
Abstract
Gender norms have been posited to impact intimate partner violence (IPV), but there is scant evidence of the longitudinal association between community-level gender norms and IPV. Using longitudinal data on 3,965 married girls surveyed in India, we fitted mixed-effects ordinal and binary logistic regression models for physical IPV intensity and occurrence of sexual IPV. We found a 26% increase in the odds that women experience frequent physical IPV per one unit increase in greater community-level equitable gender norms. We did not find an association between community-level equitable gender norms and sexual IPV. Findings suggest that the relationship between gender norms and physical and sexual IPV differs, indicating the need for tailored interventions for different types of IPV.
Background
Globally, intimate partner violence (IPV) is a human rights issue and a widespread public health challenge, with nearly one-third of women reporting experience of physical and/or sexual violence in their lifetime (Devries et al., 2013). Despite stringent laws protecting women from IPV, the prevalence of IPV in India mirrors global figures, with one in three women ages 15–49 reporting experience of physical and/or sexual violence in their lifetime (International Institute for Population Sciences, 2017). In terms of prevalence among adolescent girls and young women (AGYW), 25% of women aged 20–24 years and 18% of women aged 15–19 years reported experiencing any physical or sexual IPV violence (International Institute for Population Sciences, 2017). About 5.2% of women ages 15–49 also reported enduring sexual IPV in the 12 months preceding the survey (Coll et al., 2020). Nearly half of all women ages 15–49 years exposed to physical and/or sexual IPV reported suffering injuries, but only 14% of those who experienced IPV ever sought help (International Institute for Population Sciences, 2017). It remains a silent epidemic in India that continues to have detrimental impacts on girls and women of all ages.
In the last two decades, numerous studies have examined the role of individual risk factors and their association with IPV. Worldwide and in India, women from lower socioeconomic status, belonging to a marginalized caste, marrying below 18 years of age, having lower educational attainment, and being employed are strongly associated with greater risk of IPV (Abramsky et al., 2011; Ahmad et al., 2021; Dalal & Lindqvist, 2012; Koenig et al., 2006; Semahegn et al., 2019; Speizer & Pearson, 2011). In terms of spousal factors (factors at the level of the husband–wife dyad), studies have shown that a greater spousal age gap is associated with a higher risk of IPV for women (Koenig et al., 2006; Speizer & Pearson, 2011). Greater gap in education or income between the husband and wife is also positively correlated with higher IPV among women (Ackerson & Subramanian, 2008; Ahmad et al., 2021; Koenig et al., 2006; Speizer & Pearson, 2011). Recent evidence has also highlighted that witnessing IPV in childhood, lower empowerment, and partners’ alcohol use are the strongest correlates for IPV risk among women 15–49 years in India (Coll et al., 2021).
In addition to individual risk factors, contextual risk factors play an important role in determining IPV. Restrictive gender norms are defined as norms that sustain power and privileges of what is considered masculine or male and reinforce systemic inequalities undermining women's rights (Heise et al., 2019). These restrictive gender norms are upstream determinants of gender inequality acting as contextual risk factors. Restrictive gender norms manifest in many ways—skewed sex ratio at birth, differential educational attainment for boys and girls, early marriage for girls, gender bias in employment, higher crime rate against women, and prevalence of gender-discriminatory cultural practices (Desai & Andrist, 2010; Jayachandran, 2015; Nanda et al., 2014; Weber et al., 2019).
Despite the importance of gender norms as contextual risk factors, few studies have examined their associations with IPV risk in South Asia. Koenig et al. (2006) examined the association of community-level norms around wife-beating and crime rates in North India with IPV risk (Koenig et al., 2006). While permissive norms regarding wife beating were associated with physical IPV, the study did not find a significant association with sexual IPV. Further, a high violent crime rate at the community level was positively correlated with both sexual and physical IPV (Koenig et al., 2006). In another cross-sectional study, Ackerson and Subramanian found that differences in IPV among neighborhoods and among states were partially explained by gender inequality at the state level (Ackerson & Subramanian, 2008). In examining the role of women's educational context on IPV, Ackerson and colleagues found that living in communities with high male and female literacy levels was associated with a reduction in IPV risk after controlling for individual factors (Ackerson et al., 2008). More recently, a socioecological cross-sectional analysis of spousal violence emphasized that living in communities with inequitable gender norms (measured using men's and women's attitudes toward wife-beating), higher crime rates against women, and more marriages of women below 18 years of age were associated with greater odds of women's experience of spousal violence (Ahmad et al., 2021).
Most of the contextual research on IPV in India has used cross-sectional data with scant use of longitudinal data. Many IPV articles combine the physical and/or sexual IPV into a single outcome, limiting our understanding of how norms influence different types of IPV. Further, we know little about IPV among newly married AGYW in resource-constrained settings. This article builds on the literature on IPV by examining norms longitudinally, over a 3-year timeframe, to better understand the relationship between community-level gender norms and both physical and sexual IPV. This article aims to study the longitudinal association between community-level collective gender norms of newly married young women and the intensity of physical IPV and recent sexual IPV. We hypothesized that AGYW who live in more gender-equal communities, as defined by our collective gender norms variables, will experience less physical and less sexual IPV, after controlling for individual and relational factors.
Theoretical Framework
The theoretical framework (Figure 1) for this study is grounded in an ecological perspective that emphasizes multidimensional “embedded levels of causality” (Bronfenbrenner, 1977; Dutton, 1988; Heise, 1998). Developed by Heise (1998), the ecological framework of gender-based violence conceptualizes IPV as a function of the interacting influence of numerous factors at the individual, relational, contextual, and structural levels (Figure 1).
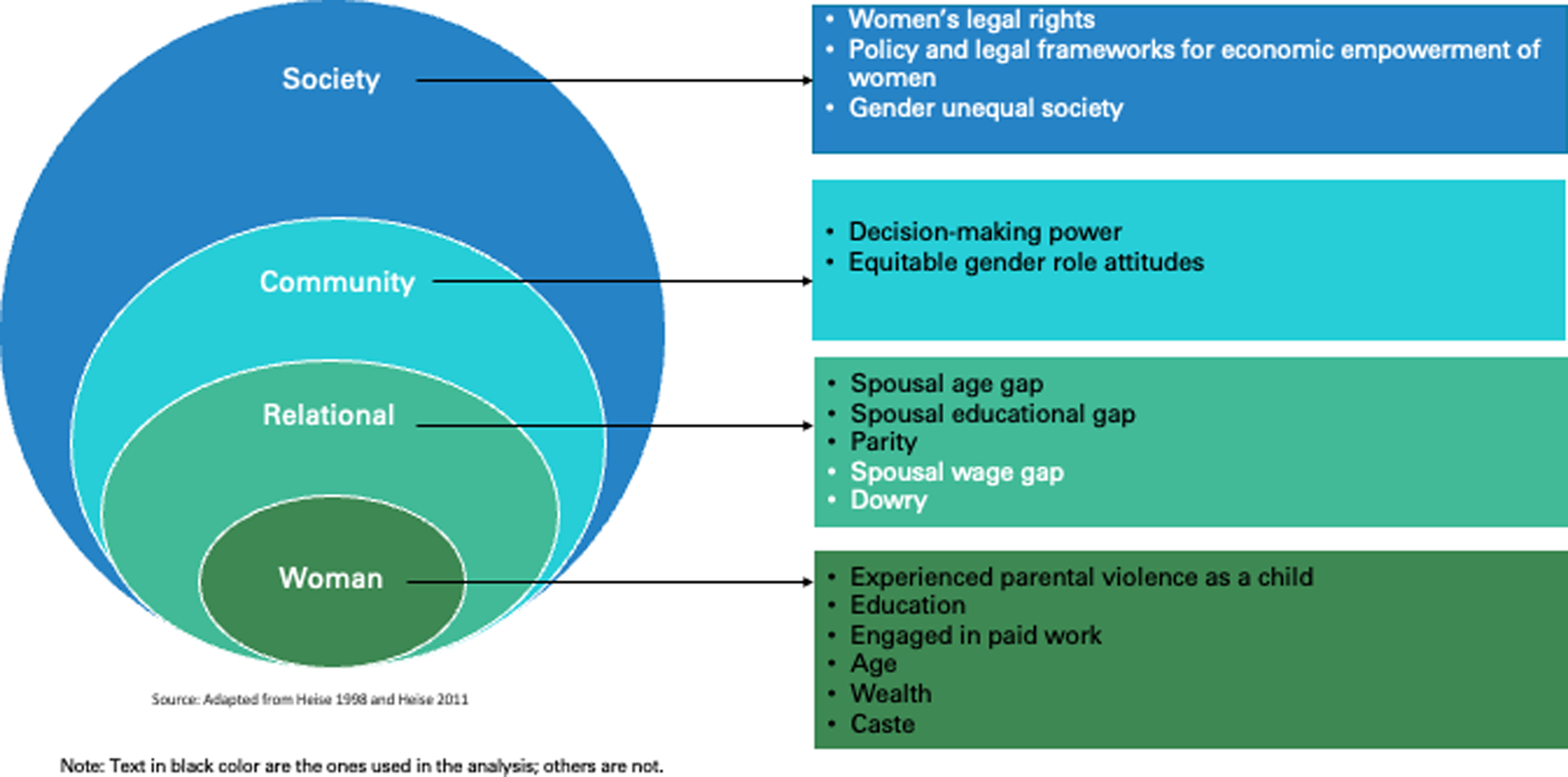
Socioecological Model Depicting the Relationship Between Community Collective Gender Norms and IPV.
Method
We used prospective cohort data from the Population Council's UDAYA study conducted in two large northern states—Bihar and Uttar Pradesh (UP)—in India (Santhya et al., 2017). The survey collected longitudinal data from married AGYW (15–19 years) who were selected using a multistage sampling strategy within 300 urban and rural primary sampling units (PSUs) representative of UP and Bihar in two waves: 2015–2016 (Wave 1) then followed-up in 2018–2019 (Wave 2). The survey covered various topics such as marriage and reproductive events, IPV, and measures related to women's empowerment including decision-making and gender role attitudes. The study received ethical approval from the Institutional Review Boards of Population Council USA and Center for Media Studies (CMS), India. Since we used deidentified data from a public website, the Harvard Dataverse, we were exempt from getting Institutional Review Board approval at the University of California, Berkeley.
Our analytic sample for analysis included 3,965 AGYW married in 2015–2016, still married in 2018–2019, and cohabiting with their husbands at both waves across 288 communities (PSUs). For the models, we omitted all communities that had only one respondent, leaving 3,959 individuals from 282 communities in the final analytic data set. We had comparable measures for AGYW across the two waves, including repeated measures of their exposure to IPV, decision-making, and gender attitudes. Our covariates/controls were selected a priori based on previous literature and theory represented as a directed acyclic graph (Figure 2; Greenland et al., 1999).
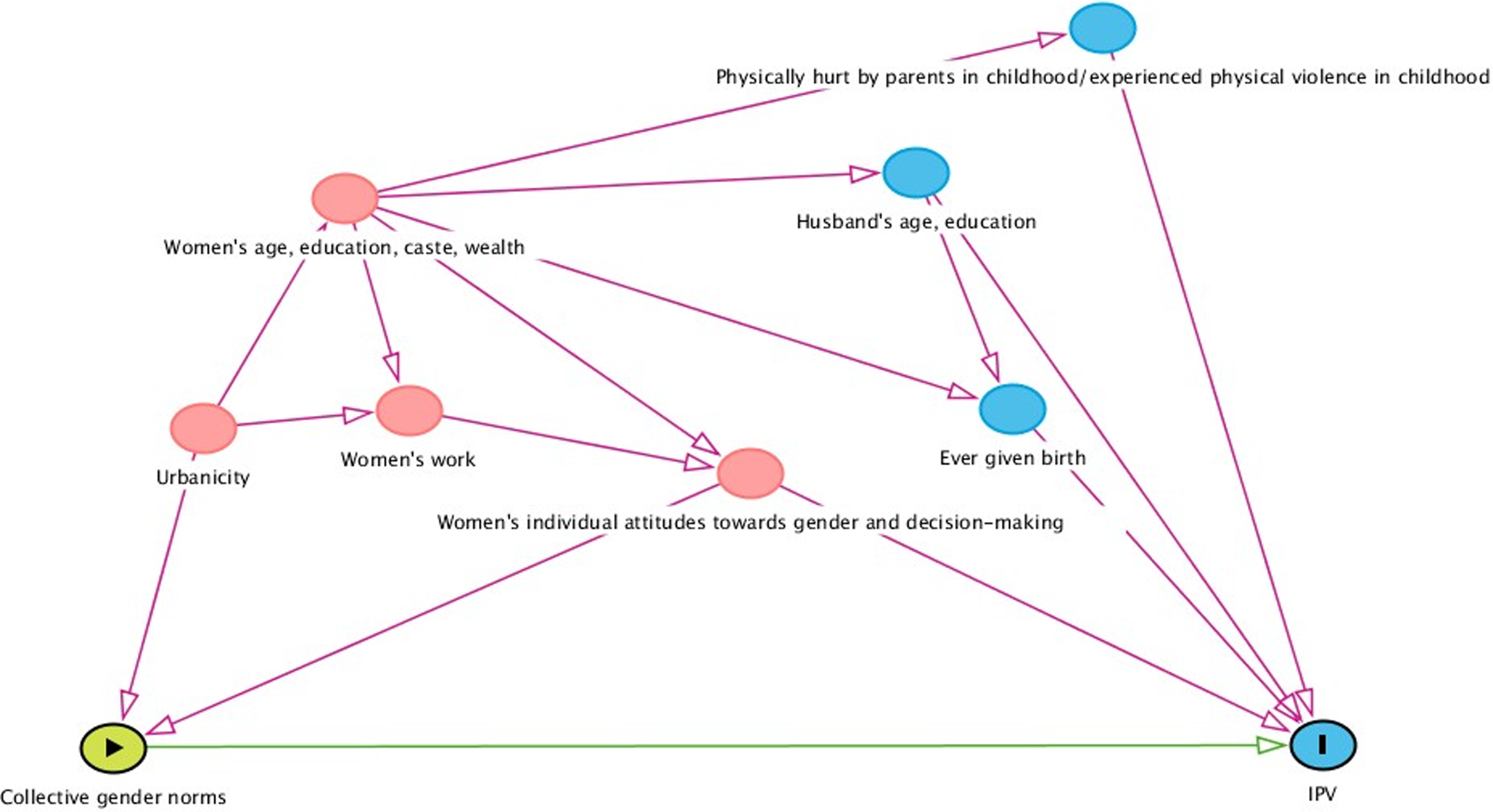
Directed Acyclic Graph Examining the Relationship Between Collective Gender Norms at the Community Level and IPV.
Measures
Dependent variables
The survey used standard questions on physical violence modeled on the demographic health surveys’ domestic violence module (International Institute for Population Sciences, 2017). Married AGYW were first asked about ever having experienced physical IPV and about recent experiences of IPV in the 12 months preceding the survey. The physical IPV questions asked the respondents if they had ever experienced any form of physical violence, including being slapped, twisted, having their hair pulled, being pushed, having something thrown at them, and being punched with a fist, kicked, choked, or threatened with a gun, knife, or a weapon. For those who had ever experienced physical IPV, a follow-up question ascertained the frequency of physical IPV in the 12 months preceding the survey, the responses for which included (a) never experienced in the last 12 months, (b) sometimes in the last 12 months, and (c) often in the last 12 months. Combining these two questions, we created an ordinal variable for physical IPV intensity that included four levels
Independent variables
Since there is no gold standard measure for gender norms, we relied on proxy measures of gender equality or empowerment focused on intrahousehold decision-making that have been used in other research domains to explore their relationship with IPV (Malhotra et al., 2002; Presser & Sen, 2000) and used the set of questions measuring gender role attitudes that were available in our survey. We developed our community-level measures using PSUs that denote a local geographical area—villages in rural areas and wards in urban areas. Below we explain how we operationalized our collective gender norm variables:
Community-level decision-making index: We used questions posed to married AGYW about who in the family mainly makes decisions related to AGYW. Women were asked who mainly decides about (a) how much education the woman should have, (b) making major household purchases, and (c) whether the woman should work or stay at home. For each of these variables, we assigned a score of 1 if AGYW reported making decisions solely or jointly with others and 0 if AGYW have no say in making decisions. Items were averaged to form a scale with higher scores indicating greater decision-making ability. The index was rescaled to range from 0 to 5. Finally, we aggregated individual women's responses at the community level for each PSU and created nonself-means by removing the index woman when averaging the responses. Community-level equitable gender attitudes index measures the respondents’ views regarding acceptable practices and behaviors for men and women. These types of attitudinal statements are used in research as a reflection of prevailing gender norms. Five statements on gender role attitudes were asked to AGYW: (a) it is more important to educate boys than girls, (b) girls like to be teased by boys, (c) girls should be allowed to decide when they want to marry, (d) husband alone/mainly should decide how household money is spent, and (e) feeding and giving kids baths is only women's responsibility. For each item, respondents indicated whether they agreed, disagreed, or “could not say.” Items were coded such that a response that was deemed equitable was coded as 1 and 0 otherwise. “Could not say” responses were combined such that the absence of an affirmative response indicated inequitable gender attitudes to ensure that we erred on the side of being more conservative. Items were added to create a summative scale from 0 to 5, with higher scores representing more equitable gender attitudes and aggregated at the community (i.e., PSU) level. We created nonself-means by removing the index woman when averaging the responses.
Other covariates known to be associated with collective gender norms and IPV were also controlled for. At the individual level, these include AGYW's age, wealth, education, caste, individual decision-making power, and individual equitable gender role attitudes. At the spousal level, confounders such as spousal age gap, spousal educational gap, and whether the respondent had ever given birth to a child were theorized to be important based on prior literature from India. We also controlled for the urbanicity of the community (urban or rural). To allow for any secular trends, we also controlled for time by including an indicator variable for the second wave.
Analysis
The relationship between collective gender norms at the community level and IPV was examined using a three-level hierarchical random-effects model (written out as a reduced-form equation) to account for the multilevel nature of the data. The three levels were waves (level 1) nested within women (level 2) nested within communities (level 3). Multiple married women were not sampled within households; thus, we do not include a household-level random intercept. Hence, variables that reflect household characteristics such as caste and wealth index were included at the individual level. We first descriptively reviewed the data for variables of interest and assessed the distributions of the variables. We then tested whether the means of the community-level collective gender norms variables changed from Wave 1 to Wave 2 by conducting paired t tests. We generated proportions of AGYW experiencing violence by ever experience of physical and sexual IPV. We used chi-square tests to examine bivariate relationships between covariates and reports of any IPV at Wave 1.
We fitted two separate regressions for the two outcomes of interest—mixed-effects proportional odds (or ordinal logistic) regression (Agresti, 2010) and mixed-effects binary logistic regression models for physical IPV intensity and recent sexual IPV, respectively, to examine the individual-level predictors first, followed by spousal-level predictors, and then finally the collective gender norms variables. We also fit a model by interacting all our covariates and collective gender norm variables with time (indicator for the second wave) to test for moderation by time. We set the level of statistical significance (Wald p value) at 0.05 for regression models except for interaction terms where we used a significance level of 0.1 and used cluster robust standard errors by PSU (community-level). We conducted paired t tests and found that the mean norms at the two waves were statistically significantly different (p < .05).
Model 1 was the unadjusted model that included our main predictors of interest, the collective gender norms that included the community-level greater decision-making power index and the community-level equitable gender attitudes index. Model 2 added the individual-level covariates including age, the AGYW's education, whether the respondent belonged to a marginalized caste, wealth index, individual-level decision-making, and individual-level equitable gender attitudes. Model 3 controlled for spousal-level covariates spousal age gap, spousal educational gap, and whether the respondent had ever given birth to a child as well as finally whether the community was urban or rural, and secular trends by including an indicator variable for the second wave. We evaluated model fit using Akaike Information Criteria (AIC) with lower values signifying better model fit. All data were analyzed using Stata Version 15.1(Stata Statistical Software: Release 15, 2017).
Results
We present the sociodemographic characteristics of our analytical sample at Wave 1 (n = 3,965) in Table 1, overall and by ever experience of physical and sexual IPV. The median age of women at Wave 1 was 18.0 years (range 15–19, IQR: 17, 19). The median number of years of formal schooling was 7 years (range 0–15, IQR: 0, 9), with nearly 27% of women having received no formal schooling. About 29% of the women belonged to a marginalized caste (scheduled caste/scheduled tribe), and 64% lived in rural communities. About 46% of the women (n = 1,824) had given birth to a child by Wave 1 of the survey. Twenty-eight percent reported ever experiencing physical IPV and 35% reported ever facing sexual IPV by Wave 1 of the survey.
Sociodemographic Characteristics of Married AGYW by Ever Experience of Physical IPV and Sexual IPV (n = 3,965).
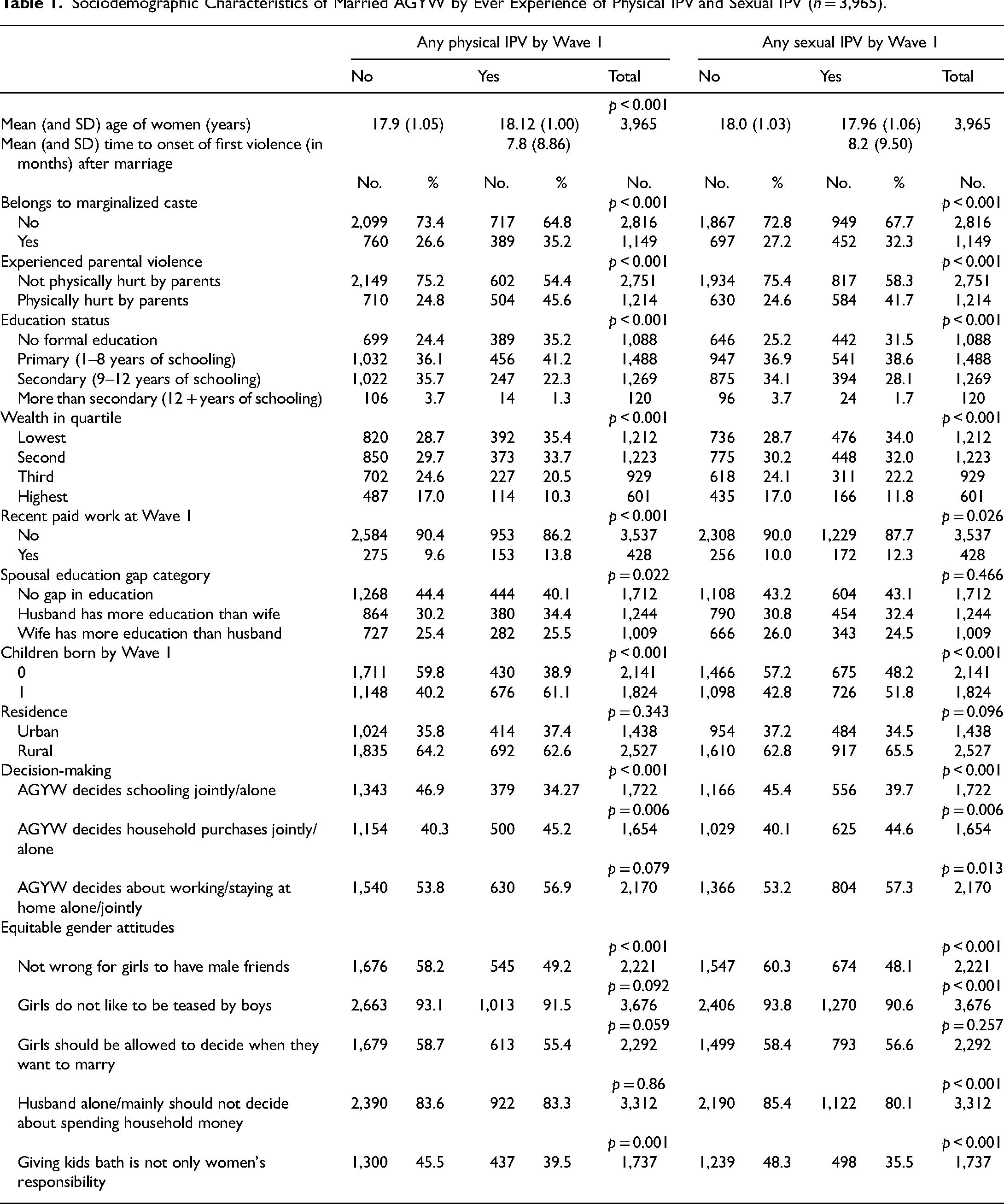
Bivariate analyses suggest that AGYW belonging to a marginalized caste, experiencing parental violence during childhood, participating in paid work in the 12 months prior to the survey, and those who had given birth were more likely to experience any IPV physical and/or sexual. We retained all the a priori control variables in our fully adjusted regression models. Table 2 summarizes the variation across communities in community-level collective gender norms variables at Wave 1 and Wave 2. We also found that mean community-level collective gender norm scores increased between Waves 1 and 2, indicating that communities became more equitable and progressive toward women over time.
Community-Level Collective Gender Norms Variables at Wave 1 and Wave 2.
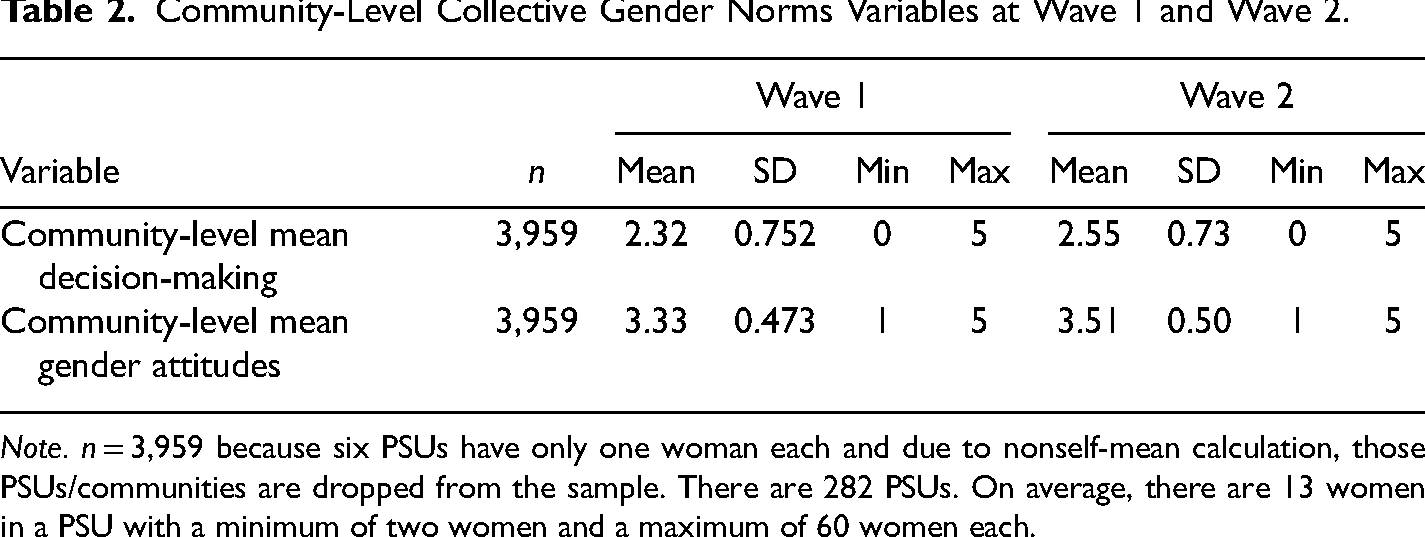
Note. n = 3,959 because six PSUs have only one woman each and due to nonself-mean calculation, those PSUs/communities are dropped from the sample. There are 282 PSUs. On average, there are 13 women in a PSU with a minimum of two women and a maximum of 60 women each.
At Wave 1, 28% of our analytic sample of AGYW ages 15–19 years had ever experienced physical violence, which increased to nearly 48% by the second wave (Figure 3). During the 12 months before Wave 1, 22% of women experienced violence “sometimes,” which increased to over a third in the second wave. For sexual IPV, 28% of the AGYW reported recent sexual IPV in the first wave, which marginally increased to 31% in the second wave.
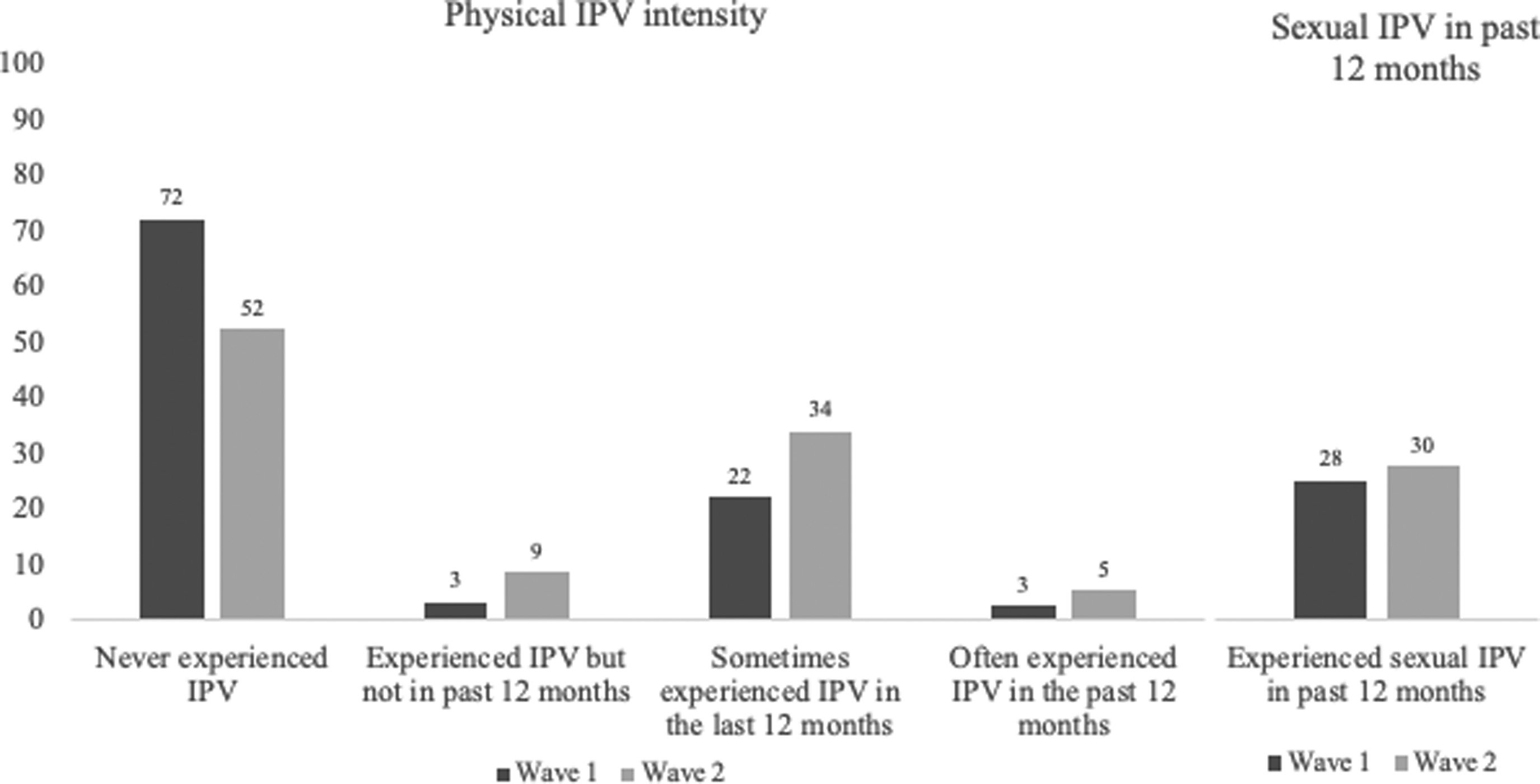
Physical IPV Intensity and Recent Sexual IPV by Each Wave.
We present results from mixed-effects ordinal logistic regression models for physical IPV intensity in Table 3. Model 3 had the lowest AIC and is therefore the final model. Controlling for individual, relational, community-level covariates, secular trends, and individual equitable gender attitudes, the estimated 26% (AOR 1.26, 95% CI: 1.10, 1.46) increase in odds of a woman experiencing “frequent” physical IPV per unit increase in community-level equitable gender attitudes on a 5-point scale. We did not observe a significant association between community-level decision-making power and physical IPV, controlling for the other variables. Table 8 in the Appendix section provides the complete set of results along with the control variables. Women's work outside the house was associated with greater odds of a woman experiencing “frequent” physical IPV (AOR 1.30, 95% CI: 1.07, 1.57). Additionally, wife having more education than the husband was also associated with a 33% increase in odds of a woman experiencing “frequent” physical IPV (AOR 1.33,95% CI: 1.13, 1.56). Pregnancy was also associated with significantly greater odds of a woman experiencing “frequent” physical IPV (AOR 2.12, 95% CI: 1.80, 2.49).
Proportional Odds Ratios and Robust 95% Confidence Intervals From Mixed-Effects Ordinal Logistic Regression Model for Physical Violence Intensity among Newly Married AGYW (n = 7,918).
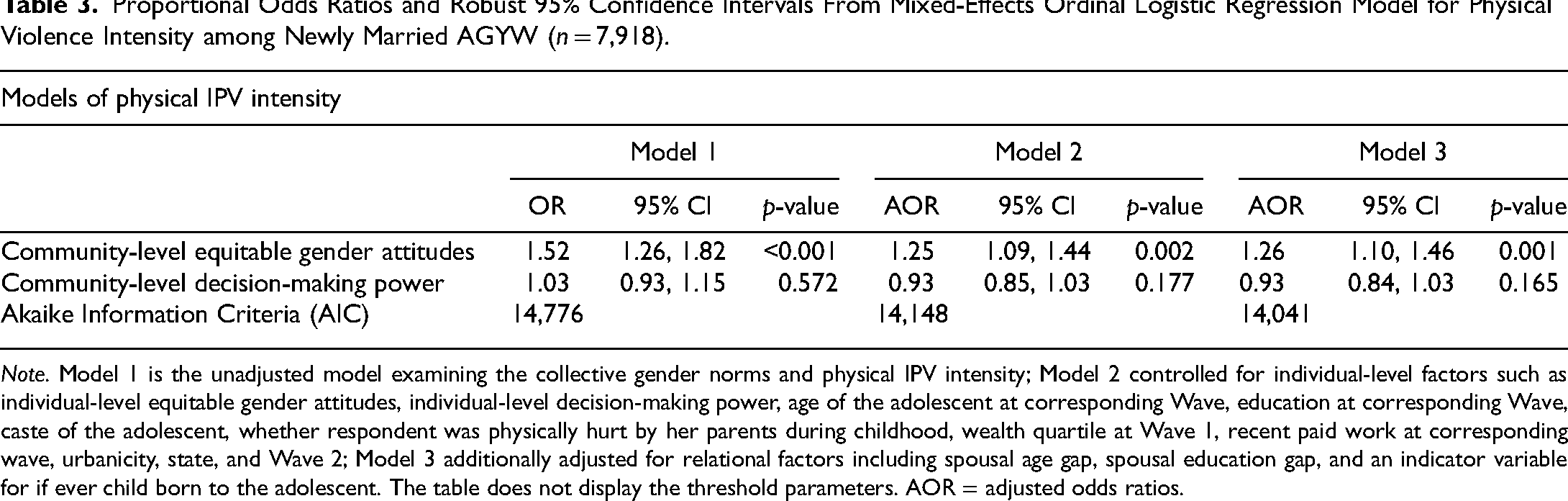
Note. Model 1 is the unadjusted model examining the collective gender norms and physical IPV intensity; Model 2 controlled for individual-level factors such as individual-level equitable gender attitudes, individual-level decision-making power, age of the adolescent at corresponding Wave, education at corresponding Wave, caste of the adolescent, whether respondent was physically hurt by her parents during childhood, wealth quartile at Wave 1, recent paid work at corresponding wave, urbanicity, state, and Wave 2; Model 3 additionally adjusted for relational factors including spousal age gap, spousal education gap, and an indicator variable for if ever child born to the adolescent. The table does not display the threshold parameters. AOR = adjusted odds ratios.
Table 4 presents results from our mixed-effects binary logistic regression for recent experience of sexual IPV. Model 1 estimates the unadjusted association between community-level collective gender norms and sexual IPV. Model 2 estimates the association between community-level collective gender norms and sexual IPV controlling for individual-level factors and secular trends. Model 3 adds the relational-level factors assumed to be confounding the association between community-level collective gender norms and sexual IPV. Based on the lowest AIC, we selected Model 2 as the final model. Controlling for individual-level covariates, secular trends, and community-level covariates, we did not find a significant association between community-level equitable gender attitudes and sexual IPV (AOR 1.00, 95% CI 0.85, 1.18) or community-level decision-making power and sexual IPV (AOR 1.03, 95% CI 0.92, 1.15) at the 5% level. Table 8 in the Appendix section displays the full set of results from the binary logistic regression examining the relationship between collective gender norms and sexual IPV.
Odds Ratios and Robust 95% Confidence Intervals from Mixed-Effects Binary Logistic Regression Model for Sexual IPV among Newly Married AGYW (n = 7,918).
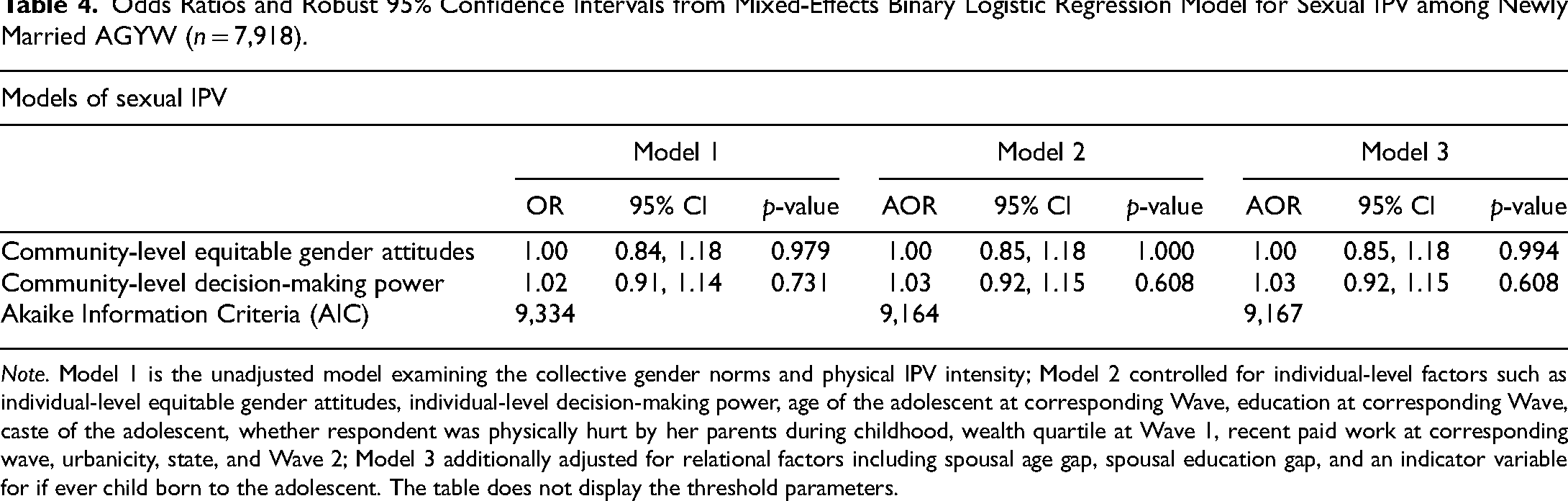
Note. Model 1 is the unadjusted model examining the collective gender norms and physical IPV intensity; Model 2 controlled for individual-level factors such as individual-level equitable gender attitudes, individual-level decision-making power, age of the adolescent at corresponding Wave, education at corresponding Wave, caste of the adolescent, whether respondent was physically hurt by her parents during childhood, wealth quartile at Wave 1, recent paid work at corresponding wave, urbanicity, state, and Wave 2; Model 3 additionally adjusted for relational factors including spousal age gap, spousal education gap, and an indicator variable for if ever child born to the adolescent. The table does not display the threshold parameters.
Interaction Analysis
In Tables 5 and 6 (in the Appendix section), we present the results from testing for interaction between community-level collective gender norms and time (indicator for Wave 2) controlling for all covariates interacted with time for frequent physical IPV and sexual IPV, respectively. The association between community-level decision-making and women's experience of frequent physical IPV increases over time (OR 1.17, 95% CI: 0.99, 1.39, p = 0.066). However, we did not find an association between community-level decision-making at Wave 2 and physical IPV intensity. We did not observe that the association between community-level equitable gender attitudes and physical IPV varied over time. We also did not find evidence that the association between collective gender norms and sexual IPV varied over time. As a sensitivity check, we fitted a binary logistic regression using the variable of recent physical IPV coded as a binary outcome (yes/no) and the results were not substantially different (Table 9 in Appendix section). Unlike the ordinal logistic regression, binary logistic regression does not assume proportional odds.
Association Between Collective Gender Norms and Physical IPV Intensity Moderated by Wave among Newly Married AGYW (n = 7,918).
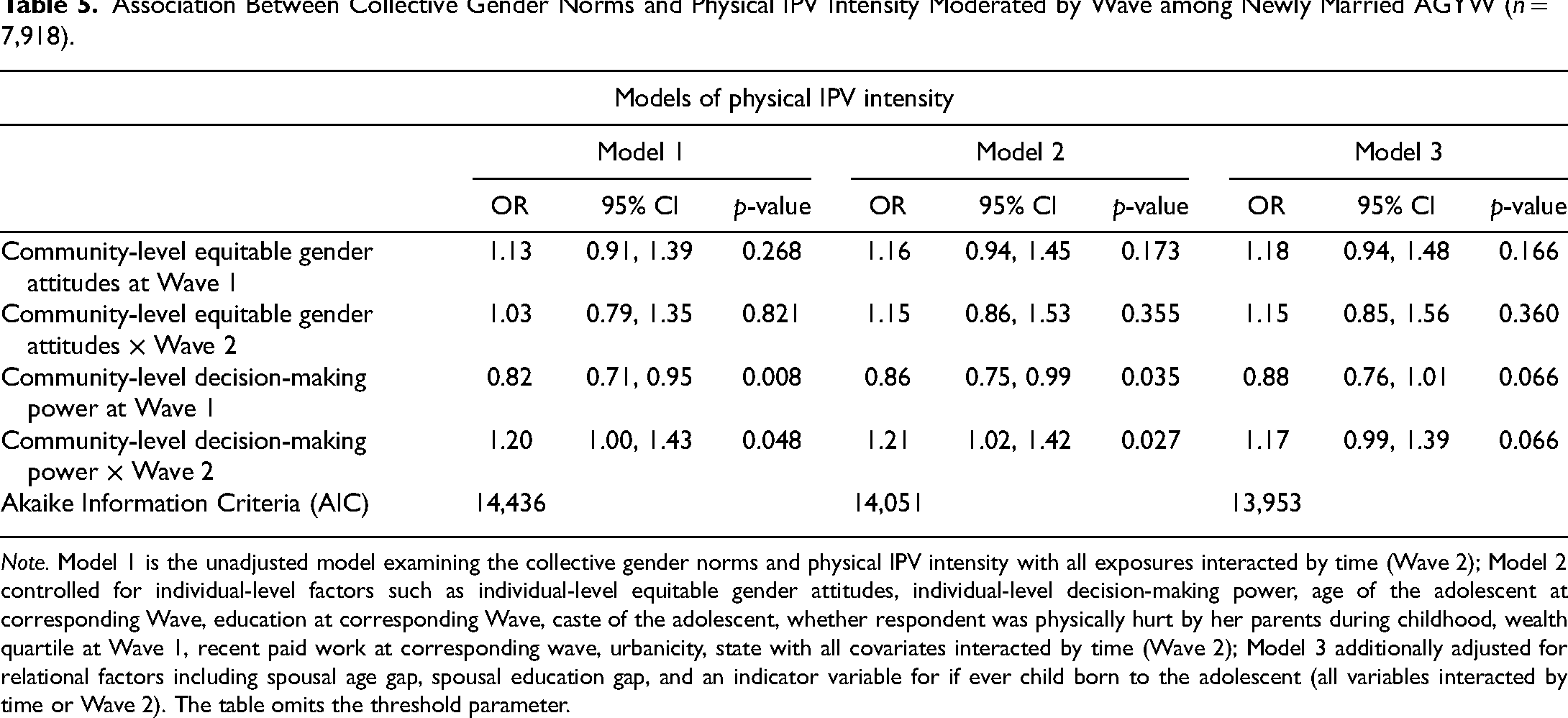
Note. Model 1 is the unadjusted model examining the collective gender norms and physical IPV intensity with all exposures interacted by time (Wave 2); Model 2 controlled for individual-level factors such as individual-level equitable gender attitudes, individual-level decision-making power, age of the adolescent at corresponding Wave, education at corresponding Wave, caste of the adolescent, whether respondent was physically hurt by her parents during childhood, wealth quartile at Wave 1, recent paid work at corresponding wave, urbanicity, state with all covariates interacted by time (Wave 2); Model 3 additionally adjusted for relational factors including spousal age gap, spousal education gap, and an indicator variable for if ever child born to the adolescent (all variables interacted by time or Wave 2). The table omits the threshold parameter.
Association Between Collective Gender Norms and Sexual IPV Moderated by Wave among Newly Married AGYW (n = 7,918).
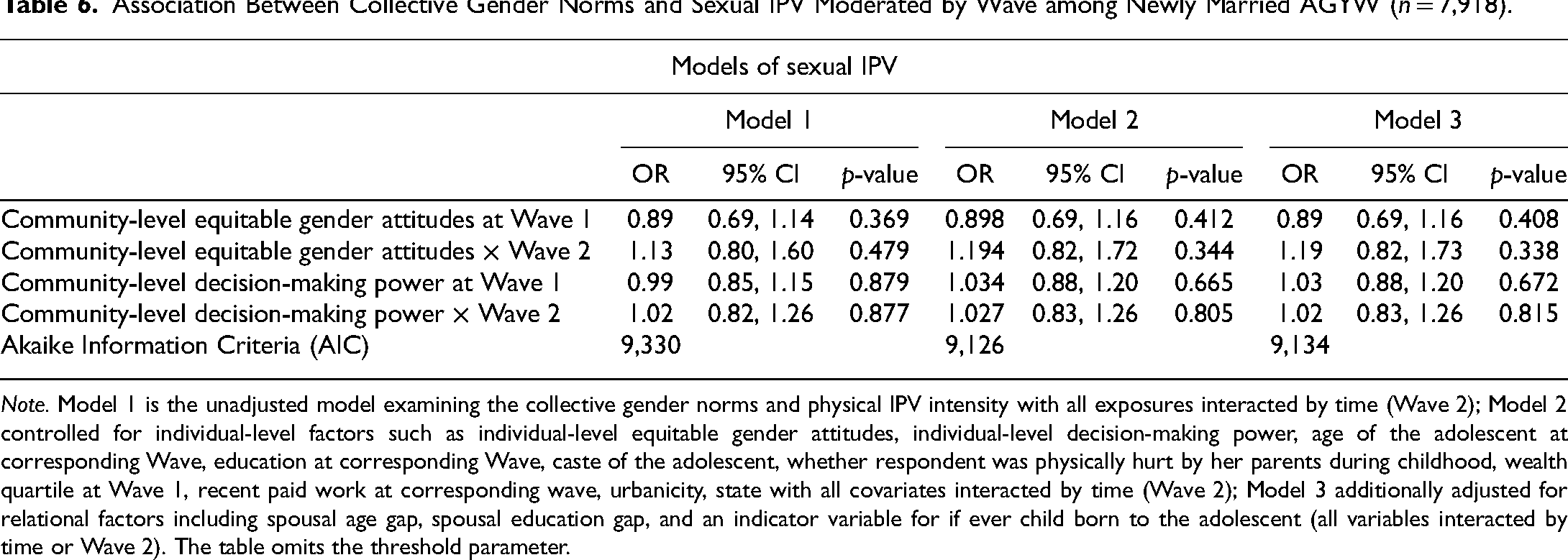
Note. Model 1 is the unadjusted model examining the collective gender norms and physical IPV intensity with all exposures interacted by time (Wave 2); Model 2 controlled for individual-level factors such as individual-level equitable gender attitudes, individual-level decision-making power, age of the adolescent at corresponding Wave, education at corresponding Wave, caste of the adolescent, whether respondent was physically hurt by her parents during childhood, wealth quartile at Wave 1, recent paid work at corresponding wave, urbanicity, state with all covariates interacted by time (Wave 2); Model 3 additionally adjusted for relational factors including spousal age gap, spousal education gap, and an indicator variable for if ever child born to the adolescent (all variables interacted by time or Wave 2). The table omits the threshold parameter.
Discussion
To our knowledge, this is the first study from India to use longitudinal data to examine the association of community-level collective gender norms with physical IPV intensity and sexual IPV experience among newly married AGYW. Using prospective cohort data of young married AGYW, we found that living in a community with more equitable gender attitudes was associated with incremental increases in odds of physical IPV intensity after controlling for individual and spousal factors, community-level covariates, and secular trends. Neither community-level gender attitudes nor community-level greater decision-making power of AGYW predicted sexual IPV. This means that the association between gender norms and IPV differs by type of IPV being examined.
Our result that the odds of greater intensity of physical IPV increases as community-level equitable gender norms increase contradicts our hypothesis and prior studies from India that have examined this relationship. Prior cross-sectional national research from India has found that women living in communities with inequitable gender norms (measured as greater proportion of men and women who justified wife beating) were more likely to experience physical IPV (Ahmad et al., 2021). Our results also deviated from another cross-sectional study in North India that showed that living in communities with inequitable gender norms (defined as men's attitudes toward wife beating) was associated with a higher risk of physical IPV (Koenig et al., 2006). Both these studies examined community-level gender norms using men's (or husbands’) attitudes toward IPV while we constructed collective gender norms variables with data only from married women because the husbands were not surveyed. Since the husbands are the perpetrators of violence, constructing the norms variables with husbands’ responses would have undoubtedly brought more nuance to our analyses. Further, our collective gender norms variables are not directly comparable to the standard attitudes toward wife-beating questions typically covered in Demographic Health Surveys. Future research should attempt to collect data from wives as well as their husbands to understand the community-level predictors of IPV.
Yet, plausible explanations for our findings exist. It is possible that women living in communities reporting more equitable gender attitudes feel more comfortable reporting violence. Particularly, with our observation that there was an improvement in gender-equitable attitudes from Wave 1 to Wave 2, there is a possibility that women are now more empowered to seek help or terminate a relationship as a response to the violence they have experienced. However, it is important to acknowledge that the sample included in Wave 2 was limited to women who were still married, which introduces the potential for bias and may lead to an overestimation of the prevalence of IPV (although only 35 women were separated and divorced between Wave 1 and 2). Or, perhaps women are less accepting of violence and thus more willing to acknowledge violence happening to them. We also observed an increase in women's participation in paid work from Wave 1 to Wave 2 and multivariable models showed that women's participation in paid work was associated with increased odds of experiencing physical IPV, consistent with prior studies from India (Pallikadavath & Bradley, 2019). The odds of women experiencing frequent physical IPV were more than two times greater for women who had experienced childbirth, consistent with a study from South Asia (Nepal) that also analyzed data from recently married women. (Raifman et al., 2021)Another possible reason for this result could be explained using the Gender Power Relation Theory (Radtke & Stam, 1994) and Backlash Theory (Mansbridge & Shames, 2008). Any change in gender power relations that threatens the status quo of men's control over economic and household resources can lead to resistance (backlash) to this change. This change can result in increased violence against women in the community (Guarnieri & Rainer, 2018; Macmillan & Gartner, 1999; Mansbridge & Shames, 2008). Evidence from South Asia suggests that women's economic empowerment is associated with an increase in IPV (Amaral et al., 2015; Chishti, 2010; Rahman et al., 2011). Changes in a normative environment favoring women can disturb power relations between genders; this can sometimes have unforeseen effects, such as men resorting to violence, especially within the relational (family) sphere, to exert their dominance and masculinity (Macmillan & Gartner, 1999).
Our results do not show a statistically significant association between women's decision-making power at the community-level and physical IPV intensity. Only one study from India that focused on married women in the slums found that women's empowerment measured at the individual level using decision-making power was protective of IPV (Donta et al., 2016). The scale used in our study was different and may not have exactly captured the range of decisions young women are in involved in. Future studies, especially qualitative work can help us understand these associations better.
The association between collective gender norms does not hold for sexual IPV in the multiple regression models controlling for secular trends and individual and relational-level factors—suggesting that the associations between the gender norms used in our study and IPV differ by the type of IPV. This finding is consistent with previous research from India that did not find a positive association between community-level inequitable gender attitudes toward wife beating and sexual IPV (Ahmad et al., 2021; Koenig et al., 2006). Our study found that women's paid work outside the house and wife having more education than husband were associated with greater odds of sexual IPV.
Gender-based violence is a manifestation of factors at different socioecological levels, and we examined gender-based violence using an ecological framework (Heise, 1998). We extended the literature on IPV and gender norms by assessing longitudinal associations between collective gender norms and physical and sexual IPV in two of the most underresourced and patriarchal settings in the Indian context, where IPV remains a pervasive public health challenge, especially among young newly married women.
This study has several strengths. First, we used a large sample of newly married young women, a population that has been relatively less researched for IPV. Second, instead of using a dichotomous physical IPV variable, we used an ordinal variable to define women's experience of physical violence intensity using four categories—never experiencing violence, not experiencing physical IPV in the 12 months preceding the survey, sometimes experiencing physical IPV in the 12 months preceding the survey and experiencing physical IPV often in the 12 months preceding the survey. Third, we used a longitudinal, prospective cohort of AGYW and communities that were followed over a three-year timeframe. Fourth, ours is one of the few studies that has examined physical and sexual IPV separately to get a more nuanced understanding of how gender norms are associated with each type of IPV.
The study has limitations worth noting. A major limitation was that the data including the community-level gender norms variables were based on only the wives and not the husbands who often are perpetrators of IPV. Constructing gender-equitable attitudes and decision-making measures using the data from the husbands/men who perpetrate IPV would have likely allowed us to construct a richer community norm variable. There is a possibility that community-level collective gender norms constructed using only married AGYW's perceived attitudes and stated behaviors do not reflect the community's underlying patriarchal and restrictive gender norms. Community-level gender norms variable was constructed only from young women (15–24 years) and not perhaps, representative of attitudes held by all women (e.g., 15–49 years) living in the community. Further, the dataset also lacked scales that have been traditionally used in IPV literature such as the gender equitable men (GEM) scale (Pulerwitz & Barker, 2008) and attitudes toward wife-beating scale (International Institute for Population Sciences, 2017). Sexual IPV was measured using a single question asking whether the respondent was forced to have sex within the 12 months before the survey. This question was not detailed enough to capture the range of sexual IPV experiences that AGYW may have faced. While our focus on newly married women (15–22 years) was a strength, questions on IPV and norms could have been sensitive for adolescents, perhaps limiting their honest responses. Further, the study was conducted in two neighboring northern states in India that have similar socio-cultural contexts. This could have limited the heterogeneity of community-level gender norms within the sample, reducing the statistical power to understand the relationship between collective gender norms and IPV. Future longitudinal studies should collect data from more diverse socio-cultural contexts and from other community members including husbands and male members to study how restrictive gender norms predict IPV.
Policy Implications
The results of this study point to future areas for investigation, particularly to disentangle pathways between different norms measures and types of IPV. Despite two decades of research on IPV, studying contextual risk factors that predict IPV remains challenging since IPV is a product of its social context. The endogeneity in the gender system makes it a complex topic to discern the impact of gender norms on IPV. The development of consistent scales and rigorous studies to understand contextual-level factors is a precursor to better understanding the interrelationships between community-level factors and all forms of gender-based discrimination and violence.
Few studies on gender norms have surveyed men and husbands in the community to measure norms. Some have used the GEM scale, which captures men's attitudes toward gendered practices, including sexual and reproductive health, sexual relations, violence, domestic work, and homophobia (Pulerwitz & Barker, 2008). This scale has been used in Sub-Saharan Africa to study IPV (Fine et al., 2021; Gottert et al., 2018; Peitzmeier et al., 2016). One study in Nepal validated and used the partner violence norms scale (Clark et al., 2018) to examine the association between gender norms and IPV. Most studies examining IPV using demographic health surveys have created social norms measured by using an additive score of attitudes toward wife beating. The scale measures the acceptability of IPV using five questions regarding the conditions under which hitting or beating one's wife would be justifiable (wife going out without telling him, neglecting the children, arguing with him, refusing to have sex with him, and burning the food).
Despite the availability of these measures, measurement of gender norms remains challenging for several reasons. First, to our knowledge, there is no consensus-based scale for measuring gender norms; no standard exists for quantitatively measuring beliefs and attitudes across cultures and over time (Vaitla, 2018). Rigorous quantitative data and measures are needed to estimate the influence of gender norms on health inequities but efforts to collect such data are at a nascent stage (Weber et al., 2019). Second, the current measures only capture individual attitudes and perspectives on community norms without directly measuring what the target population believes are norms within the community (what others do). To accurately measure norms, it is necessary to precisely conceptualize norms and differentiate them from other social constructs like personal attitudes, intentions, and beliefs.
Measurement of social and gender norms in public health research often relies on asking questions about behaviors and attitudes, which acts as substitutes for descriptive and injunctive norms (Cislaghi & Heise, 2018). Identifying this distinction is crucial to associate attitudes to specific health outcomes (Bingenheimer, 2019; Cislaghi & Heise, 2018). With the exception of a few studies such as the global early adolescence study that captured descriptive and injunctive gender norms around intimate relationships, to our knowledge, most others do not incorporate the key theoretical constructs of social norms theory (the descriptive and injunctive norms) that have been shown to influence health behaviors (Moreau et al., 2019; Trivedi et al., 2017). This limited focus on measurement could be because norms were considered too difficult to change and have been ignored in mainstream public health and global development discourse until the past two decades or so. More extensive studies on validated measures that capture descriptive and injunctive norms from both women and their husbands would make significant contributions to the literature. Further, we need longitudinal studies with multiple follow-up time points supplemented with qualitative studies. The latter should attempt to capture changing norms at the household-level from the husband-wife dyad to understand IPV from a life-course perspective.
Conclusion
Our study highlights the high prevalence of physical and sexual IPV among newly married women in Uttar Pradesh and Bihar and increases over time. We also found that the relationship between collective gender norms and IPV is different by type of IPV. More studies and validated scales to measure what the younger adult women and men believe are norms within the community (what others do) could help elucidate the relationship between gender norms and IPV. Married AGYW are a vulnerable group who face high IPV early in their marriage. While improving scales and measures may take time, interventions should continue to focus on testing interdisciplinary approaches to reduce IPV, and potentially even eliminate them.
Supplemental Material
sj-docx-1-vaw-10.1177_10778012231208999 - Supplemental material for The Role of Gender Norms on Intimate Partner Violence Among Newly Married Adolescent Girls and Young Women in India: A Longitudinal Multilevel Analysis
Supplemental material, sj-docx-1-vaw-10.1177_10778012231208999 for The Role of Gender Norms on Intimate Partner Violence Among Newly Married Adolescent Girls and Young Women in India: A Longitudinal Multilevel Analysis by Lakshmi Gopalakrishnan, Stefano Bertozzi, Patrick Bradshaw, Julianna Deardorff, Holly (Shakya) Baker and Sophia Rabe-Hesketh in Violence Against Women
Footnotes
Acknowledgements
We thank the Population Council for collecting this data and making it available in the public domain freely for scholarly and research use.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.