
Abstract
Gender-based violence (GBV) is a prevalent global problem that mostly affects females, with a significant impact on exacerbating parenting stress, affecting child upbringing, and their potential engagement in antisocial behaviours. Yet, there is limited intervention addressing this significant problem in Nigeria. Informed by the unique fusion of intersectionality and social learning theories, we make an original and significant contribution by testing a novel Problem Management plus Mindfulness informed Legal Education (PM + MiLE) to understand its feasibility in reducing stress in parenting and awareness of access to legal support channels for women with lived experiences of GBV and with child caring responsibilities in Delta state, Nigeria. We test this intervention using a randomised controlled trial with 24 participants with lived experiences of GBV who were randomly assigned to either the experimental group (PM + MiLE) or a waitlist control group. We found that respondents in the experimental group demonstrated reduced stress in parenting and awareness of legal support channels, including access to justice, compared to the control group. For the control group, the intersectional role of poor economic support, trauma from GBV, coupled with the patriarchal nature of society and culture, was still emphasised as a significant barrier to effective parenting. Insights gained from this case study have significant policy implications. The insights are also relevant and represent an important step in advancing our understanding of interventions for parental stress reduction and access to justice in other countries with a similar prevalence of GBV against women.
Introduction
Gender-based violence (GBV) is a prevalent problem globally. Data from the World Health Organisation (2024) suggest that globally, an estimated one in three (30%) of women in their lifetime have been subjected to either sexual or physical violence by their intimate partner or non-partner. In Nigeria, an estimated one in three women has experienced some form of physical GBV (Aborisade, 2024). Research has shown that violence against women can significantly affect women’s physical, sexual, and mental health, with a significant impact on those with child-caring responsibilities (Geprägs et al., 2023; Ike, Jidong & Ayobi 2023; Ike, Jidong & Ayobi et al., 2025). Such impact could further exacerbate stress in parenting and lead to significant adverse child outcomes, low educational attainment, antisocial behaviour and, in its extreme, offending (Geprägs et al., 2023; Ike et al., 2022). Yet, a gap remains in the use of psychosocial intervention to address the intersection between GBV, poor awareness of legal channels of support, and stress in parenting informed by the combined fusion of intersectionality and social learning theory.
Previous literature on GBV, both globally and nationally, has tended to focus on the causes of GBV and attributed factors such as gender stereotypes (Mulvihill & Wicky, 2024), normative expectations of femininity, prejudice, culture (Baldwin-White et al., 2023; Ike, Jidong, Ike et al., 2025), and patriarchy (Turbett, 2024) as significant contributors to GBV. Others have argued that conflict-induced displacement (Abimbola, 2024) and the pandemic (Canwat, 2024) are significant contributory factors to GBV. In Nigeria, previous literature stresses the significance of factors such as gender norms and practices, underscoring the superiority of male subjects’ patriarchal beliefs over female subjects, including traditional and religious beliefs as major contributory factors to the prevalence of GBV (Ojo et al., 2023). Concerning interventions, others have explored interventions such as tertiary institutions in addressing GBV (Ogunode et al., 2024), religious intervention (Efuntade, 2023), cognitive behaviour therapy (Mengistu, 2019), skills training for female subjects’ apprenticeship affected by GBV, and sensitisation training for apprentice instructors (Fawole et al., 2005). While this literature is valuable, there remains a gap in interventions to address stress in parenting and improve awareness of legal mechanisms of help-seeking for GBV. Thus, highlighting the urgent need for intervention to address the gap in poor help-seeking, awareness of legal support channels, and parental-related stress due to experiencing GBV.
Problem Statement (Literature Gaps) – Purpose and Research Question
Despite the growing body of literature that has identified the harmful effects of GBV in exacerbating parenting stress and harsh parenting, more studies are necessary to identify interventions that can help address the severe impact of GBV on affected victims, awareness of support channels, whilst improving parenting (Ike, Jidong and Ayobi 2023, Ike, Jidong and Ayobi et al., 2025). The literature on the intersection between GBV and parenting has primarily focused on gender transformative programmes in humanitarian settings (Meinhart et al., 2024), men’s involvement in parenting programmes to reduce GBV and child maltreatment (Handayani et al., 2024; Siu, 2017). Others have explored emotion-focused intervention (McWhirter, 2011), the Domestic Abuse Recovery Together intervention (Smith et al., 2015), and family intervention to improve occupational performance (Waldman-Lev & Weintraub, 2015).
While previous studies have also emphasised the prevalence of GBV among women with parenting responsibilities, they have, however, not tested an intervention that addresses the intersectional barriers women face in parenting as a result of GBV, legal avenues for help-seeking, including mechanisms to reduce parental stress and harsh parenting (Gurung & Acharya, 2016; Ubom et al., 2025; Uwumuremyi et al., 2025). This is especially true in countries like Nigeria, where gendered norms, patriarchy, and poor awareness of channels for support exacerbate affected women’s conditions and parental stress – by extension, leading to poor child outcomes (Ike, Jidong & Ayobi 2023).
Our study extends prior research and makes an original and significant contribution to addressing the gap by testing a unique intervention, composed of Problem Management plus Mindfulness-Informed Legal Education (PM + MiLE), in addressing parental stress and awareness of legal support mechanisms. The PM + MiLE is a low-intensity intervention that addresses parental stress resulting from GBV experience and awareness of legal channels for accountability, utilising relevant aspects of brief mindfulness, legal education, human rights awareness, and the challenges of complaint, including support. The problem management ambit addressed adversity, stress, and problem management while strengthening social support and encouraging positive behaviour modification. Underpinned by the combined fusion of intersectionality and social learning theory, our study also makes an original contribution by examining how participants perceived their experiences of GBV and stress in parenting prior to and after the intervention. The combined theoretical lens also offers unique insight into understanding how participants make sense of and, in turn, comment on their experiences of the intervention. This is as theoretically, research on GBV has tended to focus on feminist theory (Guizzo & Alldred, 2024), domestic violence theory (Merrill, 2014), and intersectionality theory (Humbert et al., 2024). Others have focused on structuration theory (Okafor et al., 2024). Yet, there is also a significant gap in the unique fusion of intersectionality theory and social learning theory in understanding this problem.
Crenshaw’s (1989) intersectionality theory offers a useful lens as it seeks to understand how the interlocking systems of power could affect those subjected to marginalisation in society. As such, intersectionality theory could help understand how the combination of individuals’ political and social identities could result in undue privilege and discrimination. Such intersection and overlap of social identities, including factors such as gender, ethnicity, religion, culture, and class, may be empowering or, in its extreme, lead to oppression. Intersectionality thus offers a unique theoretical lens to understand how the intersection of factors such as culture, feminism, patriarchy, and religion could impact women’s experiences of GBV, the stress in parenting, and their help-seeking behaviour. In addition, social learning theory could also be used to understand the significant impact of stress in parenting on children, as it relates to poor school attainment, trauma, and resort to antisocial behaviour, given their learnt and observed exposure to violence and harsh parenting. As Bandura’s (1977) social learning theory posits, people learn or acquire new behaviour through the observation and imitation of others, which is further intensified by environmental and behavioural influences and the interactions among these significant factors. The family is the first area of socialisation, and children exposed to GBV and harsh parenting due to the stress experienced by their primary caregivers (who are mostly female subjects) are more likely to suffer significant impact and poor school attainment as a result. Based on a social learning theoretical perspective, such children are at higher risk of increased mental health problems and engaging in violent behaviour as a result of observing GBV. Thus, highlighting the significance of integrating the theory in informing the specifics of PM + MiLE intervention to address the intersection between GBV, stress in parenting, and legal awareness of support channels.
It is against the preceding backdrop that the study seeks to address the following research questions:
What is the feasibility and acceptability in terms of recruitment, retention, adherence to the PM + MiLE intervention, and affected victims’ satisfaction with the intervention compared to a waitlist control group?
What is the preliminary efficacy of PM + MiLE compared to a waitlist control group in reducing affected victims’ parenting stress, resorting to harsh parenting, and improving parenting style, alongside awareness of legal channels of accountability and social support?
The primary objectives of the study are as follows:
To determine PM + MiLE’s intervention in comparison to the waitlist group’s feasibility and acceptability in terms of recruitment, retention, adherence to the intervention, and affected victims’ satisfaction with the intervention.
The secondary objectives are as follows:
To determine the preliminary efficacy of PM + MiLE compared to the waitlist group in reducing affected victims of GBV parenting stress, resort to harsh parenting, and improving awareness of legal channels of accountability and social support.
For this study, acceptability refers to acceptable levels of recruitment, retention, and adherence, which is determined by the following criteria: (a) Retention rate: Green: ≥75% of randomised participants retained by the end of the intervention; Amber: 65%–75% retained; Red: <60% retained. (b) Recruitment rate: Green: ≥80% of the target recruited. Amber 50–<80% of target recruited. Red<50% of the target recruited. (c) Adherence to PM + MiLE intervention: The percentage of participants receiving a minimum sessions of PM + MiLE (≥4 sessions) within the intervention window. Green: ≥65% adherent. Amber: 40%–64% adherent. Red: ≤39% adherent. For the recruitment target, we envisaged recruiting between 10 and 12 participants per arm as the benchmark to pilot the study. The rationale for the chosen number is based on its appropriateness for a pilot study, as reported in previous studies (Ike et al., 2024; Julious, 2005).
To address the study’s research questions, we began with a note on the methodology adopted. An in-depth analysis and report of the findings from the quantitative and qualitative datasets follows this. The findings are discussed in the context of the existing literature, and conclusions are presented alongside recommendations for addressing GBV.
Methodology
Study Design
The study is a two-arm, randomised, controlled feasibility trial. Participants were randomly allocated to either the intervention group, which received the PM + MiLE intervention, or the control group, which was placed on a waitlist to subsequently receive the PM + intervention after completing outcome assessments at baseline and the end of the intervention. The study employed a mixed-methods approach to data collection. Semi-structured interviews were conducted to gain an understanding of participants’ experiences before and after the intervention.
Ethics
Prior to the commencement of the study, and in line with global best practices, ethics approval was sought from and approved by the Jos University Teaching Hospital in Nigeria with research ethics number [JUTH/DCS/IREC/127/XXXI/2746]. The study was also duly registered on clinicaltrial.gov with a trial identification number [NCT06601023]. All participants were duly briefed on the study’s purposes and were informed of their right to withdraw. They were also informed about how their data will be used. Participants voluntarily participated in the study and signed the consent form electronically prior to their participation.
Inclusion and Exclusion Criteria
The study’s inclusion criteria were that participants must be 18 years and above, female subjects with child(ren) or with caring responsibilities for children, able to provide full consent for their participation, and residents of the study area, which is Delta state and its environs. The reason for residents to be based at the trial catchment is to enable effective follow-up and minimise the loss of participants due to unavailability. The participants were also required to speak and understand English, Nigeria’s official language. The study exclusion criteria were that participants would be excluded if they were under 18 years old, unable to consent, undergoing severe mental health treatment, or unable to speak or understand the English language. Participants were also excluded if they were not based in the trial catchment area or were unlikely to be available for follow-up.
Participant Recruitment and Demographics
A purposive sampling technique was harnessed to recruit participants who met the study’s inclusion criteria. We also leveraged support from civil societies, non-governmental organisations, and faith-based organisations to recruit participants. A snowball sampling technique was also adopted, and some participants were able to refer others sharing similar experiences. They were then briefed on the study’s purposes before deciding voluntarily to participate in the study. The research team comprised a legal practitioner and barrister, clinical psychologists, health workers, and research assistants. In total, 24 participants were recruited for the study, as previous literature suggests its appropriateness for conducting pilot or feasibility trials (Julious, 2005). The 24 participants were randomised to either the experimental group (n = 12) or the waitlist control group (n = 12). The participants’ age ranges between 25 and 45. The participants were recruited from Delta and Plateau states; however, their state of origin varied and included Edo, Delta, Plateau, Rivers, Anambra, Enugu, and Bayelsa states.
In terms of the demographic breakdown across the experimental and control groups, in the experimental group, the level of education was as follows: one participant indicated that she had attained a primary level of education, four reported having obtained only secondary education, and the remaining seven indicated that they had attained tertiary education. Regarding the control group, four participants indicated that they had attained a secondary level of education, seven had obtained only tertiary education, and the remaining one indicated that she had attained primary education. For the level of employment, eight indicated being employed in the experimental group, while the other four were unemployed. For the control group, nine were employed, while the other three were unemployed. For the control group, nine were employed, while the other three were unemployed.
Randomisation
To aid randomisation, Microsoft Excel was used to randomise participants who met the inclusion criteria into either the experimental group (PM + MiLE) or the waitlist control group. Based on the eligible participants’ list, a random value of 0 or 1 was generated using the RANDBETWEEN function in Excel, thereby choosing 0 and 1 as the range. All participants with a value of 0 were assigned to the experimental group, and all participants with a value of 1 were assigned to the control group. The method of randomisation used enabled a single sequence of random assignments, allowing participants to be assigned to either the experimental or control group based on a 1:1 ratio (Kim & Shin, 2014). All participants had equal chances of receiving either the PM + MiLE or the Waitlist control group intervention. All participants were blinded to whether they were allocated to experimental (PM + MiLE) or waitlist-control groups. Due to the study’s pilot nature, it was impossible to blind the facilitators delivering the intervention.
Intervention: PM + MiLE for Experimental Group
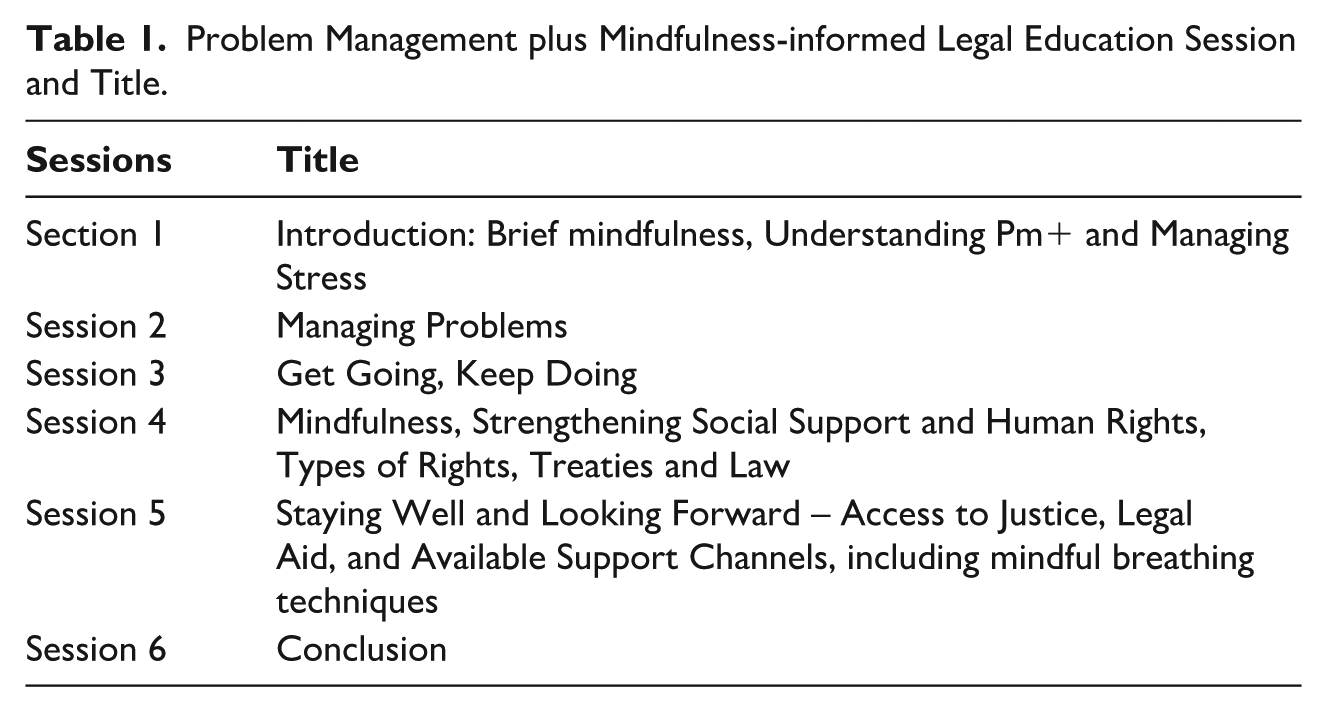
The PM + MiLE is a low-intensity intervention comprising six sessions, each lasting approximately 90 min and delivered once a week. The session covered relevant aspects of brief mindfulness, legal education, human rights awareness, and the channels of complaint, including support. The problem management ambit encompasses understanding adversity, managing stress, addressing problems, getting started and maintaining momentum, strengthening social support, staying well and looking forward, and promoting positive behaviour modification. The intervention also incorporated child development and building positive parenting interactions with children. For this intervention, we adopted the United Nations Convention on the Rights of the Child, which defines a child as anyone under 18 years of age. We also adopted the Nigerian legislation, the Child Rights Act 2003, which defines a child as a person under 18 years of age. Table 1 indicates the topics covered during the 6-week sessions.
Problem Management plus Mindfulness-informed Legal Education Session and Title.
Prior to the delivery of the intervention, a multilayer approach to adaptation was adopted. First, our previous empirical studies on GBV in Nigeria highlighted the challenges faced by affected victims, such as poor support, mental health difficulties such as depression, anxiety and trauma, including poor legal awareness and the gaps in intervention addressing the problem (Ike, Jidong & Ayobi, 2023; Ike, Jidong, Ike etal., 2025). The intervention was also informed by a public engagement conducted with women with lived experience of GBV, where the need for intervention addressing the interconnected link between GBV, parenting stress, and its impact on children was noted. We engaged with a cultural adaptation of the manual content with stakeholders (women with lived experiences), which helped shape the manual content, including incorporating culturally appropriate examples. The intervention was delivered online using Microsoft Teams.
Control Group
The control group was placed on a waitlist and provided with contact details of practising clinical psychologists and available support channels. Prior to their participation, the participants on the waitlist were also informed that after the intervention and subsequent follow-up, they would be administered the PM + MiLE intervention. The information was provided at the time of recruitment via the Participant information sheet, which described the study design (e.g. a randomised controlled trial with assignment to either an experimental group or a waitlist control group). However, after recruitment and completion of the consent form, participants were blinded to whether they were allocated to the experimental or waitlist group.
Study 1: Quantitative Study
Outcome Measures and Instruments for Data Collection
Primary Outcome Measures
The study’s primary objectives are to determine the feasibility and acceptability of PM + MiLE compared to the waitlist group, in terms of recruitment, retention, adherence to the intervention, and satisfaction with the intervention among affected victims. To assess feasibility, we used data on recruitment and the number of people willing to participate in the study. See Figure 1 of the Consort Flow diagram. Data on attendance and dropout were used to assess the acceptability of the intervention and participants’ retention, including adherence throughout the intervention, including follow-up, as shown in the Figure 1 flow diagram. Participants’ overall satisfaction with the intervention was assessed using the Service Satisfaction Scale (Ike, Jidong, Ayobi & Francis, 2023).
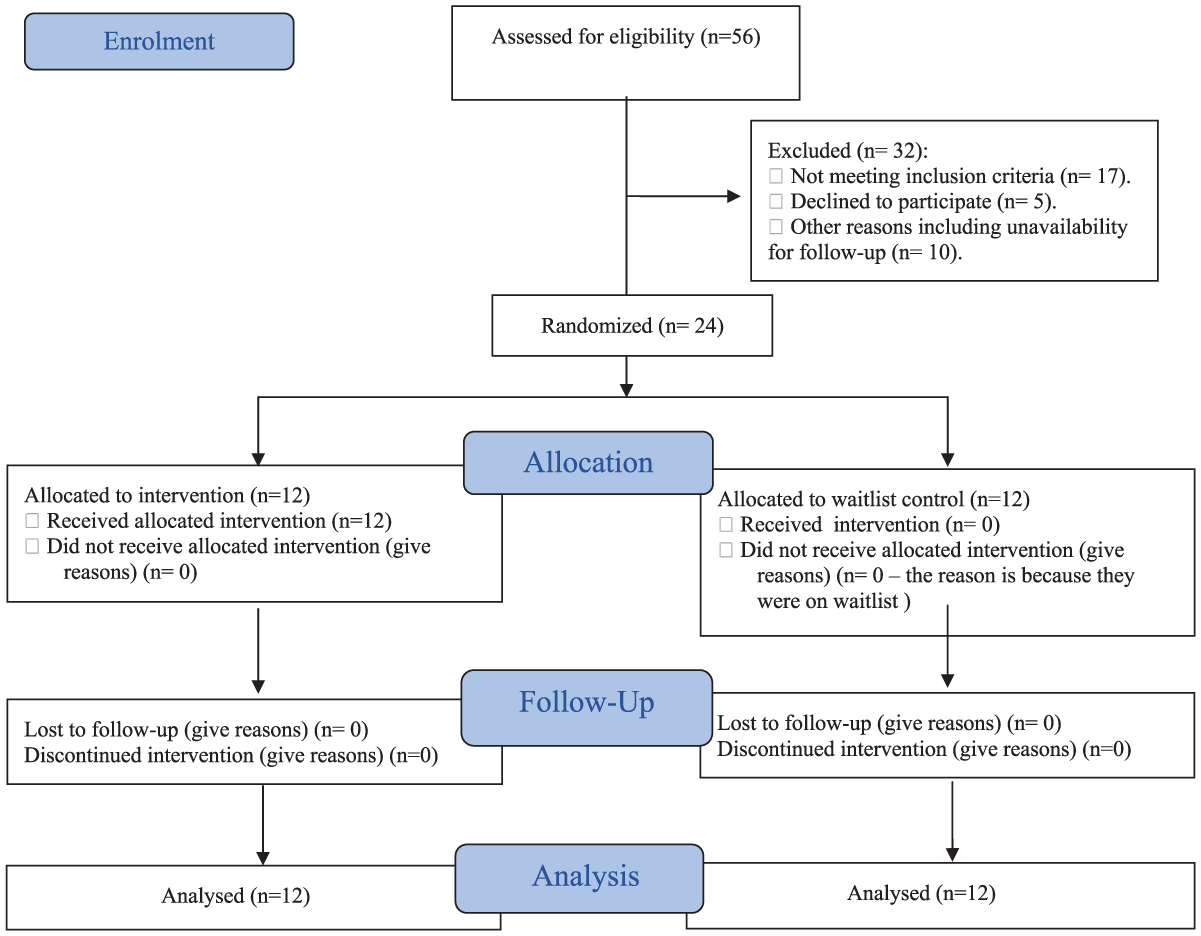
Consort 2010 flow diagram.
Secondary Outcome
The secondary outcome measure is to determine the preliminary efficacy of PM + MiLE compared to the waitlist control group in reducing affected victims of GBV resorting to harsh parenting, including parenting stress, and improving awareness of legal channels of accountability following experiences of GBV, and improving quality of life and social support. The parenting outcome related to stress and harsh parenting was assessed using the modified Harsh Parenting Scale (HPS) (Wang, 2017) and the gender-based Violence, Stress, and Parenting Scale (GBVSP). The HPS is a 4-item scale that measures harsh parenting behaviours, such as beating, yelling, or punishing children, while the GBVSP scale is a four-item scale measuring GBV and parental stress. Awareness of legal channels of accountability was assessed using the culturally adapted Legal-Informed Awareness of Complaint Channel Scale (LACCS) (Ike et al., 2024). The LACCS is a 10-item scale that measures the level of legal awareness and has a Cronbach’s alpha of α = .821. Social support improvement was assessed using the Oslo Social Support Scale (OSSS) (Kocalevent et al., 2018). The OSSS is a 3-item scale that measures the number of available social supports, the ease of obtaining practical help, and the interest or concern shown by others (Kocalevent et al., 2018). The OSSS has a Cronbach’s alpha of α = .640 (Kocalevent et al., 2018). For the quantitative data, all 24 participants (comprising those in the experimental and control groups) completed the surveys at both the baseline and the end of the intervention.
Quantitative Data Analysis
Quantitative statistical analysis was conducted using the independent sample t-test to examine the differences between the PM + MiLE intervention and the waitlist control group. The rationale for using the t-test is that our sample met the assumptions, including a normal distribution, homogeneity of variances, and two independent groups. The data scale of measurement is continuous.
Study 2: Qualitative Study
Qualitative Data Collection
Semi-structured interviews were also conducted with the participants to explore their lived experiences of engaging in the intervention and their overall thoughts about the programme. More specifically, participants were asked about their experiences of GBV, parenting, support, etc., prior to participating in the intervention, as well as their experiences with the intervention itself. See Supplemental Appendix 5 containing the interview schedule guide. Interview participants were randomly chosen to partake in the interviews using the same technique adopted for randomisation. A total of 14 interviews were conducted, comprising seven interviews in the experimental group and seven in the control group. The interviews were stopped following data saturation and the non-emergence of new data.
Qualitative Data Analysis
The qualitative data were analysed using thematic analysis, underpinned by the unique fusion of intersectionality and social learning theoretical lenses. The semi-structured interviews were recorded and transcribed verbatim. Informed by Clarke and Braun’s (2017) six-step approach to thematic analysis, we first engage in reading the transcript to ensure familiarisation with the dataset. This was followed by the second step, which involved in-depth coding of the full data to identify units of meaning. Three researchers conducted in-depth coding. The three researchers reviewed the codes against the dataset to ensure they reflected the key messages contained in the extracts. The coding process also demonstrated high reliability due to the consistency in coding among the three researchers who participated in the process. In the third stage, the codes were merged to generate themes by identifying recurrent patterns that appeared repeatedly in the coded dataset. In the fourth stage, the themes were reviewed by three researchers. The fifth stage involved defining and naming themes before finally engaging in the writing up of the findings in the sixth stage (Clarke & Braun, 2017).
Study 1: Quantitative Study Result
Figure 1 above under the primary outcomes measures shows participants’ recruitment and flow through the study, as well as the feasibility of the study in terms of recruitment. As shown in figure 1, the recruitment of participants for the intervention was feasible as we were able to reach our recruitment target in line with the inclusion criteria adopted.
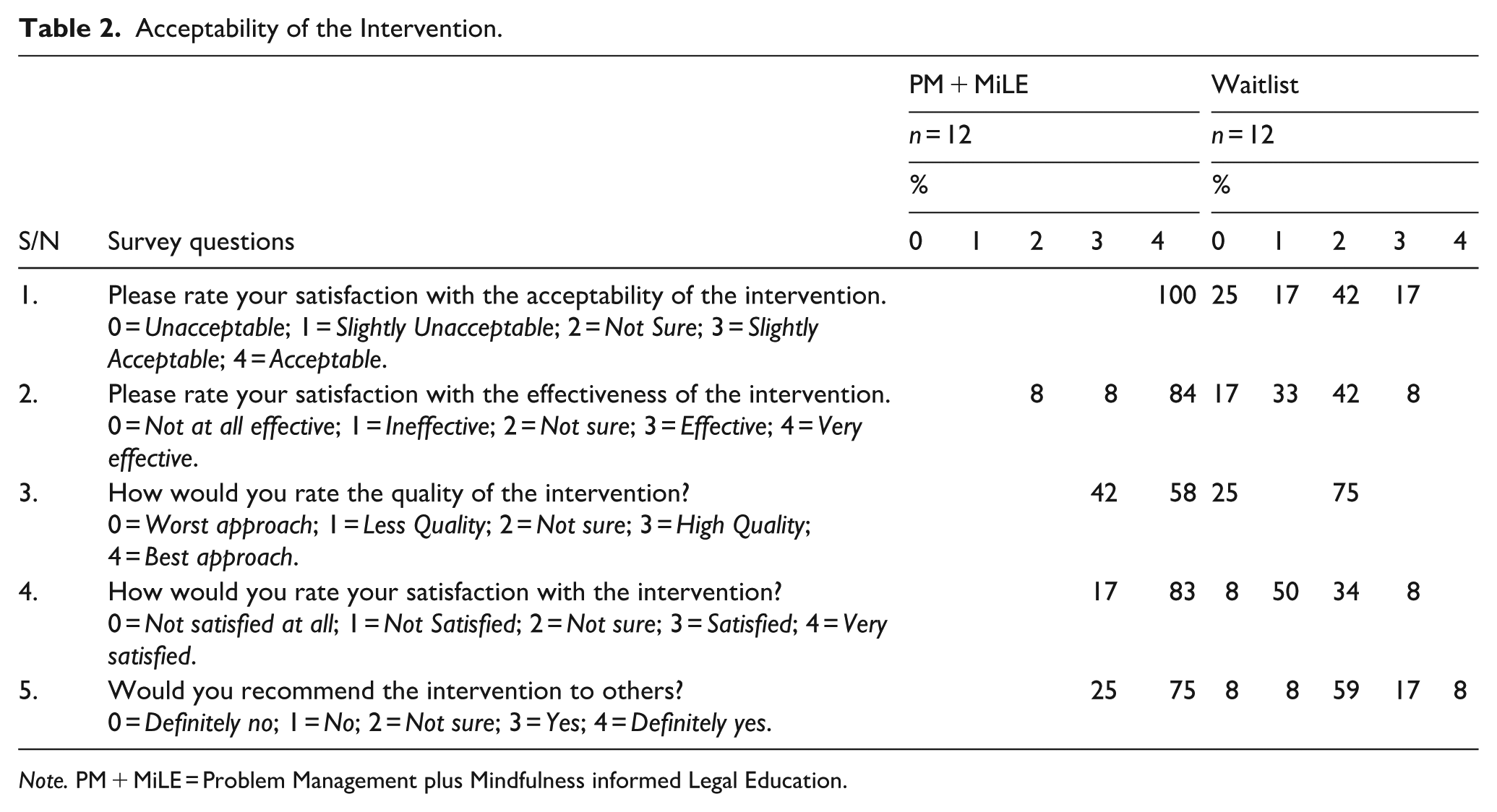
Regarding the acceptability of the intervention, as initially indicated in the study’s primary outcome, the intervention appears acceptable overall for the experimental group compared with the control group, who were also assessed based on the interventions they were aware of and had previously engaged with, as seen in Table 2.
Acceptability of the Intervention.
Note. PM + MiLE = Problem Management plus Mindfulness informed Legal Education.
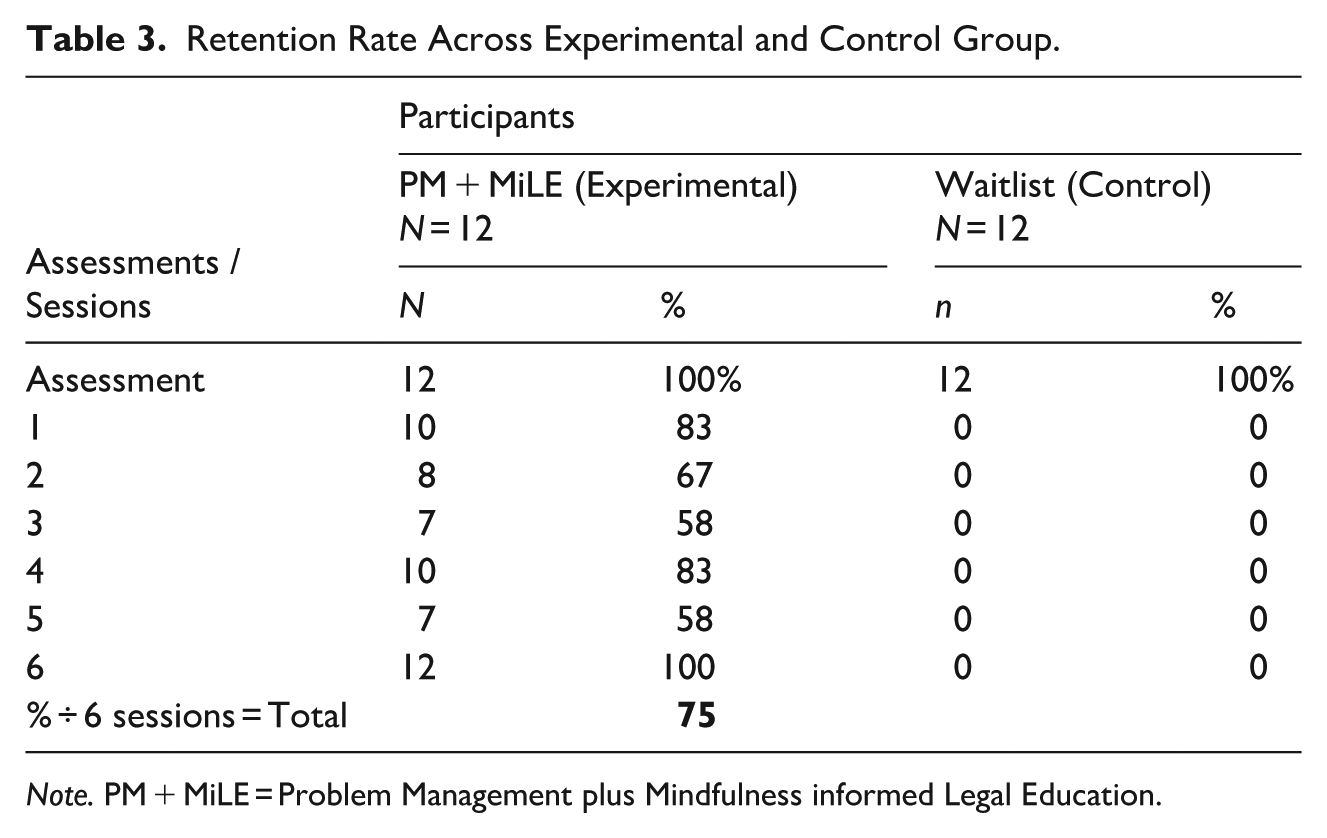
As shown in Table 2, the majority of participants in the experimental group, at 75%, indicated that they would definitely recommend the interventions to others, compared to 17% and 8% of the control group, who indicated “yes” and “definitely yes”, respectively. In terms of satisfaction with the intervention, 83% of participants in the experimental group indicated that they were very satisfied with the intervention, compared to 8% and 33%, who indicated they were not sure, and the others were satisfied with the intervention. A plausible reason for the experimental group’s positive receptiveness towards the intervention could be the rich content, which participants found more useful than the waitlist, who did not receive the intervention. Regarding participants’ retention, Table 3 shows the number of sessions participants attended. Overall, the study reported a high retention rate.
Retention Rate Across Experimental and Control Group.
Note. PM + MiLE = Problem Management plus Mindfulness informed Legal Education.
As shown in Table 3, the study recorded a high level of retention with most participants attending all sessions. The retention rates indicate that the delivery of the intervention is promising.
Secondary Outcome Measures Result
The secondary objectives of the study are to test the potential efficacy of the PM + MiLE compared to the waitlist control group in reducing affected victims of GBV resort to harsh parenting, including parenting stress and improving awareness of legal channels of accountability following experiences of GBV. The study secondary outcomes measure also seeks to determine the intervention’s effiacy in improving quality of life and social support. Table 4 presents the results of an independent sample t-test conducted at baseline and the end of the intervention for both the experimental and control, indicating that the experimental group performed better than the control group.
Independent Sample t-Test Results of Secondary Outcome Measures. Summary Table Showing HPS, GBVSP, LACCS and OSSS, Using Independent Sample t-Test and Categories Across Time at Baseline, and End of Intervention for the Experimental (PM + MiLE) Group and the Waitlist Control Group.
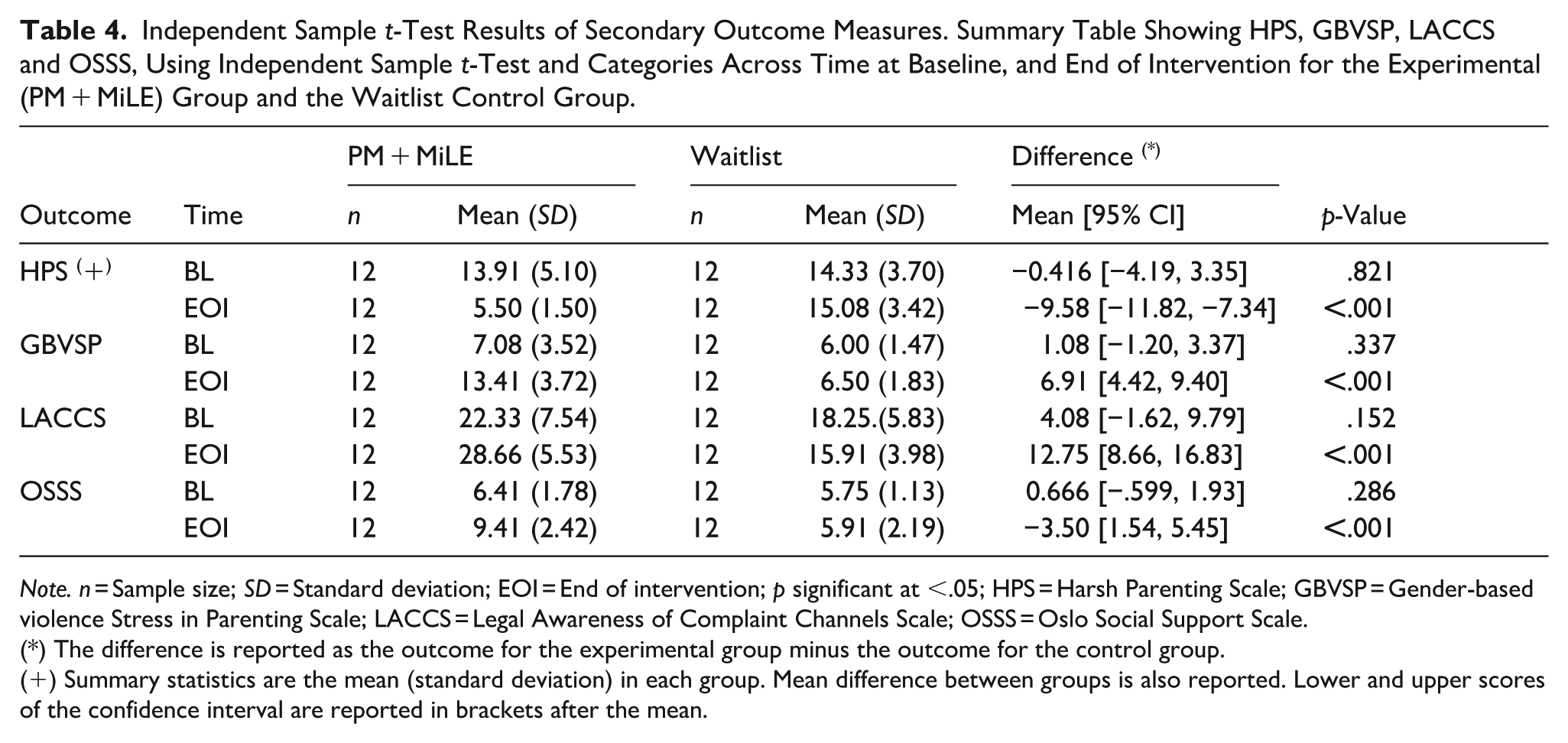
Note. n = Sample size; SD = Standard deviation; EOI = End of intervention; p significant at <.05; HPS = Harsh Parenting Scale; GBVSP = Gender-based violence Stress in Parenting Scale; LACCS = Legal Awareness of Complaint Channels Scale; OSSS = Oslo Social Support Scale.
(*) The difference is reported as the outcome for the experimental group minus the outcome for the control group.
(+) Summary statistics are the mean (standard deviation) in each group. Mean difference between groups is also reported. Lower and upper scores of the confidence interval are reported in brackets after the mean.
The preceding statistical analysis revealed significant improvements in the PM + MiLE experimental group compared to the waitlist control group across several outcomes. Compared to the control group, the 12 participants in the experimental group had significantly lower HPS scores (M = 5.50, SD = 1.50), indicating a reduction in resorting to harsh parenting at the end of the intervention than the 12 participants in the control group (M = 15.08, SD = 3.42). The results showed a significant difference, t(−9.58) = –8.87, p = .001. The reason for the positive outcome in the experimental group could be attributed to some of the topics covered, including stress management, problem-solving, and addressing adversity. Collectively, the topic enhances and equips participants with mood management skills, resulting in a bidirectional relationship that improves the outcome for participants positively, whilst reducing their resort to harsh parenting.
In terms of the GBVSP scale, participants in the experimental group had significantly improved scores (M = 13.41, SD = 3.72) indicating a reduction in GBV and stress in parenting at the EOI than the 12 participants in the control group (M = 6.50, SD = 1.83) with a significant difference, t(6.91) = 5.76, p = .001. However, for the control group, we observed no improvement, indicating ongoing stress in parenting. Regarding LACCS, the experimental group demonstrated improved knowledge of legal channels of support (M = 28.66, SD = 5.53) at the end of the intervention compared to the waitlist control group (M = 15.91, SD = 3.98) with a significant difference, t(−12.75) = 6.48, p = .001. Thus, the use of PM + MiLE appears promising in improving knowledge of legal rights, access to justice, and support. However, participants in the control group showed no improvement in their level of awareness, and this may be due to their limited exposure to awareness of legal support channels.
Regarding level of social support, the experimental group showed improvement in the increased level of social support (M = 9.41, SD = 2.42) at the end of the intervention than the control group (M = 5.91, SD = 2.19) with a significant difference, t(–3.50) = 3.70, p = .001. However, the control group performed poorly, which appears partly due to the limited information on strengthening the social support they had, which was effectively addressed in the experimental group using the PM + MiLE intervention. The data from the qualitative findings shed further light on why the experimental group performed better than the waitlist control group.
Study 2: Qualitative Findings
The findings from the qualitative data were based on participants’ lived experiences and perceptions of PM + MILE compared to those of the waitlist control group. The findings highlight the state of the participants before the intervention and after engaging in the PM + MILE compared to the waitlist control group. Informed by thematic analysis from an intersectionality and social learning theoretical lens, the following main themes emerged: Agonising experience, adverse parenting impact, poor support, enlightening content, and positive sense of empowerment. The analysed themes are addressed below.
Agonising Experience
Across both the experimental and control groups, prior to the intervention, a recurrent pattern in the dataset was the perceived agonising experience encountered by participants as a result of GBV. This experience ranges from physical abuse to poor financial independence and psychological distress, with a significant impact on their parenting role. As one participant from the waitlist control group said: I have three children. If I want to tell him to bring school fees and being that I am a worker, he takes it upon himself that since I am a worker, I need to pay the children’s school fees. So, for that reason, you see the way he takes it when you just demand the fees, the next thing you see is he is very, very angry [. . .]. So, for that reason, he just attacked me. [. . .] He just hit me because I demanded something. And so, with that, we fought, and he even injured me. I had to run to my parents, of which I am still passing through the pain up to now, and it is not really easy with me. (Fejiro)
The participant extract highlights how the intersection between multiple forms of disadvantage and inequality reinforces a distinct form of abuse experienced. The intersection between her understanding of the gendered role as a man culturally prescribed to provide for the family, coupled with the patriarchal domination by her husband, appears to significantly impact her, whilst leaving her in a vulnerable state. A plausible explanation for the participant’s views is that her understanding of caring responsibilities and required support for her husband to pay the tuition bills influences her expectations from her spouse, which appears detrimental. Physical violence appears to be resorted to by her husband to assert his male dominance and sense of control. Commenting on GBV, such as the abuser’s resort to physical violence, another participant from the experimental group recounts her experience as follows: It happened when I got married early. When I was in the early stage of marriage, I was six months pregnant, and I noticed that my husband was cheating. Unfortunately, it was with a friend of mine [. . .] So it happened that he was going out with my landlord’s daughter [. . .]. So it happened that the girl was coming to Warri, and they were doing their stuff unknowingly to me, and I never knew. It was the friend that called my attention to that [. . .] he [Her husband] was telling her [ the landlord’s daughter] that I am no longer that fresh the way that I used to be before he married me, that my body is open. You know he was saying some sort of annoying things. So, when he came back from work, I approached him because I was angry. [. . .] So, he said I should get out, and he slapped me. That was how he started beating me. I was six months pregnant. He hit me to the extent that I passed out. He was actually the one who took me to the hospital, so from that experience, I developed BP [High Blood Pressure] because he was seriously hitting me on my head. (Ngozi)
The participant’s extract denotes abuse suffered as a result of confronting her husband on the alleged accusation of infidelity. Physical violence, such as beating (e.g. hitting and smacking), was construed as a measure taken by the spouse with a detrimental effect on her health. Such a resort to violence also conjures a negative experience. Again, the intersection between the ideal body and expectation was seen to conjure a feeling of being body shamed, which, for the participants, appears very embarrassing given her condition at the time and the fact that she was a mother. The ripple effect of her reacting to the perceived disrespect and infidelity of her husband led to physical violence on his part, which unfortunately left her with a life-changing health condition.
Adverse Parenting Impact
GBV impact often transcends the immediate victims with ripple effects on children in the relationship. A recurrent pattern in the dataset was the perceived impact of such violence, which often manifests in the transfer of anger and aggression to innocent children or, in some cases, a learned behaviour which impacts children involved to the extent that it affects their behaviour in school and even their educational attainment. Commenting on its impact on the mother’s behaviour towards her children, one female subject who was a participant from the experimental group said: My experiences are so much sad because they happen to me personally. I got married a few years ago, and I had a child, so it happened that each time we had an issue like this, my husband would just beat me up. Say all sorts of things. At times he will tell me that I should pack out of his house and leave. At times, he will restrict me from moving around like, he will tell me that if I step out, he threatens me with all sorts of things. Sometimes he will lock me in the house and then he will go out and before he will come back it’s late in the night and he only have access to the door. So, at times I will get so traumatised to a point that I will have to unleash my anger on my baby. And of which it is really giving me a mental issue because anytime someone comes or if I am talking to my people on the phone and if they ask me some question it triggers my anger in the way that I will respond, and they will know that something is going wrong. I don’t want to really point it out to them so that it won’t be like I am complaining. (Fieyelami)
Commenting on the adverse impact on parenting and its negative impact on children behaviour, another participant from the experimental group said: It was not easy because, at times, the children will be seeing your weaker side. You want to hide it, but then, at times, they will definitely see it. [. . .]. At times, when they go to school, you will see their performance and their behaviour. They do not interact with people because their teachers used to and get back to us when, at times, they engage in such behaviour. (Boyelayefa)
The preceding extract denotes the adverse impact of GBV on parenting. The agonising and traumatising impact of being subjected to GBV appears to significantly impact the behaviour of affected victims who, in the form of transferred aggression, unintentionally unleash such anger on their child. The implication is that it leads to poor parenting and the inability to effectively control their emotions, which, in turn, leads to a ripple effect of bringing up children who later become adults who, in some instances, are unable to effectively manage their emotions or resort to violence as a means of resolving conflict. Thus, such unintentional learned behaviour from their primary caregiver through the social context in which it occurs could lead to a form of emulation through social learning. The implication is that it affects their relationship with others and has an impact on their educational attainment and, by extension, leads to a revolving cycle of GBV and abuse. A participant from the waitlist control group, whilst recounting her experience, also said: For the whole stress that I was going through. I was feeling a lot of pains and. Sometimes I even dislike taking care of the children. I didn’t and having time for them was something else because even I was having this constant rejection here and there. Rejection, constant fear, constant keeping to myself. So, I couldn’t take care of the children very well. It kind of made the children to also be violence on their own. Sometimes they fight. They unnecessarily fight among themselves and causes trouble outside because of what they see and lack of concern. So, the effect is that. They go out there and become violent also. (Tedjiri)
The preceding extract highlights a perceived intersection between the abuse the participant suffered and the stressful impact it had on her ability to parent. The externalising feelings experienced were also detrimental to her well-being and, as such, led to an unintended abandonment of her parenting responsibilities. These findings impact her parenting role with a detrimental effect on her children, who are then at the receiving end through copying the learned behaviour and emulating similar traits such as physical violence in their relationship with their siblings and others. Thus, it highlights the children’s negative social learning from the family as a primary unit of socialisation.
Poor Support
A recurring pattern in the dataset was the perceived limited support that participants encountered before the intervention, regardless of whether they were in the experimental or control group. This inadequate support often leads to a sense of suffering in silence due to a lack of awareness of support channels or even legal avenues for redress. Often, resorting to their faith or spiritual beliefs becomes the primary form of support they rely on. Talking about this, one participant from the experimental group said: No support. My support system was God you know. because at some point he stopped me from going to work. That if I go to work, I do see other genders at there and all that. He restricts me to a lot of things. So, at times if such things happen, I cry out my heart in my pillow. The next thing I do is that I will turn to God. But humanly support, I lack that. (Vanessa)
On a slightly similar note, another participant from the waitlist control group said: There was no formal support[. . .] I didn’t speak out to anyone. So, I concealed it. I went through the trauma all alone. I went through the pains all alone. I tried as much as possible to hide what I was going through, so there was no form of support from anywhere. So that was what makes it even worse. [. . .] I even dislike taking care of the children. (Tedjiri)
The preceding extract highlights a state of helplessness the participant faced, and again, the intersectional role of an ideal woman and the expectation for her to effectively manage the problems within her home placed a significant burden on the participant. Terms, such as “I went through the pain all alone,” are seen to be construed in ways that reinforce social inequalities and gendered norms that appear disadvantageous to the female subject, whilst having to endure the abuse in silence for fear of being labelled an ill-cultured woman unable to manage the conflict in her home. The implication is that it risks impacting parenting, as shown in the participant’s extract, which demonstrates how it adversely influenced her parenting.
Enlightening Content and Positive Sense of Empowerment
A recurring pattern in the dataset was the perceived benefit of the programme, which was mostly construed in a positive light. Most participants reported a sense of enlightenment gained during the intervention session, which involved the PM + MiLE related to the topics covered, including problem management and stress management. Talking about this, one participant from the experimental group said: I will say stress management and problem management. [. . .] because if you learn to manage problems, some reactions in life that you want to react to, you won’t do it. So, managing problems helps people not to overreact to something. It will help you, and it will also help your health. I will say my experience of the program was impactful and helpful because I have come to realize that for some decisions in life, we do not make it too quickly, and we should look at things ahead. We should look at the future before we put our hands into doing some things. (Selena)
On a slightly similar vein, another female subject who was a participant from the experimental group said: I just like this program, and one of the things I’ve learned from the problem management is, you know, we are in this life, and we see so many things in this life, especially as parents’ challenges will be there and how to manage these challenges, especially in giving, taking care of family, children’s husband you know. So, I have learned how to deal with stress or learn stress management. I really learned a lot that day. I was so happy after everything. How you can ease yourself from stress like stress from children. I learned how to ease some stress of my body. [. . .] The interesting part of it also is the legal intervention. That’s the interesting part of it because most women, like me, as I said, are not aware of their legal rights. [. . .] Like I said before, the programme is an interesting one; I pray that many people get involved. More women need to be involved. Let’s publicize it. Let’s talk about it. Let’s encourage people not to die in relationships that are not working. [. . .] Let’s also keep creating awareness of the things that are the benefits that we’re supposed to have because most people do not know about their rights. So, generally, it was a good one. (Adamma).
The preceding extract highlights the perceived sense of empowerment that participants felt in managing problems within their home and externally. GBV often conjures stress, and for the participant, the content during the intervention helped address the significant issue associated with stress, which often tends to impact their parenting through a form of transferred aggression. Regarding awareness of legal channels of support and accountability, gender-based issues are often experienced with limited awareness of support, as recounted by most participants in our study. However, after engaging in the intervention, the participant demonstrated an increased awareness of support channels, the procedures for securing legal aid, and their legal rights. Thus, this provides further evidence to explain why the experimental group did better than the waitlist control group, which was not administered the PM + MiLE. However, for the waitlist control group, the experiences with limited support were construed as negative with implications for their parenting. As one participant commented: My husband, whom I had four children with, was violent, and this affected me psychologically, mentally and physically. Initially, he had to travel to another state because he was transferred for work. So, we agreed that he could travel and come to see them as regularly each month as travelling with the kids would disrupt their education and stability. He did, and then he visits once a month, once in four months, and then just twice a year. Unknowing to me that he had another woman whom he was cohabiting with and had issues with her. When I found out and confronted him, he beat the living daylight out of me. So, the family came to speak to him, and he was so aggressive that it was over. He only sent a meagre sum of 50,000 naira to take care of the 4 children, and I had to withdraw the children from private to public school because I could not afford it. He never checks on us anymore, and the whole incident broke me down psychologically. I had no support whatsoever because, culturally, I am expected to deal with my matrimonial problems and not tell the whole world about them. So, I suffered in silence, and parenting became a nightmare as I had to deal with it all by myself.
Again, the preceding extract denotes the challenges women go through as a result of experiencing GBV. The intersection between perceived gendered roles and cultural expectations was construed to present inequality and undue privilege to the male, which was detrimental to the participant who felt unable to speak up for fear of societal reactions. Such challenges were further compounded by the poor support available to affected victims. As denoted in the participant extract, the implication is its impact on her parenting, which becomes quite difficult given the myriad of challenges, including psychological and economic impediments, she faces.
Discussion and Conclusion
GBV often affects women and girls, who are mostly the primary victims. However, the resulting harm could be severe to families and children. Research on how interventions could be used to address the intersection between GBV and parental stress in Nigeria is scarce, and this includes interventions that target the combined effect of GBV, stress in parenting, and awareness of legal channels of support in Nigeria using experimental designs. Our current study complements previous work on GBV, focusing on violence experienced by women or those pregnant or the perceptions of GBV (Adinma et al., 2019; Dahal et al., 2022; Malatjie & Mamokhere, 2024). The article primarily contributes to the broader literature aimed at breaking the cycle of violence through effective parenting and support systems. We also made a significant original contribution to the literature by adopting an experimental design informed by the unique combined fusion of intersectionality theory and social learning theory to study an understudied context. Empirically, our study yielded the findings discussed below.
Firstly, overall, we found that the PM + MiLE is feasible in terms of recruitment and participant adherence to the intervention, which holds promise for future scale-up of the intervention. The reasons for the results could be attributed to the valuable intervention contents, which were perceived as timely, given the limited support women with lived experiences of GBV face. Previous studies have shown that women with experience of GBV tend to have limited support, with no access to transportation, social services, or other resources such as public shelters for the victims subjected to abuse (Fawole et al., 2021).
Secondly, we found that stress in parenting can be addressed through intervention content that focuses on problem management using mindfulness-informed techniques and mechanisms for problem-solving. As the quantitative data show, participants in the experimental group performed better in reducing their stress in parenting than those in the waitlist group, whose scores remained unchanged. This is even though at baseline, both groups had similar levels of experiences of GBV and stress in parenting. Previous studies have shown that parental stress could be exacerbated by GBV with a significant impact on parenting (Geprägs et al., 2023; Ike, Jidong & Ayobi 2023). These findings hold significant implications for policies designed to address GBV by demonstrating the need to encourage the integration of psychosocial interventions designed to manage problems and address stress in parenting due to GBV.
Thirdly, we found that harsh parenting was prevalent across both groups at baseline. Previous studies have also shown an association between harsh parenting and children’s resort to aggressive behaviours (Holt et al., 2008; Lin et al., 2023; B. Liu et al., 2022; L. Liu et al., 2023; You & Lim, 2015). Previous theories, such as the Coercive Family Process theory, indicate that negative parent–child exchanges significantly impact the socialisation of aggressive behaviours in children (Patterson et al., 1992). More specifically, harsh parenting could provide models of aggressive behaviours to achieve personal goals (Ross & Howe, 2009). Collectively, different harsh parenting forms could make children more vulnerable to emotional dysfunction and impulsivity (Shields & Cicchetti, 2001) and more likely to resort to resolving social problems in aggressive ways (Brody et al., 2014). Our study findings show that participants in the experimental group exhibited a reduction in harsh parenting compared to those in the waitlist control group, whose scores remained unchanged. This finding implies that harsh parenting often contributes to children’s poor emotional regulation, which in turn causes aggressive behaviours, and as such, addressing this through effective intervention appears paramount. In essence, the findings hold important policy implications aimed at disrupting the revolving cycle of aggression and violence.
Finally, we found a high level of poor support experienced by victims of GBV across both groups due to the intersectional conflation of cultural norms, gendered identity, and patriarchal societal system, which serve to create inequality and exacerbate the suffering of victims of GBV who are often not aware of legal channels of support and means of accountability. However, after the intervention, participants in the experimental group demonstrated more awareness, which was empowering as they felt educated on their legal rights, access to legal aid, and mechanisms for legal accountability. The findings of poor awareness of legal support channels resonate with previous literature (Ike et al., 2022). By contrast, those in the waitlist control group showed no improvement in awareness of legal support channels or improved social support more generally, as their scores remained the same at the end of the intervention compared to the baseline.
Regarding diversity and generalisation, the findings are transferable and generalisable to other contexts and countries, sharing characteristics similar to those of our study population, such as parenting style and demographics. For example, harsh parenting is often prevalent in African contexts, including Nigeria (Ngwaka et al., 2024; Pesando et al., 2024). GBV, coupled with poor awareness of legal support channels, exacerbates the risk of resorting to such a parenting style. In this light, policymakers, researchers, practitioners, including civil society organisations working with the affected populations, are required to draw on the importance of understanding the intersection of cultural beliefs and gender inequalities associated with this population as opposed to others, including their white counterparts, because a one-size-fits-all approach might be unhelpful in addressing the complex challenge they face. In addition, poor help-seeking is quite dominant among this population, which, as other studies have shown, is also quite common among African women compared to their white counterparts, who are more open to seeking help, including psychosocial support (Shanmugam et al., 2024). As such, policymakers and stakeholders working with this population and seeking to improve the diversity of service uptake and support may benefit from applying this finding through awareness promotions of support channels alongside encouragement for help-seeking.
The study, like any other, acknowledges its limitations. This includes the small sample size and the short follow-up period, which only involved the end-of-intervention assessment. The efficacy of PM + MiLE should also be treated with caution due to the small sample size, which is not powered to detect significant effectiveness. Another limitation of the study is that we only included participants who were able to speak English; this may have excluded other participants who could not speak or understand the English language due to Nigeria’s cultural diversity. Future studies could make provision for non-English speakers to aid better inclusivity. Notwithstanding the limitations, our study’s strengths lie in its use of an experimental design informed by the combined fusion of social learning and intersectionality theories. As our findings show, addressing the combined link between GBV and stress in parenting is crucial to disrupting the revolving cycle of violence. As such, the study recommends a fully powered cluster-randomised controlled trial to test the effectiveness of the PM + MiLE across a larger sample size. The study also recommends longer follow-ups at 3, 6, and 12 months to effectively determine the efficacy of the intervention.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605251393732 – Supplemental material for Problem Management Plus Mindfulness Informed Legal Education (PM + MiLE) Intervention for Addressing Gender-Based Violence and Improving Parenting in South-South Nigeria: A Randomised Controlled Trial
Supplemental material, sj-docx-1-jiv-10.1177_08862605251393732 for Problem Management Plus Mindfulness Informed Legal Education (PM + MiLE) Intervention for Addressing Gender-Based Violence and Improving Parenting in South-South Nigeria: A Randomised Controlled Trial by Tarela Juliet Ike, Dung Ezekiel Jidong, Chiyem Lucky Nwanzu, Maureen Iru Ntaji, Daniel Kamaru Adamu, Kelvin Odeyovwi Ayobi, Mieyebi Lawrence Ike, Evangelyn Ebi Ayobi, Peremi Richmond Ike and Christopher Francis in Journal of Interpersonal Violence
Footnotes
Ethical Considerations
The study received ethical approval from the Jos University Teaching Hospital, Nigeria.
Funding
The authors received no financial support for the research and/or authorship of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Data Availability Statement
Due to the sensitive nature of the research, supporting data is not available.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.