
Abstract
Women with disability experience higher rates of family and domestic violence (FDV) compared to the rest of the population. There is limited research into how workers in FDV and disability organizations respond to violence against women with disability. Using a case study vignette of a woman with disability disclosing FDV, this phenomenological study explored how 10 employees across the disability and FDV sectors respond to disclosures of abuse, the barriers that influenced their response, and suggested ways to improve their practices. The study found that responses were often insufficient to meet the needs of women with disability.
Male violence against women is a continuing global problem with large numbers of women impacted across the life course. Such violence represents a violation of women's human rights and act as an impediment to gender equality globally (Fitz-Gibbon, 2021; Frohmader et al., 2015). About 30% of women worldwide report experiencing either physical and/or sexual intimate partner violence or nonpartner sexual violence during their lifetime (World Health Organisation, 2018). Most of this violence was perpetrated by a male partner or former partner, often referred to as intimate partner violence or domestic violence (World Health Organisation, 2018). In Australia where the study was conducted, the rates of male-perpetrated intimate partner violence are similarly high. National data reveal that 23% of women reported partners perpetrating physical violence, sexual violence, and emotional abuse and 16% reported economic abuse (Australian Institute of Health and Welfare, 2023).
Intimate partner violence occurs across all social strata; however, not in equal proportions, with some groups of women experiencing IPV at much higher rates than others in the population (Australian Bureau of Statistics, 2017; Australian Institute of Health and Welfare, 2019; World Health Organisation, 2018). Evidence reveals that higher rates of intimate partner violence are experienced among women who are confronting multiple forms of marginalization. This includes First Nations women, women living with limited income/poverty, women who are stateless, and women with disability (Cripps & Habibis, 2019; El-Moslemany et al., 2022; Fahmy & Williamson, 2018; Klingspohn, 2018; Yapp & Pickett, 2019).
In this study, the focus is on how practitioners think about the experiences of women with disability living with violence and its implications for their practice. Of the 12.8 million women in Australia, 2 million women with a disability are twice as likely to experience abuse as compared to women without disabilities (AIHW, 2019; Commonwealth of Australia, 2020; Foster & Sandel, 2010). The prevalence of abuse against women with disability is estimated to be even higher due to underreporting and inadequate data collection processes (Dowse et al., 2016). Consistent with international data trends, abuse toward women with disability in Australia is significantly more widespread in comparison to the general population and is a leading public health concern (AIHW, 2019; Dowse et al., 2016; Frohmader et al., 2015). In contrast, the number of adult women identified as having a disability and seeking support for family and domestic violence (FDV) was 1,694 over 12 months (Australian Institute of Health and Welfare, 2023). This included 481 women reporting domestic violence as their primary reason for seeking services, 859 seeking support for both domestic violence and mental health, and 354 for domestic violence, mental health, and alcohol or other drugs. This represents about 3% of all women accessing specialist domestic and family violence services annually. Our study was focused on the overrepresentation of women with disability experiencing intimate partner violence in the population compared with this low number identified as accessing specialist domestic and family violence services (Australian Institute of Health and Welfare, 2023). Muster (2021) argues that the absence of women with disability in domestic violence responses reflects services’ lack of recognition of women with disability and their diverse experiences. The response to those women with disability accessing services then becomes “additive” to the mainstream offering, rather than driven by their needs.
Increasing the viability and access of women with disability is also complicated by the varying theoretical perspectives and definitions of disability, which vary across place and time. A commonly cited definition within the disability literature at present is the International Classification of Functioning Disability and Health (ICF) which defines disability as a result of the interplay between personal and contextual factors that inhibit and impact an individual's functioning (Kostanjsek, 2011). Women with disability face discrimination due to sexist and ableist views, attitudes, and everyday social practices, which impede their freedom to enjoy basic human rights (Frohmader, 2011). Furthermore, in comparison to people without disabilities, people living with disability experience significant barriers to participation in daily life across all domains, including employment, education, health care, and social participation (World Health Organization, 2011). This is often amplified by challenges in accessing appropriate and suitable services and supports (World Health Organization, 2011). While the context is acknowledged, it presents a relatively binary analysis and emphasizes participation differences. When looking at the experiences of women with disability, feminist authors are drawing on critical and intersectional theoretical analyses, which focus on the various ways in which interlocking forms of power, oppression, and marginalization operate within the multiple and dynamic intersections of women's lives (see, e.g., Goethals et al., 2015; Shaw et al., 2012).
For this study, intersectionality points to centering how women with disability face discrimination due to sexist and ableist views, attitudes, and everyday social practices that impede their freedom to enjoy basic human rights (Frohmader, 2011). The Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability highlighted concerns about inadequate and inaccessible healthcare systems in Australia (Commonwealth of Australia, 2020). As a result of the inaccessibility of these services, women with disability are less likely to seek support, and of those who do, approximately half reported a negative experience where service providers were unable to resolve the crisis (Plummer & Findley, 2012; Pratt-Eriksson et al., 2014; Walter-Brice et al., 2012). Muster's (2021) argument is that negative experiences will continue as the particular set of risks and needs of women with a disability when living with intimate partner violence are not at the center of service responses.
Conceptualizing Violence and Abuse Against Women with Disability: Dynamic and Intersecting Forms of Marginalization
Abuse against women is any gender-based violence that threatens to, is likely to, or causes harm, suffering, coercion, or the oppression of rights in a sexual, physical, or psychological manner (Maher et al., 2018; Plummer & Findley, 2012). For women with disability, this includes denied access to medications, mobility devices, personal care, and medical appointments, financial control of their National Disability Insurance Scheme (NDIS) funding and other finances (Frohmader et al., 2015; Plummer & Findley, 2012). It also includes the violation of bodily autonomy through increased rates of forced abortion and sterilization (Maher et al., 2018). Women with disability experience all forms of abuse at a greater rate, duration, and intensity compared with women without disabilities, often resulting in more severe injuries and negative impacts (Ballan & Freyer, 2017; Frohmader et al., 2015).
The prevailing social response to able-bodied male partners of women with disability is also a critical consideration. Within the context of patriarchy and ableism, male partners are often held in high regard and beyond reproach because if they are with a woman who “may need care” this can be seen as a female role that they are willingly undertaking. There is an assumption that the relationship has a reciprocal basis and implied notion of male sacrifice, which also makes other people less likely to consider him a perpetrator of abuse. It is critical to look at the positionality of the woman and her partner across the multiple dimensions of the types of disabling conditions, such as culture, race, class, and income (Hahn et al., 2014).
Policy Context
In Australia, responses to disclosures of FDV by women with disability are influenced by legislation, funding, and services. Often referred to as working in silos, this is replicated in the delivery of health and social services where contracts and agreements set the parameters of organizational roles and responsibilities (Women With Disabilities Australia, 2020). These responses to disclosures of FDV are impeded by differences in federal and state legislation, with funding models producing added barriers for women with disability attempting to seek help (Frohmader et al., 2015). For example, disability services are subject to a combination of federal and state legislative instruments, and funding for support is subject to the objectives of the National Disability Insurance Act. In contrast, some specialist FDV services are funded by states, while others are federally funded representing a sectoral boundary (Buick et al., 2019). The multifaceted policy-making apparatus of the Australian federal system narrows the policymakers’ remits and limits the capacity to address the multiple intersections of people's everyday lives. The result is a fragmented response to an intersectional and intersectoral problem.
Despite evidence of high rates of violence against women with disability, Australian policymakers are not encouraged to address the complex intersection of women, disability, and abuse, and current national policies and plans are ineffective at accommodating women with disability (AIHW, 2019; Fitz-Gibbon, 2021; Frohmader et al., 2015). This is apparent in national policy frameworks such as the National Plan to Reduce Violence Against Women and their Children 2010–2022, which centers upon traditional conceptions of domestic violence and fails to address the other forms of abuse experienced by women with disability (Australian Government Department of Social Services, 2019). While some stages of the National Plan attempted to target abuse perpetrated against women with disability, its effectiveness was limited due to its focus on increasing the evidence base before initiating changes to service provision (Department of Social Services, 2019; Frohmader et al., 2015).
Furthermore, the national disability policy context is underscored by a “lack of understanding of the intersectional and gendered nature of violence against women with disability” (Frohmader & La Paglia, 2021, p. 24). Women with Disabilities Australia (WWDA) suggests that violence perpetrated against women and girls with disability is only considered through the lens of disability service systems (Women With Disabilities Australia, 2020). The lack of staff qualified to respond to violence and abuse means that there is a lack of rigorous oversight and protective mechanisms, and occasions of gender-based violence are often downplayed as service incidents (Women With Disabilities Australia, 2020).
Responding to Disclosures of Violence and Abuse by Women with Disability
Both the FDV and disability sectors play an important role in the services that promote safety and recovery for women with disability who have experienced abuse (Ruiz-Pérez et al., 2018). However, employees in these services appear poorly informed about how to respond to women with disability following FDV, and there are no standard protocols, mandatory reporting, or agreed routine screening assessments (Embregts et al., 2017; Healey et al., 2013). Disability organizations are usually well equipped, with accessible buildings and with staff that possesses knowledge around disability-specific needs, however, they lack the knowledge, training, and standard protocols around how to respond to disclosures of FDV (Embregts et al., 2017; Healey et al., 2013; Ruiz-Pérez et al., 2018; Thiara et al., 2011). Disability organizations are also significantly underfunded and underresourced, which may limit their capacity to provide long-term help (National People with Disabilities and Carer Council., 2009; Thiara et al., 2011).
Conversely, FDV organizations have expertise in responding to abuse, with responses including providing refuge through crisis accommodation, offering psychological support, teaching new skills, providing resources, supporting access to legal services and court support, and connecting victims to support networks (Austin et al., 2014; Thiara et al., 2011). In reality, for women with disability, FDV services may be poorly designed with inaccessible buildings, have limited staff expertise in working with disability, and often lack the resources and funding to meet their disability-specific needs (Didi et al., 2016; Thiara et al., 2011). The inaccessibility of the FDV sector has been labeled a major barrier to being able to respond to the safety needs of women with disability who have experienced abuse (Dyson et al., 2017). There is a lack of routine cross-collaboration between the FDV and disability sectors resulting in women with disability receiving inadequate support following their disclosures, thereby limiting opportunities for early identification (Frohmader et al., 2015; Mikton et al., 2014; Plummer & Findley, 2012). As such, the basic needs of women with disability are often overlooked or dismissed and women are left in unsafe environments (Plummer & Findley, 2012). Without adequate support and intervention, women with disability risk further negative life-long health, social, and economic consequences following FDV (AIHW, 2019; Ballan et al., 2014; Foster & Sandel, 2010).
Previous research into FDV against women with a disability has focused on the experience of the women, risk factors, type of abuse, and preventative measures (Didi et al., 2016; Dyson et al., 2017; Plummer & Findley, 2012). Emerging research has begun to examine Australia's legislation that protects the rights of women with disability who encounter abuse (Frohmader et al., 2015; Maher et al., 2018). Despite the increased public awareness brought about by the Australian Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability, and the high rates of violence against women with disability, there is limited research into the perspective of the service providers (Commonwealth of Australia, 2020) or exploration of the intersections between disability and mainstream supports available (Fraser-Barbour et al., 2018). It is important to understand how service providers themselves, specifically those in the FDV and disability sectors, respond to ensure women with disability are adequately supported following their disclosures of abuse (Commonwealth of Australia, 2020; Dyson et al., 2017). This is particularly relevant because it is at the frontline of practice where evidence about what responses best support women (as well as the consequences of continuing to overlook or minimize the experience of women with disability) can be identified. Consistent with the call for smaller qualitative studies that provide deep, rich insights into the severity and characteristics of violence against women with disability (Women With Disabilities Australia, 2020), this study aimed to explore the responses of employees from the FDV and disability sectors to disclosures of FDV made by women with disability.
Method
Study Design
An inductive qualitative research method was adopted for this exploratory pilot study (Thomas, 2006). We used a phenomenological design to gain insight into how workers within the disability and FDV sectors respond to disclosures of abuse from women with disability (Cypress, 2018). Phenomenology is the search for meaning or understanding of anything that appears or presents itself, as one experiences it. “Phenomenology allows researchers to gain insights that inform practice strategies and enhance practitioners’ understanding of and sensitivity to, those they serve” (McWilliam, 2010, p. 2).
Researchers conducted semi-structured interviews with participants to describe and explore their responses to disclosures of abuse (DeJonckheere & Vaughn, 2019). A case study vignette, written in first person, formed the foundation for the semi-structured interviews. Vignettes provide a simulated description of a situation that participants in this study were likely to face in their everyday work. Vignettes are a useful way for participants to examine a sensitive and complex situation they are likely to confront in health and human services (Tremblay et al., 2022). The rationale for using a case study vignette for the interview was twofold: it enabled a direct comparison between participants from the two sectors and enabled comparison within each sector, and it provided a means by which the participants’ application of knowledge and logic of their practice decisions could be examined. First-person vignettes also have the benefit of “putting the reader at the forefront in any situation” (Boxall et al., 2018, p. 889).
Participants
Participants were invited to be interviewed for this study if they worked in either the Australian disability or FDV sector and had more than six months of experience in their role. Recruitment was conducted through convenience sampling via the researchers’ networks. While researcher networks were used to recruit potential participants, all participants were interviewed by members of the research team not known to them.
Data Collection
Following an expression of interest, the 10 participants were contacted with further information about the study. Data were collected using semi-structured interviews. Five interviews were completed face-to-face, but the onset of the COVID-19 pandemic meant the remaining five interviews were done by phone (three) and Zoom videoconference (two). All interviews were audio recorded and transcribed. An interview schedule was used to ensure consistency between interviews. The participants were presented with a case vignette of a woman with a disability disclosing her encounter with abuse. After reading the vignette, participants were asked about their role in the organizations, how they would respond to the disclosure, what steps they would take, and what approaches or policies might inform their response. A final set of questions focused on what, from their perspective, would improve future responses. Interviews ranged in length from 30 to 90 min and were audio-recorded with participant consent. Participants were given a pseudonym.
Data Analysis
Reflexive thematic analysis (RTA) was conducted based on the framework by Braun and Clarke (2006, 2019), and aided by NVivo 12 (QSR International Pty Ltd., 2018). All researchers familiarized themselves with the data set by listening to all the audio interviews. These were then transcribed verbatim via Otter.ai® (2016) in preparation for analysis. Initial themes were generated by two of the researchers (EG and DM) who independently coded all 10 interviews (via NVivo 12) before discussing the findings which were reviewed and refined among the wider team. As Byrne (2021, p. 3) suggests, RTA conducted within research teams “should be collaborative and reflexive.” All researchers met to discuss findings and search for themes, then reviewed these themes with a thematic map. Discussion of the themes was undertaken with two experts in the fields of disability and FDV to address the theoretical and empirical assumptions of the analysis (Byrne, 2021; Kielhofner, 2006; Korstjens & Moser, 2018). Themes were defined and named through a continuous drafting and refining process before the final report was produced. Reflexive journaling and audio recordings were used in all stages of the analysis to document the researchers’ decision-making process to increase dependability (Darawsheh, 2014).
Ethics
This study obtained ethical approval from the Curtin University Human Research Ethics Committee, approval number HRE2019-0749. Voluntary, written informed consent was obtained from all participants, and all participants were de-identified using pseudonyms for confidentiality reasons.
Findings
Ten employees were recruited for the study, five from each sector. Their roles consisted of occupational therapists, policy officers, women's advocates, and managerial roles with varying years of experience (see Table 1).
Participant Demographic Information.
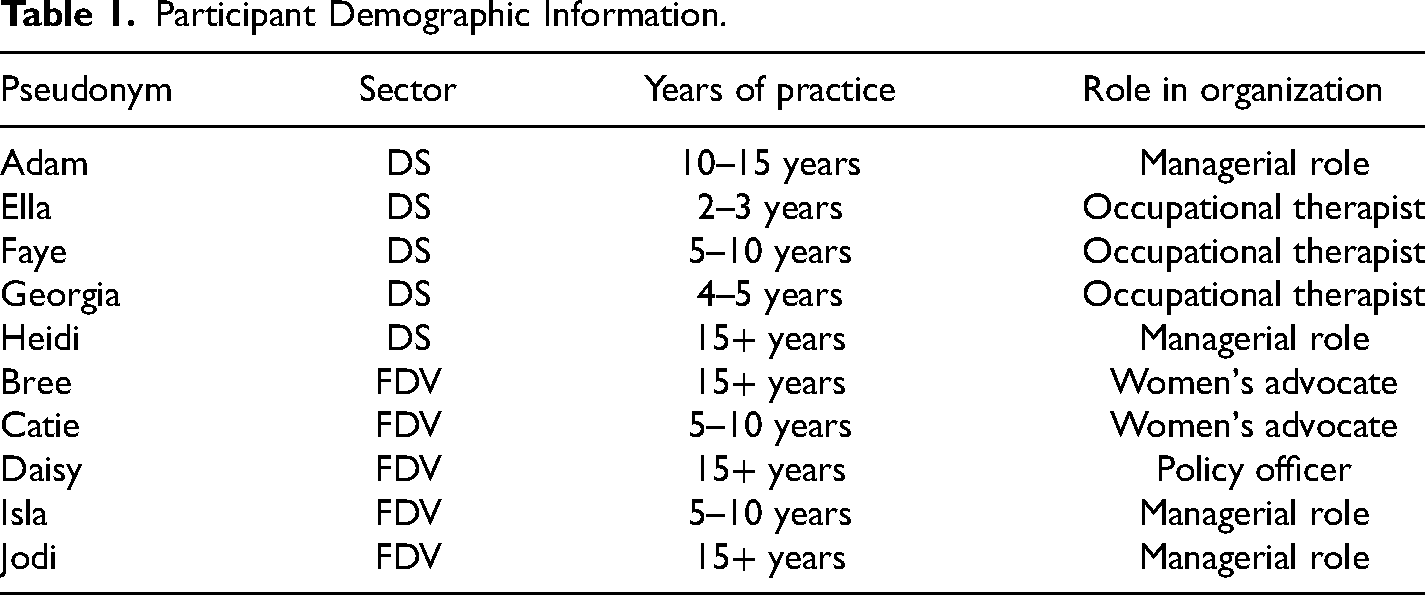
Seven interrelated themes were identified as influencing the responses of employees in the disability and FDV sectors to women with disability who experienced abuse. These were: (a) differing conceptions of disability, (b) “that's not our business,” (c) organizational policies and procedures, (d) prioritization of safety, (e) limited cross-sector collaboration, (f) accessibility of crisis accommodation, and (g) funding constraints. The themes are illustrated in Figure 1 and discussed below.
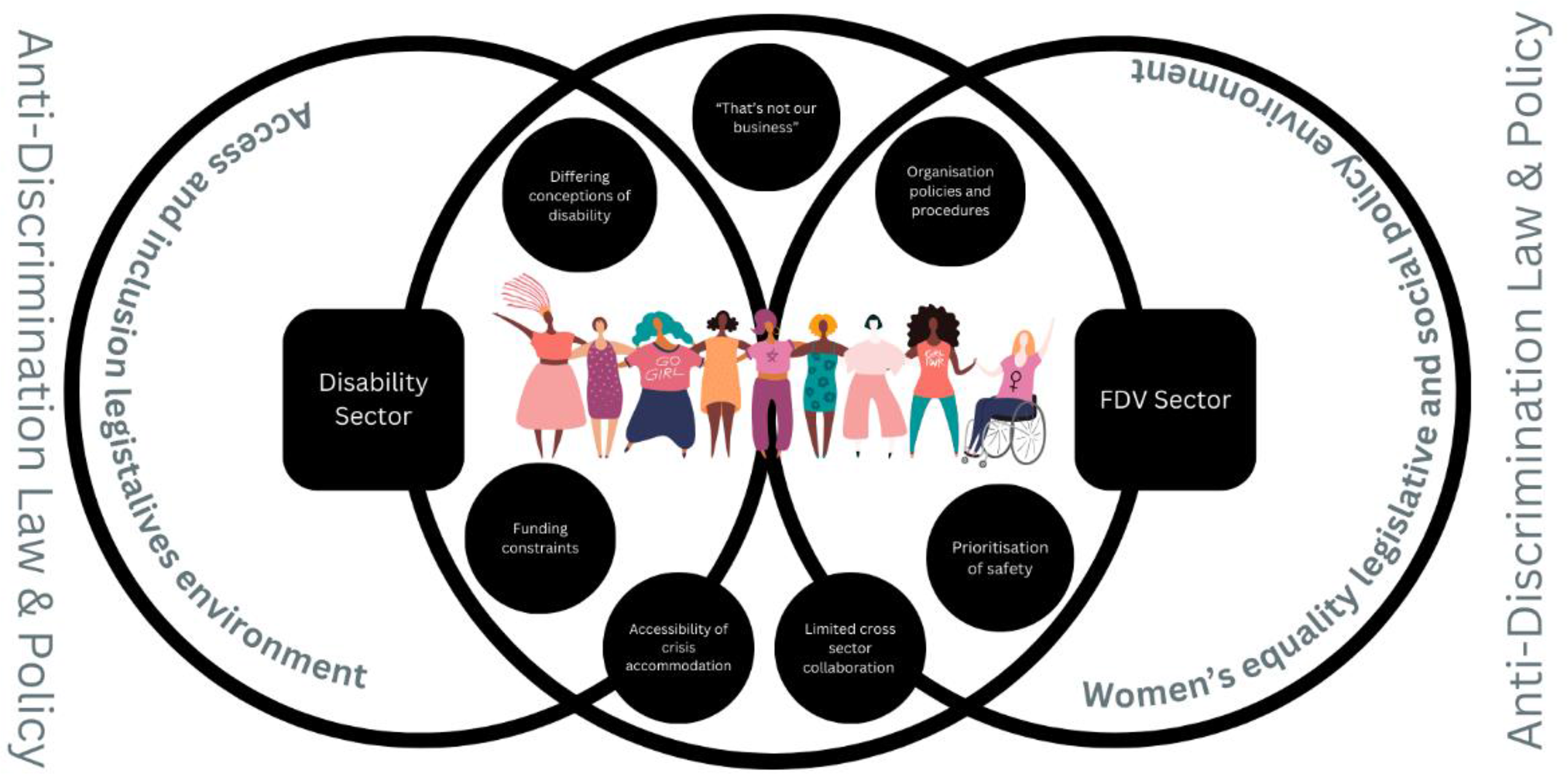
Findings Thematic Map.
Differing Conceptions of “Disability”
Participants described processes of how they would respond to disclosures of FDV by women with disabilities, which reflected their sectors of employment and more broadly, their understanding of what constituted a disability. Workers employed in the disability sector described responding to women “…living with varying disabilities” (Georgia), as including physical, intellectual or psychosocial disability. These employees were concerned with the types of disability women experienced as a key consideration in their response. This reflects the disability sector where “types” of disability direct the assessment and subsequent services. In contrast, the FDV employees tailored their responses to disclosures of abuse to the type of psycho-social disability. They considered women's experiences of alcohol and drug use as impacting function and mental ill-health, as well as women with diagnoses of anxiety and depression as being disabling. As stated by one FDV employee, “if you are counting the people that are impaired by drug and alcohol and mental health issues as having a disability, then we are managing that at a very high level” (Catie). Among the participants from the FDV sector, there was limited experience supporting women with a physical disability. One participant from a refuge explained “…the number who had hearing loss, visual loss or [the] physical need to be in a wheelchair with support was minuscule. You could count them probably on one hand” (Daisy). This may reflect the inaccessibility of refugees to women with disabilities. The responses from employees from each sector were reflective of the types of disability that were observed in their organizational settings.
“That's Not Our Business”
Employees from both the disability and FDV sectors stated that responding to disclosures of abuse from women with disabilities was outside their scope of expertise, suggesting that the intersectional complexity of the disclosure They stated they had specific knowledge about their core area of practice and a limited ability to respond to issues outside of their primary focus, suggesting that this was a specialized area of practice. Employees from the disability sector considered that responding to disclosures of FDV was outside their area of expertise and responsibility: “I’m really ashamed to say that I actually don’t know what I would do… I don’t think that it [abuse] is my organisation's responsibility… we’re not a women's refuge. That's not our business” (Ella). In contrast, employees within the FDV context highlighted their expertise in abuse, believing that disability fell outside their remit and, “whilst we’d like to support her, we are not a specialist in that area [of disability]” (Bree). These comments highlight that employees in both sectors feel uncertain when responding to the complex issue of women with disabilities who have experienced FDV, and often have a limited capacity to assist when presented with a case outside of their perceived scope of practice. Employees across both sectors considered that the intersection of women, disability, and FDV was not within their remit, which may be due to organizational or professional boundaries or sector policies and procedures.
Organizational Policies and Procedures
Sector differences in responding to FDV were shaped by organizational policies and procedures and the participant's knowledge and understanding of them. For example, disability sector employees with greater industry experience, or occupying senior managerial roles, had greater awareness and familiarity with policies and procedures within their organization. In contrast, employees with less experience working in frontline roles, could not clearly articulate what, if any, policies and procedures their organization had in place. A common response from the less experienced employees was to seek guidance from a supervisor, such as “…report[ing] that to my line manager” (Georgia). This often resulted in a delay in response as “…nothing happens fast” (Faye), leaving the woman with a disability either with no support or at potential risk of continued abuse while they waited for a response. Employees within the disability sector believed their responses to disclosures of abuse by women with disabilities would improve with the development of clear and accessible policies and procedures.
In contrast, employees in the FDV sector were familiar with their organization's policies and procedures and were able to demonstrate a clear understanding regardless of their position within their organization, with multiple policies in place including “…an assessment framework, a clinical intervention framework…ongoing therapeutic work…and we follow a three-phase trauma therapy model” (Isla). This ensured consistency within FDV organizations, as all employee's responses were guided by clear policies and procedures. These differences between the sectors highlight that the responses women with disabilities receive may vary significantly depending on the employee's knowledge of how to respond, and their familiarity of organizational policies and procedures.
Prioritization of Safety
Employees in both sectors emphasized the importance of women's safety, however, the safety needs that were prioritized differed between sectors. The disability sector employees prioritized the continuity of personal care needs to protect the woman's safety. For example, “…the fact that she's left without support workers at home is quite a dire situation and her safety is at huge risk. So, trying to find emergency support to be able to go in and give her the care support she needs [is important]” (Adam). This form of safety was focused on the woman's physical well-being, particularly where women may have relied on aides or others to maintain their health. In the FDV sector, the initial response was to secure the women's immediate safety by removing the women from the perpetrator, relocating them into crisis accommodation, and involving police and medico-legal systems. One FDV employee stated, “immediate safety first. Do they need emergency services, emergency accommodation, or police or hospital admission?” (Heidi) with another stating, “getting a family violence restraining order and having [the perpetrator] removed from the house” (Daisy). Participants from the disability sector would likely prioritize maintaining the women's care needs, while participants from the FDV sector focused on the risk and danger that the perpetrator of violence posed to the woman. Safety in this way refers to not being subjected to further or more extreme abuse at the time of disclosure. To achieve this, FDV participants prioritized the separation of the victim and perpetrator. This highlights the significant variations in the responses taken to secure the woman's safety across the two sectors.
Limited Cross-Sector Collaboration
Employees across both sectors identified that collaboration between the sectors is limited and inconsistent. The disability sector employees did not identify how they would collaborate as a matter of regular practice with the FDV sector to support women with disabilities. Disability sector employees did, however, state that they would refer to a social worker, if one was available in their organization, to connect the women with local domestic violence support.
Conversely, FDV employees demonstrated awareness of methods to involve the disability sector by identifying specific organizations to contact to arrange care, such as “…support services that help people with their NDIS and I’d be wanting to make sure she was linked in with services that would also be supporting her [disability specific needs]” (Bree). There was consensus from both the disability and FDV sectors that collaboration between the sectors is crucial to address the combination of FDV and disability, as each sector's scope lies solely in their expertise limiting either sector's ability to provide holistic care. Employees across both sectors proposed that this could be achieved through the development of joint policies and procedures. Both sectors also highlighted the importance of having contacts within either sector to support their response and thus suggested that staff from both sectors complete “joint training to build up relationships in their local areas [with other local employees]” (Daisy). The current limited and inconsistent cross-sector collaboration between the disability and FDV sectors impacts their abilities to respond to women with disabilities who experience abuse, and employees appear determined to remedy this.
Accessibility of Crisis Accommodation
The lack of availability of accessible crisis accommodation was identified by participants from both sectors as a significant barrier in responding to disclosures of abuse by women with disabilities. Common accessibility barriers to the accommodation for women with physical disability included stairs, narrow halls, and doorways, along with inaccessible kitchens and bathrooms. While it is a legal requirement for FDV services to have a wheelchair-accessible unit, the likelihood of that unit being available when required could not be guaranteed. An FDV employee stated they are “yet to see the unit being a perfect match for a family that absolutely needed that disability unit” (Catie). There were also accounts in which the accommodation was labeled “accessible,” however, when allocated to a woman with a disability, it did not meet her specific needs or cater for support workers: There's a huge paucity of crisis accommodation availability and even if it is available, the suitability to people with disabilities is sometimes a factor as well. Whether that is the physical aspect, the emotional environment, someone might have a sensory impairment or a whole range of things. So, number one is having a bed available, and number two is the appropriateness for that person. (Heidi)
Another issue identified within FDV services was not having accessible vehicles to transport women with physical disability into crisis care, as “…our vehicles won’t allow her with a wheelchair” (Jodi). In some cases, the geographical distance between crisis accommodation and the women's place of residence was a barrier. This posed an additional challenge in accessing services as the women's support workers were required to travel to provide care.
Funding Constraints
The disability and FDV sectors both highlighted financial constraints and the need for additional funding to improve services for women with disabilities who experience FDV. The disability sector employees identified current funding constraints in the NDIS when responding to crises as there is no supplementary emergency funding. This results in funding being taken out of the woman's current NDIS plan, sacrificing her therapy and assistive equipment funding to receive crisis support instead. One key issue for this is “when [clients] have 20 hours of therapy for an entire year, and you spend three hours doing a risk assessment…then they don’t get that new piece of equipment because they don’t have the hours [of funding remaining]” (Ella). This also points to a key problem related to policies and their implementation through funding of services, in Ella's example the risk assessment for FDV is treated as time from her disability support, when it is an FDV problem, so women not experiencing disability would not be subjected to “trading off” time from another service for an FDV assessment to be undertaken.
Not only did each sector identify its need for increased funding, but both also emphasized the need for additional funding to specifically improve cross-collaboration between sectors, as “the only way you can bring agencies together is if you offer money [to assist with] working together” (Jodi). Funding could be used for running joint training, collaborative case management processes, and other measures to improve identification and responses to women with disability experiencing FDV. The FDV sector highlighted the importance of funding to improve the accessibility and availability of crisis accommodation. However, participants explained women with a physical disability would be “…a low priority” (Jodi) as they are not frequent users of the service and were described as “not attracting” the same level of funding compared to women who access services with mental health conditions. Conversely, another FDV employee suggested that the low frequency of women with a physical disability seeking services is due to the inaccessibility of services, with difficulties “justify[ing] additional funding when there is no real demand, but there's no real demand because it's impossible to get into the refuge because there's no real capacity” (Daisy). Additionally, while employees recognized government efforts to improve the collaboration between the sectors, they identified that funding has been insufficient, and is too constrained to make a lasting long-term improvement.
Discussion
The findings revealed that the disability and FDV sectors responded in different ways to the same scenario of a woman with disability disclosing violence and abuse. The disability sector participants initially focused on the range of disabilities the woman may be experiencing—physical, intellectual, or psychosocial disabilities—and how this would be a key factor influencing their response. In contrast, the FDV sector participants focused on mental health and safety concerns as this was the primary type of disability they had experienced in their workplaces. It could also reflect that refuge workers view many of the signs of mental distress to be the effects of abuse (Humphreys & Thiara, 2003; Laing et al., 2012). The focus on different types of disability may also add complexity for employees in the disability and FDV sectors when determining the collaborative organizational responses required to support a range of women with disabilities who experience FDV (Maher et al., 2018; Muster, 2021). In moving forward, it is important to consider how each level of response requires change.
Policy Limitations and Potential
Consistent with other overlapping policy areas (e.g., Hussain et al., 2021), the policy silos described earlier in the paper cascade down into organizational and practice silos resulting in differential responses to women with disability experiencing FDV. Consequently, participants from both sectors described how the intersection of women, disability, and abuse fell outside of their scope of practice. This means that women with disabilities who experience FDV fall into a grey area, where neither service system adequately responds to the woman's needs. Muster (2021) argues this is a direct result of women with disability being obscured because domestic violence service designs are built upon the presumption that women are able-bodied, heterosexual, and so on.
This study further extends Muster's (2021) argument that the disability sector conceptualizations often do not gender, sexualize, or racialize their service users to consider their intersecting identities and multiple forms of marginalization. Consistent with this argument, Walter et al. (2023) suggest that both service systems are ill-equipped to respond appropriately because of the assumptions held and the barriers that exist between each sector. This is congruent with previous studies that found the disability sector was weak in its response to FDV, whilst the FDV sector was weak in its practice with disability (Dyson et al., 2017; Robinson et al., 2020).
This is further supported by Maher et al. (2018) who suggested the impact of siloed knowledge in different policy domains and services results in responses that are reflective of only partial knowledge, skills, and service delivery models. Organizational policies and procedures across both sectors must address the complex intersection of gender, disability, and abuse. Promoting the safety and dignity of women with disabilities being subjected to FDV demands a range of agencies to work together to provide support and advocacy and reduce the risk of further violence and abuse.
Policy Based on Greater Collaboration and Advancing Multiagency Working
As with earlier iterations of multiagency working in domestic violence (Hauge & Malos, 1998), an intersectoral analysis to enhance domestic violence responses to women demands a more sophisticated form of multiagency or coordinated working. Multiagency coordination is still underdeveloped as its breadth and practice require evolution to enable more comprehensive and wide-ranging responses. This presents a perennial issue in the sectors of having a skilled and well-trained workforce to respond to the community's need for safety.
Organizational Level Responses
Responses to women with disabilities who disclose FDV are mediated by the organizational context and the individual practitioner. In the disability sector, there was limited knowledge about how to respond to a disclosure of FDV and in the FDV sector, there was little experience with women with disabilities accessing the services. Due to unclear policies and procedures within the disability sector, employees have limited guidance on how to respond, often resulting in responses that are insufficient to meet the women's specific needs. This is consistent with research finding that disability support professionals are not well prepared, or well informed, about how to provide adequate responses to disclosure of abuse made by women with disability, as they have minimal understanding of FDV organizational policies and procedures (Embregts et al., 2017; Healey et al., 2013).
Mahapatro (2018) suggests that the absence of clear organizational response protocols is one of the most common factors leading to an inadequate response. Without a clear organizational remit to respond to FDV disclosures, there is unlikely to be a drive to ensure workforce development in this area, and the status quo will remain. To begin to address this aspect, organizations in the disability sector require FDV-informed policies and procedures for staff, which managers of organizations must ensure are well understood and able to be implemented by staff. This is necessary for service users to receive a comprehensive response that is appropriate to their intersectional needs. The role and responsibility of the organizations in responding to FDV have to be enshrined in the policies and procedures and the funding conditions of organizations to bring about workforce development and accountability for their responses.
A severe lack of accessible and available crisis accommodation was highlighted as a barrier to responding to women with a physical disability who experience FDV. As the FDV sector's predominant response centers on creating safety for the victim, the inaccessibility of crisis accommodation poses challenges to safeguarding the victim and enabling their care supports to follow them regardless of their residence. While FDV policies and procedures are similar, FDV services require an organizational shift and workforce development initiative to be held accountable to standards of inclusion from the architecture of services through to the knowledge base of staff.
Everyday Practice
An important finding of this study was the stark difference in what was meant by the concept of safety in the different workforces. While both groups prioritized safety, what was being prioritized differed. It was translated by disability employees to describe how they ensure the continuity of care. In contrast, for FDV employees, safety was centered on removing or reducing women's risk of further harm and violence (specifically about separation from the perpetrator at the point of crisis). While both responses are important to the woman's bodily integrity, either one on its own is unlikely to reduce current and future harm sufficiently to promote the safety and well-being of women with disability who have experienced FDV. This finding is supported by Robinson et al. (2020) who state that the disability and FDV sectors must have a holistic understanding of women with disability's specific needs, to ensure that their response targets all elements of their safety. This suggests that better training in practice responses for both workforces is critical for strong cross-sector collaboration at the organizational level.
Limited and inconsistent collaboration between the sectors was identified in the current study, and employees from both sectors agreed that their response would be improved with increased collaboration. There is little to no collaboration between the disability and FDV sectors when it comes to supporting women with disabilities (Dyson et al., 2017; Healey et al., 2013; Maher et al., 2018; Robinson et al., 2020), and as is the case with many siloed areas of practice, improved cross-sector collaboration remains a favorable goal (Buick et al., 2019) These findings are consistent with other research that suggest best practice would be achieved with closer cross-sector collaboration and a multilayered service response resulting in better outcomes for women with disability (Healey et al., 2013). It is possible that certain strategies, as outlined in public policies aimed at reducing siloed services and fostering the development of workers who cross sector boundaries (Buick et al., 2019), could be beneficial in addressing the distinct responses received by women with disabilities.
Findings are supported by studies that show that the lack of available and accessible crisis accommodation is a barrier that significantly limits services’ ability to respond (Dyson et al., 2017; Robinson et al., 2020; Thiara et al., 2011). Therefore, to improve responses, the physical accessibility of women's refugees should be prioritized using universal design principles in re-designing and developing future accommodation services. Increased funding to facilitate accessibility, training, and cross-sector collaboration may lead to improvements in responses in both sectors. Limitations with funding levels negatively impact both sectors’ capacity to improve their responses. This finding is congruent with literature that contends that the disability service system is chronically underfunded and lacks the resources for cross-sector collaboration (Maher et al., 2018; National People with Disabilities and Carer Council, 2009). Similarly, Dyson et al. (2017) found that there was limited funding within crisis accommodation refuges to support the modifications needed to develop fully accessible shelters and services. Further research should explore the funding constraints within and between the disability and FDV services, to determine how to overcome this issue and improve the responses women with disability receive when disclosing abuse.
Finally, there is a clear line between siloed policymaking within government portfolios and the service contracts for both sectors. While the Commonwealth National Policy identifies that women with disability experience higher rates of FDV and their needs should be better addressed, there are currently very few mechanisms within the federal policymaking processes that can result in implementing change in front-line services across Australia. There are projects and trials but sustained change that enables services to have the flexibility to work collaboratively at the intersections of women's lives to ensure they are safe and live free from violence remains elusive without an ongoing commitment between national and state/territory governments (Women With Disabilities Australia, 2020).
Limitations
This exploratory qualitative study has the following limitations. The participant numbers were small, the participants were drawn from a limited number of agencies due to time and resource limits and participants all voluntarily opted into the study. Phenomenology is a powerful method for examining the effects of experiences within a group of people and was appropriate for this study (Grossoehme, 2014), however, one limitation of qualitative designs such as this, is that transferability of the results is limited. Participants’ responses may have been influenced by social desirability response bias, whereby employees working within the disability and FDV sectors may have answered questions in a manner that would be viewed favorably by others, rather than an accurate reflection of how their organization (and the participants) respond to disclosures of FDV. This study sought to lessen the impact of social desirability by using a vignette in semi-structured interviews where the focus was on knowledge application. This allows for flexibility in questioning and probing to help participants feel comfortable and elicit a more authentic response. As the study elicited detailed information about the practice, it is recommended that this study be repeated with a larger sample size to identify the range of practice across both sectors. Another possible limitation could be the way that moving to an online mode due to COVID-19 impacted the data. However, a study by Oates et al. (2022) suggests this may be unfounded. They compared audio, video, chat, and survey interview methods and found “little evidence to suggest that any of these modes had substantial impacts on the validity or data equivalence of interviews” (Oates et al., 2022, p. 38). Furthermore, the authors did not investigate the impact of COVID-19 on the practice contexts, as the research protocol and half the interviews were completed before the onset of the pandemic.
Future Research
Future research should be focused on further exploring the response of Australian disability and FDV sectors to disclosures of abuse from women with disability, the barriers they encounter, and suggested ways to improve their response from the perspective of the employees within both sectors. Multiple vignettes depicting various scenarios would help explore more diverse forms of FDV. A larger research study that examines workers’ approaches in services to a larger number of women confronting a diverse range of circumstances could offer much greater nuance about how to better develop service responses. It is recommended that future research examines the implementation of organizational policies and procedures, accessibility of services, and cross-sector collaboration, to aid in developing better policy, workforce, and practice approaches that improve service responses to women with disability who disclose FDV. Finally, studies that continue to be co-designed with women with disability to develop greater insight and evidence are still necessary in this emerging area of feminist activism.
Conclusion
This study explored the responses of employees within the disability and FDV sectors to disclosures of FDV made by women with disability. Overall, the findings suggest that there are clear differences in response to women with disability between these two sectors. Each sector has expertise, which is crucial to integrating support more comprehensively for women with disability. The disability and FDV sectors have siloed organizational remits, policies, procedures, and knowledge. When both sectors act independently, they will not achieve the best outcomes for women. As a result of this dual or parallel approach, the disability and FDV sectors’ responses do not meet all aspects of the women's needs and are therefore placing some women at risk of further violence and abuse. This is exacerbated by inaccessible policies and procedures. To improve responses, cross-sector collaboration is necessary to successfully foster a healthy, safe support system for women with disabilities. Importantly, employees identified that improvements directed toward their response are constrained by limited accessibility and a lack of funding. This requires an examination of how the current policy-making mechanism in Australia's federal system could better respond to the complex intersectionality of its citizens’ lives.
Supplemental Material
sj-docx-1-vaw-10.1177_10778012241236676 - Supplemental material for How Do Employees in the Disability and Family and Domestic Violence Sectors Respond to Disclosures of Violence From Women With Disability?
Supplemental material, sj-docx-1-vaw-10.1177_10778012241236676 for How Do Employees in the Disability and Family and Domestic Violence Sectors Respond to Disclosures of Violence From Women With Disability? by Rebecca Waters, Jarla Anderson, Elise Gullotti, Gabrielle King, Demee Martin, David Hodgson, Lynelle Watts and Donna Chung in Violence Against Women
Supplemental Material
sj-docx-2-vaw-10.1177_10778012241236676 - Supplemental material for How Do Employees in the Disability and Family and Domestic Violence Sectors Respond to Disclosures of Violence From Women With Disability?
Supplemental material, sj-docx-2-vaw-10.1177_10778012241236676 for How Do Employees in the Disability and Family and Domestic Violence Sectors Respond to Disclosures of Violence From Women With Disability? by Rebecca Waters, Jarla Anderson, Elise Gullotti, Gabrielle King, Demee Martin, David Hodgson, Lynelle Watts and Donna Chung in Violence Against Women
Footnotes
Supplemental Material
Supplemental material for this article is available online
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.