
Abstract
The COVID-19 pandemic has been harmful to survivors of abuse. Less understood is the impact on staff in the violence against women (VAW) service sector. Using interpretive description methodology, we examined staff experiences during the pandemic in Ontario, Canada, and found four core themes: (1) the emotional toll of the work; (2) remote (doesn't) work; (3) work restructuring; (4) efforts to stay well and subthemes nuancing staff experiences in a sector vulnerable to vicarious trauma. This research underscores the need to mitigate experiences of stress, heavy workloads, and guilt for staff in VAW services during crises and provides action-oriented recommendations.
Violence against women (VAW) continues to pose a threat to women's health and human rights worldwide. VAW encompasses many forms of abuse that are primarily targeted against women based on unequal, and gendered, power relations (Burnett, 2012; Burnett et al., 2016; Weldon, 2002). The United Nations Declaration of the Elimination of VAW defines VAW as any act of gender-based violence that results in or is likely to result in, harm or suffering to women and girls (Walby et al., 2017). Research has estimated that 25% to 33% of women will experience some form of VAW in their lifetime (World Health Organization [WHO], 2020; Wood et al., 2022). The wide range of negative physical and mental health consequences of experiencing violence and abuse is well established (Bacchus et al., 2018; Wood et al., 2022).
Rates of intimate partner violence and other forms of VAW increase during times of crisis (Kaukinen, 2020; Moreira & da Costa, 2020; Viero et al., 2021). One such crisis, the COVID-19 pandemic, began in early 2020 and has had global impacts related to virus transmission, economic hardship, lockdowns, stay-at-home orders, and distancing guidelines (Kaukinen, 2020; Moreira & da Costa, 2020; Viero et al., 2021; WHO, 2020). The United Nations predicted that VAW rates during the pandemic would increase by 20% due to lockdowns and stay-at-home orders (Viero et al., 2021) and preliminary data have confirmed this prediction. For example, media reports suggest a 10% to 50% increase in calls to domestic violence (DV) crisis lines globally during the initial stages of the pandemic (WHO, 2020). In Canada, staff at VAW agencies have reported increases in both the prevalence and severity of violence (Trudell & Whitmore, 2020) and a widely used DV crisis line in Ontario, the Assaulted Women's Helpline, fielded a 400% increase in calls in April 2020 (Women and Gender Equality Canada [WAGE], 2021). However, these estimates are likely conservative; mandatory lockdowns, stay-at-home orders, and physical distancing guidelines produced conditions that isolated women from their abusers, limiting their ability to seek help (Kaukinen, 2020; Viero et al., 2021; WHO, 2020; Women’s Shelters Canada [WSC], 2020).
While research on the negative impacts of the pandemic on women and children experiencing abuse proliferates (Abuhammad, 2020; Aguero, 2021; Ebert & Steinert, 2021; El-Nimr et al., 2021; Gosangi et al., 2021; Jetelina et al., 2020; Sanchez et al., 2020; Uzobo & Ayinmoro, 2023; Viero et al., 2021; Wood et al., 2022), less is known about the impact on staff working in VAW service organizations. VAW staff tend to report that their choice to work in this sector is influenced by the potential to make a difference in the lives of survivors (Bemiller & Williams, 2011; Wood et al., 2020). However, VAW staff also consistently report high rates of vicarious or secondary trauma and burnout, with agencies reporting high staff turnover (Dworkin et al., 2016; Kulkarni et al., 2013; Wood et al., 2019, 2020). Staff also face barriers to service provision during times of crisis or disaster that can have negative impacts, such as feelings of increased pressure to provide services and safety with limited resources (Enarson, 1999), a higher demand for services, and concerns related to safety and ability to work (e.g., if communications are impacted or buildings are unusable, etc.) (Sety et al., 2014). Given the importance of the work they do in supporting survivors (Moreira & da Costa, 2020; WHO, 2020), the impact of the pandemic on VAW staff themselves requires greater attention.
Research examining the impact of the COVID-19 pandemic on workers in VAW agencies is still emerging. Carrington et al. (2020) investigated the impact of the pandemic on 362 Australian workers from a variety of DV agencies through a mixed-method online survey conducted in the early days of the pandemic (from June to August 2020). They found that 52% of staff felt more pressure throughout the pandemic, 52% felt isolated while working from home, 44% faced difficulties with remote work, and 17% felt they were unable to meet the demands of the work. Staff also reported increased fear for women stuck at home with their abusers with limited access to resources. To proactively prepare for the next potential crisis, staff advocated for further training and funding for technology use, as well as more or better equipment to support those working from home (Carrington et al., 2020).
Two studies conducted in the United States (U.S.) sought to better understand staff needs related to negotiating COVID-19 pandemic guidelines. Nnawulezi and Hacskaylo (2022) analyzed qualitative data from an online meeting of 840 VAW service providers (held in March 2020 and hosted by the National Alliance for Safe Housing). Service providers felt they were balancing their clients’ needs and their own potential health risks, concerns about navigating labor shortages (e.g., if staff got sick), workload changes, and job security or reductions in hours (Nnawulezi & Hacskaylo, 2022). Additionally, Wood et al. (2020) conducted an online survey of 352 staff working in VAW agencies. The majority of participants (95%) reported increased stress related to the virus and new pandemic guidelines that changed the way the work was done, such as new ways to connect with clients (e.g., video conferencing), and concerns about working remotely (e.g., maintaining confidentiality, feeling disconnected from colleagues, and lack of adequate equipment). Most (81%) reported that they were deemed “essential” workers, validating the importance of this work and qualifying some staff for hazard pay, whereas only 5% of staff faced job loss or reduced hours due to the pandemic (Wood et al., 2020). In both studies, participants felt that staff required more support, suggesting better communication across and within agencies, and further assistance with managing stressors or self-care (Nnawulezi & Hacskaylo, 2022; Wood et al., 2020).
To date, two studies conducted in Canada have assessed the impact of the COVID-19 pandemic on the VAW services sector using quantitative surveys. WSC (2020) surveyed workers at 251 shelter and transitional homes across Canada who reported changes during the pandemic related to staffing structures, additional tasks for staff (e.g., cleaning), reduced capacity at shelters, and the use of alternative spaces that made providing quality care more difficult. Two-thirds (67%) felt guidelines limited their ability to provide services to clients and 82% used virtual services with varying perceptions of effectiveness. About half (52%) also reported that when remote work was used, it had a negative impact on service delivery, such as having fewer staff on-site to support clients. Lastly, staff reported fears for women who were isolated at home with their abusers, as they saw an initial decrease in calls for accessing shelter space (WSC, 2020).
Trudell and Whitmore (2020) conducted an online survey from May to July 2020 with 376 VAW staff and volunteers across Canada, including management, residential and outreach counselors, and social workers. Participants reported that the pandemic created barriers for women to access services, such as living with an abusive person or a lack of sufficient technology or skills. Further, some felt guilty about having to turn clients away due to reductions in space. Participants shared fears about personal health risks with continuing to work, the potential of spreading the virus to family members or coworkers, confusion about public health directives, additional workloads (e.g., cleaning), and an inability to forge meaningful connections with clients due to distancing guidelines. Of those who worked from home, some reported a blurring of their work-home lives with their clients’ trauma entering their homes, issues maintaining privacy, a lack of connection to other workers or agencies, and inadequate access to equipment and skills to effectively work remotely. Additionally, 25% of managers reported having to lay off workers and 9% of staff had reduced hours. Overall, 81% felt more stress due to the pandemic, yet most (80%) also felt that despite the challenges of the pandemic, their workplace promoted the health and safety of clients and staff (Trudell & Whitmore, 2020).
The above primarily survey-based research conducted within the first few months of the pandemic shows that VAW staff working during the pandemic have faced additional pressures, stressors, service changes, and struggles with remote work. Given that those who work with highly traumatized clients are vulnerable to burnout and vicarious trauma (Dworkin et al., 2016; Kulkarni et al., 2013; Wood et al., 2019, 2020), we felt it important to understand staff experiences in greater depth and beyond the initial months of the COVID-19 pandemic. The current research, drawing on in-depth qualitative interviews, examines the experiences of staff and Executive Directors (EDs) in the Ontario VAW sector during the later months of the ongoing COVID-19 pandemic, including how staff felt the pandemic impacted their work, clients, and personal well-being. The research is framed by a unique methodological framework that combined interpretive description (ID) to analyze and situate findings for practice and policy application, and a partnered, integrated knowledge mobilization (KMb) approach that allowed for the co-construction of evidence-based key messages and action-oriented recommendations.
Methods
Overview
Data used in the current paper were part of a larger study on the impact of the COVID-19 pandemic on the VAW sector in Ontario, Canada, more broadly. In Canada, addressing VAW is primarily a provincial or territorial responsibility with some directives coming from Public Health and varying social service ministries (Government of Canada, 2021). The study took place between June and October 2020 and consisted of interviews with 8 woman-identified clients of VAW agencies, interviews with 26 staff members from VAW agencies, and 5 focus groups with 24 EDs of VAW agencies. This paper draws on data from the focus groups and staff interviews specific to staff experiences. The one-on-one telephone interviews with staff members averaged about 1 hour and were conducted by the study interviewer. The focus groups were conducted by phone or over Zoom, were an average of 2 hours, and were facilitated by a lead team member who led the discussion, and a co-facilitator who monitored the discussion, contributed questions to further explore ideas, and took field notes. All interviews and focus groups were recorded, professionally transcribed verbatim, de-identified, and checked for errors.
Data collection and analysis were conducted using ID, a methodology that emphasizes contextualizing findings in social, cultural, historical, and political environments (Thorne, 2016; Thorne et al., 2004). ID is a practice-based framework that highlights the possibility of multiple perspectives of reality and the importance of the co-construction of knowledge between researchers and participants (Thorne, 2016; Thorne et al., 2004). An integrated KMb approach (Kothari & Wathen, 2013, 2017) was also used to ensure that actionable messages were generated by and for the VAW sector in addressing the impact of the COVID-19 pandemic. A more in-depth outline of the methods for this research is presented in Mantler et al. (2021).
Participants
Participants for the staff interviews were recruited through flyers and an email call to organizations, via sectoral list-servs, to circulate study information to staff and other agencies. Focus group participants were recruited through purposive snowball sampling, where EDs involved in the project referred other organizational leaders who were then invited to participate via email. All 26 interviewed staff members self-identified as women. All staff were employed at women's shelters across Ontario in various roles, including residential counseling (54%), sexual assault (15%), outreach counseling (8%), and support (i.e., food, cleaning, etc.) (4%) and had first-hand experiences of changes in the work, services delivery, and service demand. The majority of staff (65%) were employed on a full-time basis and 15% were relief or casual. About a quarter of the sample (23%) reported working remotely during the pandemic. Finally, none of the participants indicated having been directly exposed to the COVID-19 virus while at work.
All focus group participants were EDs of VAW or related agencies that served women experiencing violence (e.g., counseling and victim services), with the majority (58%) located at women's shelters. EDs are uniquely positioned to provide insight into how the work changed during the pandemic and how this impacted their staff from a leadership perspective. The 24 EDs served a range of community sizes, with 42% at rural agencies and the remainder in urban settings. Only two EDs (8%) identified their agencies as serving primarily Indigenous clients. The majority of EDs self-identified as women (83%), held an undergraduate bachelor's degree or higher (92%), and were an average age of 48 years.
Coding and Analysis
ID and KMb allowed for an iterative, reflexive, and dynamic data analysis process. A preliminary codebook was developed by the research team; it initially included broad, general codes, which were refined through an iterative process of coding and discussion.
The core coding team included seven people, and each transcript was coded using Quirkos (2020, Version 2.4.1), specialized qualitative data management software, by two people randomly assigned to each transcript. Each person first coded their assignments independently using line-by-line coding and then met with the other person to discuss the process and any suggested changes to the codebook. The evolving analysis was reviewed and discussed by the core coding team until all interview and focus group data were coded, after which the research team synthesized the data into larger themes. Finally, Quirkos data files were merged to compile coded data from all research team members into one file per data set.
The coding of staff and ED data led to the development of themes related to the impacts of the COVID-19 pandemic on staff in the VAW sector, which are presented below. Researchers ensured that quotes and themes represented a variety of participant voices and experiences.
Ethical Considerations
The project was approved by Western University's Non-Medical Research Ethics Board (Protocol #115865). Informed verbal consent was obtained from each participant prior to data collection and numeric codes were assigned to ensure confidentiality.
Findings
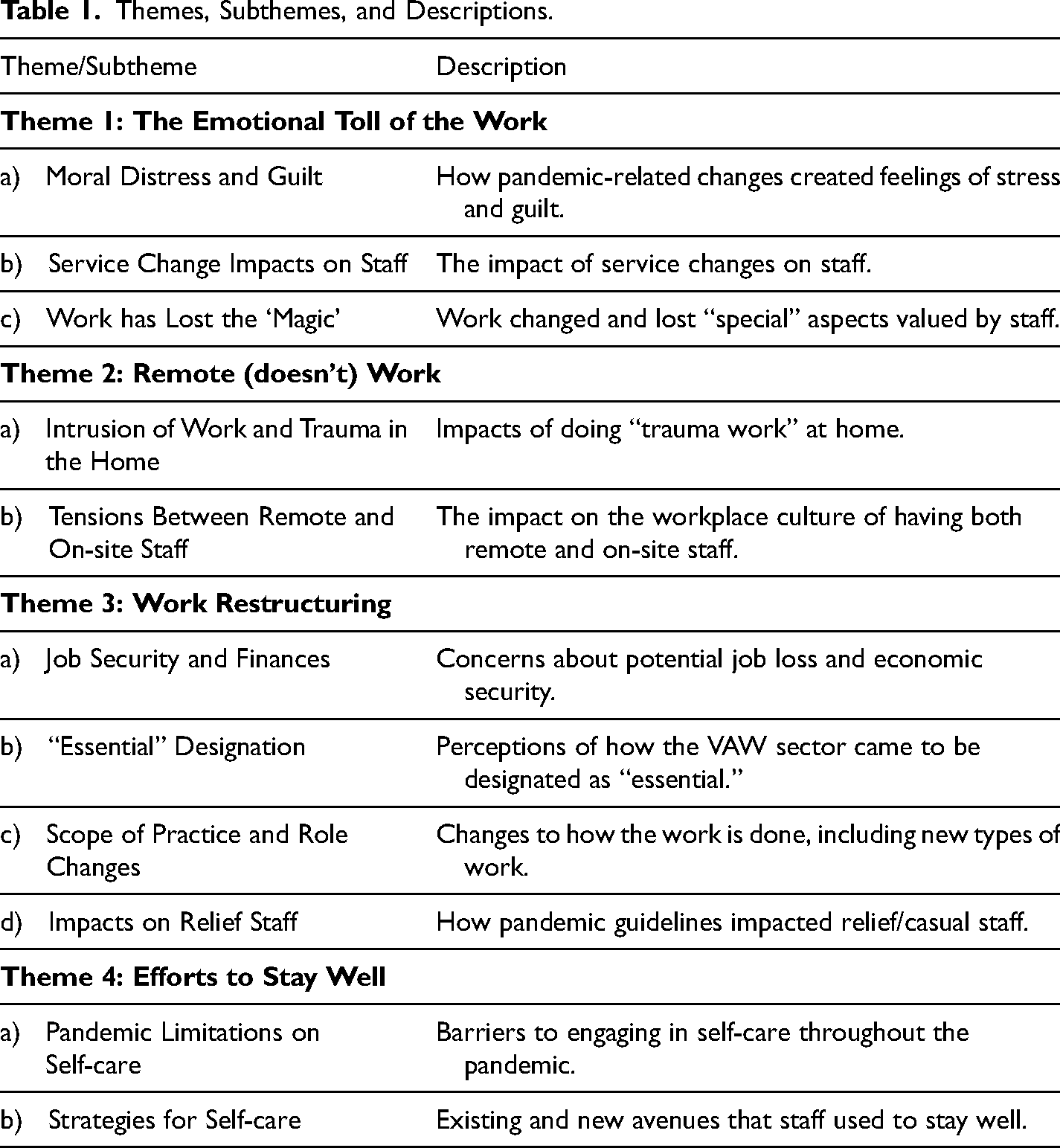
Four core themes specific to staff experiences, each with two to four subthemes, were identified from interview and focus group data. These themes, subthemes, and their descriptions are detailed in Table 1.
Themes, Subthemes, and Descriptions.
The Emotional Toll of the Work
I think just the impact on the staff I think was a lot more than people would think it would be, right?… It was extremely stressful to work through COVID. (Staff (S), ID125)
An important impact of the changes wrought by the COVID-19 pandemic was the emotional toll experienced by staff serving clients who were facing significant and immediate trauma due to their violence experiences, exacerbated by the uncertainty and disruption caused by pandemic-specific and -related changes. This was articulated in three main ways, as follows.
Moral Distress and Guilt
Participants shared concerns that initial decreases in the number of calls to their agencies meant that women were not able to reach out for help and may be suffering abuse in isolation. However, when women did reach out, staff felt the impact of limitations on the number of available shelter beds due to public health guidelines for communal spaces in residential services. Many staff reported feelings of guilt when receiving calls from women in unsafe situations and not having a bed to offer or not knowing where to refer women because pandemic guidelines meant significant changes in community resources. Being able to help fewer women and having less resources to refer women to led to staff fearing for women's safety. Further intensifying these fears, some staff noted that they were receiving more intense calls, with women who were sometimes unable to speak freely if their abuser was in the home, which led staff to fear for women who may not be able to reach out for help in the future.
Additionally, many staff reported that part of the increased emotional impact of the pandemic came from ever-changing service mandates that narrowed the scope of practice, especially within organizations’ residential services. These changes left staff with feelings of moral distress and guilt about their inability to help clients or potential clients not meeting the “severity thresholds” (i.e., those who were at low or moderate risk) now required for shelter, but still at risk of violence and its impacts. One staff member stated, … it feels too like we need to be sticking to our mandate so much more because [of] the severity of the calls we get… if [women are] calling, they’re calling because there's nothing else for them to do. So, we almost need to be protective of the beds that we do have, to make sure that we have them available for women of really high risk… (S110)
Service Change Impacts on Staff
Intertwined with the issue of moral distress, some staff members reported feelings of helplessness or hopelessness related to their ability to provide needed levels of service. Extended lockdowns meant that usual care strategies within and outside the shelter—from how to interact with women to how to get them safe housing or addictions or mental health support—were evolving daily. One staff member explained, I want to help people and I felt that I was letting a lot of people down based on our crisis line and people calling in for space. Everywhere in the city being full, having nowhere to house people… it feels hopeless when you’re talking with somebody and you have nothing to offer them… because every resource has been exhausted. (S118)
On top of this, staff reported that the pandemic led to limitations regarding the flexibility they could offer clients, something they normally would prioritize, and this led to feelings of inefficiency. Staff at agencies that were using alternative spaces, like motel rooms, to adhere to public health guidelines that reduced shelter beds, tended to report concerns with flexibility and safety. For example, motels offered less flexibility for meeting client needs off-site, reaching women to work on a housing plan or provide support, and developing rapport. Motels also did not have the same safety mechanisms in place as the shelter (for additional findings specific to motel use, see Mantler et al., 2021).
There were conflicting accounts, however, when it came to perceptions of the intensity of the workload. Some staff reported feeling the effects of reduced capacity in shelters; one (S102) said, “It's [about] ‘butts in seats’ [e.g., number, or lack, of people in the shelter]. You can kind of walk around the building… So, yeah. I read a lot of books and I read a lot of blogs and look at a lot of photography and try to… stay present and not be too bored.” In contrast, other staff felt that the work remained busy and active, particularly for those who were navigating remote work and trying to connect virtually or by phone with clients.
Work has Lost the “Magic”
Participants were clear that their choice to enter the VAW sector was motivated by a desire to do good work, connect with clients, and make a difference. Despite the potential for vicarious trauma from exposure to extensive client trauma histories, staff indicated that there were parts of the job that made it all worth it, such as being able to support women and children through difficult times, eating meals with families, watching children to give moms a break, and hugging women and children. The pandemic, however, put a strain for some staff on the things that would usually bring them joy in their job. Staff were dealing with multiple losses related to how pandemic guidelines changed their work, such as physical distancing guidelines that prevented them from meeting with women in offices and masking guidelines that made staff feel like they were unable to forge meaningful connections with clients. One staff member lamented the loss of some of the personal aspects of the jobs that she was missing, I don't like the way the work's changed… I’m a people person, I love talking with the women, I love spending time with the women and children, and that has really diminished. Like, I can't hold the baby, I can't go in and just say, “Hey, give me your baby for an hour so you can go take a nap.” I can't do any of that. (S125)
However, staff attempted to reclaim some of the “magic” that the pandemic and related guidelines stripped from their work by using clever workarounds, such as having distanced meetings outside. In other cases, EDs reported that staff rejected the use of personal protective equipment (PPE) guidelines altogether to prioritize making connections with clients.
Remote (Doesn't) Work
While more staff were working from home, the VAW sector was faced with determining how, if at all, “trauma work” (i.e., working with women and children experiencing or fleeing abuse) could effectively be done remotely. As noted previously, the majority of staff in the current study were not able to conduct their work from home. For those who were able to work remotely (23% of shelter staff), significant barriers to working from home were reported.
Intrusion of Work and Trauma in the Home
Staff experiences of working remotely were nuanced in ways that highlighted the complexity of this sector and the benefit of clear boundaries between work and home life. Staff indicated that working from home was, in some ways, positive as it allowed them to safely continue important work with women and children experiencing violence. However, staff also consistently reported that working from home had many negative, unanticipated consequences on their home lives, such as upsetting the balance they had struck between their personal and professional lives. Participants working remotely reported difficulty in letting the complex or difficult cases go once their workday had ended as it felt like the work, and the trauma, remained inside of their homes. One staff member shared her perspective that shifting to working from home altered the level of comfort she felt in her personal spaces, I was working in my sunroom because it was light and it was a nice space, [but] I abandoned that because it just… didn't feel good anymore… I didn't want my workspace to be a place where I enjoy—like used to really enjoy kind of just relaxing in because it just blended too much together… your workspace [needs] to be your workspace. And then your other places in your home need to be like your sanctuaries. (S101)
Additionally, some remote staff felt unable to disconnect from the work (e.g., always answering emails, management and EDs always feeling “on-call,” etc.) and they felt isolated from their colleagues with less ability to discuss difficult cases, debrief, and receive support.
There were also concerns about the logistics of working from home, such as having proper equipment, having to buy equipment without reimbursement, having or finding dedicated office spaces, and technological skills required to conduct their work virtually. Concerns about challenges related to maintaining confidentiality and privacy while working from home were common. For example, staff who also had children at home during the pandemic had to navigate maintaining confidentiality for clients while also attending to children's needs. Remote staff shared some of the workarounds they used to ensure confidentiality was maintained, such as using sound machines to mask conversation, and/or having locks on office doors.
Tensions Between Remote and On-site Staff
Finally, decisions about who was able to work from home and questions about how working remotely impacted the work led to some tensions between those who could work remotely and those who remained on site. The division of staff between on-site and remote work limited the connection and support that all staff could receive from their colleagues at a time when daily changes were wearing hard on staff. Some on-site staff shared feeling abandoned by staff who were working remotely and expressed feelings of loneliness being on site without their colleagues. At the same time, staff working from home reported similar things, such as feeling isolated from their colleagues and feeling guilty about not being on-site with their teams.
Some staff reported feeling angry and frustrated that while their workload increased on-site with additional tasks, such as cleaning duties and meal delivery, they perceived remote staff having less work to do. Further, staff felt frustration with remote staff who did not seem to have what they needed to complete their work, further adding to the workloads of on-site staff who did additional tasks to support their remote colleagues. This led to some staff feeling like those working remotely were “slacking off” or off-loading their responsibilities, as this participant said, We’ve had a few calls from some of our people working at home saying, “I’m working from the cottage and I don't have a printer or internet, can you do this, that and the other thing for me?” And I’m like, “Oh that must be rough, being at the cottage working from home.” (S108)
One ED summed up the mixed impact of remote work on the culture of their workplace, And as time went on—and we’re going to have to repair this over time—there really is sort of this two solitudes of culture where those that, you know, for lack of a better term, were doing the work in front of the clients every day had it hard… and feeling a little bit like the people at home were slacking off, even though the people at home were doing work and in some cases being more productive at home… (Focus Group (FG), ID 203)
Work Restructuring
The pandemic presented other concerns for staff related to how the work was organized, how changes were communicated and understood, and how or when the VAW sector was recognized by the government as an “essential” service.
Job Security and Finances
As in many service sectors during the pandemic, VAW staff were worried about the potential for job loss or reduced hours and feared that COVID responses would mean austerity and restructuring within the sector. A few staff members felt that management could have communicated more clearly about whether layoffs would be happening, particularly among remote workers who felt “out of the loop” of the day-to-day work in the shelter. Despite the fear of some staff that layoffs might be coming, many staff members felt their managers were clear in communicating that layoffs were off the table and that staff who needed to take time away from work would be supported in doing so. However, behind the scenes, management and EDs were also feeling uncertainty related to sufficient staffing levels and funding that did not align with new realities during the pandemic. One stated, I don't feel that we have the time to give [staff time off] because one thing is the commitment to service, another thing is… maintaining [staff's] jobs, and my own job too. And what we saw with funding was—depending on where your funding comes from… if you closed because you needed time to regroup… you weren't funded anymore. (FG202)
Some staff were faced with decisions about continuing to work or opting for government subsidies that supported those who were unable to work during the pandemic for a variety of reasons. Facing cuts in hours due to the pandemic and concerns about their personal health and financial stability, some staff chose to take a leave of absence and receive the Canada Emergency Response Benefit (CERB), a government subsidy for those whose work was impacted by the pandemic. This decision, however, was not made lightly, as staff felt that rules about repaying CERB were not clearly laid out, making this decision risky. Some reported resentment toward those who opted to take CERB instead of continuing to work as this left more work for the remaining staff to do and fewer options for coverage if staff needed to take time off.
“Essential” Designation
For the VAW sector, uncertainty about layoffs and service closures came with additional worries, such as wondering how clients would be supported throughout the pandemic if VAW services, including shelters, were restricted or forced to close. This led to some questions about the delay in designating VAW staff as “essential” workers by the provincial and federal governments, a designation that qualified them for pandemic pay top-ups but also highlighted the importance of work in this sector and the need for VAW services to remain open during the pandemic. At the same time, staff raised questions as to whether pandemic pay was enough, as one staff member (S115) noted, “… am I only worthy of $4 hazard pay?” Additional questions arose about which workers qualified for pandemic pay; managers and EDs noted that they did not receive top-ups because they primarily were able to conduct their work from home. While managers and EDs acknowledged their ability to work remotely, they also felt that by not qualifying for pandemic pay, their work or role was deemed less valuable.
Scope of Practice and Role Changes
For those who continued to work on-site during the pandemic, there were significant changes to their roles. On-site counselors at shelters reported that while their jobs were once focused on supporting women to understand their experiences and develop the next steps for safety and healing, their days were now filled with additional tasks like cleaning, cooking, or meal delivery. One staff member discussed how these changes impacted her, I actually despise that now we’ve got to do this disinfecting list during the day and then at night time, on our midnight shift you have to do – clean every room… I didn't go to school to become a f***ing cleaner, that's why I went to school so I could get out of cleaning, which I was doing. (S111)
Participants also noted that they were spending more time on the phone, attempting to complete things like housing applications that would typically take much less time. Keeping up with changes related to COVID-19 and other resources was also a new part of their job, such as determining which organizations were open or what their hours were. Some staff developed strong relationships with workers at other agencies to ensure the lines of communication about operations remained open and to continue supporting clients as best they could.
A few participants also reported that their policies related to harm reduction and substance use had to change to align with pandemic guidelines that encouraged people to limit outings as much as possible. This posed some tensions for staff who, to limit potential exposure to COVID-19, now facilitated the safe use of substances within the shelter, something they would normally encourage and support clients to do off-site. One staff member (S115) explained necessary policy adaptations due to the impact of outing limits for substance-involved clients, “We used to have a strict no marijuana and like no substance use on property and it came down to us… turning into a ‘wet’ shelter where if a resident was suffering with alcoholism we had to work with them to provide alcohol.”
Impacts on Relief Staff
Staff consistently said that relief staff members, who usually do not have set hours, tended to be overworked during the pandemic because they were relied on to cover time off for full- and part-time staff. In some cases, relief staff reported working up to 44 hours or more per week, well beyond the usual hours of full-time employees. There was increased pressure, from the perspective of relief staff, to be available for shifts, both to maintain hours for their own support and to be seen as reliable by their colleagues. However, being constantly on-call, coming in for last minute shifts, and working long hours took a toll on relief staff, as this participant said, But, if you’re working 44 hours a week at a women's shelter, with women who are severely traumatized and children who are severely traumatized, during… a global pandemic [laughs], where… all the staff you’re working with are traumatized. Like, sometimes it's just—it's not worth it to take the shift. (S105)
To add to their experiences, both relief and regular part-time and full-time staff identified that relief workers do not qualify for benefits or paid time off. Although they were heavily relied on to take shifts, without access to paid time off to recharge, some relief staff questioned whether their roles within the agency or their personal well-being were as valued as those of full- or part-time staff. Participants consistently felt that relief staff needed to be entitled to some form of benefits, sick time, or paid time off, both during and after the pandemic, to have the resources to adequately take care of themselves.
Efforts to Stay Well
Managing personal well-being is not something new for staff who work with clients who have experienced severe trauma. However, the pandemic presented a unique circumstance where staff in the VAW sector, much like other sectors, had to find new ways to engage in self-care.
Pandemic Limitations on Self-Care
A number of participants felt their regular self-care activities were hindered by pandemic guidelines. For example, staff who regularly exercised or did other forms of physical activity (e.g., yoga) were unable to partake in this kind of self-care due to mandatory closures of nonessential businesses, which included fitness centers. Spending time with family and friends, a valued form of self-care, was also limited by COVID-19 gathering restrictions, particularly for participants who did not live with their loved ones. One stated, I have a partner but I couldn't – we don't live together, so I couldn't see him for three months. That was very hard. And because being where I worked, in the shelter, was obviously a risk to him and [he] at the time was working from home and obviously then like we weren't, you weren't allowed to see people outside of households… I didn't really have the resources to take care of myself. (S106)
Many participants felt they were balancing their own safety and that of their friends or family with their need for informal support. Even those who were able to have physically distanced meetings with their supports indicated that because they were not able to hug or enter each other's homes, the support wasn't the same.
Strategies for Self-Care
Many participants reported that despite pandemic limitations, they were able to use some reliable sources of self-care that adhered to public health guidelines. As noted above, some staff were able to lean on informal supports such as family and friends, within pandemic guidelines, to keep themselves grounded. Staff found new ways to connect with these supports that adhered to physical distancing guidelines, such as meeting outside and distanced, or using Zoom and other virtual platforms to connect. One participant (S107) indicated that her friends encouraged her to be creative in finding ways to connect, “… it was my extrovert friends that were saying, ‘Is there anything going on this weekend?’ And I was like, ‘Well you can come over and sit in my driveway if you want.’” Some also reported engaging in more at-home self-care activities, like meditation, yoga, exercise, nature walks, and gardening.
At work, some staff were able to have regular check-ins with managers or colleagues in person, over the phone, or virtually, and this was a valued form of self-care during the pandemic. Staff also noted the importance of using work benefits, if they had them, or doing counseling on their own as a normative strategy for self-care during the pandemic.
Taking time off was perceived as an important tool for self-care but also something that caused feelings of guilt and resentment. Some participants reported feeling encouraged and supported by other staff and management or EDs to take the time they needed away from the work so that they could come back recharged and ready to support women and children. One ED shared that their agency went further in supporting staff needs by instituting new policies that expanded what time off looked like, We created new days off for people… we also allowed people to opt-out of working. We couldn't pay people to be off unless… they had COVID or they were getting tests or whatever that was, but if [they] just were like I’m out, I don't feel comfortable, they would be entitled to their job whenever this was over. (FG202)
However, some staff reported feeling resentment toward colleagues who took time off and a lack of support as they felt they couldn't take time off if there was no one to cover their shifts. These staff members felt there was some unfairness related to who got to take time off and when and what it meant for shelter staff who may then have to work short-staffed if another coworker needed to take time off (e.g., if they got sick).
Particularly for management and EDs, there were concerns about what taking time off meant for their workloads in the future, since no one covered for them when they were away from work. This meant that time off wasn't relaxing or a time to recharge but, rather, was filled with anxiety about what the work would look like when they returned. Some staff members reported being impacted by managers or supervisors taking time off because they felt that leaders should be there to guide them through the pandemic. At the same time, managers and EDs who needed to take time off reported some feelings of guilt about not being there to support their workers, even if they needed to take time off as a legitimate form of self-care.
Discussion
Jobs in the VAW sector are associated with increased potential for burnout, exposure to violence and trauma, and vicarious trauma (Dworkin et al., 2016; Kulkarni et al., 2013; Wood et al., 2019, 2020). The findings of this study illustrate that such day-to-day impacts of working to provide care for women and children experiencing violence were exacerbated in multiple ways by the COVID-19 pandemic. It is important to note that our findings are contextualized within a sector that is gendered; the majority of staff and ED participants identified as women. The COVID-19 pandemic has undoubtedly had an immense impact on staff in services that are traditionally female-dominated, such as nurses and personal support workers. Emerging research has demonstrated that women working in healthcare during the pandemic have experienced high levels of stress and burnout (Sriharan et al., 2020) and nurses have experienced increased stress and risk of posttraumatic stress disorder (Sharour & Dardas, 2020). Further, research so far shows that women face economic hardship from the pandemic, including job loss or reduced hours (Sampson et al., 2021), and hardship associated with providing caregiving support in the home on top of other obligations (Hazarika & Das, 2020). This research highlights the importance of acknowledging the gendered impact of COVID-19. The findings of the current study expand current knowledge by exploring the compounding impacts of serving highly traumatized clients, along with new, COVID-specific, stressors.
We found that staff felt the impact of the pandemic itself, changing pandemic guidelines, and concerns about the virus in a variety of ways. First, public health guidelines for congregate living spaces reduced capacity in shelters and altered shelter mandates to prioritize the highest risk cases when staff were seeing more severe reports of abuse. Consistent with the previous literature, this led staff to feel that they were unable to serve clients across the usual spectrum of needs, and were afraid for women and children who were isolated with their abusers (Carrington et al., 2020; Trudell & Whitmore, 2020; Wood et al., 2020; WSC, 2020). In tandem, community resources changed their hours of operation and methods of contact, which caused stress for staff who were trying to support clients. Staff were worried about the potential for layoffs, and that they might lead to closures of essential services that women needed during the pandemic, such as shelters and counseling. Some conflicting research has emerged regarding job security, as Wood et al. (2020) found that only 5% of VAW staff lost their jobs due to the pandemic, in contrast with Trudell and Whitmore’s (2020) research suggesting that 25% of leadership reported layoffs. However, most staff in the current study reported that they were reassured their jobs were secure and necessary, highlighting the importance of VAW services and the need for these services to continue during the pandemic. Staff noted a need for better communication and collaboration between agencies in the social sector, especially during the pandemic, a finding noted in recent research (Nnawulezi & Hacskaylo, 2022).
COVID-19 guidelines also changed the way that staff could do their work due to PPE and distancing rules, shifts to remote work, and changes in their roles that prioritized meal delivery and cleaning over counseling and case management. These changes lead to frustration as staff tried to provide flexible support, and develop creative workarounds to support clients. Previous research has found similar results, such as staff feeling unable to meet the demands of the work or the needs of clients during the pandemic as workloads increased and spaces were restricted (Carrington et al., 2020; Trudell & Whitmore, 2020; WSC, 2020; Wood et al., 2020). Interestingly, in the current study, some staff felt their workloads increased while others reported a sense of boredom, causing them to question the value of their work during the pandemic (i.e., feeling like a seat filler, rather than a counselor), something that other research has not yet documented. Our finding that the work had lost its “magic” where staff felt the rewards of the work were diminished due to not being able to meet with clients in-person was also found in Trudell and Whitmore’s (2020) research. These findings highlight how the pandemic not only altered what staff did, but also their perceptions of the work itself, such as its value.
The need to do what we’re terming “trauma work” from home had additional unintended consequences beyond the ability to provide flexible support to clients. One recent study has documented some positive aspects of remote work, such as being able to alternate schedules and swap workers if someone became ill (WSC, 2020). However, for participants in the current study, working from home was framed as not ideal for such core tasks as debriefing or connecting with colleagues, developing rapport with clients, maintaining privacy and confidentiality, and separating the emotional impacts of the work and their home spaces. In line with the current study, recent research has clearly documented that staff working remotely during the pandemic felt isolated from their colleagues (Carrington et al., 2020; Trudell & Whitmore, 2020; Wood et al., 2020) and a lack of work and personal life separation (Trudell & Whitmore, 2020; Wood et al., 2020). While disruptions to work-life balance may have been a common experience for any worker adapting to working from home, the feeling that the trauma of their work was invading their home, we argue, is unique to the VAW sector and other helping professions. A novel finding of the current research was the division created between remote and on-site staff. This division undermined aspects of the work environment that staff were used to, such as leaning on one another for support, debriefing, and working as a team, and damaged relationships between workers that they felt would need to be repaired over time.
There were several structural level changes that were designed to provide support to VAW workers during the pandemic, however, the unequal application of these changes led to varied experiences for staff. While the government was acknowledging “essential” staff in sectors across the country, the recognition of VAW workers was delayed about a month, at least in Ontario (relative to other work roles). This left many staff feeling like their work, their personal health and safety, and their clients’ experiences were devalued; no research to date has explored the impact of being deemed “essential” or delays in receiving this designation. In line with recent research (Carrington et al., 2020; Nnawulezi & Hacskaylo, 2022; Trudell & Whitmore, 2020), staff in this sector had to balance concerns related to their own personal safety from COVID-19 with wanting to continue to provide service to their clients. Government subsidies, like CERB, were created with the intention to support workers who were unable to continue working during the pandemic. However, staff in the current study shared difficulties with deciding whether to take CERB to prioritize their health and safety (i.e., not work) or continuing to work, a dilemma that has not been documented in other research. This was an important consideration since the choice of some staff to stop working impacted service delivery for clients (e.g., not enough staff on site), and remaining on-site staff (e.g., lack of shift coverage that prevented time off or a lack of on-site support that was integral to their work). With a limited staff complement for various reasons, relief staff felt pressure to be available for shifts, sometimes last minute, with little to no support from formal benefit packages or time-off allowances. This novel finding is contextualized by research that has explored the precarity of relief staff's employment in the VAW sector (Seifert et al., 2007), while also highlighting exacerbated feelings of stress and trauma that relief staff felt working long hours during the COVID-19 pandemic.
Lastly, in a sector where self-care is central to mitigating the impact of vicarious trauma and burnout, the pandemic caused staff to change the way they attended to their own well-being. Previous research has shown that VAW staff value support from their workplace in developing good self-care strategies (Nnawulezi & Hacskaylo, 2022), managing their stress (Wood et al., 2020), and developing a coping plan (Carrington et al., 2020). Staff in the current study consistently reported the importance of prioritizing their self-care during the pandemic and many showed tenacity and creativity in finding ways to keep themselves well that fit with pandemic guidelines, such as distanced meetings with supports and engaging in physical activities (i.e., yoga, nature walks) from home or outside. Taking time off and using formal benefit packages were valued strategies for staying well that were encouraged by managers and EDs, though, as noted above, not all staff had equal access to these resources.
Limitations and Future Research
The current study was conducted from June to October 2020, with most data collected by the end of August. This captured a short period of time when the second wave of the pandemic had crested in Ontario and then eased somewhat, but before vaccines were widely available. Whether experiences shifted over time with subsequent waves, the roll-out of vaccines and changes in the potential for staff to be exposed to COVID-19 at work is not known. It is also unknown how our findings generalize to other regions across Canada, and beyond, given that our sample included only staff and leadership from VAW residential settings in Ontario.
Recommendations
Several action-oriented recommendations based on the experiences and perspectives shared by staff and EDs are presented below. Overall, our findings highlight the need for VAW staff to be considered “essential,” for “trauma work” in the shelter and through outreach to be recognized as valuable and necessary and for greater awareness of the difficulties that staff face in serving clients, especially during times of crisis. Ongoing preparedness efforts (e.g., updating crisis plans) are necessary for the VAW sector to limit impacts of crises (pandemics or otherwise) on services and staff.
First, we recommend that policy actors and funders ensure that clear and consistent guidance, as well as effective communication, are maintained with the VAW services sector. In addition, decision-makers should work closely with this sector during times of crisis to ensure changes do not fundamentally alter effective service delivery. Second, in acknowledging the interconnectedness of community services for survivors, the potential impact of service restrictions and closures across the VAW sector should aim to reduce pressure on staff and enhance their capacity to help women and their children. Improved information-sharing between sectors and services (e.g., hours and services available) is a high priority.
Third, if remote work is required for staff in this sector, they need appropriate workspaces that promote safety, privacy, and physical well-being, as well as additional training and resources (such as secure laptops), to effectively work from home. Fourth, leadership in VAW agencies must ensure that decisions, such as those related to remote work or job security, are communicated clearly and transparently. Leadership should also be available on-site, as public health guidelines allow, and/or remain in close contact with their staff to assess ongoing impacts, including on staff well-being. Fifth, minimizing additional tasks, where possible, such as cooking, cleaning, or meal delivery, would reduce pressure on staff to meet the increased demands of working during a pandemic. Finally, we recommend that efforts be made to validate and encourage the use of multiple forms of self-care, including providing counseling service/employee assistance plans and encouraging time off for all staff, especially those in casual or relief roles, and for management or EDs.
Conclusion
The pandemic changed the way that work with women and children experiencing violence was done, and this impacted how staff felt about their ability to support clients. Overall, staff reported extra stressors due to COVID-19-specific and -related changes to their work, and limitations to their regular self-care strategies, which exacerbated the potential for negative outcomes, including stress, moral distress, feelings of disconnection from clients and colleagues, and vicarious trauma. We strongly recommend that the experiences of staff in this sector be considered when developing future pandemic/crisis plans, with a key goal being to support staff in navigating their mental health and well-being during and after a crisis. VAW staff consistently advocate for their clients and work toward the elimination of violence; that same level of care and support should be consistently and equitably extended to all workers in this sector.
Footnotes
Acknowledgements
We sincerely thank our partnered agencies in Ontario, Canada: Anova in London, Women's Rural Resource Centre in Strathroy, Optimism Place in Stratford, Women's Interval Home of Sarnia-Lambton, Faye Peterson House in Thunder Bay; all agencies who participated in the recruitment of participants, and Drs. Eugenia Canas, Susan Rodger, and Victoria Smye.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada (Connection Grant/611-2020-0204) and Western University (Catalyst Grant/49301). Wathen is funded by an SSHRC Canada Research Chair in Mobilizing Knowledge on Gender-Based Violence. For more information, visit: ![]()