
Abstract
Approximately 50% of both men and women will experience emotional intimate partner violence (IPV) in their lifetime—a form of violence highly associated with other forms of IPV—making it important to develop further understanding of for assessment and treatment purposes. The bio-psycho-social model was used to guide the study. Utilizing data from 181 studies, yielding 348 effect sizes, we conducted a meta-analysis examining mental and physical health correlates with emotional IPV perpetration and victimization. We also examined if mental and physical health correlates were significantly stronger for emotional IPV perpetration or victimization, as well as if correlates were stronger for men or women. Suicidal ideation, post-traumatic stress, anxiety, depressive symptoms, borderline personality disorder (PD), psychological distress, physical pain, trauma, anger, shame, poor physical health, antisocial PD, and somatic symptoms were significantly associated with emotional IPV victimization. Borderline PD, narcissism, emotional dysregulation, anger, post-traumatic stress, antisocial PD, psychopathy, depressive symptoms, anxiety symptoms, and trauma were significantly associated with emotional IPV perpetration. Anger, emotional dysregulation, and psychopathology were stronger correlates for emotional IPV perpetration compared to victimization, and post-traumatic stress disorder (PTSD) and psychological distress were stronger correlates for victimization. PTSD and suicidal ideation were stronger correlates of IPV victimization for women than men, and anger was a significantly stronger correlate of IPV perpetration for women than men. This study highlights the importance of a holistic approach when working with victims and perpetrators of IPV, focusing on the importance of taking all aspects of the bio-psycho-social model into account.
Intimate partner violence (IPV) describes physical violence, sexual violence, or psychological harm by a current or former intimate partner or spouse (Smith et al., 2017). IPV is a serious public health crisis, as well as a violation to human rights (Campbell, 2002; Garcia-Moreno et al., 2006; Tjaden & Thoennes, 2000). IPV victimization is related to a host of negative consequences, such as depression, anxiety, post-traumatic stress, suicidal behavior, chronic pain, and injury (Campbell, 2002; Smith et al., 2017).
In this study, we focus specifically on emotional IPV. Emotional IPV includes nonphysical behaviors that are used to control, subdue, punish, or isolate another person by use of fear and/or humiliation (Engel, 2002). Emotional IPV can include insults, threats, yelling/screaming, emotional manipulation, and/or constant verbal put-downs or rejections. Emotional IPV is the most prevalent form of IPV experienced, with nearly 50% of both men and women reporting emotional IPV victimization in their lifetime (Black et al., 2011; Carney & Barner, 2012). Still, emotional IPV tends to receive the least amount of attention compared to physical or sexual IPV (Stern et al, 2019). Stern et al. (2019) also identified how a lack of understanding of emotional IPV can impact individuals’ perceptions of what constitutes emotional IPV, potentially impacting client or clinician ability to identify emotional IPV and utilize effective prevention protocols and responses.
Examining correlates of IPV perpetration and victimization can enhance our efforts to reduce and eliminate IPV. Knowledge of these correlates can help clinicians better identify when one may be at risk for IPV within their relationship. Due to the high prevalence of IPV and its association with a variety of issues, such as relationship dissatisfaction (Gewirtz-Meydan & Finzi-Dottan, 2021) and mental health problems (Rogers & Follingstad, 2014) that may lead someone to seeking services, it is essential that health professionals are aware of correlates of IPV and related assessment and treatment considerations. Fitzgerald (2020) found that women are more likely to report emotional IPV compared to physical and sexual IPV, making it critical for assessment purposes. Additionally, emotional IPV victimization is highly associated with other forms of IPV, such as physical IPV (Spencer et al., 2022), further emphasizing the importance of assessment for general violence intervention. The purpose of this study was to conduct a meta-analytic review examining the association between emotional IPV perpetration and victimization, and a variety of indicators of poor mental and physical health, in addition to examining the differences in the strength of these associations for gender (men vs. women) and direction of violence (perpetration vs. victimization).
Bio-Psycho-Social Theory
IPV is a serious health epidemic that is a contributing factor to traumatic physical injuries and mental health conditions for perpetrators and victims (Murphy et al., 2014). Understanding disease beyond diagnosis, to include the biological, psychological, and social facets of etiology, has revolutionized modern understanding of disease (Havelka et al., 2009). The bio-psycho-social model, a model that highlights the interaction and interconnection between biology, psychology, and social/environmental factors, has become an integral part of diagnosing and treating all mental health diagnoses (American Psychiatric Association, 2013). There is a clear connection between negative physical health symptoms and mental health symptoms, as well as environmental and contextual factors that can contribute to both physical and mental symptoms (Danese & Tan, 2014; Wittenberg et al., 2013). IPV can be viewed as a contextual factor associated with negative impacts on both biological and psychological factors for victims of IPV (Yim & Kofman, 2019), as well as a potential consequence of the stress associated with biological and/or psychological symptoms, such as emotional dysregulation related to mental health problems (Lee et al., 2020; Stith et al., 2008). Emotional IPV victimization has been linked to poor mental health outcomes, such as post-traumatic stress disorder (PTSD; Hegarty et al., 2013), anxiety (Shorey et al., 2012), depression (Gibbs et al., 2018), and suicidal ideation (Pico-Alfonso et al., 2006). IPV has also been associated with negative physical health outcomes for victims, such as overall poor general health, increased health service inquiry, stress-related conditions, physical injuries, chronic pain, reproductive disorders, poorer pregnancy outcomes, and even death (Murphy et al., 2014; Plichta, 2004). Overall, the bio-psycho-social model takes into consideration the interplay between biological, psychological, and social factors that may contribute to both mental and physical illness. We utilize this theoretical framework to examine the relationship between mental and physical health factors and emotional IPV.
Gender Differences in Mental and Physical Health Disorders
Extensive research has demonstrated gender differences in the prevalence of mental health rates and symptomology, supporting gender-focused treatment and prevention efforts. Women are more likely to be diagnosed with depression, generalized anxiety disorder, PTSD or borderline PD, while men are more likely to be diagnosed with antisocial PD or a substance abuse disorder (American Psychiatric Association, 2013; Eaton et al., 2012; Kuehner, 2003; McLean & Anderson, 2009; Tolin & Foa, 2006). Longitudinal data suggests these differences may start as soon as early adolescence (Hankin et al., 1998). There are also differences between gender in symptom presentation, with women showing a tendency toward internalizing symptoms and men tending toward externalizing more frequently (Eaton et al., 2012; Tolin & Foa, 2006). One study found these differences to be related to coping, noting that the women in their sample tended to ruminate more frequently on their problems and negative emotions than did men, while the men were engaging in active problem solving more often (Eaton et al., 2012). Another example is found in a study examining symptoms of borderline PD, where women reported higher levels of negative affect, feelings of emptiness, unstable relationships, and self-harm than men with the same diagnosis (Hoertel et al., 2014). In the same study, men were found to be more likely to report intense anger, impulsivity, and higher levels of avoiding abandonment than women.
Physical health is also abound with differences in rates and outcomes by gender, with studies showing these differences in areas like heart disease and failure, cancers, neurological diseases, and obesity, among many others (Regitz-Zagrosek, 2012). Although women’s life expectancy is increasing at a higher rate than men’s, research has found that women appear to experience higher rates of physical illness—a phenomenon referred to as the “gender paradox” (Gove & Hughes, 1979). While women are more prone to acute conditions and disabilities, men are more likely to be subjected to more chronic or debilitating conditions (Gove & Hughes, 1979). Due to the evidence suggesting that there can be gender differences related to mental and physical health conditions, we seek to identify if mental and physical health correlates for emotional IPV perpetration and victimization significantly differ between men and women.
Unique Contributions of the Study
There have been several meta-analytic studies examining the relationship between health correlates and IPV, yet none have directly examined the relationship between various mental and physical health correlates and emotional IPV perpetration and victimization. Several meta-analyses examining health correlates of IPV have been identified in the literature (Bacchus et al., 2018; Beydoun et al., 2012; Birkley et al., 2016; Buller et al., 2014; Devries et al., 2013; Golding, 1999; Oram et al., 2014; Spencer et al., 2019; Taft et al., 2011; Trevillion et al., 2012). However, some of these studies only focus on physical IPV and do not examine emotional IPV (e.g., Golding, 1999; Spencer et al., 2019). Other studies focused on IPV generally and did not specify type of IPV (e.g., Bacchus et al., 2018; Buller et al., 2014). Additionally, other studies only examined the relationship between IPV to a specific mental health outcome, such as depression (Beydoun et al., 2012) or PTSD symptoms (Birkley et al., 2016; Taft et al., 2011). Some studies also focused specifically on either IPV perpetration (Oram et al., 2014; Taft et al., 2011) or IPV victimization (Devries et al., 2013; Trevillion et al., 2012). Only one study has examined the relationship between mental health correlates and male perpetration, male victimization, female perpetration, and female victimization, but it only examined physical IPV and did not include emotional IPV (Spencer et al., 2019). To date, no meta-analyses have included information on physical health correlates for emotional IPV for both men and women.
The current meta-analysis builds on previous literature by providing a more extensive review of mental and physical health correlates for both perpetration and victimization of emotional IPV. Additionally, this study reports on the most extensive variety of correlates, including a host of mental health correlates (depressive symptoms, anxiety symptoms, post-traumatic stress symptoms, borderline personality disorder [PD], antisocial PD, narcissistic personality traits, emotional dysregulation, psychopathy, anger, trauma, shame, psychological distress, and suicidal ideation) and physical health correlates (physical pain, somatic symptoms, sexually transmitted infection, and general poor physical health). Finally, this study seeks to gain more information related to gender differences, as well as if there are different associations between perpetration and victimization for these correlates.
The Present Study
Examining physical and mental correlates of IPV perpetration and victimization can enhance our efforts to reduce and prevent IPV. Due to the high prevalence of IPV and its association with a variety of issues, like mental health and physical health problems (Campbell, 2002; Rogers & Follingstad, 2014), it is essential that physical and mental health professionals are aware of correlates of IPV. The purpose of this study was to conduct a meta-analytic review examining the association between mental and physical health factors and emotional IPV perpetration and victimization, as well as examining the differences in the strength of these associations for direction of violence (perpetration vs. victimization). Lastly, due to the potential gender differences in mental and physical health symptoms, we seek to examine if there are significant differences between men and women regarding mental and physical health correlates for emotional IPV.
Methods
Literature Search
Standard protocols were followed in order to identify studies to be included in the current meta-analysis (Borenstein et al., 2009; Card, 2012; Hunter & Schmidt, 2004). Database searches (Proquest, PsychInfo, Education Resources Information Center, Sociological Abstracts, Social Services Abstracts, and Proquest Dissertations and Theses) were utilized to identify original research articles, dissertations, and theses published between 1999 and 2019. The Boolean search terms used to conduct the search were related to emotional (emotional OR psychological OR mental OR verbal), abuse (abus* OR maltreatment OR violen* OR aggress* OR domestic violen* OR perpetrat* OR victim), intimate relationships (marital OR married OR spouse OR partner OR intimate OR dating OR relation* OR couple OR roman*), and correlates (correlat* OR path* OR risk marker OR risk factor OR predict* OR associat* OR relation). Database searches identified 31,321 studies for potential inclusion in the analysis.
Inclusion and Exclusion Criteria
Articles were included in the analysis if they (a) examined emotional IPV, (b) provided statistical information to calculate at least one bivariate effect size, (c) examined adult intimate partner relationships, (d) examined mental or physical health factors as correlates, and (e) were written in English. Articles were excluded from meta-analysis if they (a) did not separate types of IPV in their analyses/examine emotional IPV specifically, (b) did not provide quantitative data to calculate at least one bivariate effect size/were qualitative/were review articles, (c) did not examine adult intimate partner relationships (e.g., examined adolescent populations), (d) did not examine mental or physical health correlates for emotional IPV, or (e) were not written in English.
In the original search, we identified 31,321 studies for potential inclusion in the analysis. The first round of screening included abstract and title reviews, and if there was potential for the article to be included in the analysis, we included the article in the second round of screening. We included a total of 2,912 studies in the second round of screening, which included a full-text review of articles. There was a total of 1,272 duplicate studies, leaving 1,640 articles for further review. A total of 444 did not examine emotional IPV, 317 did not examine correlates for emotional IPV, 244 did not examine mental or physical health factors, 172 did not provide usable data, 152 were not quantitative, 65 did not examine IPV at all, 55 examined adolescent samples, and 11 were not written in English. This left a total of 181 studies, yielding 348 effect sizes, to be included in the analysis.
Coding Procedures
Procedures provided by Card (2012) were followed to collect pertinent information from all studies included in the analysis. A 23-item code sheet was created in order to collect data from each included study, including information on how data was collected, the sample size, sample characteristics, and demographic variables, how emotional IPV was defined, as well as the information needed to calculate at least one bivariate effect size. All studies included in the analysis were cross-coded by two separate researchers. Researchers achieved a 97.73% agreement rate on initial coding. When there were coding discrepancies, the lead researcher would meet with the two coders to discuss and collectively come to a consensus on the correct coding.
Analysis Plan
We used Comprehensive Meta-Analysis 3.0 (Borenstein et al., 2014) to enter the data from each study and run the analyses. The data was analyzed using a random-effects approach to account for true population differences between studies by accounting for both within-study and between-study variance (Borenstein et al., 2009, 2010; Card, 2012). This approach improves the generalizability of the findings compared to a fixed-effect approach. For each mental or physical health correlate found in at least three unique studies, an aggregate effect size (Pearson’s r) was calculated using the study as the unit of analysis. First, we measured the strength of the link between each mental and physical health factor and IPV perpetration, then again for IPV victimization for both men and women.
All meta-analyses are subject to the “file-drawer” limitation (Hunter & Schmidt, 2004), which means that there is a tendency for insignificant studies to go unpublished, leading to potential publication bias. This can potentially bias meta-analyses, as insignificant findings may not be able to be identified for inclusion in the analysis. To ensure the results were robust against potential publication bias, for each correlate that was found to be significantly related to emotional IPV and found in at least three studies, we employed two analyses: the classic fail-safe n (Rosenthal, 1979) and the trim and fill plot (Duval & Tweedie, 2000). The classic fail-safe n (Rosenthal, 1979) identifies the number of null studies that would be needed to make the association insignificant at the p < .05 threshold. This test is particularly helpful, as there is an explicit cutoff criterion for what is considered robust against potential publication bias, which is found by taking the number of studies included in the analysis, multiplied by 5, and then adding 10 to that number. If the classic fail-safe n is above that number, the finding is considered robust against potential publication bias (Rosenthal, 1979). Duval and Tweedie’s (2000) trim and fill plot identifies the number of studies that are theoretically missing to ensure that there is a symmetrical distribution of results on a funnel plot.
Next, we compared each factor on whether it had a stronger link with emotional IPV perpetration versus victimization by calculating a Q-statistic. A significant Q-statistic suggests that there is significant heterogeneity, or difference, between the two groups. We then utilized the same method to examine if there was significant heterogeneity, or difference, between men and women on correlates for emotional IPV victimization and emotional IPV perpetration.
Results
A total of 181 studies were included in the analysis. The total sample size from all studies was 195,749. Of the 108 studies that reported information on race and/or ethnicity of participants, 24,572 were White, 11,741 were Black, 3,958 were Hispanic or Latina/Latino, 3,541 identified as “Other,” 3,472 were Asian, and 1,377 were Native American or Alaskan Native. A total of 73 studies did not report on the race or ethnicity of participants. Samples included in the study came from 35 unique countries. The majority of the studies were from the United States (n = 107), followed by Spain (n = 16), Canada (n = 5), South Africa (n = 4), and the United Kingdom (n = 4). A total of 128 studies examined male perpetrators of emotional IPV, 44 examined both male and female perpetrators, and 9 studies examined female perpetrators. There were 131 studies that examined female victims, 43 examined both male and female victims, and 7 examined male victims of emotional IPV.
Emotional IPV Victimization
The strongest factor associated with emotional IPV victimization was suicidal ideation (r = .36, p < .001; see Table 1), followed by post-traumatic stress symptoms (r = .32, p < .001), anxiety symptoms (r = .30, p < .001), depressive symptoms (r = .28, p < .001), borderline PD (r = .28, p < .001), and psychological distress (r = .26, p < .001). Physical pain (r = .23, p = .035) and trauma (r = 0.19, p < .001) were also significantly associated with emotional IPV victimization. Physical pain was only examined in female samples. Anger (r = .18, p < .001) and shame (r = .16, p = .012) were significantly associated with emotional IPV victimization, but were not robust against potential publication bias, suggesting these results should be interpreted with caution. We found that poor physical health (r = .15, p < .001), antisocial PD (r = .13, p = .011), and somatic symptoms (r = .10, p = .020) were also significantly related to victimization, although antisocial PD and somatic symptoms were not robust against potential publication bias and should be interpreted with caution. Emotional dysregulation, psychopathy, and sexually transmitted infections were not significantly related to emotional IPV victimization.
Mental and Physical Health Factors Associated With Emotional IPV Victimization.
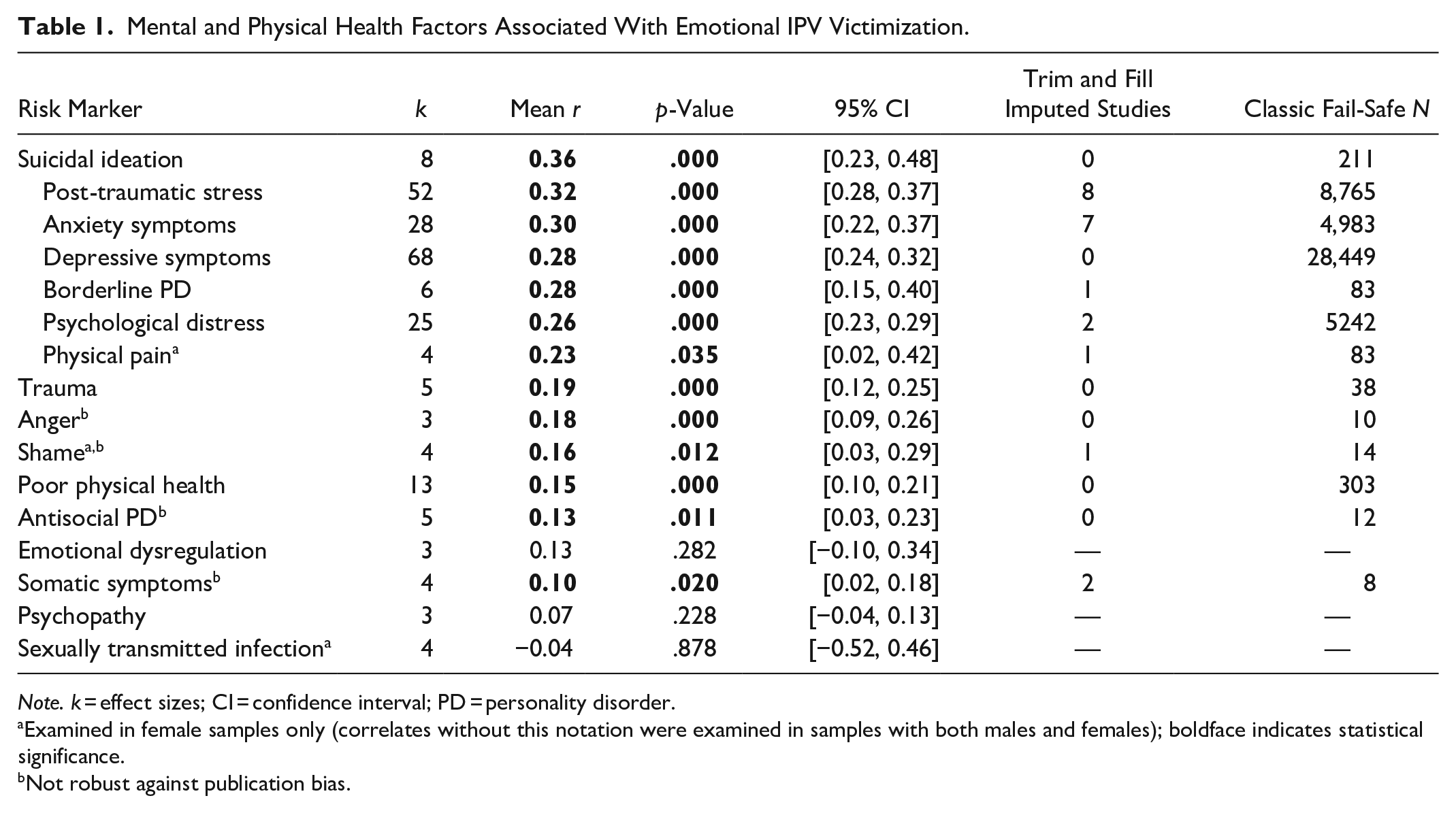
Note. k = effect sizes; CI = confidence interval; PD = personality disorder.
Examined in female samples only (correlates without this notation were examined in samples with both males and females); boldface indicates statistical significance.
Not robust against publication bias.
Emotional IPV Perpetration
The strongest factor associated with emotional IPV perpetration was borderline PD (r = .42, p < .001; see Table 2), narcissism (r = .41, p < .001), emotional dysregulation (r = .29, p < .001), anger (r = .27, p < .001), post-traumatic stress symptoms (r = .25, p < .001), and antisocial PD (r = .25, p < .001). Additionally, psychopathy (r = .23, p = .003), depressive symptoms (r = .23, p < .001), anxiety symptoms (r = .22, p = .007), and trauma (r = .12, p < .001) were significantly related to emotional IPV perpetration. Psychological distress was not significantly related to emotional IPV perpetration.
Mental and Physical Health Factors Associated With Emotional IPV Perpetration.
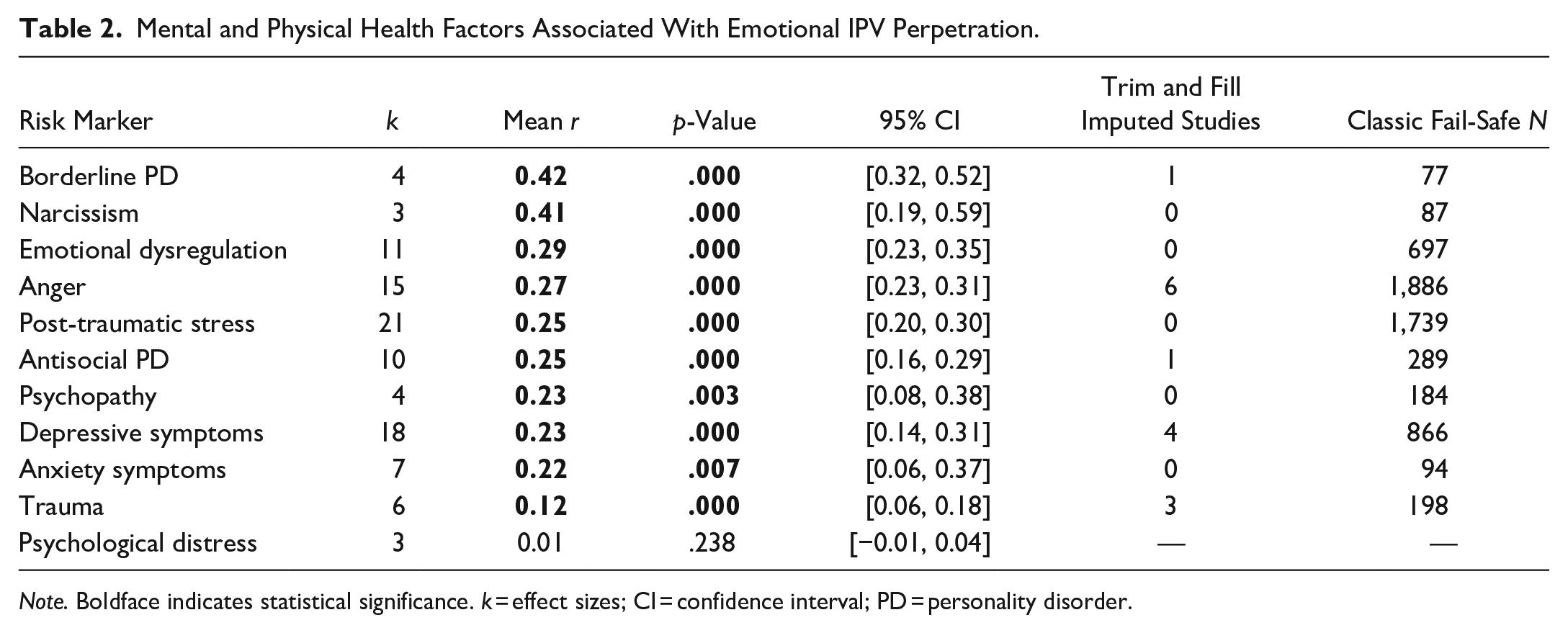
Note. Boldface indicates statistical significance. k = effect sizes; CI = confidence interval; PD = personality disorder.
Comparing Emotional IPV Perpetration and Victimization
A total of 10 factors were examined for both emotional IPV perpetration and victimization. The strength of the association with perpetration was compared to the strength of the association with victimization to see if factors significantly differed in their relationship with perpetration and victimization. We found that anger had a significantly stronger relationship with emotional IPV perpetration compared to victimization (Qb = 4.27, p = .039; see Table 3). It was also found that there was a significantly stronger relationship with emotional IPV perpetration compared to victimization for emotional dysregulation (Qb = 4.68, p = .030) and psychopathy (Qb = 8.65, p < .001). Post-traumatic stress symptoms (Qb = 4.00, p = .044) and psychological distress (Qb = 19.54, p < .001) had significantly stronger relationships with emotional IPV victimization compared to IPV perpetration. There were no significant differences for antisocial PD, anxiety symptoms, borderline PD, depressive symptoms, and trauma when comparing the strength of the relationships between emotional IPV perpetration and victimization.
Comparing the Strength of Mental and Physical Health Factors as Correlates for Emotional IPV Perpetration Versus Emotional IPV Victimization.
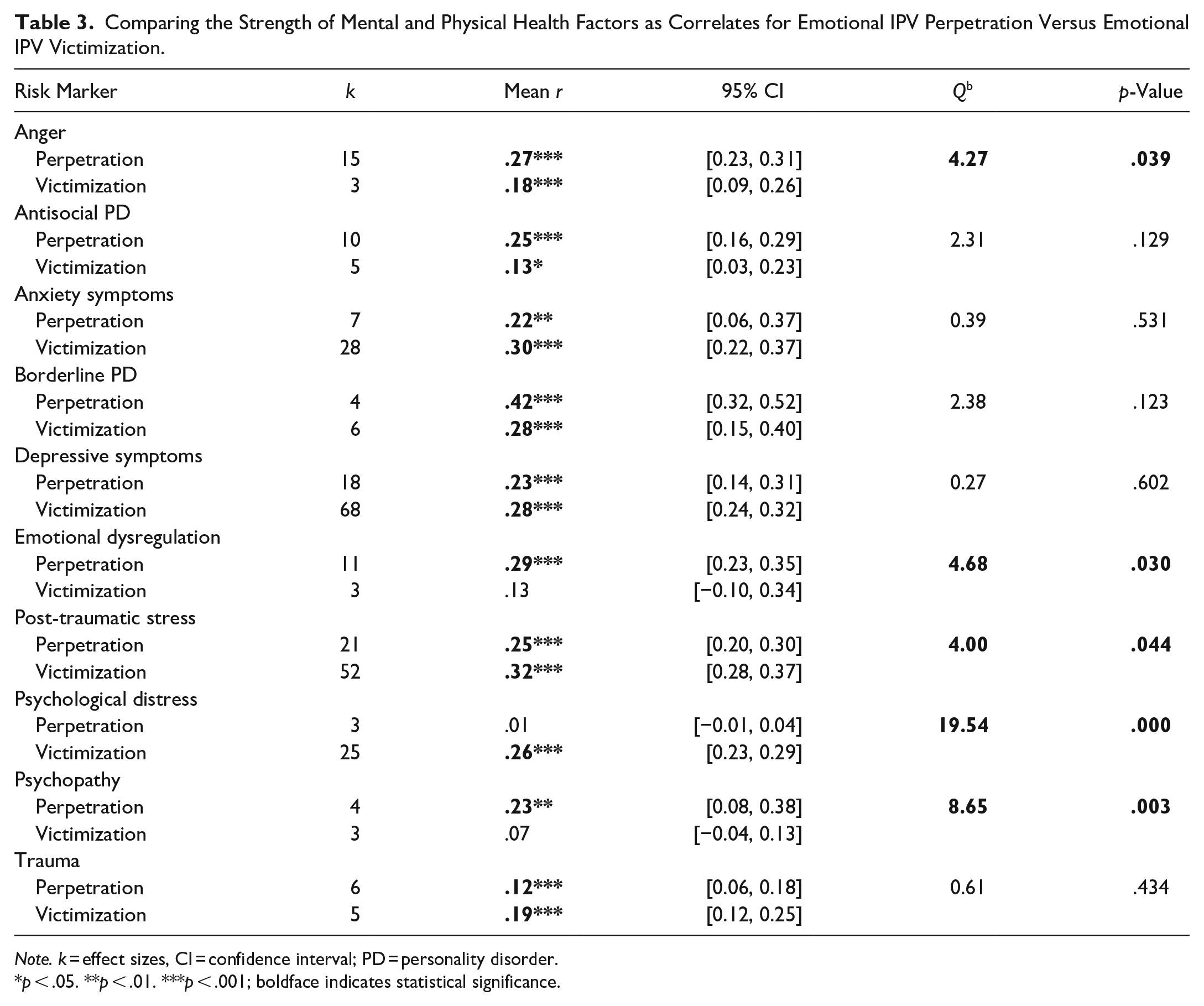
Note. k = effect sizes, CI = confidence interval; PD = personality disorder.
p < .05. **p < .01. ***p < .001; boldface indicates statistical significance.
Gender Differences
Post-traumatic stress (Qb = 4.31, p = .037; see Table 4) and suicidal ideation (Qb = 5.07, p = .024) had significantly stronger associations with emotional IPV victimization for women compared to men. There were no significant differences in anxiety symptoms, depressive symptoms, psychological distress, and trauma as correlates for emotional IPV victimization between men and women. Anger (Qb = 23.63, p < .001; see Table 5) was a significantly stronger correlate for emotional IPV perpetration for women compared to men. There were no significant differences in antisocial PD, anxiety symptoms, depressive symptoms, emotional dysregulation, post-traumatic stress symptoms, and psychological distress as correlates for emotional IPV perpetration for men and women.
Comparing the Strength of Mental and Physical Health Factors as Correlates for Emotional IPV Victimization Between Men and Women.
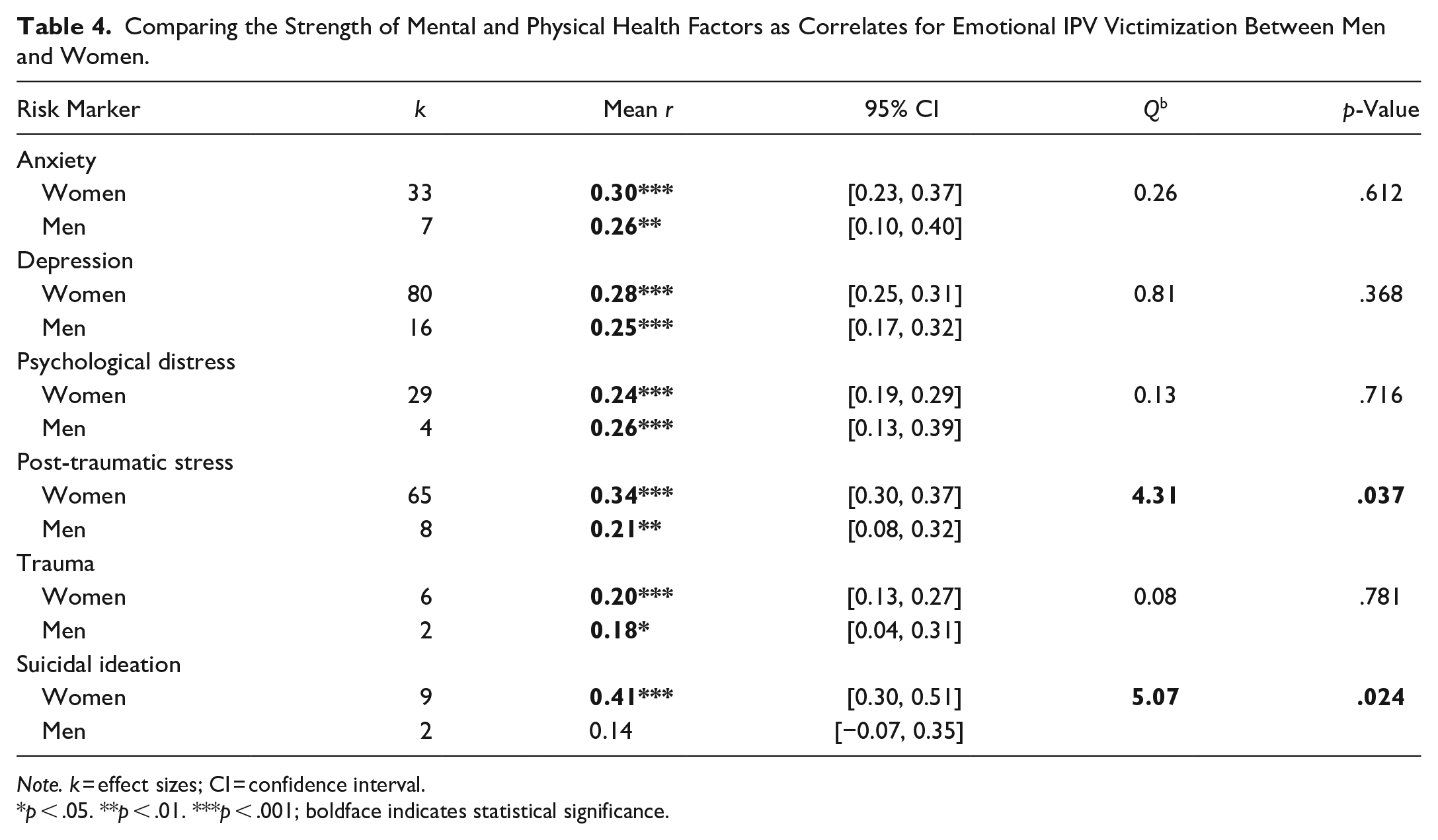
Note. k = effect sizes; CI = confidence interval.
p < .05. **p < .01. ***p < .001; boldface indicates statistical significance.
Comparing the Strength of Mental and Physical Health Factors as Correlates for Emotional IPV Perpetration Between Men and Women.
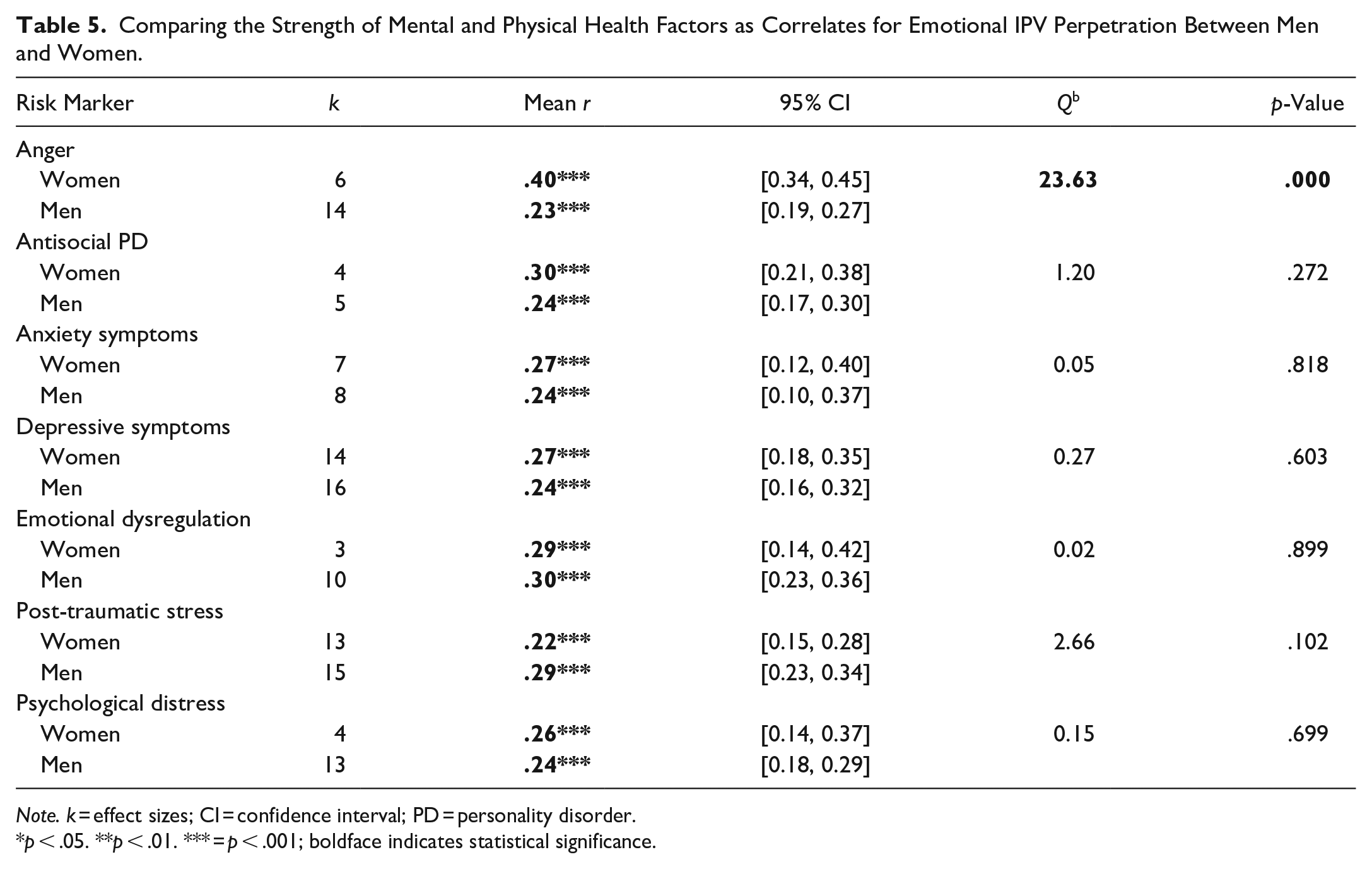
Note. k = effect sizes; CI = confidence interval; PD = personality disorder.
p < .05. **p < .01. *** = p < .001; boldface indicates statistical significance.
Discussion
Our study builds on a previous meta-analysis, which linked depression, anxiety, PTSD, antisocial PD, and borderline PD to physical IPV perpetration and victimization (Spencer et al., 2019), by examining how these diagnoses, as well as other indicators of poor health, relate to emotional IPV perpetration and victimization. To our knowledge, this is the first meta-analysis to date that examines both mental and physical health correlates of emotional IPV. Our meta-analysis identified significant associations between emotional IPV perpetration and victimization, and a range of factors related to poor health, providing further evidence for the connection between poor mental and physical health and IPV.
In addition to identifying mental and physical health correlates of emotional IPV perpetration and victimization, our study compared the strength of these associations between victimization and perpetration, as well as men and women. Anger, emotional dysregulation, and psychopathology were all found to be stronger correlates for emotional IPV perpetration, while PTSD and psychological distress were found to be stronger correlates for victimization. When comparing the strength of these associations between men and women, our meta-analysis revealed PTSD and suicidal ideation were stronger correlates of IPV victimization for women, in addition to anger being a significantly stronger correlate of IPV perpetration for women.
Our results found that, in order of strength, suicidal ideation, post-traumatic stress, anxiety, depressive symptoms, borderline PD, psychological distress, physical pain, trauma, anger, shame, poor physical health, antisocial PD, and somatic symptoms were significantly associated with emotional IPV victimization. This meta-analysis confirms previous research that depressive symptoms, anxiety, post-traumatic stress, and psychological distress are associated with exposure to emotional IPV (Lysova et al., 2019; Renner, 2009; Reuter et al., 2017). These findings also complement a recent meta-analysis that found depression, anxiety, PTSD, antisocial PD, and borderline PD are significantly associated with victimization of physical IPV for men and women (Spencer et al., 2019). Though our study examines correlates, and we cannot determine if these factors of antecedents or symptoms of emotional IPV, many of these factors are previously established as consequences of IPV victimization (Coker et al., 2002; Dutton et al., 2006). It may be that the IPV is a cause of the mental or physical health symptoms, or that emotional IPV victimization is exacerbating negative health symptoms.
We found that borderline PD, narcissism, emotional dysregulation, anger, post-traumatic stress, antisocial PD, psychopathy, depressive symptoms, anxiety symptoms, and trauma were significantly associated with emotional IPV perpetration. When utilizing the bio-psycho-social model, many of these mental health symptoms may create a context in which IPV perpetration may be likely to occur. For example, borderline PD has been linked with emotional dysregulation and impulsivity, narcissistic PD is connected to a lack of empathy for others, and antisocial PD is associated with aggression and impulsive behavior (American Psychiatric Association, 2013).
In addition to highlighting correlates that were significantly related to emotional IPV, it is also important to identify correlates with insignificant relationships with emotional IPV perpetration or victimization. Emotional dysregulation, psychopathy, and sexually transmitted infections were not significantly related to emotional IPV victimization. It is possible that emotional dysregulation and psychopathy are more related to perpetration than victimization (Lee et al., 2020; Tharp et al., 2012). It may also be that sexually transmitted infections would more likely be related to sexual IPV victimization, as sexual IPV victimization has been associated with HIV infections (Zhang et al., 2012). Psychological distress was not associated with emotional IPV perpetration. We did find a significant relationship between psychological distress and victimization, which may highlight that psychological distress is more strongly related to emotional IPV victimization than perpetration. It is important to note that although these factors were not significantly related to emotional IPV in the meta-analysis, it does not mean that they cannot be present in cases of IPV and still may warrant attention in treatment.
Comparing Perpetration and Victimization
Our study compared 10 correlates to assess if there was a significantly stronger relationship with emotional IPV perpetration or victimization. Notably, 50% of these correlates did show significant differences. Anger, emotional dysregulation, and psychopathy had significantly stronger associations with perpetration compared to victimization. Interpreting these results through a bio-psycho-social lens, anger and emotional dysregulation could be contributing to men and women being unable to control their physical or emotional arousal, thus leading to perpetrating emotional IPV against one’s partner. These could also occur within the context of an argument or conflict, where individuals may not be able to control their anger or reactivity, which suggests treatment modalities that include affect regulation or anger management skills may be useful for reducing or preventing emotional IPV perpetration. One example would be Stith et al.’s (2011) Domestic Violence-Focused Couples Therapy treatment approach, which is a supported treatment modality with components of affect regulation and mindfulness. Additionally, it is unsurprising that psychopathy was more strongly linked to emotional IPV perpetration than victimization, as psychopathy has been linked to various forms of IPV perpetration with medium effects (Mager et al., 2014) and is less likely to be a consequence of IPV victimization, as psychopathy has been considered to be stable over the lifespan (Loney et al., 2007).
Psychological distress and post-traumatic stress symptoms were more strongly linked to emotional IPV victimization compared to emotional IPV perpetration. Post-traumatic stress has consistently been identified as a consequence or symptom of IPV victimization (e.g., Campbell, 2002; Hegarty et al., 2013). When examining the development of PTSD, a key component is experiencing an adversarial life event, which could be experiencing abuse in one’s intimate relationship (Koenen, 2006). Psychological distress could also be viewed as a consequence of emotional IPV victimization, as well as a symptom of another mental health problem such as post-traumatic stress, depression, or anxiety.
Gender Differences
We were able to compare six correlates for emotional IPV victimization between men and women and seven correlates for emotional IPV perpetration between men and women. For emotional IPV victimization, two of the six correlates significantly differed, with post-traumatic stress and suicidal ideation being stronger correlates for emotional IPV victimization for women compared to men. This may be related to women suffering more severe symptoms following IPV victimization than men, which may be related to how mental health symptoms differ between genders, such as women experiencing more internalizing symptoms, or ruminating on negative emotions more frequently than men do (Eaton et al., 2012; Tolin & Foa, 2006). However, this may also be related to the context in which the emotional IPV occurs, specifically with lifetime victimization. One study found that, when accounting for lifetime exposure to violence, there were no differences between men and women on victimization and negative emotional and physical outcomes (Pimlott-Kubiak & Cortina, 2003). This is interesting, considering overall, women experience higher rates of IPV victimization in general (Black et al., 2011). Utilizing the bio-psycho-social framework, it is necessary to examine the development of negative mental health symptoms, which includes the relationship between lifetime and compounding victimization (and multiple forms of victimization) and negative mental health consequences.
This meta-analysis also found that anger was a significantly stronger correlate for emotional IPV perpetration for women than it was for men. Interestingly, research has found no gender differences related to experiences of anger (Zoccali et al., 2007). One review that examined women’s anger and aggression highlights that often women are not socialized to express anger in a healthy way and that women’s level of anger is strongly related to interactions with individuals closest to them (Thomas, 2005). This highlights the importance of social components in explaining the relationship between anger and emotional IPV perpetration, as women may not have experienced socialization of healthy expressions of anger, which may result in emotional IPV perpetration when experiencing conflict with an intimate partner. A holistic approach accounting for biological, psychological, and social interactions to help explain gender differences in correlates of IPV perpetration or victimization is needed to inform practice and intervention.
Clinical Implications
Consistent evidence supporting the association between poor mental and physical health and IPV perpetration and victimization makes IPV a relevant issue for all health providers. Whether someone is seeking services specifically for IPV or not, it is vital to assess for violence and monitor risk factors, recognizing that violence may be underreported or under-played. Individuals may feel more comfortable reporting emotional IPV compared to sexual or physical IPV (Fitzgerald, 2020), so it is essential for clinicians to be aware of what emotional IPV consists of and its impact.
Clinicians working with individuals or couples who are experiencing IPV and health concerns need to consider the influence of these experiences on one another to ensure appropriate treatment. If health issues are seen as a consequence of the abuse, IPV focused treatment, such as batterer intervention programs (Cheng et al., 2021), or couples-based treatment (Karakurt et al., 2016), may be appropriate. Additionally, research has found that when working with victims of IPV, treating depressive symptoms and PTSD through cognitive behavioral therapy (CBT) was found to reduce revictimization rates (Iverson et al., 2011). A recent meta-analysis examining the effects of brief interventions with IPV victims found that CBT-based programs specifically tailored to victims of IPV showed the largest effects in treatment success (Arroyo et al., 2017). This highlights the need to account for the social context (in this instance, IPV) that may be causing or exacerbating mental health symptoms during treatment. For situations where IPV is considered a consequence of the health condition, focus on and stabilization of the health issue with safety planning related to IPV may be appropriate.
The health correlates examined in this study may range in their severity, impact, and treatment outcomes, further impacting treatment considerations. While mood disorders have been found to be able to be lessened or eliminated over time and treatment, PDs have been found to be more persistent and impactful (Skodol et al., 2010), which may relate to why perpetrators with certain personality disorders, like borderline PD or antisocial PD, have been found more susceptible to recidivism post treatment (Llor-Esteban et al., 2016). This suggests that those experiencing chronic mental or physical health concerns may benefit from consistent IPV screening and preventative efforts. Further understanding of how IPV operates differently between various diagnoses (short vs. long term illness, physical vs. mental health) is needed to enhance our ability to accommodate for these differences, improving overall treatment.
In addition to the integral role of mental and physical health in IPV intervention efforts, it is also necessary to highlight the role of mental health treatment and support for IPV prevention efforts. Previous research has found that mental health treatment has been linked to a reduction in future IPV victimization among women who have experienced IPV in the past (Iverson et al., 2011). Additionally, community programming meant to prevent IPV has found a reduction in mental health symptoms, as well as a reduced likelihood of both IPV perpetration and victimization for men and women (Dunkle et al., 2020). It is important to include mental health treatment into IPV primary prevention efforts in the future (Gevers & Dartnall, 2014). See tables 6 and 7 for critical findings from the study and implications for future research and practice.
Review of Critical Findings From the Study.
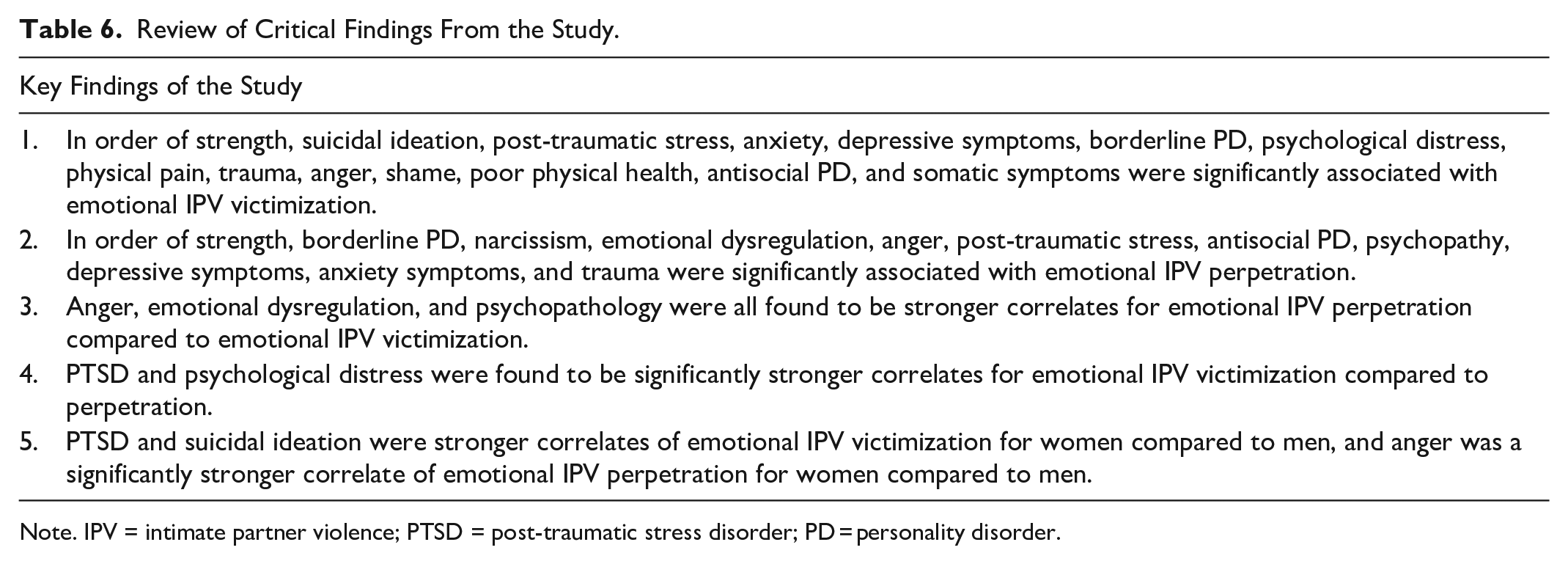
Note. IPV = intimate partner violence; PTSD = post-traumatic stress disorder; PD = personality disorder.
Implications for Future Research and Practice.
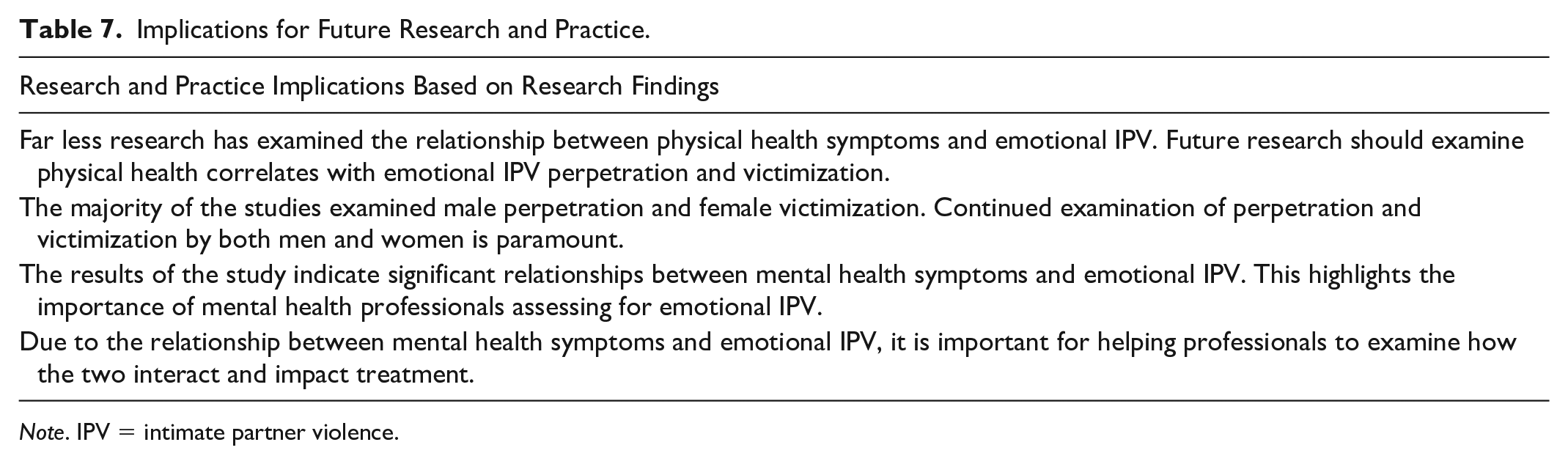
Note. IPV = intimate partner violence.
Limitations and Future Research
A limitation for all meta-analyses is the potential that studies for inclusion were missed or unidentified, and this is a potential for the current meta-analysis. In order to assess this limitation, we did conduct tests of publication bias. Several of our findings (the relationships between emotional IPV victimization and anger, shame, antisocial PD, and somatic symptoms) were not robust against publication bias and should be interpreted with caution. Another main limitation was the lack of articles identified that focused on specific correlates. For example, only three or four unique articles examined the relationship between emotional IPV victimization and physical pain, somatic symptoms, anger, emotional dysregulation, shame, sexually transmitted infections, and psychopathy.
Overall, far less research has examined the relationship between physical health symptoms and emotional IPV victimization, and we did not have enough data to meta-analyze the relationship between emotional IPV perpetration and any physical health symptoms. Future research should examine physical health correlates with emotional IPV perpetration and victimization in order to gain a greater understanding of the relationship between emotional IPV and physical health. Additionally, many of the studies focused solely on female victimization and male perpetration of emotional IPV. With approximately 50% of both men and women experiencing emotional IPV in their lifetime (Black et al., 2011), continued examination of perpetration and victimization by both men and women is paramount. Additionally, we did not find enough studies that examined other gender identities, and we were only able to examine differences between males and females. We also did not examine additional demographic factors in our analysis that may impact the relationship between emotional IPV and physical and mental health, such as race/ethnicity, age, sexual orientation, socioeconomic status, or ability. Future research would benefit from examining additional demographic factors to further enhance our understanding of the connection between emotional IPV and mental and physical health symptoms.
Conclusion
The current meta-analysis expands on previous literature examining the link between health and IPV by examining both physical and mental health symptoms, as well as focusing solely on emotional IPV, whereas previous meta-analyses have examined either physical IPV or all types of IPV together. The analysis identified top health correlates for emotional IPV perpetration and victimization and found that anger, emotional dysregulation, and psychopathology were stronger correlates for emotional IPV perpetration compared to victimization, and PTSD and psychological distress were stronger correlates for victimization. The analysis also revealed that PTSD and suicidal ideation were stronger correlates of IPV victimization for women than men, and anger was a significantly stronger correlate of IPV perpetration for women compared to men. The results of this study highlight the importance of utilizing a holistic approach, taking into account physical health, mental health, and social factors, when working with perpetrators or victims of IPV in a mental or physical health setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.