
Abstract
Ongoing health issues influence the postseparation lives of survivors of intimate partner violence (IPV). This study identified associations between health following IPV and demographic, housing, employment, and social participation factors. Survivors of IPV in Australia were surveyed. Logistic regression assessed factors of interest with physical and mental health conditions. Six hundred and fifty-eight women participated. Physical health issues were associated with reduced skills and confidence in employment. A mental health diagnosis was associated with women not working as desired and lower incomes. Screening for health impacts and longer-term responses to women could reduce the long shadow of IPV impacts.
Introduction
Violence against women occurs at unacceptably high levels, and international evidence consistently reports a lifetime prevalence of one in three women experiencing male violence (World Health Organization, 2005). This paper focuses on a common form of violence against women, intimate partner violence (IPV). The long shadow cast by IPV is often not well understood with community attitudes suggesting that women “should just leave” (Webster et al., 2018), when in fact postseparation is a time of heightened risk and most women separating from abusive partners experience forms of continuing postseparation IPV (Spearman et al., 2022). This paper reports on research that aimed to investigate the long shadow of physical and mental health outcomes for women who have experienced IPV and how this relates to the citizenship domains of employment, income, housing, and social participation after women leave their abusive partner. These citizenship domains are crucial, as they are the foundation of modern life and central to women rebuilding their lives.
Defining the Dimensions of Intimate Partner Violence
IPV can involve abuse and violence that is physical, sexual, financial, emotional, and/or psychological. Key to the definition of IPV is that it is a purposeful set of tactics used by the perpetrator to exert power and control over their partner or ex-partner to induce fear (Chung & Wendt, 2015). Patterns of perpetration can shift over time and with changing circumstances to maintain control over the other party. For example, women separating from abusive partners can experience IPV tactics such as stalking, financial abuse, and intimidation of family members, which may not have occurred during the relationship. In Australia, where the study was conducted, 23% of women report having experienced violence or abuse from a cohabiting partner or ex-partner (Australian Bureau of Statistics, 2017). One in six women has experienced at least one incident of physical and/or sexual violence by a cohabiting partner (Webster, 2016).
Physical and Mental Health Impacts of IPV
Research has continued to reveal the extensive and long-standing physical and mental health impacts of IPV (Campbell, 2002; Coker et al., 2002). Early cross-sectional studies found that, compared to women reporting no experiences of abuse, women who have experienced IPV are more likely to report physical ill health and disabilities, including musculoskeletal, neurological, cardiovascular, genito-urinary, respiratory, and digestive tract conditions and symptoms (Campbell, 2002; Coker et al., 2002). In addition, recent studies of women accessing domestic violence shelters showed that women's sleep was significantly impacted by IPV, and five of the seven items on the sleep disturbance index were associated with coercive control and the effects of PTSD (Jackson et al., 2020). The Australian national longitudinal women's health study, which has a broadly representative sample, showed that across three generations of women over a 16-year period women's physical and mental health and physical function were poorer and their pain levels were higher compared with their age cohorts not reporting IPV (Loxton et al., 2017; Wathen et al., 2018).
Research over time has consistently shown that women with IPV experiences report their health as poorer compared to cohorts reporting no IPV (Campbell, 2002; Coker et al., 2002; Loxton et al., 2017). Women's self-reports on their health show that 83.5% of women reported IPV negatively affected their health (Wadsworth et al., 2018).
While the mental health of women who have experienced IPV is often poorer than their counterparts, concerningly, it remains poor for many women over time. An early meta-analytic review identified strong associations between IPV and mental health concerns, such as posttraumatic stress disorder (PTSD), depression, suicidality, and alcohol and drug abuse (Golding, 1999). This review showed that the severity and prevalence of depression and PTSD among women who have experienced IPV were related to the severity and duration of the violence they experienced. Recent studies are examining these associations further. Research by Wadsworth et al. (2018) shows the relationship between coercive control and subsequent PTSD and how this contributes to sleep disturbance which results in further poor health outcomes. The findings of the study by Jackson et al. (2020) suggest that PTSD is the leading emotional distress characteristic among IPV survivors. In further research on the contribution of specific forms of abuse to women's mental health, Stylianou (2018) identified the association between economic abuse and IPV survivors’ reports of depressive symptoms. She posits that economic abuse creates sustained economic dependence, which can not only prevent women from leaving their partner but also prevent them from being able to financially care for their children, and that such enduring oppressive conditions result in depressive symptoms.
Longitudinal research indicated that participants reporting IPV and poor health at a young age were more likely to have persistently poor health over the life course compared with those reporting IPV and poor health at an older age (Loxton et al., 2017). If women's physical functioning and mental well-being are chronically impaired because of IPV, this will impact the employment and lifetime earnings of many women. A Canadian population-based study by Du Mont and Forte (2014) found women experiencing multiple and severe forms of violence from a partner were more likely to have debilitating mental ill health, which prevented them from engaging in various forms of social and economic life. Subsequent studies have also found that women with experiences of IPV and poorer health outcomes are also more likely to be living on low incomes or lower incomes than prior to IPV (Loxton et al., 2017; Wathen et al., 2018). Studies of accessing help also revealed women on low incomes were overrepresented among survivors and how this influences what services they can even access in some countries, for example, in the United States where mental health services may only be available to those who can afford to pay (Machisa & Shamu, 2022; Wadsworth et al., 2018).
This study sought to extend previous research about factors that may contribute to the mental and physical health outcomes of women who have experienced IPV, by examining variables in the domain of citizenship. Studies have not always identified whether women had poor mental health prior to the IPV or after it began. This study addresses this question and examines the relationship between mental and physical health outcomes and women's employment, housing, and social participation after separating from a violent partner. There is currently limited research examining how health outcomes intersect with these citizenship domains when women reestablish their lives after IPV.
Previous research has found that IPV can erode such citizenship domains, during and after the relationship. IPV has been established as a primary reason for women's homelessness, and the negative impacts on housing circumstances are compounded for women who are, or have been, dependent upon their partner's financial support (Baker et al., 2009; Niolon et al., 2009; Pavao et al., 2007). Further, women's access to and availability for employment, which are impacted by IPV, also limit housing access and standards of living (Abraham, 2010; Staggs et al., 2007). IPV can also impact social participation due to the loss of social networks, discrimination, a low sense of belonging and confidence, and low community trust (Du Mont & Forte, 2014). Limited social support has also been identified as a factor that leads to women being vulnerable to multiple forms of IPV (Sanz-Barbero et al., 2019). This study examines the interrelationships between health outcomes and these citizenship domains.
This study aimed to illustrate the long shadow cast by IPV and identify factors associated with women's health status, housing, and economic and social outcomes of women who experienced IPV in their lifetime. Specifically, the likelihood of women reporting long-standing physical and mental health conditions following IPV was investigated in relation to demographic factors; the citizenship domains of housing, income, employment, and social participation; history of intimate partner violence; and psychological well-being. Hypotheses within the study were:
A diagnosis of a mental illness will be significantly associated with poorer outcomes for employment, housing, and social participation. A long-standing physical health condition will be significantly associated with poorer outcomes for employment, housing, and social participation. Poor employment, housing, and social participation outcomes will be significantly associated with long-standing mental and physical health conditions.
Methods
This study formed the first stage of a larger project aiming to develop new theoretical insights into gendered violence as a basis for future policy directions. A nonexperimental, observational design was employed to investigate cross-sectional relationships between long-standing mental and physical health conditions among women who have experiences IPV and outcomes for employment, housing, and social participation. In order to understand the impact of IPV on the citizenship domains of housing, employment, and health, data were collected from Australian women via an extensive community-based online survey conducted in 2016–2017. To investigate how variables such as employment and participation were influenced by IPV, some survey items were retrospective, asking participants to rate variables, such as psychological wellbeing and impact on employment, before, during, and after IPV. Other survey items were cross-sectional, including current employment and wellbeing. This paper mainly reports on the quantitative survey data, although some qualitative data from the open-ended survey responses will be used in the discussion section to elucidate the quantitative findings.
Participants
The study was granted ethical approval by the University of South Australia's Human Research Ethics Committee. Participants were recruited via convenience sampling. We aimed to obtain a community sample to provide broad-based understandings of the impact of IPV. This approach was employed as previous studies into IPV often drew on samples from women accessing domestic violence and related services, rather than a wider cross-section of women. We aimed for a sample size large enough to enable comparisons between different subgroups of women. We sought diversity across the sample in relation to socioeconomic background, age, ethnicity, ability/disability, indigenous status, women with and without children, and women residing in cities, regional areas, and remote areas.
To achieve our sampling aims, the survey was advertised to women in Australia by engaging with local, state, and national media to promote participation, and social media advertising and human service organizations that provide support to women experiencing intimate partner violence also promoted the study in agencies and through other avenues such as agencies’ websites and newsletters. The investigators also promoted the survey through their universities’ networks. This combination of strategies aimed to ensure a diverse sample of women, including those who had not, and were not, accessing formal support services. To be eligible for this study, participants needed to be female, over 18 years of age, residing in Australia, self-identifying as having a history of IPV, and no longer residing with the violent partner. Survey responses were anonymous, and respondents accessed the survey online, which enabled participants to complete the survey at a convenient time and pace, while also ensuring safety. There was also the option to complete the questionnaire in hard copy form or via a telephone interview, which some women opted to do. Prior to and on completion of the survey, respondents were provided with information about where to access support services in the event that participation in the research caused emotional or psychological distress.
Survey
The online survey was administered using SurveyMonkey™, a web-based platform for the creation and dissemination of surveys. The survey comprised 57 questions answered via a combination of nominal scales and text boxes that allowed for open-ended descriptions and examples of IPV impacts. Respondents provided demographic information (e.g., age, locality, income bracket and source, education level, and cultural background), housing, employment, daily activity participation, and health information (physical health conditions and mental health) using predetermined categories.
The duration of IPV was measured by asking participants “How many years have you experienced IPV?”, and responses were grouped into 5-year intervals. IPV was measured in terms of physical, sexual, psychological, financial, and spiritual forms of violence, with participants able to select the frequency of these violent behaviors (“Never,” “Sometimes,” or “Often”). Participants also indicated whether they sought help for IPV and whether they experienced violence from other family members (“Yes” or “No”).
Mental health diagnoses were measured through self-reporting. Participants indicated whether they had ever been diagnosed with a mental illness in their lifetime, the name of the diagnosis, and the period of time in which the diagnosis was given relative to their experience of IPV (i.e., before, during, or after the relationship with a violent partner). Participants were also asked to rate their current psychological wellbeing (i.e., at the time of completing the survey) and to make retrospective ratings of psychological wellbeing in relation to their experience of IPV (i.e., (before, during, and after the violent relationship).
Physical health was measured by asking participants, “Do you have any long-standing physical health conditions, impairment, or disability that has lasted or expected to last 12 months or more?” (“Yes” or “No”). Participants were also asked to specify their physical health conditions.
Data Analysis
The statistical analyses were performed with SPSS version 22 (IBM Corp, 2013). First, univariate analysis was conducted to identify factors associated with physical and mental health conditions in women who experienced IPV to include in the second stage of analysis. A series of Chi-square or Fisher's exact tests were conducted, using the dichotomous physical health question and having a diagnosis of a mental health condition as dependent variables. Variables associated with participant demographics, IPV history, housing, previous experience of employment, daily activity participation, and perceptions of psychological well-being were entered as independent variables. Assumptions of independence and expected frequencies were met. Independent variables with two-sided p < 0.05 in the univariate tests were selected to progress to the next phase of analysis, a consecutive multivariate analysis.
In the final stage of analysis, we examined the association of independent variables selected from the univariate analyses with the status of participants’ physical and mental health conditions by fitting two logistic regression models, respectively, after adjusting for the effects of the other variables. Dummy coding was applied to categorical variables. Assumptions of independence, multicollinearity, linearity, and sample size were met. The magnitude of the association between these variables and the health status was evaluated through the estimate of adjusted odds ratios (OR) and the corresponding 95% confidence intervals (CI). The stepwise procedure was applied to the logistic regression analyses with both significance level for entry (SLE) and significance level for stay (SLS) set to 0.15 (Hosmer & Lemeshow, 2000). As such, nonsignificant variables were excluded from the final model. Hosmer-Lemeshow goodness-of-fit test was used to examine the fit of the final model. Two-sided p < 0.05 was considered statistically significant. G*Power version 3.1.9.1 was used to conduct post hoc power analyses (α = 0.05; Faul et al., 2009). Final conclusions were drawn from the multivariate analysis only. Responses to open-ended questions were used to assist the interpretation of the statistical analysis and provide descriptions and examples of IPV impacts.
Results
Participants
In total, 658 women participated in the study, aged between 18 and 80 + years (59.3% aged below 45 years). Over a third of respondents (38%) lived with their children (without a partner), 17% lived alone, and approximately a third (31.7%) of the respondents had remarried or repartnered and were living with that partner when completing the survey. A majority of participants (79.4%) had at least one child, and nearly half (47.7%) lived with their children. Two thirds of participants (66.2%) lived in a city, 31.2% in regional locations, and 2.6% lived in a remote area. Approximately one third of participants had an annual income below AUD$30,000. Missing data were minimal, with an average of 2.7% (SD = 4.0) missing data per variable.
Factors Associated With Physical Health Conditions
Univariate analyses showed that participants with long-standing physical health issues were significantly older, the duration of the IPV was longer, and the range of violence and its frequency was greater and reported poorer psychological well-being than those without long-standing physical health conditions or disabilities (see Table 1). A greater proportion of participants with long-standing physical health issues had more frequently experienced different types of IPV and sought assistance compared with the rest of the sample. The physical health issues women commonly described included chronic pain as a result of untreated injuries and associated limitations to their mobility, hypertension, and hearing loss.
Results of Univariate Analyses for the Status of Physical Health Conditions in Women Who Have Experienced IPV.

Long-standing physical health conditions, impairment, or disability that has lasted or is expected to last 12 months or more; bChi-square tests or Fisher's exact tests were used.
*p < 0.05. **p < 0.01. ***p < 0.001.
Significant variables from the univariate analyses were selected for the subsequent multivariate analysis. After nonsignificant variables were removed (SLE and SLS = 0.15), the final fitted logistic analysis (Table 2) revealed that participants with long-standing physical health issues were more likely to be older, seek assistance about IPV, experience violence from other family members, have poorer psychosocial well-being, and receive a diagnosis of mental illness than those without long-standing physical health issues. Participants with long-standing physical health issues were also more likely to have reduced confidence and skills for paid employment. Participants without long-standing physical health issues were more likely to perceive the experience of IPV as preventing them from working in a desired way. The post hoc power analysis showed an adequate power (1-β error probability > 0.95) for all the associated variables except current psychological well-being (1-β error probability = 0.48).
Final Model of the Logistic Regression Analysis for the Status of Physical Health Conditions in Women Who Have Experienced IPVa.
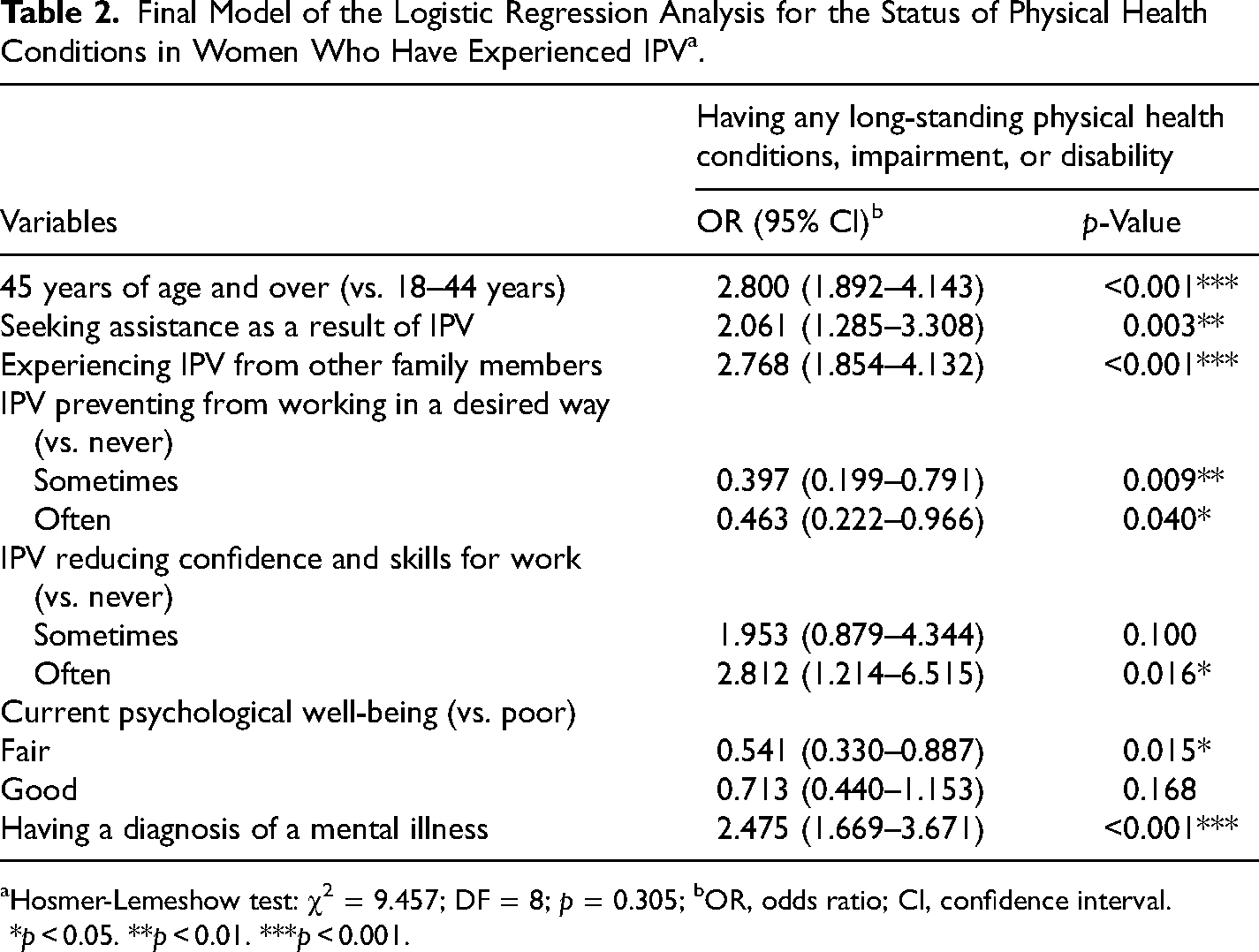
Hosmer-Lemeshow test: χ2 = 9.457; DF = 8; p = 0.305; bOR, odds ratio; CI, confidence interval.
*p < 0.05. **p < 0.01. ***p < 0.001.
Factors Associated With a Diagnosis of a Mental Illness
In total, 347 participants (53%) reported a mental illness diagnosis at some point in their lifetime. Forty-five participants (13%) reported a diagnosis before experiencing IPV, increasing to 43% during the violent relationship and 44% after leaving the relationship. The main diagnoses reported were anxiety, depression, and posttraumatic stress disorder. The results of univariate analyses showed that participants with a diagnosis of mental illness in their lifetime were significantly younger, had lower incomes, and more frequently experienced violence from other family members than those who did not have a diagnosed mental illness (see Table 3). In addition, participants with a diagnosis of mental illness experienced poorer psychological well-being before and after IPV as compared with those without a diagnosed mental illness.
Results of Univariate Analyses for the Diagnostic Status of Mental Illness in Women Who Have Experienced IPV.

Have you ever been diagnosed with a mental illness in your lifetime? bChi-square tests or Fisher's exact tests were used.
*p < 0.05. **p < 0.01. ***p < 0.001.
Significant variables from the univariate analyses were included in the subsequent multivariate analysis. The final fitted logistic model, after nonsignificant variables were removed (SLE and SLS = 0.15), revealed that participants with a diagnosis of mental illness were more likely to have lower incomes and poorer psychological well-being after the experience of IPV than those without a mental illness diagnosis (see Table 4). In addition, participants with a diagnosed mental illness were more likely to describe that their partners’ violence had prevented them from working in a desired way and were more likely to participate in support groups after IPV. The post hoc power analysis showed an adequate power (1-β error probability is between 0.78 and 0.99) for all the associated variables.
Final Model of the Logistic Regression Analysis for the Diagnostic Status of Mental Illness in Women Who Have Experienced IPVa.
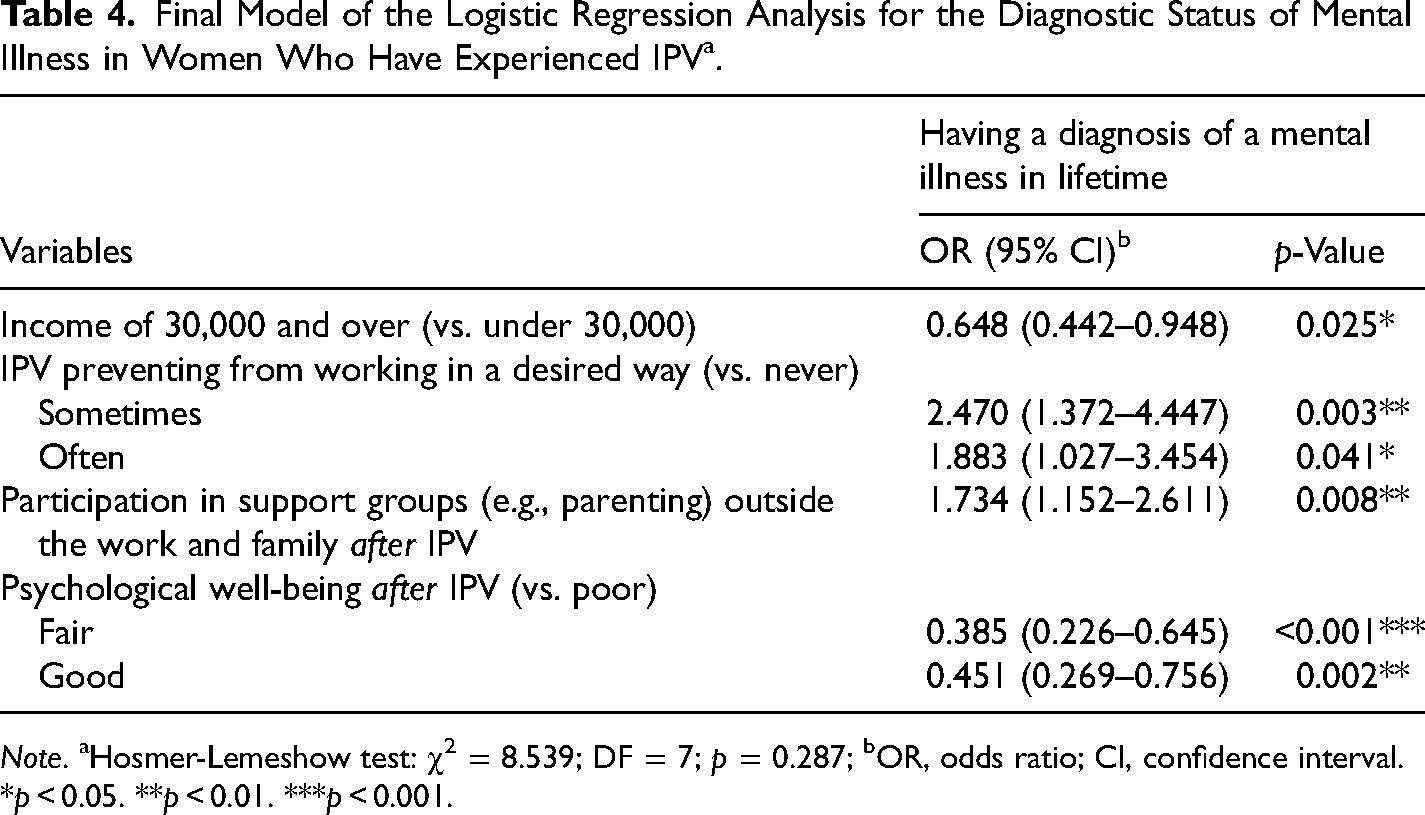
Note. aHosmer-Lemeshow test: χ2 = 8.539; DF = 7; p = 0.287; bOR, odds ratio; CI, confidence interval.
*p < 0.05. **p < 0.01. ***p < 0.001.
Discussion
The relationship between IPV and the consequent physical and mental health effects for many women has been well-established. This study sought to extend previous research by investigating the relationship between poor health outcomes and demographic factors, housing, employment history, and IPV experience. Results from the current study suggest that it is not simply the severity and frequency of IPV that may influence physical and mental health outcomes for women during and long after IPV. The hypotheses predicted that variables such as employment, housing, and social participation would be significantly associated with poor mental and physical health outcomes. However, we did not predict that physical and mental health would also be associated. Previous literature demonstrates that women do not experience the physical and mental health consequences of IPV separately; instead, they experience resultant, combined, and intersecting health problems (Coker et al., 2002). The relationships between current psychological well-being, psychological well-being after IPV, and physical and mental health in this sample further demonstrate women's experiences of multiple health issues concurrently. Women who rated their current psychological well-being as “fair” had lower odds of a long-standing physical impairment than women who rated their psychological well-being as “poor.” Further, those who rated their psychological well-being as “fair” or “good” after IPV had lower odds of a mental illness diagnosis. In addition, women with a mental illness diagnosis had higher odds of also having a long-standing physical health condition. These results illustrate the complex and dynamic nature of physical and mental health outcomes for women who have experienced IPV, such that the effects often accumulate across women's lifetimes and influence the experience and/or development of adverse physical and mental health outcomes. For example, Dutton et al. (2006) demonstrated how mental health issues impact behaviorally (e.g., low energy levels for exercise or job seeking) and physiologically (e.g., increased stress hormones with continuing threats to safety and financial insecurity) that can lead to cardiovascular or inflammatory health issues. While analysis and interpretation of results in the current study present physical and mental health outcomes separately, it is important to emphasize they are rarely experienced as such. They are intertwined and intersect in everyday life, often in an ongoing way as this study participant describes: The injuries I sustained physically and emotionally have affected my ability to work and provide for my family & myself, therefore my child doesn’t get to go away for holidays, the car constantly needs repairs, the bills continue to pile up….the list goes on. I recall my last job interview a couple of years ago for a sales management role, when my medical condition had deteriorated but I was desperate for an income - the General Manager asked me about my child (in a kind way) & I burst into tears. I had lost my confidence, my business “head” and the woman I thought I was. I was suffering major depression and PTSD, yet refused to believe it as all I had circling around in my head were the bills that needed to be paid. DV goes much farther than the time a woman leaves. Its effects are life changing, destructive and continuing far beyond the reach of what society may think.
Physical Health
A long-standing physical health condition was hypothesized to be associated with and predicted by housing, employment, and social participation outcomes. The hypothesis was partially supported as women who reported that IPV “often” or “sometimes” reduced their confidence and skills in the workplace had increased odds of a long-standing health condition. IPV places women at great risk of unemployment and job instability (Pollack et al., 2010; Staggs et al., 2007). Injury inflicted prior to work is a common disruption, preventing women from attending or performing well at work (Swanberg et al., 2005). Women experiencing harassment or violence often report poorer health, a lower sense of confidence in the workplace, and higher rates of absence due to sickness or injury (Hensing & Alexanderson, 2000).
Interestingly, women who reported that their experiences of IPV reduced their ability to work as desired (in terms of full- or part-time work, had lower odds of a physical disability or impairment. It is possible women with long-term physical health conditions in this sample did not consider themselves “not able to work as desired,” due to having limited expectations of the hours and type of employment they could manage with their health. As mentioned previously, women were often on low incomes; in the qualitative data from the survey, they describe combinations of government entitlements being received with casual or part-time work of differing kinds. In the open-ended response to describe examples of IPV impacts, this participant is solely reliant on income support payments and describes the poverty trap from her partner's financial abuse and the health effects of IPV: My disabilities are all as a result of domestic violence, therefore I cannot work. When I was working a large majority of my income went to paying off debt he had on my credit card. As a single parent with no support from family or friends you were isolated from, your income (if able to work) is capped as you can’t travel (i.e., a sales job, work shifts, weekends or nights). It restricts what industries you work in, not being able to study as I can't afford to, therefore it's a vicious cycle in trying to earn an income and get ahead. Plus, my medical bills have cost the majority of my pension - specialists, chiropractor, physio, doctors, cardiologist etc. Not all tests & doctors bulk bill!
In addition to the variables in the stated hypotheses, long-standing physical health conditions were predicted by age, such that women over 45 years of age had higher odds than those aged 18–45. The long-standing health conditions women reported included muscular-skeletal-related chronic pain, such as chronic back pain, high blood pressure, and mild cognitive impairments, e.g., memory loss and limited retention, after being subjected to violence over a period of time. The impact of IPV on health appears to be cumulative, with repeated violence associated with greater chronic health issues in older women compared with younger groups (Fisher et al., 2011; Sanz-Barbero et al., 2019; Stöckl & Penhale, 2014). Older women may have remained in abusive relationships longer due to generational beliefs about separation, a lack of access to any other financial options, fear of adult children's reactions, and a fear of leaving the family home (Penhale & Porritt, 2010). They may also experience violence not only from partners but family members, such as adult children (Penhale & Porritt, 2010). Age may possibly be a novel factor in IPV that increases the odds of long-standing physical impairment or disability due to prolonged exposure to violence, cooccurring family violence, or the cumulative effects of violence. This suggests that assessing older women's relationship and family history when they present with physical health issues may help identify previously hidden IPV (Loxton et al., 2006).
Existing literature suggests that the physical health impacts of IPV are a significant factor for women deciding to seek assistance. Both formal (counselors, medical doctors) and informal (friends, family) forms of help-seeking increase with the severity and frequency of IPV (Ansara & Hindin, 2010; Ergöçmen et al., 2013). Specifically, IPV resulting in physical injury is a significant predictor for both formal and informal help-seeking (Barrett & St. Pierre, 2011). The women in this sample who reported seeking help for IPV were more likely to have a long-term physical health condition, suggesting that injury or impairment may be a decisive factor or trigger for women when deciding to seek assistance and support for IPV, along with other known catalysts for help-seeking such as the impact of IPV on children (Stanley & Humphreys, 2015). The health issues considered in this sample are long-standing and/or expected to last for 12 months or longer and will undoubtedly affect many facets of women's lives. This highlights the importance of early identification of IPV and, once identified, to emphasize help-seeking and available supports and resources prior to the time when there is going to be a level of physical harm that will result in long-standing physical health issues and likely mental health issues.
Women reporting violence from a family member, in addition to a partner, had greater odds of a physical impairment or disability. Cooccurring or cumulative violence may lead to greater impacts on physical health of the victim (Penhale & Porritt, 2010; Sanz-Barbero et al., 2019). Davies et al. (2015) found that women who have experienced multiple abusive partners or a longer duration of violence had significantly worse health outcomes when compared to groups reporting fewer or shorter abusive relationships. Women who experience violence from multiple people known to them, including a family member and a partner, are often at greater risk of physical impairment or disability as a result, suggesting cooccurring violence may warrant specific focus in further research.
Mental Health
In contrast to women with long-standing physical health conditions, women who reported a reduced ability to work as desired were more likely to have a diagnosed mental illness, supporting the third hypothesis. In general, people diagnosed with a mental illness or psychosocial disability have lower employment rates than those with a physical disability and may experience disruption to employment due to the episodic nature of some mental illnesses and discrimination in the workplace (Australia Bureau of Statistics, 2012). However, in Australia, less than 10% of people with a mental illness receive a disability support pension (Mental Health Australia, 2014). This disparity is potentially due to the difficulties people with mental health issues have in meeting eligibility criteria, which require a current diagnosis, impairment that has been present for more than 2 years, and the ability to demonstrate that their condition is being treated and has stabilized (Mental Health Australia, 2014). Consequently, many people with mental ill health live with situations of precarious employment and the financial disadvantage that follows, particularly for women who also have primary care responsibilities for children. Participants gave the following descriptions of these experiences, highlighting the interrelated impacts of IPV on their well-being. The violence has left me with mental health issues (depression, anxiety, PTSD) and therefore I am unable to work consistently as I never know if I am going to be able to function adequately on any given day; it affected my reliability.
Sometimes I don't get involved in activities because I am exhausted, depressed and/or financially drained. Sometimes it is just too hard to put myself out there. A lot of activities these days have some sort of cost attached as well. Even though I have a good income the cost of legal bills, psychology, doctors’ visits due to stress related illnesses makes it hard.
I had to become self employed to assist my son with his developmental delays and be able to work around his needs and support him. His father has not been at all supportive in 18 years, in fact he has negated everything I have tried to do to support our son. Major depressive disorder and PTSD has had a huge impact on my ability to work full time and support my son alone.
These findings highlight a worrying disparity between the support available for physical conditions/disabilities and mental health issues. Considering the possible interactions between IPV, disability, and financial support may help address this gap further. More support for women experiencing IPV and the mental distress such abuse causes may help reduce the length and severity of these effects of IPV so that women's social, economic, and health outcomes are improved in the longer term.
Women who reported a higher income (over $30,000 a year) had lower odds of a mental illness diagnosis than those earning below $30,000. IPV has been linked to physical health symptoms at lower income levels, and this relationship may apply to mental health, with the inverse relationship between IPV and mental health well documented (Adams, Bybee, et al., 2013a; Campbell & Lewandowski, 1997; Golding, 1999; Sutherland et al., 2001). IPV can exacerbate stressors that women on low incomes have to address (such as maintaining housing and utilities) and may increase financial reliance on an abusive partner, potentially increasing the risk of mental health issues (Adams, Tolman, et al., 2013b). Findings suggest that without such income-related stressors, higher-income women experiencing IPV are at lower odds of receiving a mental illness diagnosis. An alternative explanation is that women with higher incomes may access support outside the mental health system, leading them away from the possibility of receiving such diagnoses. Future research that further examines the role of women's economic security and health outcomes following IPV would be of great value.
Our findings indicated that women reporting participation in support groups (such as parenting groups) after IPV were more likely also to have a concomitant mental illness diagnosis. Women may view their involvement in these groups as facilitating social connection, recovery, and healing. Our findings suggest that further research into help-seeking and mental health in the context of IPV would help establish the benefit of such groups in recovery and healing.
Limitations
An outcome variable of a diagnosis of mental illness may mask variability in mental health, as not all women experiencing mental health issues may have a formal diagnosis. Measures of psychological distress or mental health may more accurately capture mental health outcomes. Despite the open-ended accounts of participants indicating the onset of health conditions during and following IPV, it is important to note that not all mental and physical health outcomes may be directly related to IPV. The lack of a comparison group is a methodological limitation; however, other longitudinal research with large populations of women do reveal significantly poorer outcomes for women reporting IPV compared with their peers reporting no experience of IPV (Loxton et al., 2017).
Even though the sample was broadly representative of the Australian population, there were fewer women from ethnic backgrounds. This is likely the result of the survey only being available in English and its reliance on English language skills, as well as potential cultural barriers around acknowledging IPV in some cultural groups. Furthermore, there were also a lower number of women who experienced IPV in same-sex or lesbian relationships. This could be due to not explicitly targeting women who identify as lesbian or bisexual through specific services and media.
Conclusions
This study aimed to understand the likelihood of women reporting long-standing physical and mental health conditions following IPV in relation to demographic factors, history of IPV, housing, previous experience of employment and daily activity participation, and psychological well-being. Findings demonstrated the merit of investigating health outcomes regarding these factors and provided preliminary evidence on the relationships between them. This research expands upon the established relationship between the severity and frequency of violence and health and may help identify potential risks (e.g., increased age and prevention from working as desired) and protective factors (e.g., income) in relation to women's physical and mental health. Understanding factors relating to the likelihood of long-term physical and mental health effects can inform future screening to ensure risk factors are identified early and responses are tailored to be more effective. Importantly, this research and previous studies confirm the importance of providing a longer-term response to women survivors of IPV beyond the point of crisis and early separation, as many are still facing significant challenges to reestablish their lives due to poor health, limited income, and social isolation. Informed policy responses can help reduce both physical and mental health impacts for women, both during and after IPV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Australian Research Council, Discovery Projects Scheme (Project ID: DP130104437).