20.8% worked full-time.
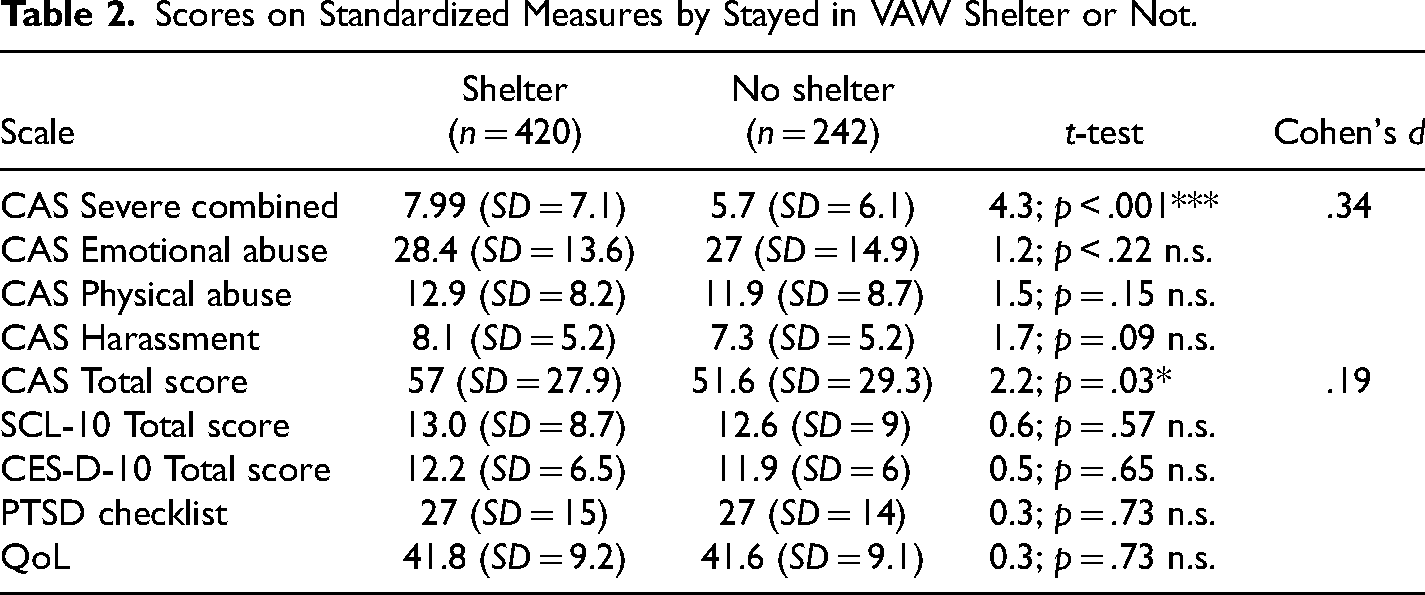
With respect to a history of child maltreatment, 21.2% reported none, 24.5% reported child abuse not including child sexual abuse, and over half (54.3%) reported having been sexually abused as children. Almost half of the women (291 of 658 or 44.2%) reported that they had at least one disability. Of these, about one-third (30.6%) had a physical disability only, one-quarter had a mental health disability only (25.2%), and 44.3% self-reported having both a physical and a mental health disability. Average scores on the CAS subscales were well above the suggested clinical cutoff scores (see Table 2). None of the average scores on measures of mental health functioning was in the clinical range. Average scores on the Quality of Life Questionnaire were 41.7 (no clinical cutoff).
Scores on Standardized Measures by Stayed in VAW Shelter or Not.
Differences Based on VAW Shelter Stay Versus None
Several demographic characteristics (see Table 1) differentiated women who had resided in VAW shelters (n = 420 or 63.4%) from those who had not (n = 242 or 36.6%). Those who had sought shelter had significantly less annual income and more of their partners were of Indigenous origins. With regard to the women's scores on the standardized measures (see Table 2), women who did not seek shelter reported less severe violence on the Severe Combined Abuse and the CAS Total Abuse subscales, both indicating less IPV, and they reported fewer PTSD symptoms.
Perceptions of the VAW shelters
The 420 women shelter residents rated the first shelter in which they stayed as quite a bit/very helpful (65.3%), somewhat helpful (17.5%), and not at all/a bit helpful (18.2%). About one-quarter (26.1%) had stayed in only one shelter, one-third (33.4%) had stayed at two shelters, one-fifth (19.4%) at three shelters, and 13.3% at four shelters, with only a minority having stayed at five or more VAW shelters (7.8%). Comments with respect to the shelters are divided by those that are positive versus those that are negative. The categories in each are detailed in the following sections with supporting direct quotes.
Positive Shelter Features
The 398 women who commented on their shelter residency mentioned 610 positive features including counseling and support from shelter staff, safety, help with housing, access to basic needs in the shelter, referrals to resources outside of shelter, in-shelter groups, other women residents, childcare, shelter rules, and follow-up (see Table 3).
Positive Comments about Shelter Featuresa.
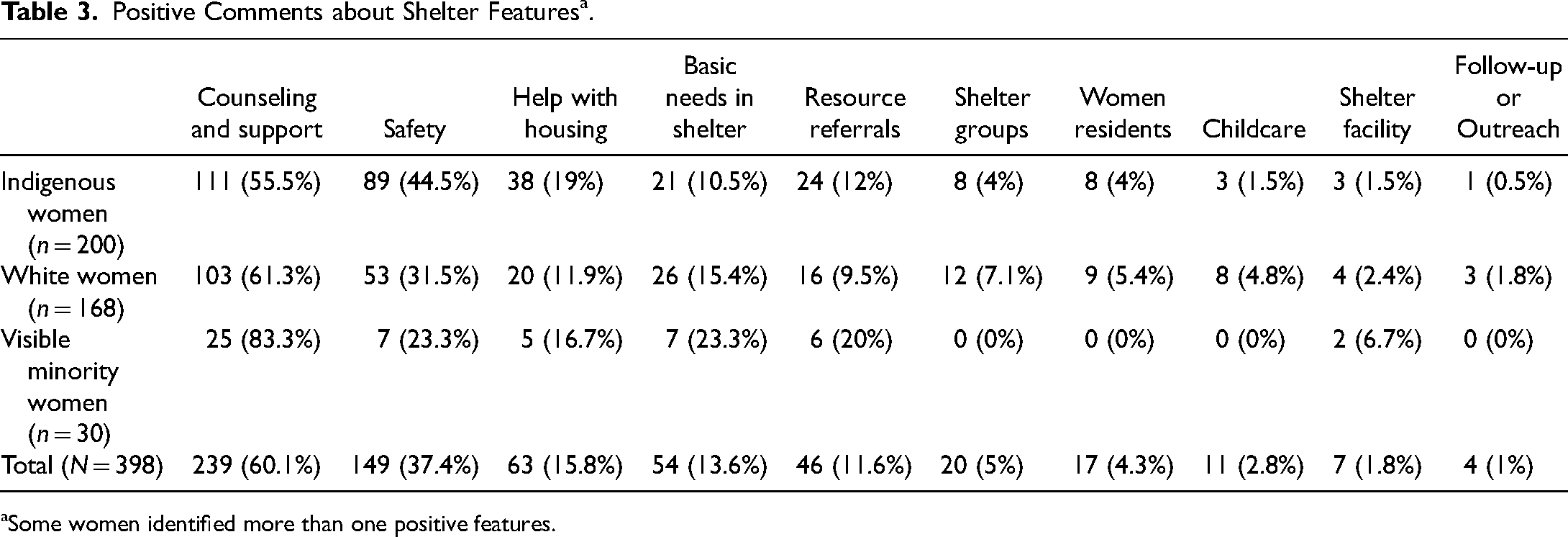
Some women identified more than one positive features.
The most mentioned positive feature of the VAW shelters was the counseling and support from shelter staff, noted by 239 women (60.1%). Examples included “They were there to help me; to not push me. They give you pros and cons; they help you develop your own safety plan. What I especially like is that they don’t try to make up your mind for you,” “They were kind and nice. I felt embarrassed to go into a shelter, but they made it seem okay to be there,” and “I was deprogrammed. I was seriously brainwashed prior to going there, so they helped me to work through that. They taught me how to protect myself and gain self-worth. They were also very protective of me.” The safety of the shelter was the second most often mentioned positive feature (n = 149; 37.4%), exemplified by the following, “If it weren’t for them, I wouldn’t be alive,” “It was helpful because I ran out of places to hide in [name of city] and he wouldn’t know to look for me there,” and “Gave me a safe bed to sleep in. Safe place to play for my kids.”
Smaller proportions of the women (n = 63; 15.8%) mentioned that assistance in finding housing and accessing basic needs was appreciated, e.g., “Showed me how to get into low-income housing. Took me to see some houses and gave me info on getting furniture, food, vouchers for clothes” and “Helped me find a place to live and set me up with furniture.” A similar proportion (n = 54; 13.6%) mentioned the importance of the shelter providing them with basic needs during their residence there, e.g., “Gave me a bed to sleep in. Gave me food, transportation” and “Children's needs clothing/toys/diapers/formula, a place to stay, eat. Access to phone. Privacy.” Referral to outside resources beyond housing were also appreciated (n = 46; 11.6%). Comments included, “I was referred to Social Services and that was helpful,” “Helpful in setting me up with legal aid,” and “They advocated for me with other agencies.”
The final five categories were identified by only small proportions of the women (5% or less) but deserve mention. The in-house shelter groups were identified as helpful, as the following comments portray. “Took me to support domestic violence meetings, I wasn’t alone!” “They showed me through groups that hitting is not right and living in fear is not right. They showed me and gave me strength to say I am not going to do this anymore,” and “Counselors did a once-a-week group that was very helpful.” The other women shelter residents were described as helpful, as in the following: “I felt a community sense with the other women in the same situation,” “They helped because I talked to other women with similar experiences,” and “It was nice to meet people who had the courage to leave.”
The shelter facility and shelter rules were mentioned by some women: “The security system was great. They had all kinds of videos about abuse, they had books. I had my own private room and bath. They had clothing, toiletries, everything (food). You had chores, you helped each other to cook. Mothers and children were there, and everyone helped each other. It was phenomenal, you felt like it was home. I didn’t want to leave” and “They had a lot of rules but I’d rather live by them than the rules my partner made me live by.”
Childcare was mentioned as a positive by some women, although always in short descriptions such as “childcare good”. The final positive category was comments about follow-up or outreach programs. “The best thing is the follow-up worker comes to our place instead of having to travel.”
Negative Shelter Features
The 398 women who commented on their shelter stay mentioned 256 issues that were with respect to some staff not being available or supportive, shelter rules/facility, need for in-house programs, problems with other residents, need for follow-up, no childcare, need for culturally relevant services or racism, and children being apprehended by child protective services (see Table 4). In contrast to the most positive feature being the counseling and support from the shelter staff, the most mentioned negative feature was with respect to shelter staff not being available or supportive (n = 96 or 24.2%). Interestingly, this was noted by a higher proportion (35.5%) of our Indigenous participants. Comments from all respondents included concerns about both the quality of the counseling and that staff were not available or did not approach the women to offer assistance: “Counselors were not very good. They should have more sympathy and more compassion. One was very mean and would take out her moods on the women,” “It was a cold, isolated feeling attached to it. I felt so alone, and the staff left you alone. I needed someone to talk to, trauma counseling. I expected it. My expectations were not met,” “The workers were in the office all the time, and no one was supervising the common areas. I had to get out of there,” and “Women who have gone through trauma and abuse need to be able to approach someone. Or someone to approach them. Needs to be more one-on-one—advocating for the victim to begin talking and begin to learn to socialize again. There wasn’t enough of that in the shelters.”
Negative Comments about Shelter Featuresa
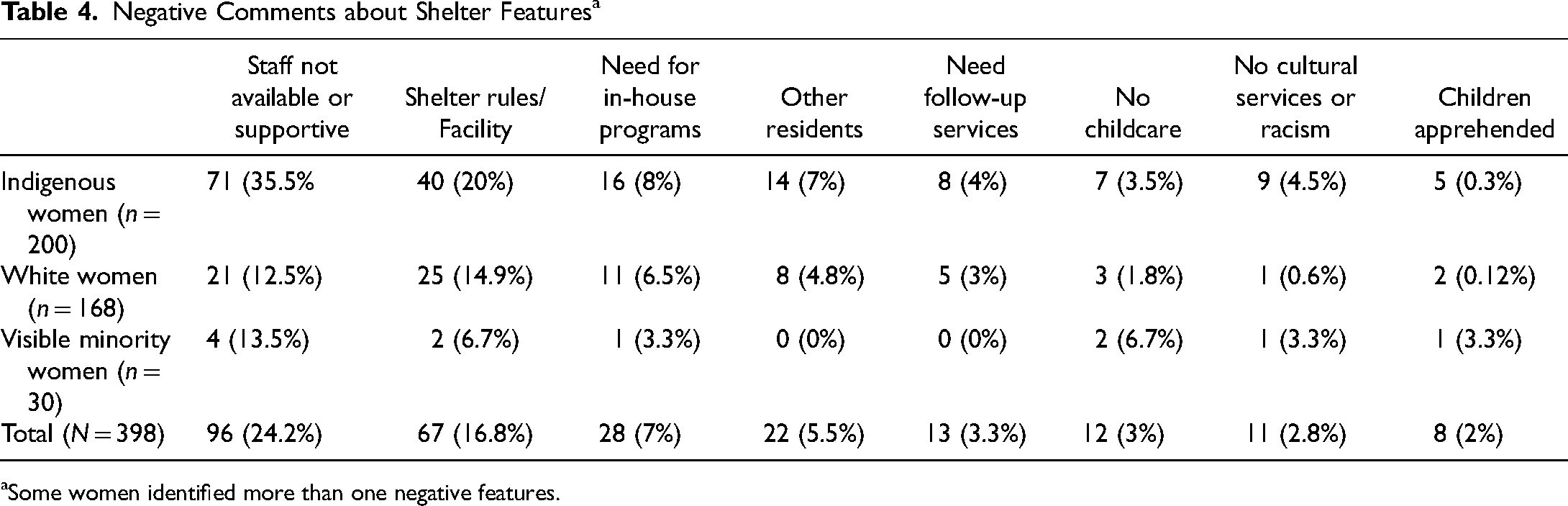
Some women identified more than one negative features.
The shelter rules or the facility was the second most documented concern (n = 67), raising issues including the chore schedule, the cleanliness of the facility, and the short length of stay. “You are required to leave after three weeks. I had been severely beaten yet the staff expected me to have everything in place and I couldn’t. Staff are needed to assist women with weighing out the pros and cons,” “I found out that I couldn’t access a shelter once a male child turns 7 years old. You are only allowed to stay at shelter for ten days and this is worrisome because it's not enough time,” “It was supposed to be my safe haven. The kids sometimes annoy me. Sharing bathrooms really bothers me,” “They didn’t like my kids touching everything. It was a place for women and children, yet they couldn’t touch anything. I just wanted to leave,” and “It was dirty. There was a lice breakout. We had a tiny room and a bed/cot we unfolded the cot and there was a big clump of hair.” A more comprehensive comment is as follows: Inside the shelter was dysfunctional—the shelter had bed bugs, and that wasn’t being addressed. Sleep was huge issue. Policy towards sleeping—quiet times, not honored. I couldn’t sleep. Instead of following policy and asking other residents to tone it down. I felt I couldn’t complain because if I needed shelter again, they might turn me away.
A smaller number of comments (n = 28) were about the need for more in-house programs. “No support groups meetings or information sessions or guest speakers regarding spousal abuse. It was just a place to stay and eat,” “The shelters seem to be very busy, there are no organized activities like women's groups. One has to look for her own,” “There was not enough counseling. The concentration was to get you out. Trying to push you out,” and “Could have used healing circles or one-on-one counseling”.
Twenty-two comments were concerns about other shelter residents, such as “It was very good, but lot of drugs were going on in there,” “Belongings were stolen and damaged”, “Other women were very intimidating—the women who were staying there,” “A client there was a problem, drinking, upset so I went back,”
The final four areas of concern accounted for less than 4% of the negative comments each but, nonetheless, represent important issues. A need for follow-up services or help with accessing housing was mentioned in 13 comments: “I had a hard time getting a referral for housing from them. I had to leave message after message at their office. They were not much help with connecting me with other services I needed at the time,” “No follow-ups/no support after leaving,” and “There was not enough guidance for me or follow up. I expected some help in finding a direction in life. I felt lost after I left there, thinking, ‘What was that experience, what did I learn?’”
No childcare in the VAW shelter was considered problematic in 12 comments. “Childcare was inadequate. I had to ask other women there to take care of my children so I could go see my lawyer,” “Not helpful—no childcare in building, no time for just me. I was tired the whole time. If I had to go out, I had to take all four children,” “There was no childcare. How do you look for housing with four children in tow?” and “Pre-school care almost nonexistent—only had one preschooler but would have liked support because I really felt I couldn’t cope.”
Eleven women commented about the lack of cultural interventions or explicit racism. All but two of these comments were from Indigenous women. Four comments were about the need for Indigenous culturally sensitive practices: “I had to explain about going to a ‘sweat,’ as it helped me look within and learn things about myself. It would be a good program to have at the shelter,” “They need to be more helpful with spiritual practices,” and “[Shelter] didn’t have that cultural component to it, no smudging. I think the staff needs cultural awareness training. Just because we don’t look people in the eye or face when we listen, doesn’t mean we are not listening. This is not directed only to the Aboriginal people. A lot of people do this.” Another woman noted, “shelters need to be culture sensitive in regard to food, etc.”
The remaining seven comments were about racist attitudes from shelter staff: “Some counselors made me feel uncomfortable. I think it was racially based. Some rushed me out too fast. Undermined me, like I didn’t know what I wanted,” “I was treated differently. Aboriginal women were asked to leave, sent to other facilities. They said we did not fit criteria yet a non-Aboriginal was allowed to stay even though she had the same problems,” “The White professionalism gets in the way of helping Aboriginal women. They make us feel inferior,” “Racist, discriminating against Aboriginals, unqualified workers, unfamiliar resources,” and “My counseling was tweaked with racism; the counselor was Filipino, and it did not make me feel comfortable.” A woman with a visible minority identity commented, “Racism was a factor occasionally. This made me feel worse—that it might be better to return to my abusive partner.”
Eight women described the possible or actual apprehension of children by child protective services. For two women, this was prior to coming to the shelter: “Forced to go to shelter by Child Protective Services. They took my children” and “Social services told me to leave partner to get my son back. Shelter didn’t want me because I didn’t have my son.” A third woman of Indigenous identity feared that her children could be apprehended in the shelter: “Aboriginal women had their children apprehended; three or four women here lost their children, so there was a great fear in me for my children.”
For the other five women, their children were apprehended while they were in shelter, commenting, for example: “Native women get their children apprehended because they don’t understand how we parent, or why we can’t buy expensive Pampers and our children get a rash. There are a lot of things that we Aboriginals complained about; things that are not right.” They said I had to go to the doctor because my baby had diarrhea and, if I didn’t, they’d apprehend him. So, I cooperated. The doctor told her that he just had a diaper rash. Then shelter staff said, ‘I’m going to call my supervisor to see if I should apprehend him.’ And they did. I called my band. The next day they made some calls and got my child back. The doctor was shocked that they took him. “I was using alcohol and prescription drugs at the time. My son was apprehended while in shelter,” and “Made me mad because they took my kids.”
Discussion
The current study is unique in that it provides a broad overview of women's perceptions of VAW shelters for IPV. Those who did not access shelters were less likely to be from visible minority backgrounds, less likely to live in medium-sized communities, reported more annual income, more had postsecondary (university) education, more were working full-time, and more had not likely to have experienced child abuse. More of their partners were White. Women who did not seek shelter had experienced less violent behaviors from partners, as identified on the Severe Combined Abuse subscale and the CAS Emotional Abuse subscale. These results are similar to those of other studies showing that structural inequalities largely account for shelter use (Burnett et al., 2016; Goodman et al., 2009).
Some women stayed in multiple shelters, perhaps identifying the lack of some services such as counseling in one, to what they were offered in another, or the impact of enforced limits on length of stay. Almost three-fifths (59.5%) of the women had stayed in one or two VAW shelters, different from the stereotype of abused women returning to shelters multiple times (Aguirre, 1985; Cannon & Spark, 1989). The women varied in complexity of their situations and made difficult decisions about when and how to leave abusive partners, facing structural barriers they could not individually overcome.
Similar to previous research on women's experiences in VAW shelters (Dewey & St. Germain, 2014; Goodman et al., 2009; Tutty, 2006, 2017), the women had mixed reviews about their shelter residence. Overall, however, the positive comments (610 of 866 or 70.4%) outweighed the negative ones (256 or 29.6%). As mentioned, 420 shelter residents rated them as quite a bit/very helpful (65.3%), somewhat helpful (17.5%), and not at all/a bit helpful (18.2%). This contrasts with a separate analysis of 98 women's impressions of counseling from shelter staff (Tutty, 2023), in which 86 (87%) rated the shelter counseling/groups as quite a bit/very helpful, five (5.1%) rated these as somewhat helpful, and seven (7.1%) rated these as not at all/a bit helpful. That satisfaction with the shelters holistically was more negative could be seen as representing the complexity of VAW shelters, in which women have multiple experiences, including counseling and advocacy but experienced the challenges of communal living and responding to facility rules and expectations.
The top positive categories were identical to the four services that 112 Canadian shelter directors and frontline staff mentioned as central in the Harris et al.(2014) study that included safety, the provision of basic needs while in shelter, help with housing and referral to community resources (reported separately in this analysis), and counseling and education. These four issues stood alone in the positive category (36.4%, 13.6%, 15.8%, 11.6% and 60% respectively).
Most of the women's concerns have also been identified in previous studies, including some staff being unresponsive and the behavior of a few other shelter residents (Dewey & St. Germain, 2014; Goodman et al., 2009; Tutty, 1998, 2017). In examining the positives and negatives, significant numbers were with respect to the same issue. The counselors and support were mentioned as positive by 60.1% but as of concern by 24%; help with housing by 15.8% contrasted to a need for assistance with housing by 7%; other women residents as positive by 4.3% but as negative by 5.5%; childcare was 2.8% positive and 3% negative; and follow-up programs were seen as positive by 4% and as needed by 3%. While not directly comparable, in-house shelter groups were seen as positive in 5% of comments, while the need for more in-shelter programs (including groups) was raised in 7% of comments. In some ways, these areas constitute a wish list of needed services from residents.
Racism and the threat of or actual removal of children by provincial child protective services were the only stand-alone negatives. Although a relatively rare occurrence, child apprehensions were noted more by Indigenous women (5 of 8), consistent with other shelter research (Burnett et al., 2015; Fauci & Goodman, 2020; Goodman et al., 2020; Pajak et al., 2014; Thomas et al., 2015) and the high proportion of Indigenous children taken into care when IPV is an issue in Canada (Brownridge et al., 2017; Robertson et al., 2021; Tutty & Nixon, 2020).
Across all categories, Indigenous women made the most critical comments about their shelter stays, although they also had the highest proportion of positive comments about safety and referrals for housing. Indigenous Peoples in the prairie provinces constitute 39.2% of the First Nations population and 50.4% of the Métis population in Canada (Statistics Canada, 2011). Notably, as far as we could tell, none of the shelters commented upon in the current study were specific to Indigenous women (Burczycka & Cotter, 2011) and, as such, all would be considered “mainstream.” While comprising a relatively small percentage of the total number of negative concerns, the explicit mentions of racism from staff and the implied racisim in the negative comments about shelter staff not being responsive are critical to note and have been documented in previous research (Baskin, 2012; Tutty, 2015).
Implications for VAW Shelter Organizations
Overall, the positive comments outweighed the negative (70.4% versus 29.6%), and the categories fit exactly with what Canadian shelter directors and staff had previously identified that VAW shelters provide (safety; basic needs; referral to housing; community reports; and counseling/education) (Harris et al., 2014). This validates the importance of the services to the women in our study who were seeking support after IPV.
Nevertheless, the women also identified concerns that merit attention. Burnett et al. (2016) nicely sum up the challenges and intricacies of shelter directors and staff in adequately meeting the complex needs of their women residents, especially when some women have mental health issues, such as PTSD or misuse substances. Although concerns such as the lack of responsiveness of some shelter staff have been previously documented (Dewey & St. Germain, 2014; Tutty, 2006, 2015, 2017), the overtly racist attitudes mentioned by a small number of respondents have not. That Indigenous women reported the highest proportion of negative comments about the staff, mentioning, for example, a lack of empathy or a refusal to connect suggests that this may also constitute racism. The negative staff behaviors described above could also be interpreted as subtly racist, especially since, in this category, 74% of the comments were from Indigenous women. Two issues emerge from this: the possibility of staff burnout or vicarious trauma and the need for cultural safety training for staff.
Vicarious trauma (or secondary traumatic stress) can be an issue for all shelter staff, but even more so when staff were also IPV survivors, a not-uncommon circumstance (Frey et al., 2017; Wilson & Goodman, 2021). When affected by vicarious trauma, professionals may avoid clients by not being sympathetic, appearing to simply go through the motions or physically removing themselves, similar to what the women in our study described. Trippany et al. (2004) suggest that preventing (or ameliorating) vicarious trauma can be achieved through agencies taking responsibility, providing staff with education about vicarious trauma, peer supervision, and supporting personal coping mechanisms, such as promoting a balance of work, play, and rest.
Regarding cultural sensitivity, rather than offering “cultural competency,” newer articles suggest programs promoting “cultural safety” (Curtis et al., 2019). These seek to improve care through becoming aware of differences, decolonization, power relationships, using reflective practice, and allowing the client to decide whether a clinical encounter is safe—ideas that are especially applicable to working with clients of Indigenous origins but promote a more client-specific approach generally. A Canadian Indigenous cultural safety program described by Browne et al. (2021) exemplifies this strategy and provides a model for professionals.
Study Limitations and Strengths
This secondary analysis was of a study conducted almost two decades ago; nevertheless, it raises questions about how well VAW shelters provide services to their residents that merit attention. With secondary analyses, one is limited by the nature of the original study, which, in this case, relied on a convenience sample of women from VAW shelters or counseling agencies. As such, the results are not generalizable to other abused women in Canada's prairie provinces.
The women were asked only a brief question about what they thought of the shelters in which they resided. While some comments were in-depth, the women were not asked about the positive and/or negatives in a comprehensive manner. As such, the resulting comments must be regarded as whatever was top of mind. Future in-depth enquiries about women's experiences in VAW shelters are needed to evaluate their experiences and satisfaction. The themes that emerged from the current qualitative study could be used to organize possible categories of advantages and disadvantages of shelter stays.
A strength of the current study is that the women constitute a large sample of IPV survivors from the Canadian prairies, with more than half of Indigenous background, a group whose well-being is particularly important in Canada but who may not be included in IPV research. This is especially important given their high risk of serious IPV (Statistics Canada, 2016) and higher use of VAW shelters (Maxwell, 2022). Further, Indigenous women are likely to have been negatively impacted by the consequences of colonialism (Brownridge, 2008; Burnett et al., 2015; Ogden & Tutty, 2023; The Truth and Reconciliation Commission of Canada 2015). The Indigenous women in our study identified especially concerning behaviors on the part of some shelter staff. In general, the women's candor with respect to their opinions about the shelters in which they resided adds important feedback for VAW shelters to consider.
Conclusion
Although women's impressions of VAW shelters have previously been studied (Allen et al., 2021; Bennett et al., 2004; Chanley et al., 2001; Grossman & Lundy, 2011; Ham-Rowbottom et al., 2005; Sullivan & Virden, 2017a; Sullivan & Virden, 2017b; Tutty, 2015; Voth Schrag et al., 2020), the current research is unique in having a large sample with a substantial Indigenous subpopulation, a group whose views about VAW shelters have seldom been documented. While the comments were sometimes brief, most conveyed clear opinions about both positive and negative features of their shelter stays. The inclusion of multiple jurisdictions further strengthens the finding.
To conclude, the women's impressions and views of the VAW shelters in which they resided provided confirmation of shelter strengths and several concerns that, we would argue, have not previously been documented. The generally positive nature of most of the comments provides important feedback to clinicians and points to the need for primary and secondary prevention of IPV, addressing structural factors that shelters alone cannot change. The negative comments and suggestions merit attention and careful consideration for shelter operation.
Footnotes
Acknowledgments
The CURA team: Dr. E. Jane Ursel and Marlene Bertrand (Manitoba Department of Family Services and Housing, MB) are the Co-principal Investigators; Dr. Kendra L. Nixon; Dr. Christine Ateah; Dr. Janice Ristock; Dr. Lori Wilkinson; Colin Bonnycastle; and Dr. Jocelyn Proulx (University of Manitoba); Dr. Johanna Leseho and Dr. Roberta Graham (Brandon University); Dr. Linda DeRiviere and Dr. Michelle Owen (University of Winnipeg); Anna Pazdzierski (Nova House, Selkirk, MB); Karen Peto (YWCA Brandon); Margaret Marin and Darlene Sutherland (Osborne House, Winnipeg); Dr. Mary R. Hampton; Dr. Bonnie Jeffery; Dr. Darlene Juschka; and Dr. Wendee Kubik (University of Regina); Dr. Stephanie Martin (University of Saskatchewan); Carol Soles (Prince Albert Emergency Shelter for Women); Debra George (Family Services Regina); Dr. Karen Wood (Tamara's House, Saskatoon); Maria Hendrika (Provincial Association of Transition Houses Saskatchewan); Angela Wells (Family Support Centre, Saskatchewan); Dr. Leslie M. Tutty; Dr. H. L. Radtke; Dr. Wilfreda Thurston; and Dr. Erin Gibbs Van Brunschot (University of Calgary); Dr. Caroline McDonald-Harker (University of Alberta); Dr. Ruth Grant Kalischuk (University of Lethbridge); Jan Reiner and Carolyn Goard (Alberta Council of Women's Shelters); Brenda Brochu (Peace River Regional Women's Shelter); Kristine Cassie (YWCA Lethbridge); and Pat Garrett (WINGS of Providence, Edmonton).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: Social Sciences and Humanities Research Council (SSHRC) Community University Research Alliance (CURA); Alberta Centre for Child, Family, and Community Research; Alberta Heritage Fund for Medical Research; the Prairieaction Foundation; and TransCanada Pipelines.