
Abstract
In this study, linear mixed-effects regression analyses were used to examine whether sociodemographic variables, abuse-related variables, and well-being variables were associated with symptoms of depression and post-traumatic stress disorder (PTSD) in abused women residing in shelters. Results pointed out that symptoms of depression severity were positively associated with migration background and the experience of physical abuse and negatively associated with self-esteem and social support. PTSD symptoms were positively associated with the experience of sexual abuse and negatively associated with self-esteem. Within women’s shelters, staff could be sensitive to improving the social integration of women, especially those with a non-Dutch background, and strengthening the women’s social networks and their self-esteem.
Keywords
Introduction
Intimate partner violence (IPV) is a major public health concern and a violation of women’s human rights (World Health Organization [WHO], 2014). Worldwide, almost one third (30%) of all women who have been in a relationship have experienced physical and/or sexual violence by their intimate partner (WHO, 2014). The implications of IPV are extensive and include physical, mental, sexual, reproductive health as well as other health problems (Campbell et al., 2002; WHO, 2014). The negative mental health consequences most frequently associated with IPV are depression and post-traumatic stress disorder (PTSD; Campbell & Lewandowski, 1997; Dienemann et al., 2000; Golding, 1999; Jones, Hughes, & Unterstaller, 2001).
Depression is defined as a state of low mood and loss of interest or pleasure that can affect a person’s thoughts, behavior, feelings, and sense of well-being (American Psychiatric Association, 2013). In survivors of IPV, depression can severely influence women’s ability to establish and maintain relationships, contributing to social isolation and decreased access to social support (Carlson, McNutt, Choi, & Rose, 2002; Helfrich, Fujiura, & Rutkowski-Kmitta, 2008; Nathanson, Shorey, Tirone, & Rhatigan, 2012). High levels of depression have been found in 35-70% of female IPV survivors (Gerlock, 1999; Golding, 1999; Nathanson et al., 2012; Petersen, Gazmararian, & Clark, 2001; Stein & Kennedy, 2001).
PTSD may develop in some people after experiencing a traumatic event, including experiences with IPV (American Psychiatric Association, 2013). The symptoms of PTSD include re-experiencing, avoidance, negative alterations in cognitions and mood, and arousal (American Psychiatric Association, 2013). High levels of PTSD symptoms have been found in 55-92% of women with a history of IPV (Gorde, Helfrich, & Finlayson, 2004; Humphreys, Lee, Neylan, & Marmar, 2001; Jones et al., 2001). Both depression and PTSD among abused women have been found to be persistent, with symptoms continuing to exist when the abuse has ended (Campbell & Lewandowski, 1997; Campbell & Soeken, 1999; Campbell, Sullivan, & Davidson, 1995; Mechanic, Weaver, & Resick, 2008; Zlotnick, Johnson, & Kohn, 2006).
Taking refuge in a shelter usually is a last resort for women in their effort to escape violence and end IPV (Berk, Newton, & Berk, 1986; Shostack, 2001). Research has shown that shelters and crisis centers are being used by women who experience the most severe abuse (Ansara & Hindin, 2010) and report more related injury and mental health problems than abused women not residing in shelters (Johnson, Zlotnick, & Perez, 2008; Jones et al., 2001; Saunders, 1994).
Only a limited number of studies have examined depression or PTSD in IPV survivors during their shelter stay. An early study by Mitchell and Hodson (1983) showed high levels of depression, low self-esteem, and social isolation among shelter-based abused women (Mitchell & Hodson, 1983). Clinically significant levels of depression were reported in 43% of a sample of abused women receiving extensive services from a crisis or transitional shelter after their shelter exit (Ham-Rowbottom, Gordon, Jarvis, & Novaco, 2005). The 12 months prevalence of major depression in a shelter-based sample of abused women in the United States was estimated to be 51% (Helfrich et al., 2008). Clinical levels of PTSD in shelter-based abused women, as reported across studies, range from 40-84% (Ham-Rowbottom et al., 2005; Jones et al., 2001; Kemp, Rawlings, & Green, 1991; Mertin & Mohr, 2001). Depression and PTSD usually show high comorbidity, also in shelter samples (Ham-Rowbottom et al., 2005; Nixon, Resick, & Nishith, 2004).
Factors associated with depression and PTSD in adult abused women are many, and they include among others young age (Hazen, Connelly, Soriano, & Landsverk, 2008; Wrangle, Fisher, & Paranjape, 2008), a high number of children (Campbell & Lewandowski, 1997; Cascardi, O’Leary, & Schlee, 1999; Jones et al., 2001), and for depression, migration (Prosman, Jansen, Lo, Fo, & Lagro-Janssen, 2011). In addition, for both depression and PTSD, factors are frequency and severity of physical (Campbell et al., 1997; Golding, 1999; Jones et al., 2001) and sexual abuse (Bennice, Resick, Mechanic, & Astin, 2003; National Coalition Against Domestic Violence [NCADV], 2015; Plichta & Falik, 2001), low self-efficacy (Sullivan, McPartland, Price, Cruza-Guet, & Swan, 2013), poor self-esteem (Campbell & Alford, 1989; Cascardi & O’Leary, 1992; Sato & Heiby, 1992), and little or no available social support (Campbell et al., 1997; Rodriguez et al., 2008; Wong, Tiwari, Fong, Humphreys, & Bullock, 2011).
The above-mentioned factors related to symptoms of depression and PTSD are found in studies including broad categories of abused women. The aim of this study was to investigate whether these factors are also valid for adult abused women in shelters, who represent the extreme end of severity of abuse. Research in this subgroup of abused women is scarce, possibly because these women may not be willing to participate in research as sharing their experiences may be risky and their partners may not approve. Therefore, this study contributes to the literature as well as to everyday practice because it may provide women’s shelters with important information to better attune their services to the needs of abused women and to possibly reduce symptoms of depression and PTSD in these women.
We included the previously mentioned variables and categorized them into sociodemographic variables (age, migration background [Dutch or non-Dutch], and number of children), abuse-related variables (sexual and physical abuse), and well-being variables (self-efficacy, self-esteem, and available social support). The latter variables may be amenable to modification, by the women themselves or professional interventions.
Method
Participants
This study was part of a larger research project by Impuls—Netherlands Center for Social Care Research (Radboud University Nijmegen Medical Center) and the Netherlands Institute of Mental Health and Addiction on supply and demand among abused women in women’s shelters (Wolf, Jonker, Nicholas, Meertens, & Te Pas, 2006; Wolf, Jonker, Nicholas, & Putriss, 2007). Women were recruited at 18 of the 39 women’s shelters in the Netherlands. The 39 shelters were stratified by the four regions of the Netherlands (north, east, south, and west) and approached per stratum on a randomly ordered list.
To be eligible for the study, women had to be aged 18 years or older, survivor of IPV by a male (ex-)partner, and having been admitted to a shelter between mid-November 2004 and mid-March 2005. By stratified sampling, four categories of women were approached: (a) Dutch women in short-stay shelters (3 weeks or less), (b) Dutch women in long-stay shelters (3 weeks or more), (c) non-Dutch women in short-stay shelters, and (d) non-Dutch women in long-stay shelters. The aim was to reach 40 women in each category. In total, 490 women were approached to participate, of whom 218 (44.5%) could be interviewed. Reasons for nonparticipation were refusal to participate in the study, inclusion in wrong stratification categories, or no interpreters available (Jonker, Sijbrandij, & Wolf, 2012).
For the purpose of this study, we excluded 34 women because they missed outcome measures relevant for this study due to the use of a shortened version of the questionnaire, which was used if women did not speak Dutch and had to be interviewed in a foreign language. We used this shorter questionnaire because we expected that the translation of questions would considerably lengthen the interview. The final number of women in the current study was 184.
Procedures
At each shelter location, an assigned staff member screened and approached women using a randomly ordered registration list of all the women living in the shelter. After giving written informed consent, women were interviewed face-to-face by trained research assistants. All instruments, including self-report measures, were administered in-person because a substantial but unknown proportion of the shelter-based women are illiterate. Each woman received 15 Euros for their participation. The method of the study has been reported elsewhere in more detail (Jonker et al., 2012).
Measures and Instruments
Sociodemographic Characteristics
Sociodemographic characteristics collected were age, marital status, country of birth, migration background (Dutch/non-Dutch), number of children, educational level, and employment status. Educational level was divided into low (no formal education or primary education only), average low (prevocational education, junior general secondary education, or prevocational secondary education), and average high to high (vocational education, general secondary education, pre-university education, professional higher education, or academic higher education).
Abuse-Related Variables
The type of abuse experienced before shelter entry was assessed using a self-developed question: “What kind of violence did you experience by [NAME ABUSER]?” Women could select one or more of the following options: physical violence (“like being beaten, kicked, or objects thrown at you”), sexual violence (“like intimacy you didn’t want or like, or rape, for example when he came home drunk”), and psychological violence (“like threats, or he had no respect for your feelings, said things to hurt you or prohibited you to go outside”). Women were also asked how long they were in a relationship with the abuser and whether the violence had become more severe over time. Furthermore, they were asked if they had been in touch with the abuser during their shelter stay.
Mental Health
Depressive symptoms were measured with the Dutch version of the Center for Epidemiological Studies Depression Scale (CES-D; Hanewald, 1987; Radloff, 1977). The CES-D is a self-report measure with 20 items related to depressive symptoms during the past week. An example of one of the items is as follows: “I had trouble keeping my mind on what I was doing.” Item scores are rated on a 4-point scale ranging from 0 (seldom or never) to 3 (always or almost always). Total scores range from 0-60 and are categorized according to the following criteria: scores 0-15.5 for no depression, scores 16-20.5 for mild depression, scores 21-30.5 for moderate depression, and scores of 31 and higher for severe depression (Radloff, 1977). The Dutch CES-D showed good internal consistency and high convergent validity in several samples (Bouma, Ranchor, Sanderman, & Sonderen, 1995). Cronbach’s alpha in this study was .91.
Symptoms of PTSD were measured with the Dutch version of the 15-item Impact of Event Scale (IES; Brom & Kleber, 1985; Horowitz, Wilner, & Alvarez, 1979). The IES is a self-report instrument to assess changes in response action to potentially traumatic events. One of the scale items is as follows: “I tried not to talk about it.” Item scores are rated on a 4-point scale: 0 (not at all), 1 (seldom), 3 (sometimes), and 5 (often). Responses were summed to give total PTSD symptom scores (range: 0-75). A summed score higher than 26 indicates the probable presence of PTSD (Chemtob, Tomas, Law, & Cremniter, 1997; Mooren, de Jong, Kleber, & Ruvic, 2003). The Dutch IES has adequate internal consistency and convergent validity in samples of people afflicted by violence, calamities, or war (van der Ploeg, Mooren, Kleber, van der Velden, & Brom, 2004). Cronbach’s alpha of the IES in the current study was .85.
Well-Being
Self-efficacy was measured by the Dutch version of the General Self-Efficacy Scale (GSES; Bosscher & Baardman, 1989; Sherer et al., 1982). This scale contains 12 items regarding the expectations people have of their capacities. An example of an item is as follows: “If something looks too complicated I will not even bother to try it.” Item scores are rated on a 5-point scale ranging from 1 (strongly agree) to 5 (strongly disagree). Summed scores range from 12-60, and a higher total score is indicative of more self-efficacy (Bosscher & Smit, 1998; Bosscher, Smit, & Kempen, 1997; Woodruff & Cashman, 1993). The Dutch GSES demonstrated acceptable internal consistency and construct validity in samples of people older than 55 years (Bosscher et al., 1997). Cronbach’s alpha of the GSES in this study was .73.
Self-esteem was examined using the Dutch version of the Rosenberg Self-Esteem Scale (RSES; Rosenberg, 1965; van der Linden, Dijkman, & Roeders, 1983). The RSES measures global self-worth and contains 10 statements which can be scored on a 4-point scale ranging from 1 (strongly agree) to 4 (strongly disagree). One of the statements is as follows: “I wish I could have more respect for myself.” All items were summed to create the total score (range: 10-40), with higher scores indicating stronger levels of self-esteem. The RSES shows satisfactory reliability and validity with samples of abused women (Blascovich & Tomaka, 1991; Kim & Kim, 2001; Woods Cox & Stoltenberg, 1991). For this sample, Cronbach’s alpha was .86.
Social support was assessed using a self-developed question: “Do you get help or support from other people (e.g., seeking comfort, emotional support, getting things, arranging things)?” If affirmed, women were asked how many people provided support. A total score was obtained by adding the total number of persons from whom the woman received support, with a “no” answer to the first question coded as zero.
Data Analysis
Statistical analyses were performed using SPSS version 20.0. Frequencies and means were used to describe women’s sociodemographic characteristics, abuse-related variables, mental health, and well-being. Missing items on a scale were substituted with the individual’s mean score on the particular scale if no more than 20% of the items were missing (Shrive, Stuart, Quan, & Ghali, 2006). Otherwise, the women were excluded from the analysis.
We selected control variables based on associations with depression and PTSD in previous research (Jones et al., 2001; McGrath, Keita, Strickland, & Russo, 1990; Patel et al., 2010). Control variables consisted of age, migration background, number of children, and physical and sexual abuse by (ex-)partner. First, Pearson correlations were calculated to examine significant associations between the control variables, well-being, and symptoms of depression and PTSD. Second, correlations between the independent variables were inspected for multicollinearity. The highest correlation did not exceed .52, indicating there was no multicollinearity. Third, we specified two linear mixed-effects models for predicting depression and PTSD symptoms. In these analyses, shelter organization was specified as a random factor to account for non-independence of data. Marginal R2s were calculated to describe the proportion of variance explained by the fixed factors. The p values less than .05 were considered to be statistically significant.
Results
Participants
Characteristics of the study sample are given in Table 1. The 184 interviewed women averaged 32.6 years of age (range: 18-58 years) and 41.3% were married. The majority of women (82.6%) had children (range: 0-5) and more than half (57.1%) were from a non-Dutch background (predominantly Moroccan, Surinamese, or Turkish). Most of them (71.4%) were first-generation migrants (she and at least one of her parents were born outside the Netherlands). The remaining 28.6% of the women were second-generation migrants (born in the Netherlands and at least one of the parents was born outside the Netherlands). A quarter of the women (24.5%) had no education or finished only primary school. At the time of the interview, 83.2% of the women were unemployed.
Characteristics of the Women in the Study.
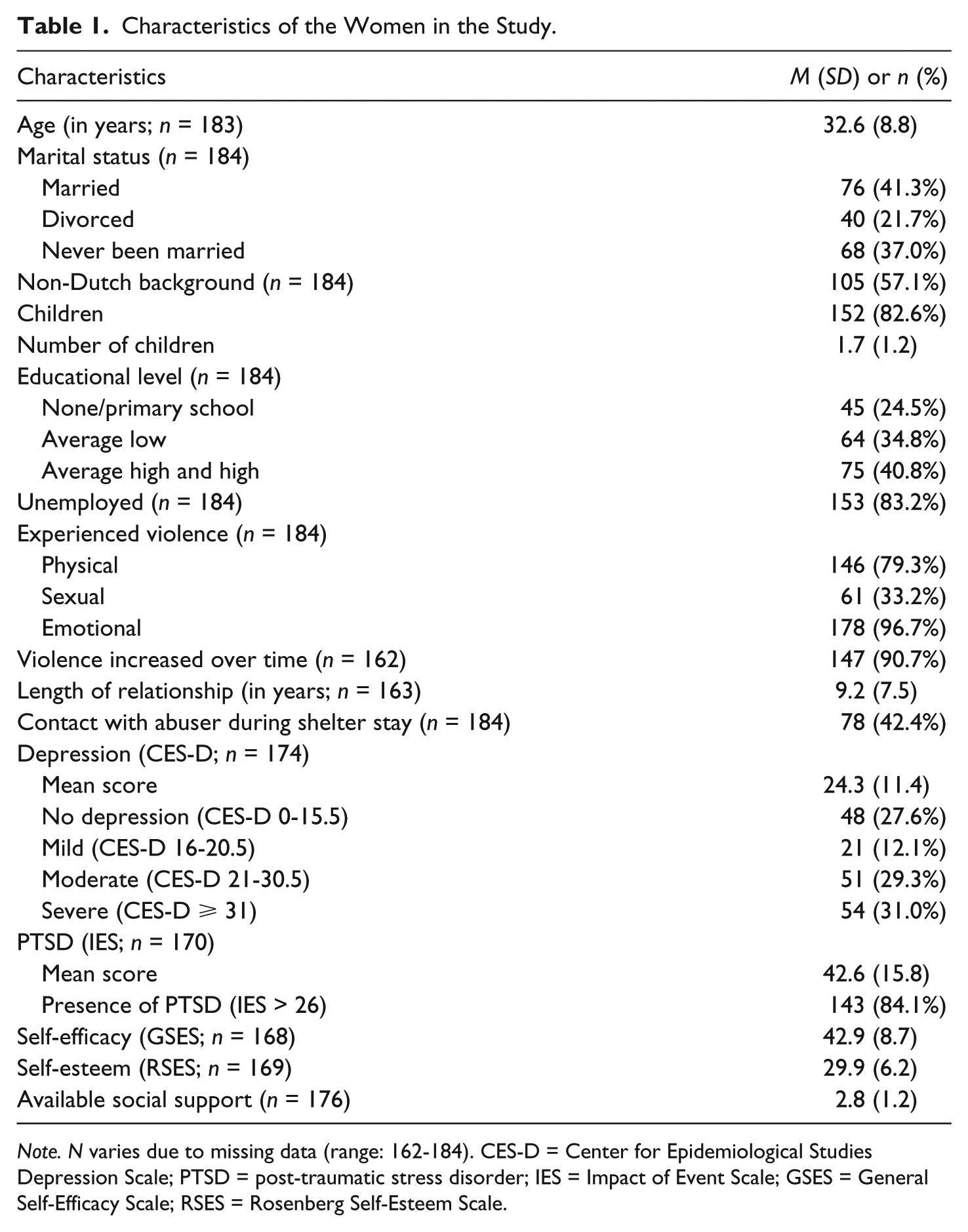
Note. N varies due to missing data (range: 162-184). CES-D = Center for Epidemiological Studies Depression Scale; PTSD = post-traumatic stress disorder; IES = Impact of Event Scale; GSES = General Self-Efficacy Scale; RSES = Rosenberg Self-Esteem Scale.
Nearly all women (96.7%) reported emotional abuse, 79.3% reported physical abuse, and 33.2% suffered sexual abuse by their (ex-)partner before shelter entrance. The mean length of the relationship with the abusive (ex-)partner was 9.2 years (range: 0.5-36 years), and most women (90.7%) reported that the violence had increased over time. Nearly half of the women (42.4%) reported having been in touch with the abuser during shelter stay.
Almost three quarters of the women (72.4%) reported symptoms of depression, and the majority (84.1%) were suspected to suffer from PTSD. According to Dutch norm scores, the mean self-efficacy score (M = 42.9) in the study group was average (Bosscher, Laurijssen, & Boer, 1992). With a mean score of 29.9, the women’s level of self-esteem was comparable with the score of women in the Dutch population (Sandfort, de Graaf, & Bijl, 2003). On average, the women mentioned two persons from whom they received social support (range: 0-4).
Missing Data
A total of 51 (23.4%) women were not included in the linear mixed-effects model to predict depression due to missing values for any of the scales in the analysis. In the model to predict PTSD symptoms, a total of 52 (23.9%) women were not included for the same reason. For most of them (n = 34), the cause was the use of the short version of the questionnaire due to language difficulties. The excluded women were significantly more often from a non-Dutch background (p < .001). No significant differences were found for age.
Univariate Analyses of Symptoms of Depression and PTSD
Table 2 shows the correlations between the outcome measures, the control variables, self-efficacy, self-esteem, and available social support. Depression scores were related to migration background, number of children, self-efficacy, self-esteem, and available social support. Depression scores were not related to age and physical and sexual abuse. Depression and migration background were positively related (r = .20, p = .01), indicating higher depression scores for women from a non-Dutch background. Women with more children reported lower depression scores (r = −.17, p = .03). Higher self-efficacy (r = −.39, p < .001), higher self-esteem (r = −.59, p < .001), and more available social support (r = −.33, p < .001) were also associated with lower levels of depression.
Correlations Between Control Variables, Well-Being, and the Outcome Measures.
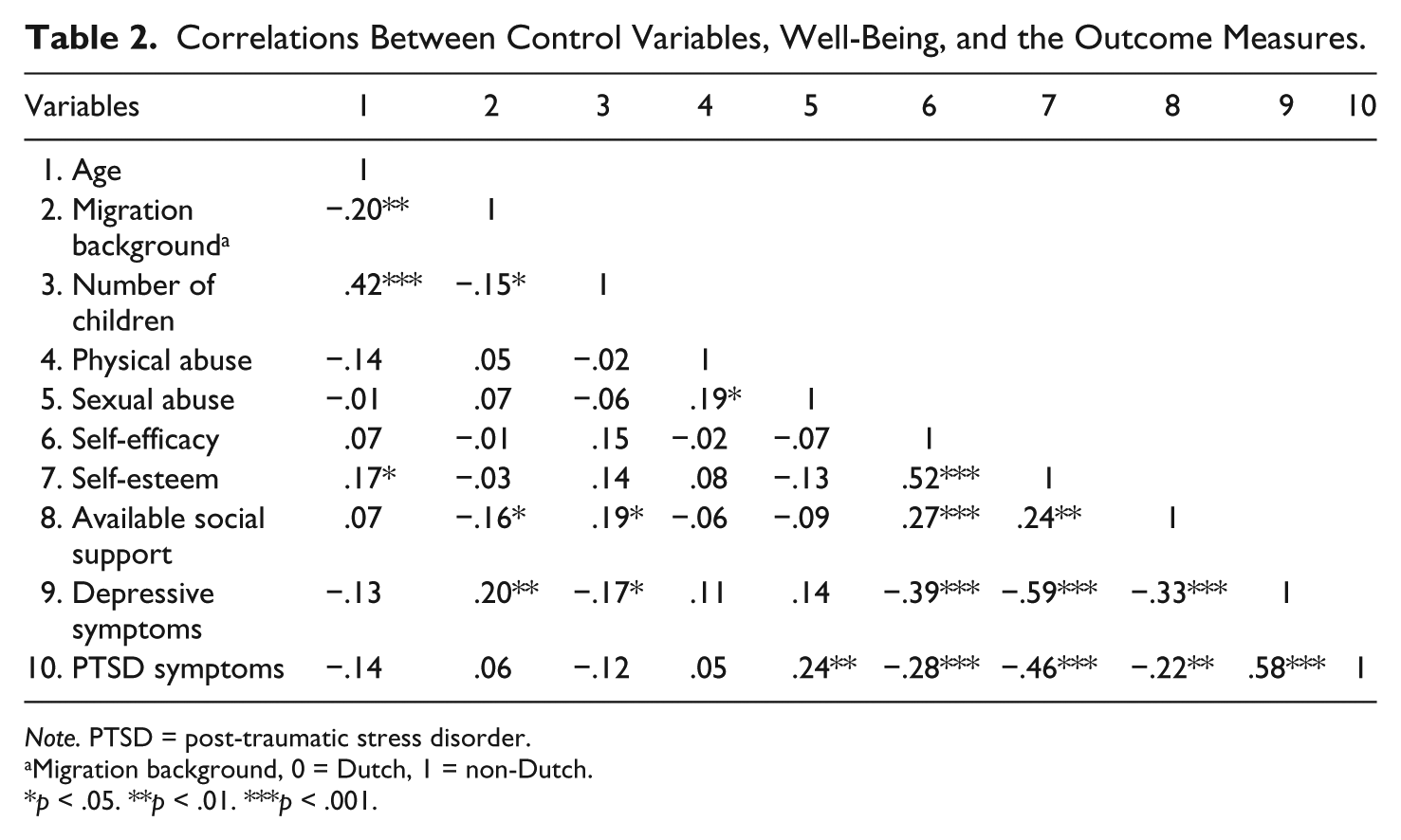
Note. PTSD = post-traumatic stress disorder.
Migration background, 0 = Dutch, 1 = non-Dutch.
p < .05. **p < .01. ***p < .001.
PTSD symptoms were related to sexual abuse, self-efficacy, self-esteem, and available social support. No associations were found with age, migration background, number of children, or physical abuse. Women who experienced sexual abuse, reported more symptoms of PTSD (r = .24, p = .002). As with symptoms of depression, higher self-efficacy (r = −.28, p < .001), higher self-esteem (r = −.46, p < .001) and more available social support (r = −.22, p = .01) were associated with lower levels of PTSD symptoms.
Linear Mixed-Effects Models
The results of the two linear mixed-effects models evaluating the contribution of self-efficacy, self-esteem, and available social support in symptoms of depression and PTSD are presented in Table 3. After controlling for the effects of age, migration background, number of children, and physical and sexual abuse, both self-esteem and available social support remained significantly associated with symptoms of depression, while self-efficacy showed no effects. A non-Dutch background and having experienced physical abuse were significantly associated with higher levels of depressive symptoms. Self-esteem and available social support were associated with significantly lower levels of depressive symptoms. For example, for a 1-unit increase in self-esteem, depressive symptoms decreased with 0.97 points. The marginal R2 value of this model was .38.
Results of the Linear Mixed-Effects Models for Depression (n = 167) and PTSD (n = 166).
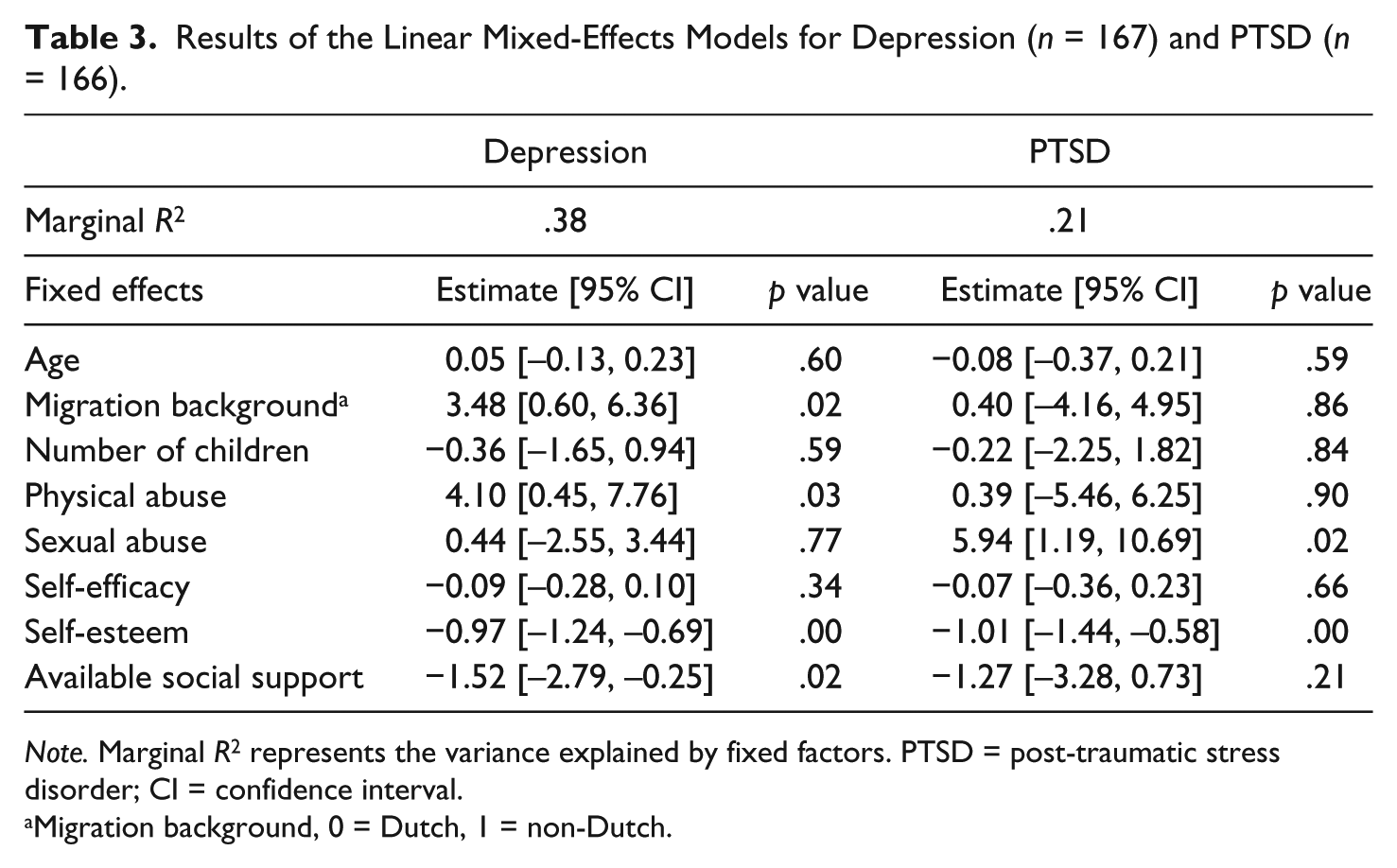
Note. Marginal R2 represents the variance explained by fixed factors. PTSD = post-traumatic stress disorder; CI = confidence interval.
Migration background, 0 = Dutch, 1 = non-Dutch.
Regarding PTSD symptoms, after controlling for the effects of age, migration, number of children, and physical and sexual abuse, the model shows only a significant association with self-esteem. The experience of sexual abuse was associated with higher levels of PTSD symptoms. Self-esteem was associated with significantly lower levels of PTSD: for a 1-unit increase in self-esteem, PTSD symptoms decreased by 1.01 points. The marginal R2 value of this model was .21.
Discussion
This study provides important information about factors related to symptoms of depression and PTSD in a Dutch shelter-based sample of abused women. In this sample, the levels of depression and PTSD are high. The scores of self-reported depressive symptoms (M = 24.3, SD = 11.4) are within the clinical range. More than 70% (72.4%) of our sample had scores above the cutoff score of 16 (indicating at least mild clinical depression). Similar high rates of CES-D scores were found in abused women at shelter entry (Lewis et al., 2006) and at shelter exit (Campbell et al., 1995).
Regarding women’s PTSD symptoms, high IES scores (M = 42.6, SD = 15.8) were found, with 84.1% of the women meeting the threshold for a probable PTSD diagnosis (Foa, Riggs, Dancu, & Rothbaum, 1993; Lewis et al., 2006). These scores are comparable with the shelter samples of Ham-Rowbottom et al. (2005) and Kemp et al. (1991).
Our findings confirm an earlier report showing that the prevalence rates of depression and PTSD are the highest in sheltered IPV survivors (Golding, 1999). Across diverse samples, comorbidity between PTSD and depressive symptoms is common; almost half of the people diagnosed with PTSD are also diagnosed with depression (Cascardi et al., 1999; Dillon, Hussain, Loxton, & Rahman, 2013; Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995; Nixon et al., 2004; Rytwinski, Scur, Feeny, & Youngstrom, 2013; Stein & Kennedy, 2001). In a study of PTSD and depression prevalence within a shelter sample, Nixon and colleagues found that 75% of IPV survivors were diagnosed with PTSD and 54% were diagnosed with depression (Nixon et al., 2004).
To examine which factors (i.e., sociodemographic variables, abuse-related variables, and well-being variables) were associated with symptoms of depression and PTSD, we examined the univariate relationships between CES-D and IES scores, the control variables, self-efficacy, self-esteem, and available social support. Two linear mixed-effects models showed that factors predicting depression were migration background, the experience of physical abuse, a lower level of self-esteem, and low available social support. PTSD symptoms were predicted by the experience of sexual abuse and lower levels of self-esteem.
Although limited research has been conducted in shelter samples, our findings are in line with other research that depression was related to physical violence (Campbell et al., 1995; Cascardi et al., 1999). However, we did not replicate earlier findings that physical abuse was related to PTSD symptoms (Cascardi et al., 1999). An explanation for not finding an association between the presence of physical abuse and PTSD symptoms may be the measurement of abuse-related variables. In our study, women could indicate whether or not they experienced physical abuse in the past. This resulted in a high rate of physical abuse experienced (approximately 80%), with limited variance to detect differences. We confirmed, however, that PTSD symptoms were related to sexual abuse similar to previous studies (Bennice et al., 2003; Pico-Alfonso, 2005). Sexual abuse within an intimate relationship has been shown to be an independent factor contributing to severity of PTSD symptomatology, even beyond the impact of physical abuse (Bennice et al., 2003).
Our study showed that a lower level of self-esteem predicted both symptoms of depression and PTSD. Other studies also found associations among self-esteem, IPV, and mental health outcomes (Bradley, Schwartz, & Kaslow, 2005; Campbell & Alford, 1989; Cascardi & O’Leary, 1992; Sato & Heiby, 1992; Zlotnick et al., 2006). It is possible that self-esteem and depression as well as self-esteem and PTSD are associated because they may share underlying constructs, and items on the instruments may show overlapping content (e.g., with measures of personality and affect; Kernis, 2013).
Women in the current study who reported having lower levels of available social support experienced more severe depressive symptoms. These findings are consistent with previous literature on shelter samples (Campbell et al., 1995; Coker et al., 2002; Mitchell & Hodson, 1983). Other research has indicated that supportive networks may protect women from re-abuse (Bowker, 1984; Goodman, Dutton, Vankos, & Weinfurt, 2005; Krishnan, Hilbert, & VanLeeuwen, 2001; Tan, Basta, Sullivan, & Davidson, 1995; Thompson et al., 2000).
A remarkable finding in the current study is that migration background was related to symptoms of depression. A study including Dutch women attending general practices showed that migrants were significantly more often victims of IPV and suffered more frequently from severe depression than Dutch women (Prosman et al., 2011). Previous studies found that migration status is not necessarily associated with IPV (Du Mont & Forte, 2012; Wong et al., 2011).
Limitations
Our study has some limitations that should be taken into account. First, it was a cross-sectional study that does not allow any inferences about temporal or causal relationships. Moreover, although we tried to recruit a random sample of women admitted to shelters across the Netherlands, 46% of women who were eligible to participate in the study were not screened or interviewed. An additional 34 women had to be excluded because of missing data due to the use of the shortened version of the questionnaire for women who did not speak Dutch, possibly biasing and limiting the generalizability of our results. Moreover, the way we measured physical abuse (we did not ask the number of abuse experiences and the severity of physical abuse), truncated the range on this variable and may have limited our ability to detect significant correlations with depression. Furthermore, our findings are limited only to help-seeking female IPV survivors residing in women’s shelters. In addition, the use of self-report instruments to assess symptoms of depression and PTSD may have led to over-reporting, as shown in previous studies (Engelhard et al., 2007). In our study, the report of women’s PTSD symptoms should be interpreted with caution. In some cases, women resided in the shelter no longer than 3 weeks and may still be in a situation where there is threat or danger. Therefore, some of the women may clearly display criteria associated with PTSD but may not qualify for the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) PTSD diagnosis because the time criterion of symptom presence of at least 4 weeks is not met (American Psychiatric Association, 1994). Further assessment will be necessary to make an accurate diagnosis of psychopathology. Finally, diversity in cultural background may have impacted the results.
Research Implications
Our study is among the first to report predictive relationships in depression and PTSD symptoms in women residing in shelters, who suffered more extreme levels of abuse. There is a great need for more research into this vulnerable group of IPV survivors, for example, randomized controlled trials (RCTs) evaluating shelter interventions. The high levels of depression and PTSD found in this shelter sample warrant adequate mental health consultation. Further research is needed to evaluate the efficacy of shelter staff conducting routine assessment of depression and PTSD, to indicate mental health treatment by a professional within or outside women’s shelters.
Clinical & Policy Implications
The presence of symptoms of depression and PTSD in the majority of our shelter sample reveals the importance of specialized mental health treatment, yet few shelters offer such service. Shelter staff’s counseling consists of education to increase understanding of patterns of violence and linking women to resources in the community (Woodcock, 2007). The most effective interventions for individuals experiencing depression and PTSD appear to be cognitive-behavioral treatments (CBT; Bisson, 2007; Foa et al., 2005; Iverson et al., 2011; Nathanson et al., 2012). Prolonged Exposure (PE) and Cognitive Processing Therapy (CPT) are the two specific CBT treatments offered (Resick et al., 2008). Eye movement desensitization and reprocessing (EMDR) is effective as a treatment for symptoms of PTSD (Seidler & Wagner, 2006; van Etten & Taylor, 1998; van Minnen, Hendriks, & Olff, 2010).
More insight into factors that influence symptoms of depression and PTSD in abused women may assist shelter workers and other health care professionals in providing appropriate care as well as in developing effective programs for treating the negative health outcomes of IPV, focusing on factors that are amenable to modification, such as self-esteem and available social support. Professionals may help women build and maintain a sustainable social support network and, to improve their self-esteem, improve women’s capacity to fend for themselves and help them strengthen their ability to cope (Jonker, Jansen, Christians, & Wolf, 2014). Research showed that a strengths-based approach for abused women and their children in which advocates were instructed to focus on actively assisting mothers to access community resources, caused improvement in women’s depression and self-esteem over time (Sullivan, Bybee, & Allen, 2002).
The current study showed high rates of depression and PTSD, and it has expanded our understanding of factors that influence symptoms of depression and PTSD in a shelter sample of abused women. These findings speak to the importance of shelter workers paying attention to the mental health problems women are experiencing and underline the necessity for appropriate shelter interventions.
Footnotes
Acknowledgements
We would like to thank the clients and professionals in all the women’s shelters for their participation in this research project.
Authors’ Note
The first two authors contributed equally.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.