
Abstract
Black transgender women are disproportionately affected by violence and poor care-delivery, contributing to poor mental health. Little is known regarding the effect of transgender and gender diverse (TGD) community connection (TCC) on health. This analysis (a) explores relationships between TCC, polyvictimization, and mental health and (b) analyzes how TCC influenced help-seeking following violent experiences among Black transgender women. Mixed-methods data from 19 Black transgender women were analyzed using correlational and thematic content analyses. Findings suggest that TCC is associated with improved help-seeking and mental health among Black transgender women, highlighting a need for longitudinal research to identify approaches for leveraging TCC.
Introduction
Transgender and gender diverse people (TGD; people whose gender differs from what is normatively expected of their assigned sex at birth) face threats of violence in their daily lives, predicated by historical and present-day societal oppression related to gender minority status. For Black transgender women, gender oppression is intertwined with racial oppression, thereby amplifying their risk for polyvictimization (i.e., experiencing multiple forms of violence, sometimes concurrently, throughout the lifespan) above other groups (Graham, 2014; Koken et al., 2009; Singh & McKleroy, 2011). The effects of polyvictimization vary in presentation, duration, and severity, and survivors often seek help for coping with the mental effects of violence, in addition to other emergent needs. Potential helpers may include people who occupy formal (e.g., law enforcement officers or case workers) and informal (e.g., friends or relatives) roles. However, it may be difficult for Black transgender women to ask for assistance from the institutions and individuals known to perpetrate violence against them (White Hughto et al., 2017; Wirtz et al., 2020). Therefore, accessing help from people within their TGD community may allow Black transgender women who are survivors of polyvictimization to gain tailored support based on peers’ similar experiences with discrimination and/or violence (Suitor et al., 1995). In this article, TGD community is referring to TGD people in a person’s immediate self-defined community (e.g., neighborhood, city) and the larger collection of TGD people (e.g., online, internationally, nationally) that they access or to whom they experience an emotional connection. To further elaborate, TGD community connection—defined as (a) a sense of emotional belongingness (emotional TGD community connection) and (b) behavioral participation with the TGD community (behavioral TGD community connection)—may help mitigate the negative effect of experiences of violence on mental health for Black transgender women (Pflum et al., 2015; Sherman, Clark, et al., 2020). Yet, the lack of inclusion of Black transgender women in research exploring the linkages between TGD community connection, help-seeking, and mental health limits our understanding of help-seeking and recovery in those who have survived violence.
Polyvictimization, Gender, and Race
There is a paucity of research exploring the prevalence of polyvictimization between and within gender diverse groups. Generally, what has been found thus far suggests that violence exposure and polyvictimization are common among TGD people (Pflum et al., 2015; Sterzing et al., 2017, 2019). Specifically, a disturbingly high prevalence of childhood abuse, gender-based violence, school-based violence, intimate partner violence, and hate crimes have been documented among TGD population samples (Reuter et al., 2017; Rodríguez-Madera et al., 2017; White Hughto et al., 2017; Wirtz et al., 2020). One recent study found polyvictimization rates among TGD youth (aged 14–19 years) to be nearly twice that of cisgender sexual minority peers (Sterzing et al., 2017, 2019). Gender-based differences in polyvictimization scores comparing cisgender and TGD people highlight the injurious effects of gender discrimination on TGD health. Additional existing inequities between Black transgender women and non-Black TGD people emphasize the deleterious effects of intersectional racism and gender oppression (Dinno, 2017).
In a Huffington Post essay, businesswoman, entertainer, and transgender rights advocate, Angelica Ross, stated, “being trans comes at a high cost, but being Black and trans can cost you your life” (Ross, 2015). In just a few words, Ross poignantly summarizes how the intersection between anti-Black and anti-transgender violence (defined as “transmysogynoir”) endangers Black transgender women (Krell, 2017). Accordingly, research examining Black transgender women’s experiences with stigma (e.g., discrimination) reports pervasive victimization from multiple sectors of society (Graham, 2014; Koken et al., 2009; Nemoto et al., 2011). The limited literature which compares violence between Black transgender women and other TGD people supports Ross’s statement, showing a significantly (a) higher risk of violence exposure among Black transgender women compared to their White peers and (b) higher risk of homicide among Black transgender women compared to transgender men and gender diverse peers of the same race and White transgender women (Dinno, 2017; Reuter et al., 2017). For example, in a prospective study of lesbian, gay, bisexual, transgender, and queer (LGBTQ+) young adults, researchers found significantly elevated levels of verbal and physical intimate partner violence among Black and TGD youth (Reuter et al., 2017). United States (U.S.) studies of homicides have similarly found that risk of intimate partner violence and homicide vary significantly by ethnicity (higher for Black v. non-Black) and sex assigned at birth (higher for male v. female at birth), with the highest rates among Black transgender women (Dinno, 2017; Reuter et al., 2017). The existing scholarship and activism surrounding violence inequities among Black transgender women are crucial to raising awareness of the physical threats faced by this community; however, more remains to be known about the mental and emotional toll of polyvictimization exposure among racial minority transgender women.
Mental Health—Depression and Post-Traumatic Stress Disorder
There is a high prevalence of depression and post-traumatic stress disorder (PTSD) among TGD people compared to the general population (Kessler et al., 2009; Kilpatrick et al., 2013; Nuttbrock et al., 2014; Reisner et al., 2016; Sherman, Poteat et al., 2020; White Hughto et al., 2017). Nuttbrock et al. (2014), reported an incidence of depression five times higher among TGD participants assigned male at birth than the general population and a prevalence of lifetime depression symptoms at 55% (Eaton et al., 1997; Kessler et al., 2003; Nuttbrock et al., 2014). PTSD has been largely understudied among TGD people (Valentine & Shipherd, 2018); however, one study of transgender women found a significantly higher prevalence of symptoms of PTSD compared to transgender men and an overall prevalence (44%) significantly higher than the general public (10%; Kilpatrick et al., 2013; Reisner et al., 2016). Victimization (Nuttbrock et al., 2014; White Hughto et al., 2017) has been associated with mental health disorders among TGD people; however, associations with polyvictimization have been understudied (Sherman, Poteat et al., 2020; Sterzing, Ratliff et al., 2017). One study of TGD and cisgender sexual minority youth (aged 14–19 years) suggested that higher levels of post-traumatic stress were associated with greater adjusted odds of being polyvictimized in the last year (Sterzing et al., 2017). Another study with Black and Latinx transgender women found that polyvictimization was associated with increased symptoms of depression and PTSD (Sherman, Poteat et al., 2020). The deleterious effects of victimization on mental health are well-documented, and research with transgender women of color presents compelling evidence of how combined transphobia and racial discrimination destabilize mental health through psychological abuse (Jefferson et al., 2013; Nemoto et al., 2011). Nevertheless, the potential impact of modifiable factors, such as help-seeking and transgender community connectedness, on the relationship between polyvictimization and the mental health of this community have yet to be explored.
Help-Seeking
Help-seeking is defined by the steps that people take to solicit resources from others (Gourash, 1978). After an experience of violence, survivors may need help with fulfilling a range of needs including securing safe housing, filing a police report, and coping with mental distress. Yet, the process of seeking help can be complicated by intrapersonal, interpersonal, and structural barriers (Kaukinen, 2002; McCart et al., 2010). For example, Black transgender women in crisis may wish to seek help from friends, family, and members of their community (informal sources), as well as more formal sources such as health care providers and police (Lytle et al., 2018). However, fear of transphobia, social isolation, and a lack of community resources can prevent them from doing so (Calton et al., 2016; Guadalupe-Diaz & Jasinski, 2017).
Among victims of violent crimes, help-seeking from law-enforcement and other formal support sources is universally low (Kaukinen, 2002; McCart et al., 2010). The National Crime Victimization Survey reported that despite a trend of increasing violent-crime victimization, less than half (43%) of violent crimes were reported to police in 2018 (Morgan & Oudekerk, 2019). While, cisgender violence survivors report fear of retaliation from the perpetrator as a barrier to seeking help from legal authorities (Calton et al., 2016), Black transgender women may additionally avoid the criminal justice system to minimize risks for further victimization or “misarrest” (Calton et al., 2016; Guadalupe-Diaz & Jasinski, 2017; Irvine, 2014; Mohamed, 2015). For example, a research-community partnership in New Orleans found that Black transgender people were among other racial and ethnic minority groups who were four times more likely to experience police harassment compared to cisgender peers (Irvine, 2014). Black transgender women may also be excluded from seeking asylum from violence shelters, which typically restrict admission to cisgender women only (Greenberg, 2012; McCart et al., 2010). Moreover, institutionalized stigma, discriminatory treatment, and medical expenses may constrain help-seeking from health providers (Calton et al., 2016; White Hughto et al., 2017).
Data show that victimization survivors are more likely to seek help from informal networks, consisting of kin and friends (McCart et al., 2010). One study found that slightly less than a quarter (22%) of victimization survivors sought help from informal sources, while nearly an equal proportion sought help from the police (23%; Kaukinen, 2002). By encouraging people who have been victimized to seek formal help, informal helpers such as family or friends are pivotal to brokering support from resource providers and law enforcement agencies. Family members also serve as a source of comfort in the midst of adversity (Calton et al., 2016; Morgan & Oudekerk, 2019). However, familial rejection is common among transgender women with a sizable proportion who report feeling estranged from their families (Greenberg, 2012; Koken et al., 2009; Riggs & Toone, 2017; Wirtz et al., 2020). Help-seeking from family can also be deterred by previous experiences of violence from family (Koken et al., 2009). Collectively, the above factors may severely restrict the availability of safe and reliable helpers that Black transgender polyvictimization survivors have at their disposal. Nonetheless, there is strong evidence that suggests that LGBTQ+ and TGD-specific networks have the potential to provide multidimensional support for navigating barriers and coping with the distress resulting from adversity (Graham, 2014; Pinto et al., 2008; Riggs & Toone, 2017).
TGD Community Connection
Social and emotional integration within LGBTQ+ and TGD-focused networks may provide Black transgender women with the protection and motivation to seek help both from informal and formal resources. TGD community connection is a term used to define the degree of behavioral and emotional attachment that a TGD person has to a gender-focused network. Seminal theory on social integration explains how embeddedness and intimacy within networks shape socio-behavioral pathways, ultimately impacting health (Berkman et al., 2000). As a form of social integration which bonds TGD people to one another, TGD community connectedness (TGD community connection) may influence help-seeking behaviors among polyvictimization survivors while also facilitating psychological adaptation (Kawachi & Berkman, 2001; Pflum et al., 2015; Sherman, Clark, et al., 2020). A study on emotional transgender community connectedness with TGD feminine spectrum people (including women, transgender women assigned male at birth, and gender diverse people assigned female at birth) found that emotional transgender community connectedness was associated with fewer symptoms of depression and anxiety (Pflum et al., 2015). It is likely that Black transgender women who have survived polyvictimization will reap the same psychological benefits from TGD community connection. However, current evidence is based on mostly White TGD people and precludes examinations of behavioral TGD community connection as a potential mechanism for mental wellness.
Purpose
In this study we aim to (a) describe experiences of victimization, symptoms of depression and PTSD, and TGD community connection; (b) explore the associations between polyvictimization, symptoms of depression and PTSD; and (c) analyze how TGD community connection influenced decisions to seek help and the help-seeking process following an experience of violence among Black transgender women in Baltimore, MD and Washington, DC.
Methods
Quantitative and qualitative data include (a) semi-structured in-person interviews, (b) community asset maps, (c) trauma history timelines, and (d) a tablet-based questionnaire. A priori codes, informed by the minority stress model and intersectionality framework, guided questionnaire and interview guide development, data collection, and analysis. The minority stress model identifies distal and proximal stressors that impact mental health among people with one or more minority identities (Brooks, 1981; Hendricks & Testa, 2012; I. H. Meyer, 2003). The intersectionality framework describes the lived experience of people based on their co-occurring and intersecting social identities and the patterns of oppression or privilege that stem from micro-level social identities (e.g., race, gender) and macro-level structural factors (e.g., racism, cisgenderism) through a historical lens (Bowleg, 2008; Bowleg et al., 2003; Crenshaw, 1989, 1990). Our approach was informed by tenets of narrative analysis and Bowleg’s techniques to measure intersectionality (Bowleg, 2008, 2012; Riessman, 2008). This allowed the stories of participants to stay intact and provide opportunities to voice their experiences as they relate to their co-occurring identities within the current social context.
Participants
A total of 19 Black transgender women were recruited from the Baltimore, MD (n = 9) and Washington, DC (n = 10) metropolitan areas. All participants completed the survey and interview process, with exception of one person who did not complete the depression screener and two people who did not complete the PTSD screener. The median age of participants was 37 years (IQR = 24). Of participants, 36.8% did not complete high school or an equivalent, 52.4% were employed, and 10.5% of participants spent 10 or more nights in the past year with nowhere to sleep (Table 1).
Characteristics of Study Population (N = 19).
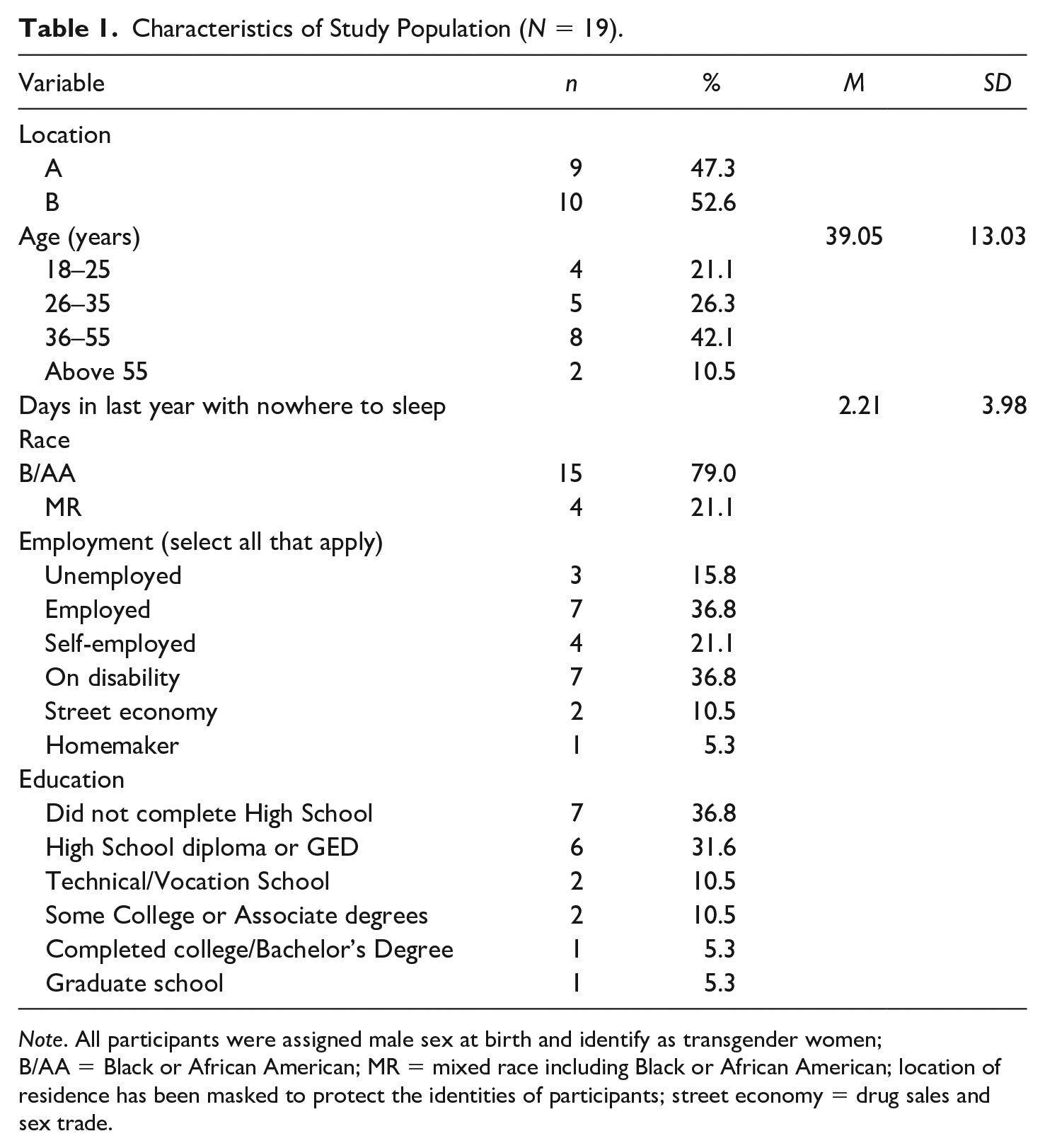
Note. All participants were assigned male sex at birth and identify as transgender women; B/AA = Black or African American; MR = mixed race including Black or African American; location of residence has been masked to protect the identities of participants; street economy = drug sales and sex trade.
Setting
Legacies of racial, ethnic, and income segregation in Baltimore, MD and Washington, DC result in many majority Black neighborhoods experiencing intense poverty and high violent crime rates (Friedman et al., 2017). The effect of living in such neighborhoods can be direct, through exposure to violence, or indirect, through discrimination and social status (Mode et al., 2016); thus, analysis, results, and discussion will consider the impact of city of residence and such historical context.
Recruitment
Participants were recruited via purposive sampling (Patton, 2014) based on geographic location (Baltimore, MD or Washington, DC metro areas). Inclusion criteria consisted of (a) self-identified as Black or African American or multiracial including Black or African American; (b) assigned male sex at birth; (c) current gender identity as transgender or gender different from birth sex; and (d) aged 18 years or older. We collaborated with one local LGBTQ+-serving health care clinic per metro area and an LGBTQ+ community-based organization in Washington, DC to assist with recruitment, community advisory board (CAB) development, and community dissemination of results. Recruitment strategies included distributing flyers to LGBTQ+ organizations and clinics, universities, and community colleges in both metro areas; LGBTQ+ and TGD group social media platforms; peer referral; and word of mouth.
Data Collection
Data were collected by the primary author. Participants met with the primary author at a private location of their choice in the community. Participants were asked to complete a tablet-based questionnaire (via tablet-based software using the data management and surveying system, SurveyCTO; http://www.surveycto.com/product/secure.html) and to participate in semi-structured interviews. The interviews lasted on average 1.5 hr and participants received US$50.00 as remuneration for their participation.
Safety protocols
Safety protocols (i.e., Immediate Danger Protocol, Suicidality Protocol, and General Community Resource Protocol) were developed in collaboration with the CAB consisting of Black transgender women residing in the metro areas of interest. Each study participant received the General Community Resource Protocol, and no one required the initiation of the Immediate Danger Protocol or the Suicidality Protocol. This study was approved by the Johns Hopkins Medicine Institutional Review Board.
Measures
Demographic variables included gender identity, age, race, ethnicity, and city of residence (i.e., Baltimore, MD or Washington, DC). Gender identity was captured using a two-step method: (a) What is your current gender identity? (Female/woman, Transgender female or trans woman, Gender fluid, Different identity) and (b) What is the sex you were assigned at birth on your original birth certificate? (male, female, intersex, unsure). All included participants identified as a Female/woman, Transgender female or trans woman. Lifetime polyvictimization was captured using the polyvictimization inventory (PV; α = .90; ranging from 0 to 15; 15-item; binary yes/no; spanning three domains of violence: sexual violence, physical violence, and threats of violence) which was operationalized as a continuous variable (Poteat et al., 2017; Sherman, Poteat et al., 2020). Past 2-week depression symptoms were captured via the Patient Health Questionnaire 2 (PHQ2; α = .64; ranging from 0 to 6; 2-item; 4-point Likert-type) and operationalized as (a) a continuous variable and (b) a prevalence using a cut off of 3 was used to indicate a clinical need for further assessment and treatment (Kroenke et al., 2003; Sherman, Poteat et al., 2020). Self-reported depressive symptoms are greatly influenced by time proximity; therefore, most self-report measures suggest using a 2-week timespan verses a lifetime measure of depressive symptoms (Kroenke et al., 2003). Lifetime PTSD symptoms were captured via the Primary Care PTSD Screener (PTSD-PC; α = .78; ranging from 0 to 4; 4-item; binary yes/no) and was operationalized as (a) a continuous variable and (b) a prevalence using a cut off of 3 was used to indicate a clinical need for further assessment and treatment (Cameron & Gusman, 2003; Sherman, Poteat et al., 2020). Emotional TGD community connection was captured via the Transgender Community Connectedness subscale from the Gender Minority Stress and Resilience Measure (α = .72; ranging from 0 to 10; 5-item; 3-point Likert-type) and was operationalized as a continuous variable (Testa et al., 2015).
Semi-structured interviews
Main topics of the interview included: (a) daily stressors and stress coping; (b) social support mechanisms; (c) community map; (d) trauma history timeline; (e) exploration of a self-selected experience of violence; (f) review of the help-seeking process following the identified exposure to violence; (g) engagement in care related to the incident; (h) general mental health following the incident; and (i) community connections and defining community. The interview guide was revised as necessary with CAB input before and throughout data collection.
Community asset mapping
Community asset mapping is a collaborative exercise between participant and interviewer used to identify TGD community connection. This method co-created a graphical representation of informal and formal sources of support available in the participant’s community (Kramer et al., 2012; Lightfoot et al., 2014). Participants used a template and specific stickers representing a priori characteristics to create their maps to show people and places in their lives (see Supplemental Material, Appendix). Since no psychometrically evaluated measures exist to date to identify both behavioral and emotional TGD community connection (Sherman, Clark et al., 2020), TGD community size from community asset maps (measuring behavioral participation with proximity scoring to denote sense of emotional belonging obtained from the community asset mapping) were compared with emotional TGD community connection scores to identify the appropriateness of using community asset maps to capture emotional and behavioral TGD community connection.
Trauma history timelines
Participants used trauma history timelines to identify their life-burden of violence. This method increases participant recall of traumatic events and is used to validate, quantify, and amplify other forms of data collection (Bornstein et al., 1998; Hassan, 2006; Van der Vaart, 2004). Participants were provided with violence/traumatic event examples, given a timeline template and allowed to work independently to create their timelines. Once completed, they guided the interviewer through their timeline and identified the experience of violence they wanted to explore in greater detail.
Analysis
Quantitative Analysis
Mann–Whitney U testing was used to compare differences in TGD community size between high and low emotionally connected groups (via emotional TGD community connection scores with high emotional connection = ≥6; low emotional connection = ≤ 5) to explore the appropriateness of community asset mapping in capturing behavioral and emotional TGD community connection (Aim 1). Spearmen’s rho correlation matrices and partial correlation analyses were conducted to (Aim 2) (a) identify correlations between polyvictimization and depression and PTSD and (b) explore the influence of emotional TGD community connection, behavioral TGD community connection, and additional sociodemographic covariates (city of residence and age) identified from previous research and from within the qualitative interviews (Sherman, Poteat et al., 2020). Strength of correlation was determined using p value < .10 (two-sided) and with the following scale: rs < .30 = negligible, rs = .30 to .50 = low, rs = .50 to .70 = moderate, rs = .70 to .90 = high, rs > .90 = very high (Mukaka, 2012). Statistical analysis was conducted using SPSS (IBM Corp., 2013).
Qualitative Analysis
All interviews were audio recorded, transcribed verbatim by three study team members, and reviewed for accuracy by the primary author. Transcripts were compared with the community maps to identify which people and places were identified as a TGD or LGBTQ+ community member/entity, identifiers were removed, and pseudonyms were assigned. Transcripts were then (a) read multiple times to identify stories and plots, (b) analyzed for interviewer discourse influence in responses and recorded memos/comparing field notes, (c) cleared of interviewer questions and prompts, and (d) organized by stories in stanzas based on the participant’s natural story flow (Priest et al., 2002; Riessman, 2008). Processed transcripts were uploaded for analysis to the mixed-methods analysis software, Dedoose (Sociocultural Research Consultants, 2018) where they were coded and linked to the quantitative survey data. Transcripts underwent multiple layers of coding (Hendricks & Testa, 2012) with a priori codes based on theoretical tenets identified from (a) minority stress (Brooks, 1981; Hendricks & Testa, 2012; I. H. Meyer, 2003; Sociocultural Research Consultants., 2018); (b) current research regarding TGD community connection; and (c) intersectionality (Bowleg, 2008). Two coders analyzed each transcript separately, then discussed and resolved discrepancies. The a priori codebook was modified based on emergent themes as coding progressed (Riessman, 2008). Once coding was complete, interactions between codes across and within interviews were evaluated, consolidated, and collapsed to form major themes by the first and second authors (A.D.F.S. and S.A.). A.D.F.S. and S.A. identified exemplars of thematic findings separately, then discussed and agreed upon exemplars for each theme to be merged with the quantitative findings. Constant comparison was used during transcription and analysis to continuously assess saturation (Bryman, 2016). Saturation was reached after 16 interviews, and we continued recruitment for three additional interviews to verify saturation.
Data Integration
All statistical findings were compared with narratives to identify areas where integration enhanced explanation, and triangulation strengthened interpretation (Creswell & Plano Clark, 2011). Any identified connections or discrepancies between the two sets of findings were highlighted and discussed by the team for interpretation.
Methods of Trustworthiness
The research team consisted of a Black heterosexual cisgender woman, a White queer non-binary person, a White pansexual gender-fluid person, two White heterosexual cisgender women, and an Indian heterosexual cisgender woman. Team members completed bracketing via reflexive journaling to identify potential biases and establish dependability (Tufford & Newman, 2012). Reflexive journal entries were reviewed as a team and included the following main themes: (a) participants would report high exposures to violence, sex work, homelessness, and discrimination and (b) participants would endorse higher community connection to TGD community compared to LGBTQ+ community. These themes were considered, and their influences discussed throughout data collection and analysis. Credibility was established through collaboration with CAB members with results presented to the CAB for member checking, confirmation, and further contextualization. Confirmability of the findings was established via the triangulation of the multiple sources of data (i.e., field notes, memoing, CAB input, survey data, community asset mapping, trauma history timelines, and interview transcripts).
Results
Aim 1. Describe Experiences of Victimization, PTSD and Depressive Symptoms, and TGD Community Connection
All participants experienced violence with 94.7% experiencing multiple types of violence (Table 2). The median polyvictimization inventory score of 3 (IQR = 4) matched the median number of violent experiences captured on the trauma history timelines (3; IQR = 4) and the median number of violent experiences discussed in the interviews (3; IQR = 5). People who used violence against the participants included peers, parents, siblings, extended family, strangers, intimate partners, sex work clients, landlords, police, medical professionals, university administration, and correctional officers. Domains of violence included physical; sexual; threats of violence; verbal/psychological abuse; child endangerment, abuse, and neglect; bullying; and denial of access to education. Several participants noted complex experiences in which they were subject to multiple types of violence during the same event or time period in their life-course (e.g., during a period of increased social vulnerability such as homelessness, substance use, or street economy 1 involvement).
Victimization Scores From All Data Sources, Depression and PTSD Scores.
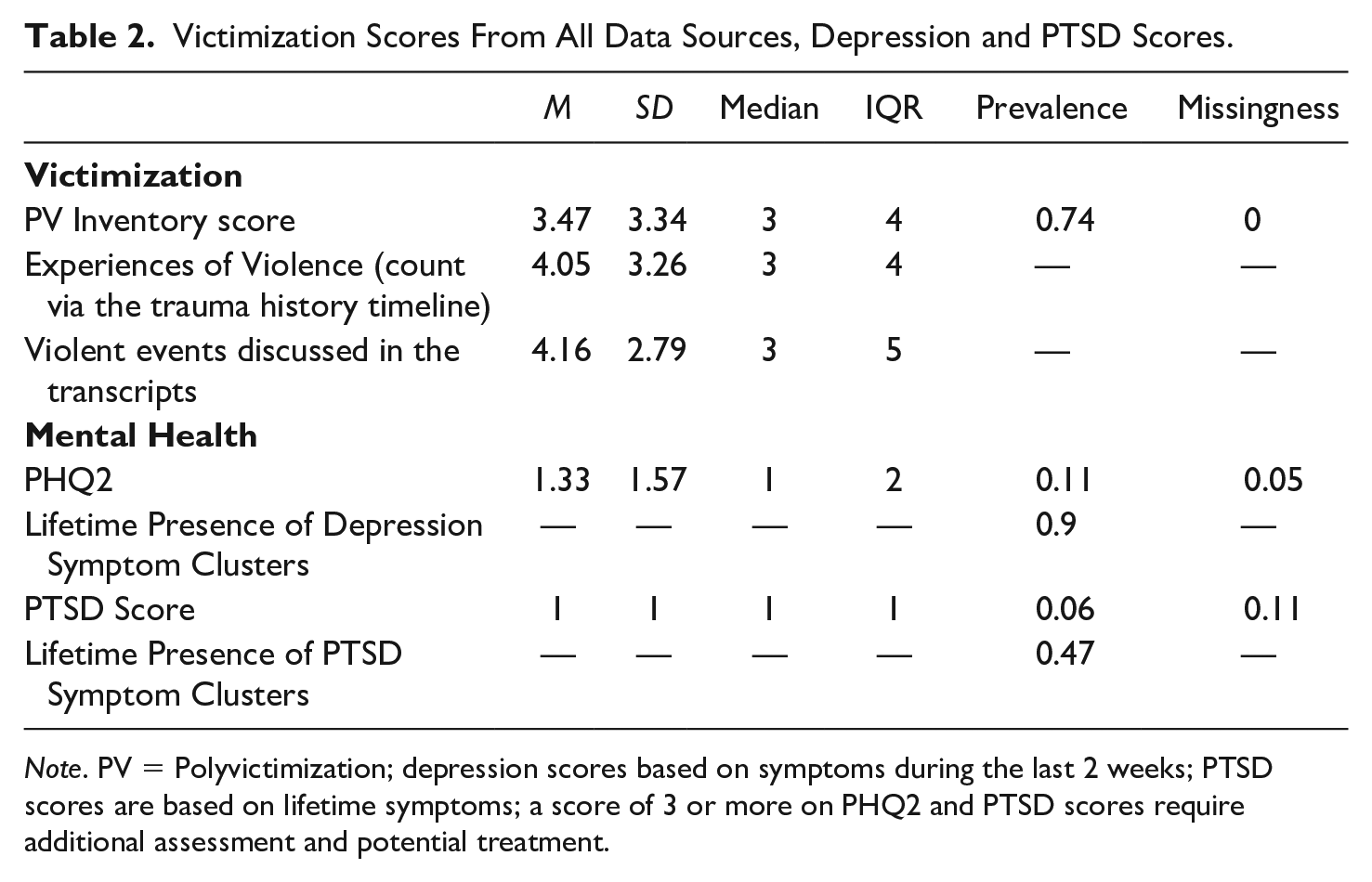
Note. PV = Polyvictimization; depression scores based on symptoms during the last 2 weeks; PTSD scores are based on lifetime symptoms; a score of 3 or more on PHQ2 and PTSD scores require additional assessment and potential treatment.
Perceived ableism (stigma against people with varying cognitive or physical ability/disability), racism, cisgenderism (identity-based and expression-based), heterosexism, HIV-related stigma, and geographic targeting influenced experiences of violence. Specifically, the interaction between racial belongingness and gender presentation influenced many experiences. Rejection, discrimination, or physical and verbal attacks by Black community members due to non-conforming gender expression were prevalent. Diamond shared, I can feel their [Black cisgender men] energy come off and it feels threatening and alarming. . . . I’m afraid of them [Black people] more than afraid of White people and, especially with Black men, they’re much more masculine, so it, it scares me off.
As seen with Diamond, several participants reported increased fear of Black cisgender men than other potential agents of violence, recalling past physical, sexual, and verbal attacks by people from this group. In addition, some participants noted their gender expression was perceived to be “disgraceful” to the Black community making them a target within the Black community, while being targeted by the general population because of both their race and gender expression. This “fear of Black cisgender men” and “Blackness” is related to systemic racism and racist propaganda promoted throughout U.S. history, which has portrayed Black cisgender men as violent attackers or “thugs” and has contributed to police brutality and mass incarcerations of Black cisgender men nationwide (Smiley & Fakunle, 2016). The effect of historical and current day systemic racism against Black cisgender men and Black families will be detailed further in the “Discussion” section.
Symptoms of depression and PTSD
Depression scores on the PHQ2 ranged from 0 to 6 (median: 1; IQR: 2; n = 18) with six of the participants scoring 0 on the scale (Table 2). The prevalence of depression in past 2 weeks was 11.1% (n = 2/18). Participants were asked about their mental health following an experience of violence and their mental health history during the interviews. The median lifetime PTSD score was 1 (IQR = 1; n = 17/19), see Table 2. The prevalence of PTSD symptoms throughout the life-course was 5.9% (n = 1/17). Narratives revealed varying symptoms clusters throughout the lifespan of participants with 89.5% (n = 17/19) experiencing symptom clusters consistent with depression, 47.4% (n = 9/19) experiencing symptom clusters consistent with probable PTSD, and 36.8% (n = 7/19) exhibiting symptom clusters consistent with possible comorbidity of depression and PTSD. For instance, Onyx shared her experience with possible comorbid symptom clusters, My mental health was gone! Shattered! [After the violent event]. Yes!!![I had flashbacks] You know, I would wake up in cold sweats. Because of how he was hitting my face. The trauma of it all. . . . Uh huh [my eating changed]. I got real skinny. Nightmares, jumping up off the bed, doing like this [flinching]. Blocking my face. Think that somebody’s going to hit me, you know? Right now, to this day, you could scare me like that (snaps fingers). Like if someone was to come around this corner right now, I would jump through the roof right now. I don’t know why I’m like that to this day. . . . I cry a lot. Out of the clear blue sky.
Upon further evaluation, there were significant correlations between comorbid symptom clusters and PTSD symptom clusters (p < .001; rs = .81) and lifetime PTSD scores (p < .10; rs = .47) and no significant association with depression symptom clusters, polyvictimization, emotional TGD community connection, age, or city of residence (Table 4). Results suggest that symptoms of PTSD may be driving the relationship between co-occurring symptoms of PTSD and depression.
TGD community connection
The majority of participants (73.7%; n = 14/19) had emotional TGD community connection scores that were consistent with feeling connected to the TGD community with a median emotional TGD community connection score of 7 (IQR = 4). Community asset mapping revealed that community sizes (Table 3) and the sense of connection to the TGD community was consistent with emotional TGD community connection scores. A Mann–Whitney U test indicated that the number of TGD community members in the inner circle of the community asset maps (i.e., most connected to) was greater for those participants who felt emotionally connected to the TGD community (Mdn = 0) than those who felt neutral or disconnected (Mdn = 1), U = 10.00, p < .05.
Transgender and LGBTQ+ Community Size and Level of Emotional TGD TCC.
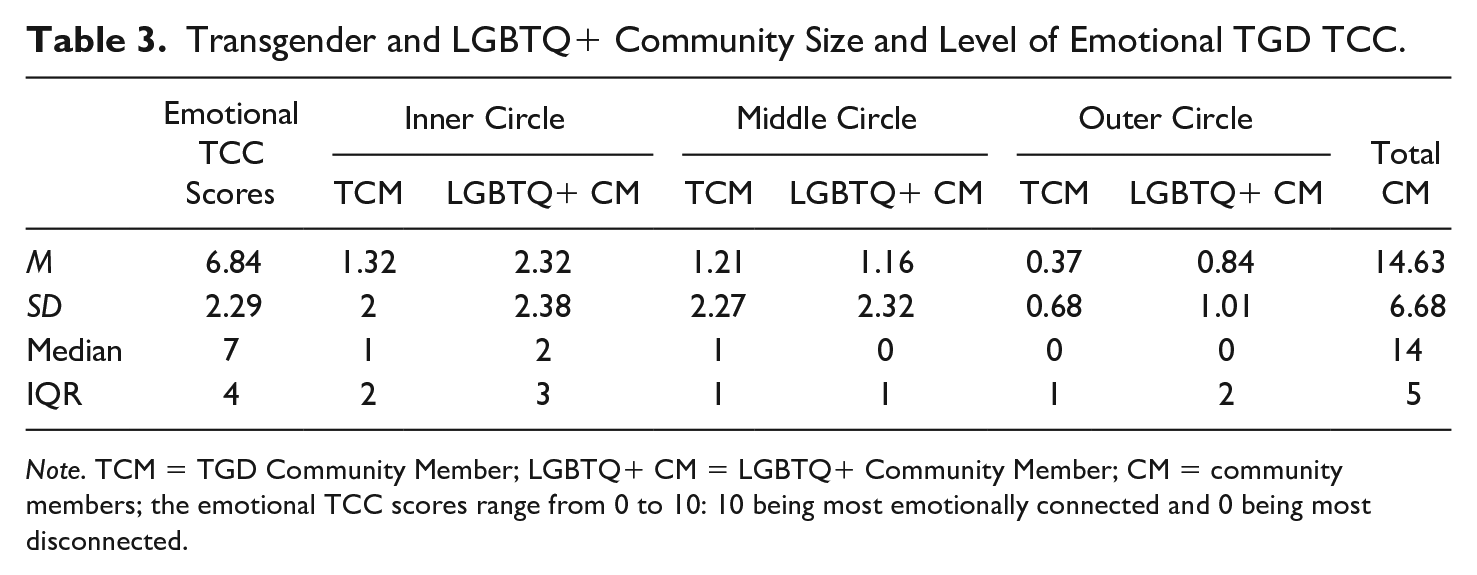
Note. TCM = TGD Community Member; LGBTQ+ CM = LGBTQ+ Community Member; CM = community members; the emotional TCC scores range from 0 to 10: 10 being most emotionally connected and 0 being most disconnected.
Some participants identified no difference between the TGD community and the greater LGBTQ+ community, while others noted many differences. Specifically, one participant noted that event planning around community events is often better funded, attended, and managed for LGBTQ+ events versus TGD events, which has led her to participate in and work for LGBTQ+ general events in lieu of TGD-specific events. Other participants noted racial differences between the groups. Labradorite described TGD events as being more racially focused compared to LGBTQ+ events: We had 16 days of celebration and we had discussions like PrEP with the youth and then we had conversations like gay men bridging the relationship with the transgender community and we had spiritual events, award ceremony, community mixers, [and] a ball for the youth. So, we had a variety of different things that focuses on our [the TGD community] needs along with our Black pride.
Several participants confirmed Labradorite’s sentiments regarding LGBTQ+ events were more focused on White peers and particularly sexual minority peers.
Several participants noted previous or current involvement with House and Ballroom events. House and Ballroom refers to a subculture or community that performs and competes in balls, created and predominated by Black LGBTQ+ people (Kubicek et al., 2013). Opal shared her excitement and emotional connectedness to a large national house, House of Balmain, “[I am a part of the], LGBQ, fashion, Balmain . . . I love Balmain anything. I have like 5 Balmain dresses. So, I feel like I’m in the family.” Participants commonly reported these events and communities as being a source of emotional strength, supportive of Black pride, and inclusive of all LGBTQ+ people.
Finally, medical and community-based organizations were often considered by participants to be LGBTQ+ community serving centers, but rarely considered part of the TGD community unless they specifically provided knowledgeable and affirming assistance to the participant themselves. An institution was rarely identified as TGD serving without also being LGBTQ+ serving. However, it was equally as common for participants to note no differences between the LGBTQ+ community and the TGD community and, as a result, did not identify with the TGD community.
Aim 2. Explore the Associations Between Polyvictimization, Symptoms of Depression and PTSD, and Emotional TGD Community Connection
Past 2-week depression symptoms were significantly correlated with current emotional TGD community connection scores (rs = −.47; p < .05) and city of residence (rs = −.56; p < .05) with more depression symptoms among those in Baltimore, MD (Table 4). Current emotional TGD community connection was independently significantly correlated with age (rs = .63; p < .01) and city of residence (rs = .53; p < .05), with stronger emotional TGD community connection scores in Washington, DC (Table 4). Partial correlations between past 2-week symptoms of depression and current emotional TGD community connection, controlling for (a) city of residence, (b) age, and (c) city of residence and age, were all non-significant (p > .05). There was no significant relationship of past 2-week depression and lifetime polyvictimization. However, lifetime symptoms of PTSD were significantly correlated with lifetime polyvictimization scores (rs = .61; p = .01); but correlations with all other covariates of interest were not significant and below .40 with the exception of depression (PHQ2; r = .40; p = .11) and age (r = −0.44; p = .08; Table 4; Mukaka, 2012). The associations remained strongly correlated when controlling for (a) city of residence, referent = Washington, DC; partial correlation (rp) = .55; p < .05, (b) age (rp = .51; p < .05), and (c) city of residence (referent = Washington, DC) and age (rp = .53; p < .05).
Spearman’s Rho Correlation Matrix for Variables of Interest.
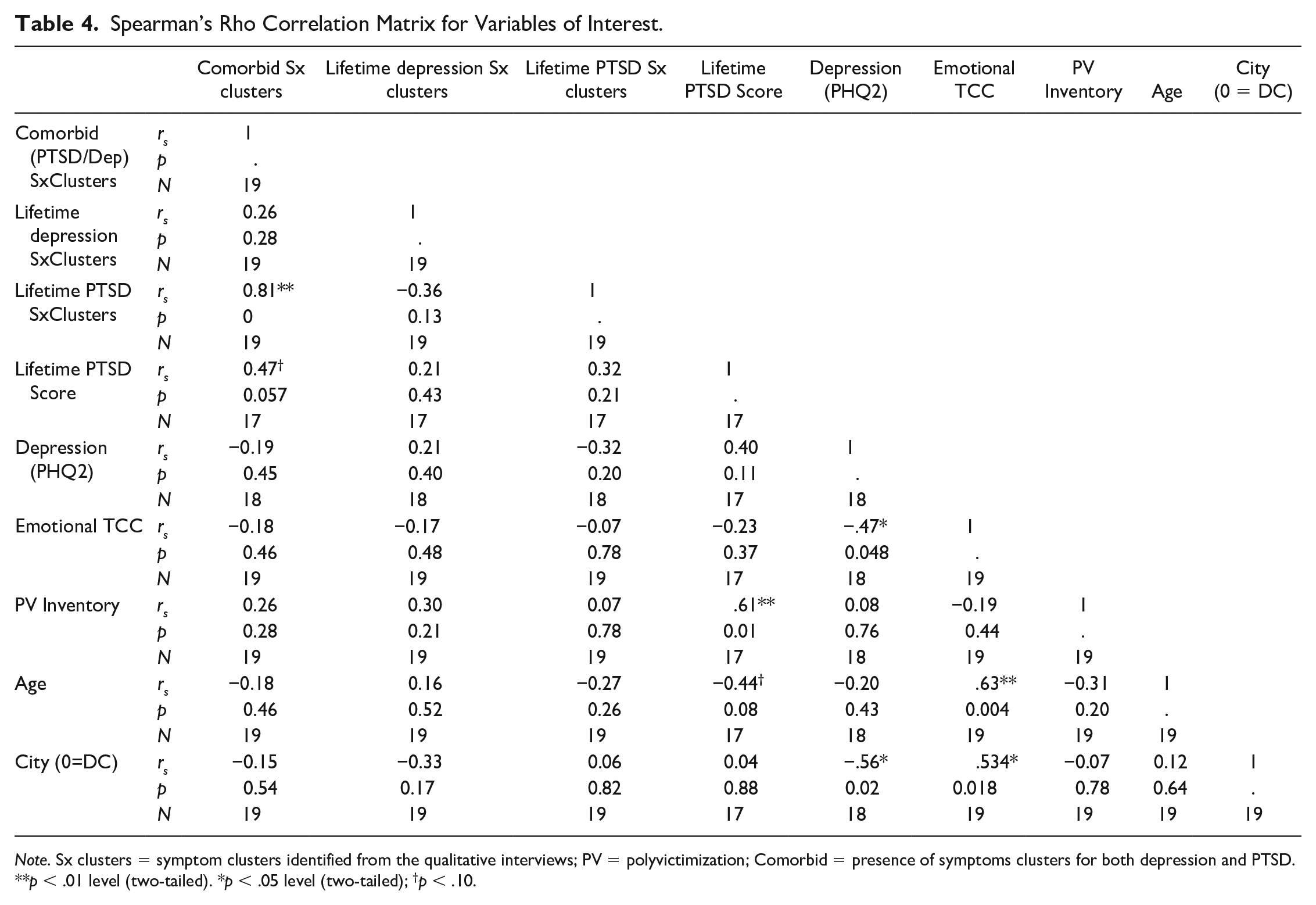
Note. Sx clusters = symptom clusters identified from the qualitative interviews; PV = polyvictimization; Comorbid = presence of symptoms clusters for both depression and PTSD.
p < .01 level (two-tailed). *p < .05 level (two-tailed); †p < .10.
Aim 3. Analyze How TGD Community Connection Influenced Decisions to Seek Help and the Help-Seeking Process Following an Experience of Violence
Three main themes were identified from the participant narratives regarding the influence of TGD community connection on decisions to seek help and the help-seeking process. Themes include: (a) Revictimization during Help-seeking, (b) Behavioral TGD Community Connection is Instrumental in Obtaining Help, and (c) Threats to Confidentiality and Peer-victimization in Formal Settings. Comparison between the participant narratives and community asset maps allowed researchers to identify formal and informal resources as connected to the LGBTQ+ community, the TGD community, both, or neither. Due to the perceived overlap between the TGD and LGBTQ+ communities by participants, the influence of both communities is captured in the themes discussed below.
Theme 1. Revictimization during help-seeking
Participants reported experiencing verbal or physical abuse from formal resources—that is, responding police officers, university administration, and medical personnel—which participants felt was related, in some cases, to their race and, for others, to their gender expression. Pearl discussed her gender being associated with mistreatment from police, “. . .because I’m a trans woman, and if I call the police and men come, it’s always, ‘So, what did you do? What did you, what, what partchu play in it?’” In addition, some participants noted that when police arrived on scene and believed the participant to be a cisgender woman, they were more often than not treated well, trusted by police, and seen as a victim not a perpetrator.
Verbal abuse from formal resources often took the form of victim blaming as seen above, refusal to use the individual’s name and pronouns, or minimizing the violence. Instances of victim blaming were also common among interactions with informal resources like cisgender and TGD peers and kin. Diamond shared, I went to one of my best friends [queer-identified cisgender woman; part of the LGBTQ+ community] for support and she said, “Well maybe if you didn’t dress that way, you know, you wouldn’t have gotten sexually assaulted.” And, I remember thinking, “No, you should know better” and then we got in a fight about it, but, you know, people are allowed to wear whatever they want, even if I’m wearing something that shows cleavage or not, you shouldn’t touch me.
There were varying results of help-seeking from formal and informal resources related to this further victimization. Formal entities were often found to be unsuccessful in resolving the incident by connecting the survivor with proper care or obtaining justice for the survivor, whereas informal resources were often instrumental in encouraging and connecting survivors with trusted formal sources of assistance (see Theme 2).
Theme 2. Behavioral TGD community connection is instrumental in obtaining help
Positive interactions with law enforcement and medical personnel occurred commonly in the presence of gender-affirming and knowledgeable individuals, such as LGBTQ+ police liaisons and at clinics that participants described as LGBTQ+ or TGD friendly institutions. Pearl shared her experience navigating a negative encounter with police by engaging the LGBTQ+ police liaison, I got robbed at like 6 o’clock in the morning. Didn’t have on no slutty clothes . . . I had on a nice little dress. Wasn’t too short . . . The man [police officer] ask me, oh, he told me, “You wasn’t dressed like that you may had not gotten robbed.” And I said, “You know what? Instead of calling you I should have called [the LGBTQ+ police liaison].” . . . And I called her right there, while he was right there. . . and she chewed him out. And he was suspended.
Similarly, informal resources, specifically LGBTQ+ and TGD community members often connected participants to trusted resources or accompanied participants while seeking help to provide emotional support and protect against further victimization from formal resources. Opal shared, “[Following an experience of violence] I was walking on [the] interstate and [transgender woman] told me to come to [LGBTQ+ community organization]. She gave me $7 and she said, “If you make it, I know you’re strong.” She said, “You’re strong now” but she’s like, “I know you’ll be stronger.” As seen in Opal’s case, these community members were also instrumental in providing financial support and getting the participant to safety.
Despite previous or current negative experience with formal resources, some participants found ways to work within formal resources to identify confidants and gain the assistance that they needed. Opal discussed her hesitance in connecting with LGBTQ+ and TGD peers at a formal resource because of people “talking” about her behind her back. However, Opal was able to find a few transgender women that she trusted to help her navigate the system and learn how to care for herself, [After arriving at the LGBTQ+ community organization], they showed me how to be a woman. They showed me how to shave my face, they showed me how to calm down, they showed me how to be more like, expressive of my feelings. And that really changed my life.
As with Opal, the other participants found a trusted key informal resource (e.g., LGBTQ+ or TGD peer or kin) that was pivotal in helping the participant navigate the formal resource.
In several instances, past negative experiences with police and the medical system (formal resources) discouraged survivors from seeking help until prompted and assisted by peers and/or kin. Amber shared a complex experience with receiving conflicting messages from peers, At first I . . . wasn’t gonna . . . then I was gonna do it [call the police], but then I changed my mind. I didn’t want to do it. But then I felt like I was forced to do it ‘cause someone suggested it, so I tried to get ahold of ‘em at [the] hospital, I didn’t have a phone and they [a friend] talked me out of it . . . then someone did get in touch with them [against my will] and said it was taken care of, but I never heard anything else from them [the police] . . . I never saw them again, so it was just weird.
On the few occasions when survivors were connected to police or medical assistance against their will or without their knowing, as seen with Amber above, such connections were often unsuccessful in obtaining help or problem resolution.
Theme 3. Threats to confidentiality and peer victimization in formal settings
Participants often felt that medical establishments and community-based programs with other transgender women and gay cisgender men employees fostered a culture of gossip and judgment. Sunstone shared, A lot of the Black tran[s] girls, [and] the gay Black men—they are in a position to really do change for the community and . . . they are not . . . They are there for the stipend, the check, the grant . . . and they will do a little bit, and this is happening today . . . because society the way it is I find that a lot of them it’s a buddy system if I know you, you know me, you put me on, I might not even qualify. But you know because we need a gay person in there . . . they get in the position and . . . there’s instant chit chatter . . . it’s in the DNA.
As seen with Sunstone, participants questioned the validity and appropriateness of employing community members who were perceived to be under-trained or were noted to disclose private medical information about participants to other community members. In addition, participants reported no longer seeking care from places where peers and friends or family of peers worked based on fears of confidentiality loss and experiences of non-authorized disclosure of personal health information. Tiger’s Eye shared with us, that her cousin found out she was HIV-positive from a mutual acquaintance who happened to be Tiger’s Eye’s medical case manager: The reason I don’t have a case manager is because . . . all of a sudden, she [my cousin] texts me, like, “What’s your address?” So, I give her my address, she comes to my party. She was like, “You wanna tell me somethin?” I’m like, “huh?” She like, “You got something” to tell me? I was like, “No.” She was like, “Don’t you go to [LGBTQ health clinic]?” And I’m like, “Yeah, for my hormones.” She was like, “You got HIV?” And it was like, “What? . . . why you asking something” like that? She was like, “Because, my friend works there and she’s a case manager.”
Other participants described similar encounters, where they saw someone they knew in the clinic and left and never returned for care due to perceived threats to confidentiality. Finally, participants who expressed their gender more fluidly or ambiguously, or those who were HIV-positive, reported experiencing ridicule by older peer transgender women and gay cisgender men in formal resource settings, especially from peers who ascribed to a conventional standard of feminine gender presentation. This peer violence made many participants question the confidentiality of seeking help from those entities and as a result, participants often felt discouraged from seeking help from or disclosing information in these settings.
Discussion
Violence
The findings from this mixed-methods study corroborate the alarmingly high prevalence of violence and polyvictimization exposure as reported in previous qualitative and quantitative research with Black transgender women (Sherman, Poteat et al., 2020; Wirtz et al., 2020). The prevalence of polyvictimization among the participants in this study echo the results found by a study with a larger (N = 197) but otherwise similar sample from the same geographic area, in which 91.4% of Black transgender women reported exposure to multiple types of violence (mean number of types of violence experienced: 7.71; SD = 4.58; Sherman, Poteat et al., 2020). Also, like Graham’s (2014) study with young Black transgender women, we found that participant narratives were saturated with multiple accounts of abusive interactions within the spaces which protect many non-black and non-trans people, such as schools, churches, and the criminal justice system. Taken together, the results of this study and previous ones indicate that polyvictimization against Black transgender women is a pervasive issue in need of systemic reform (Wirtz et al., 2020). However, contradictory policies challenge progress toward safeguarding Black transgender women from equitable treatment after experiencing violence. For example, the reauthorization of the Violence Against Women Act in 2014 included provisions which extended legal measures to LGBTQ+ survivors of victimization. At the time, the legislation aimed to improve protections and access to support services for LGBTQ+ survivors of violence. Nevertheless, the protections specific to transgender women were widely disputed in Congress when the reauthorization of the Violence Against Women Act emerged (Cochrane, 2019). Furthermore, the recent erasure of Patient and Protection Affordable Care Act provisions which protected TGD people from health care discrimination effectively increases their vulnerability to experiencing violence and refusal of treatment from health providers (Gupta, 2020).
Mental Health
Past 2-week depression scores for this sample were slightly lower (M = 1.33; SD = 1.57) than in previous research (M = 1.86; SD = 1.713) of past 2-week depression with similar samples, which may be due to the small sample size and methods of community recruitment from clinical settings (Sherman, Poteat et al., 2020). Nonetheless, our interviews revealed that the vast majority of participants (90%) had symptom clustering consistent with possible depression over the life-course, which is consistent with theory and research accounts explaining the adverse mental health impacts of chronic and intersectional minority stress that Black transgender women endure (Crenshaw, 1990; Graham, 2014; I. H. Meyer, 2003; Tufford & Newman, 2012). Discordant findings from this study and similar previous research regarding the association between polyvictimization and past 2-week depression may be explained by a variety of other factors, including measure brevity (Budge et al., 2013; Reisner et al., 2016; Sherman, Poteat et al., 2020; Tufford & Newman, 2012), the relatively small study sample size (n = 19), and lack of cross-cultural scale validity.
The significant correlation between lifetime polyvictimization and lifetime PTSD symptoms mirror findings in previous research (Andrews et al., 2015; Charak et al., 2019; Ford et al., 2013; Sherman, Poteat et al., 2020). Furthermore, our results suggest possible comorbid depression and PTSD symptom clusters among participants. Comorbid depression and PTSD is highly prevalent in cisgender survivors of violence, and studies suggest that PTSD drives the association (Blanchard et al., 1998; Hurlocker et al., 2018; O’Donnell et al., 2004). Given that 54.8% of PTSD cases worldwide are rated as being severely debilitating based on World Mental Health Surveys (Kessler et al., 2009), it is crucial to further investigate protective mechanisms, such as TGD community connection, that may improve PTSD symptom management and reduce the longer term effect on functionality in this population.
TGD Community Connection
Overall, emotional TGD community connection scores confirmed the reliability of community asset mapping to identify both emotional and behavioral components of TGD community connection, indicating that community asset mapping may be an effective and insightful method to capture TGD community connection in future research. Associations between emotional TGD community connection scores and mental health have varied in previous studies with larger samples. One study found no significant associations between emotional TGD community connection and mental health among 197 Black and Latinx transgender women (Sherman, Poteat et al., 2020), while another found an association between emotional TGD community connection and depression using the Center for Epidemiologic Studies Depression Scale-10 (CESD-10; N = 865 majority White TGD sample; Pflum et al., 2015). These discordant findings in the literature suggest that emotional connectedness may be functioning differently for Black transgender women when compared to the larger TGD community and/or White peers. The pervasive and disparate stigma and violence exposure experienced by Black transgender women compared to the larger TGD community and White transgender women (Dinno, 2017; Graham, 2014; Krell, 2017) may be contributing to decreased accessibility to community resources regardless of their level of reported emotional connectedness, suggesting that emotional connectedness may not be as strong a predictor of mental health as behavioral TGD community connection.
Our interviews revealed that behavioral interaction with TGD peers and TGD formal entities was instrumental in connecting survivors to care. These findings support previous research highlighting the utility of engaging with same-gender and same-race peers (Sherman, Clark, et al., 2020). Specifically, support from peer transgender women encouraged health-seeking behaviors and engagement in care regarding sexual health and gender-affirmation among transgender women in Guatemala (Boyce et al., 2012) and was associated with improved mental health, increased resilience, decreased acculturative stress and feelings of isolation, and improved access to formal resources among transgender women in the U.S. and United Kingdom (Cerezo et al., 2014; Graham et al., 2014; Hines, 2007; Pinto et al., 2008; Reisner et al., 2009). Also, TGD youth of color found engagement with TGD peers of the same race validating of both their gender and racial experiences (Singh, 2013). Our findings and previous research suggest that those who are behaviorally connected to a TGD community have higher likelihood of improved mental health, accessing health care, and obtaining help post-victimization. Thus, behavioral participation may be a better predictor of mental health outcomes among this community. Future research may need to include separate measures of emotional connection and behavioral participation to parse out potential effects on health.
Help-Seeking
Interviews revealed that the interplay of race and gender expression influenced participant experiences of revictimization when seeking help. This confirms previous research highlighting a disparity in violence exposure based on race and gender (James et al., 2016). The U.S. Transgender Survey data (N = 27,715) showed that 33% of transgender women reported experiencing verbal harassment in public by strangers in the past year, with the highest rates among multiracial transgender women (51%; James et al., 2016). More specifically, a recent study has noted a similar interplay among those seeking help following exposure to intimate partner violence, with participants reporting that calling the police was not an option due to past exposures to racism and cisgenderism in police interactions (Guadalupe-Diaz & Jasinski, 2017). Recognizing that the Black community and the TGD community are not monolithic homogeneous communities, our findings illustrate a complex interplay between the two “communities.” Participants shared their fears, hopes, and experiences navigating the intersection of these communities, which highlights a need to target community building and the integration of safe spaces within and between communities.
Experiences and fears of Black cisgender men being agents of violence were not uncommon among participants and may be related to internalized racism and historical demonization of Black cisgender men in the U.S. Historically, government policies and local practices such as redlining, dictated where Black families could live and obtain education and employment. These policies have been traced to historical media portrayals and political demonization of Black cisgender men’s bodies and masculinity, targeted because Black cisgender men were seen as a threat to White men’s power (Dines, 1998; Smiley & Fakunle, 2016). The narrative of Black cisgender men being “brutes” or “thugs” has been perpetuated throughout U.S. history and has resulted in mass incarceration of generations of Black cisgender men in the U.S. (Browning et al., 2001; Smiley & Fakunle, 2016). This, in turn, has destabilized the structure of countless Black families by diminishing Black men’s gender power and skewing gender expectations of masculinity toward aggression. Thus, findings regarding Black cisgender men being disproportionately feared or acting as agents of violence should be considered within this context.
Victim blaming, commonly noted in research with cisgender survivors of violence (S. Meyer, 2016), was a predominate experience noted by Black transgender women in our sample during help-seeking post-exposure to violence. Participants were attributed blame from both formal and informal resources (including LGBTQ+ and TGD community members) often explicitly related to their physical appearance, via race, clothing, or gender expression. Previous research regarding racism, racial stereotyping, and rape victim blaming has shown that victims of interracial rapes were blamed more than victims of intraracial rapes, via vignettes comparing Black and White women as victims and Black and White men as perpetrators (George & Martínez, 2002). In that study, assumed cisgender men rated victims as more culpable than assumed cisgender women did, and racism scores were positively associated with the severity of victim blaming endorsed by participants (George & Martínez, 2002). This interplay between racism and victim blaming may be compounded by the effect of traditional gender role stereotyping. A review of the victim-blaming cisgender literature has found that women who violate traditional gender role stereotypes (with men being socialized to be the sexual initiators and women to be sexually passive) are attributed more blame than those who conform to them, and people who endorse traditional gender roles attribute higher levels of blame to victims than those who do not endorse traditional gender roles (Grubb & Turner, 2012). Widespread victim blaming experienced by participants, compounded by the effects of racism and cisgenderism, reveals a systematic deficit in how survivors of violence are treated within society. Past experiences with victim blaming may delay help-seeking, which, in turn, may put Black transgender women at further risk for worse mental health outcomes.
Finally, while engaging with formal resources, participants reported threats to confidentiality and experiences of peer victimization specific to gender presentation and HIV status. This had a negative effect on the help-seeking process for many participants. This is concerning and contradictory to existing evidence that shows community representation in health care settings helps to improve health outcomes and health care utilization among minoritized and disenfranchised racial and ethnic groups (Jackson & Gracia, 2014; Rosenthal et al., 2010; Swider, 2002; Williams et al., 2016). Several initiatives nationwide have focused on integrating community-representative community health workers to assist in health education, community outreach, and health care navigation, specifically targeting racial and ethnic minoritized communities (Swider, 2002). Such strategies focusing on community representation and community integration have been suggested and successfully used in interventions and clinical settings to address negative effects of stigma and victimization affecting TGD people (Matsuno & Israel, 2018; White Hughto et al., 2015).
Conversely, the threats to confidentiality noted by our participants do corroborate narratives from other transgender women and may be related to the size of the TGD community, delivery method of assistance (specialized clinic days or specialty clinics), and scarcity of resources in certain settings, such as sex work environments (Sherman, Clark et al., 2020). One example of threats to confidentiality was seen among Guatemalan transgender women, who reported that they feared their peers would disclose their HIV status to sex work clients, which would result in a loss of clientele and associated income needed for survival (Boyce et al., 2012). Thus, those participants prioritized their ability to obtain monies for survival over their other health care needs, and delayed or refused to seek care from TGD-focused clinics for fearing or previously having their HIV status disclosed against their will (Boyce et al., 2012). In that study, participants were more concerned with fellow patients than clinic employees; however, it is unclear if clinic staff were representative of the community. These concerns highlight a need for improving ethics and confidentiality protocols, training, and implementation in formal resources to allow people to feel safe and supported when help-seeking and receiving health care or support. Finally, interventions should focus on rebuilding trust between formal resources and the greater TGD community to dispel fears and heal trauma from previous negative experiences. To do this, formal resources should partner with informal community leaders and various community representatives to create and facilitate community-engagement interventions to establish trust between formal sources and the TGD community.
Limitations
There are several limitations that are important to note. The depression and PTSD screeners were not validated with Black transgender women and may not accurately capture cultural differences in manifestations of depression and PTSD for this group. Our convenience sampling from community and LGBTQ+ based health centers may have resulted in a more community-connected sample and thus may have impeded variability to see a true effect of emotional TGD community connection. This study lacked a measure of behavioral participation to quantitatively analyze its influence on the association between polyvictimization and mental health outcomes. In addition, the small sample size and regional focus limits the generalizability of our results to other groups and geographic areas. The study was also underpowered to accurately detect any effects including moderation of the relationship between polyvictimization and mental health by emotional TGD community connection. Finally, the Black community is not a monolithic group and variations in experience based on race, ethnicity, and experiences with colorism (stigma related to skin tone can be perpetuated within groups of the same race or ethnicity and by people of differing races or ethnicities) may impact the variables discussed in this analysis. However, colorism did not permeate the narratives of participants and racial and ethnic variation of the sample was limited. Future research should work to understand variations based on race, ethnicity, and experiences with colorism. Despite these limitations, a major strength of this study was the use of multiple innovative data collection methods allowing for the identification of numerous domains of violence, frequency of exposures, and the capturing of behavioral TGD community connection via community mapping and qualitative inquiry. The use of these methods provided a robust description of participants’ life experiences and allowed participants to define their community and their perceived place in it.
Conclusion
Black transgender women living in Baltimore, MD and Washington, DC experience multiple types of violence throughout their lifespan that directly correlate with mental health symptoms. Those seeking help from formal and informal resources often experience victimization via victim-blaming, physical violence, or psychological violence related to racism and cisgenderism. This, along with fears of loss of confidentiality, isolates survivors and may decrease help-seeking after subsequent violent experiences. This study was not able to fully explore the moderating influence of emotional TGD community connection on mental health outcomes; however, participant narratives revealed that behavioral TGD community connection was instrumental in successfully obtaining help post-exposure to violence. Behavioral TGD community connection is a modifiable construct that could mitigate the effects of violence on mental health by increasing utilization of formal and informal resources. Researchers would benefit from including a community building component into future interventions to increase individual and community resilience and rebuild trust between the TGD community and formal resources.
Supplemental Material
sj-pdf-1-vaw-10.1177_10778012211013892 – Supplemental material for Transgender and Gender Diverse Community Connection, Help-Seeking, and Mental Health Among Black Transgender Women Who Have Survived Violence: A Mixed-Methods Analysis
Supplemental material, sj-pdf-1-vaw-10.1177_10778012211013892 for Transgender and Gender Diverse Community Connection, Help-Seeking, and Mental Health Among Black Transgender Women Who Have Survived Violence: A Mixed-Methods Analysis by Athena D. F. Sherman, Sarah Allgood, Kamila A. Alexander, Meredith Klepper, Monique S. Balthazar, Miranda Hill, Christopher M. Cannon, Deborah Dunn, Tonia Poteat and Jacquelyn Campbell in Violence Against Women
Footnotes
Appendix
Acknowledgements
We would like to thank the participants who bravely shared their stories with our team. The time you invested in this study will not go silently into the pages of a journal but will be the flames to burn down broken systems, and the foundation to rebuild the supports the TGD community deserves. The systems in place have failed many of you, time and time again. We dedicate this work to you all and vow to work with the community to improve health care provision for TGD survivors of violence. And to one of our participants who passed this year: you will forever be remembered, and your words and strength will be instrumental in creating interventions for women like you. We wish all participants strength, happiness, and support in your days to come. Finally, we would like to thank the institutions and individuals (remaining anonymous for confidentiality) who contributed time and resources to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received partial funding from the following sources: the Robert Wood Johnson Foundation Future of Nursing Scholars, the Scholl Award from Johns Hopkins School of Nursing, and the Post-doctoral to Faculty fellowship at the Nell Hodgson Woodruff School of Nursing at Emory University.
Supplemental Material
Supplemental material for this article is available online.