
Abstract
Complex health care interventions often consist of specific and non-specific effects and can present a methodological and intellectual challenge to researchers. This is especially the case in Complementary and Integrative Medicines (CIM), where research may inadequately capture the holistic nature of therapies, affecting the quality of outcomes and evidence reported. This article introduces a novel approach that advances methodology and helps researchers to “step inside” the therapeutic drama, to improve the quality of evidence produced. The method, termed Theatricality, was trialed in five complementary health centers across four European countries and provides a fresh view of therapy, where the interventions, practitioners, and researchers appear bound by their context and space, creating, or limiting the potential for these acts. Delivered as an adjunct to Ethnography, this approach offers a new way of conceiving, capturing, and communicating whole health care performances that may help to improve the quality of evidence in complex health care interventions.
Keywords
Introduction
Complex health care interventions require research approaches that capture both their specific and non-specific actions and effects. The UK Medical Research Council (MRC) published a framework for researchers and research funders on developing and evaluating complex interventions in 2000 (Campbell et al., 2000), with updates in 2008 (Craig et al., 2008) and in 2021 (Skivington et al., 2021). Complementary and Integrative Medicines (CIM) are complex health care interventions that include many fields of therapeutic specialty and may also be delivered in a variety of health care settings including outpatient and inpatient; primary, secondary, tertiary, and private care; and health education and research (Kienle et al., 2019).
It is a foundation of holistic philosophy that the whole is greater than the sum of parts (Paterson & Britten, 2008). In health and healing, this means it is the cumulative effects of all things (not just theory and practice), that creates the potential for either wellness or illness to occur. In CIM research, many trial and study designs can struggle to embody this principal. This means efforts that aim to challenge and understand the value of various contextual elements within therapeutic encounters often observe or study these as isolated aspects only (Boon et al., 2007; Bradbury et al., 2016; Fønnebø et al., 2007; Hawe et al., 2004; Ho et al., 2021, 2022; MacPherson & Thomas, 2008; Williams & Kamper, 2012). However, the assumption that specific and non-specific effects of an intervention can be considered as separate, non-interacting phenomena, may be an over-simplification (Milgrom, 2014).
CIM research is largely driven by the aim of building therapy evidence in line with other allied health approaches: using randomized controlled trials (RCT); evidence-based medicine (EBM); pursuing efficacy beyond placebo; and/or reducing holistic treatments to their individual components (Chiappelli et al., 2005; Eisenberg et al., 1993; Fung & Linn, 2015; Thompson & Weiss, 2006; Witt & Holmberg, 2012). Much debate remains about the validity and feasibility of applying the RCT or EBM model alone in CIM, raising concerns that where the sum of the parts fails to adequately capture the whole, evidence will be inconsistent or unreliable and lead to false negative results (MacPherson & Schroer, 2006; Milgrom, 2014).
The ongoing failures of CIM research to not sufficiently value or publish contextual data suggest a challenge to engage holistically with these phenomena, which limits the value of such work. Some variables have been explored within CIM practice; however, there is still a dearth of studies exploring “whole of practice,” highlighting the complexity of this. Reliance on reductionist approaches limits our understanding of variability on therapy experience and patient outcomes, while calls have long been made for a clearer characterization of treatment processes to support more appropriate design of therapy evaluations (MacPherson et al., 2006) and, more recently, some consideration of how indigenous and western worldviews can seek to reconcile this issue (Massey & Kirk, 2015). This creates a starting point to consider the adequacy of different approaches to researching complex health care performances, including CIM, and the knowledge this produces.
This article describes the development and first application of a novel research methodology and method, aligned with a holistic paradigm, that researchers across a variety of disciplines (not only health care) may find useful for conceiving, capturing, and communicating complex social and lived performances.
Holism in Health care Research
It is striking that the recommended lens for the practice of CIM therapy and research can be so different. For therapy, the aim is often to take the various fragments a patient brings to their session and restore wholeness to them in whatever way one is able, guided by the holistic principles and philosophy underpinning the modality being used. For a researcher, the aim is conversely to take wholeness and fragment it into smaller pieces to enhance understanding and generate evidence, guided by the reductionist principles and philosophy of scientific inquiry. This creates a novel research–practice gap, where the design, conduct, and reporting of studies that contribute to the evidence base in CIM struggle to reflect the paradigms within which real-world practitioners may operate. Equally, research evidence may struggle to be implemented into clinical practice, where this does not appear relevant to how practitioners work. Such dichotomy has the potential to undermine and devalue practice, and limit meaningful clinical benefits.
A further paradox within this is that, while CIM research evaluations typically focus on the effect of interventions on specific problems, in real-world practice many CIM therapies aim to treat the whole person, not just their problems. This can lead CIM research to perpetuate a reductionist approach to health and illness that is often incongruent with real-world practice and the intentions behind any treatments, and challenges the potential value of any study published. The evidence base within CIM should be generated with quality and rigor, and so it is important for the “research agenda” to complement the “practice agenda,” to achieve both transferability and trust in research outcomes.
Cassidy’s (1994) now dated, but seminal text highlights the lack of congruence and resonance between the paradigms/processes of popular research methodologies and CIM therapies, and remains as relevant now as when it was written; the result being that both policy and provision are impacted by limits on research in this area. To apply the principles of CIM to research in this area would ensure that any appraisal is multi-dimensional and loaded with “equal if different value” (Cassidy, 1994:11). There is a unique opportunity for those working in this field to champion a more congruent approach to the modalities they investigate and support the use of complementary and integrative health care practices for patients with quality evidence.
Theatricality as Method
To meet the challenge of exploring the gaps and enhancing research design and reporting in CIM, we developed Theatricality, a method based upon two central ideas: that every room or public space has “a design that sets up potential relationships between people” (Read, 2005:53); and that social situations can be perceived and described using the language of theater (Burns, 1972).
To translate this concept into an applied research method, we developed a simple yet focused research schedule (Table 1) and constructed a holistic approach that includes various Acts, to provide a baseline structure for capturing the richly complex and comparable data across a variety of health care settings and sequence the work that would underpin each of these Acts. The primary aim of this was to ensure the researcher sees whatever is there to “be seen,” rather than what the researcher may or may not want to see. Employing this “structure” for viewing therapy spaces like theater sets was a useful “anchor” that worked well across our range of different therapeutic, geographic and cultural settings.
TFM Observation Schedule.
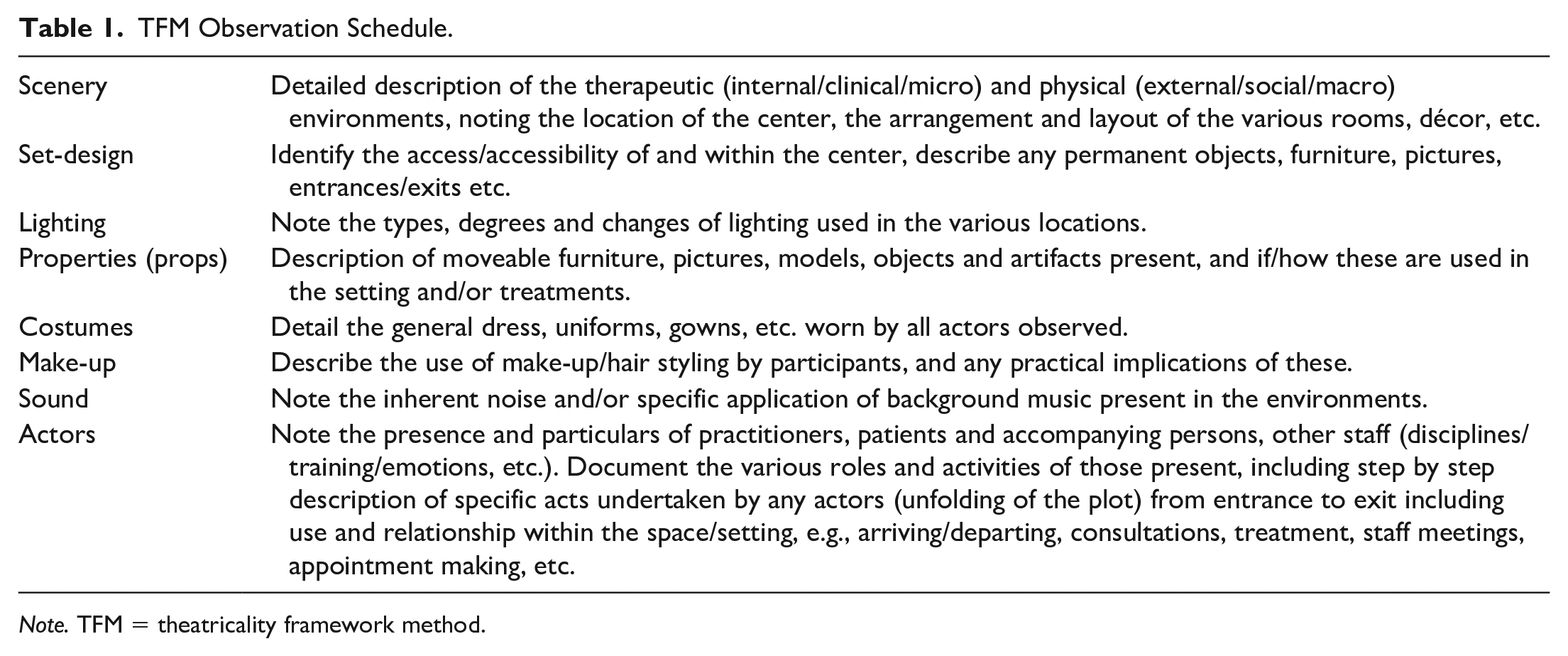
Note. TFM = theatricality framework method.
This baseline structure, termed Theatricality Framework Method (TFM), supported the participant observations and in-depth interviews by enabling a more holistic immersion within the constructed nature and fabric of the field settings, providing a thorough foundation for engagement with: (a) the spatial context; (b) actions that occur within the space; and (c) the dialogue/stories of other patrons and actors. This “intimate knowledge” was essential for us to “penetrate [participants] circle of response” (Goffman, 1989:125).
Act 1: The Spatial Context
Whatever their primary purpose, performance spaces are composed of scenographic elements (i.e., scenery, set-design, lighting, properties, costumes, make-up, and sound). Using this natural scenographic framework to document complex spatial composition revealed a dynamic and holistic complexity with potential to impact both the characters and the unfolding plot (why theater directors take such care when “staging” their productions). Taking the view that health care settings are just as carefully staged as artistic settings, we documented these scenographic elements and revealed a level of detail that could otherwise be routinely overlooked, which provided a route for the researcher into a level of immersion close to that of the original “creator.”
Guided by this TFM observation schedule, each space (external, communal, and therapeutic) encountered was viewed from the perspective of an audience member and described as if it were a carefully constructed theater set. Set plans (sketches) and notes were made in a fieldwork journal, under their relevant scenographic heading, detailing the choice, composition and placement of materials and objects, and the relative impact of these within the whole scenic composition and overall performance. The thickness of these descriptions could run into several pages and describe elements of the setting that some researchers may consider superfluous, particularly in regard to therapeutic application. However, it was not the role of the researcher to decide what is important and what is not, nor to pre-judge what aspects of the spatial context may or may not have active purpose, in the “scene as a whole.”
Embedding the researcher’s engagement with these spatial dynamics to a level comparable with that of the creator or architect of the space made it possible to achieve a level of familiarization beyond that expressed even by some participants, for whom such relationships could often be tacit or implicit. As an activist in the art of documenting various field sites, the researcher was duty-bound to ensure that each description provided sufficient detail of the “space” that (in theory) these could be re-created or re-enacted in another location (as a theater production “on tour”). This brought an added benefit of making “stage directions” simpler to create and, in later action observations and participant interviews, prepared the researcher to adopt the role of informed interviewer, able to better empathize and therefore engage with any commentary made.
Act 2: Actions That Occur Within the Space
Formal observations typically occurred after individual settings had been fully described, documented, and appraised. Co-operation with therapy practitioners was an essential aspect of this, and all observations were structured around existing daily practice schedules, to cause as little disruption to everyday working as possible. These were often completed while performances were in progress, and captured in the form of detailed stage directions: noting entrances and exits, use of props, dialogues, and so on. After the scenes concluded, reflexive/side comments were added, to become part of the whole data set. Where aspects noted also related to observations within the treatment area, descriptions were used to compare or contrast the data. Where treatment observations were absent, they supported and contextualized the interview data and character monologues, enabling a more rounded picture. During all data collection, the primary focus of attention was the actions, with the researcher’s responses to these becoming clearer or more actively engaged during re-listening to the audio-recorded interviews or reflexive analyses.
This also provided an active-reflexive opportunity to participate in observation with synthesis, and holistic appreciation of the acts, as they were witnessed. To be holistically faithful to the phenomenon of whole therapy practice, the researcher had to be open to it; not only to observe and talk to people but to also gain a personal contextual understanding of their experience and realities, alongside their own.
Act 3: The Dialogue/Stories of Other Patrons and Actors
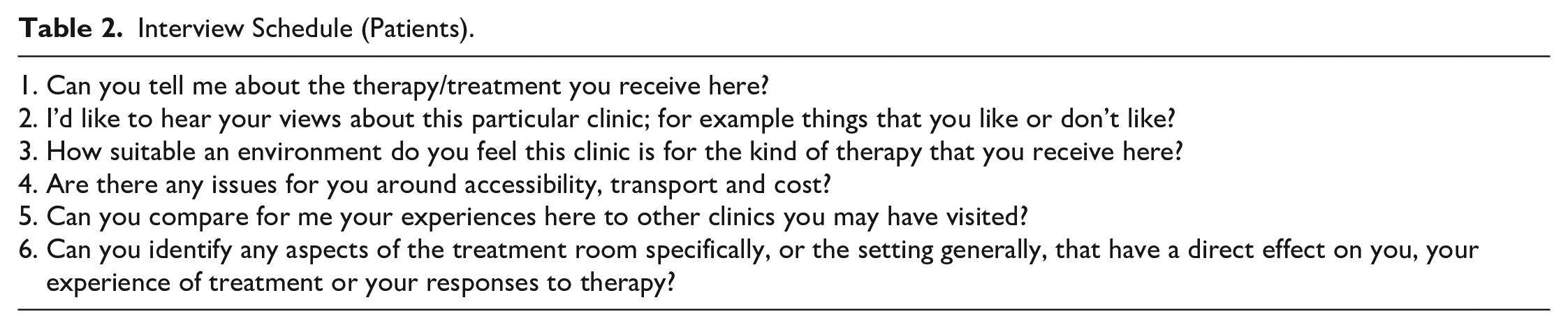
As a further dimension to the data, semi-structured in-depth interviews were conducted with practitioners and patients, across all sites. Under the concept of “whole therapy experience,” these explored the wider contextual experiences of therapy; from choice, style and use of the general and local settings (including physical and dynamic factors) and the motivations or journeys into therapy of all involved (patients, clients, practitioners, and therapists). Two distinct yet similar schedules of questions guided these: one for patients (Table 2) and one for practitioners (Table 3).
Interview Schedule (Patients).
Interview Schedule (Practitioners).
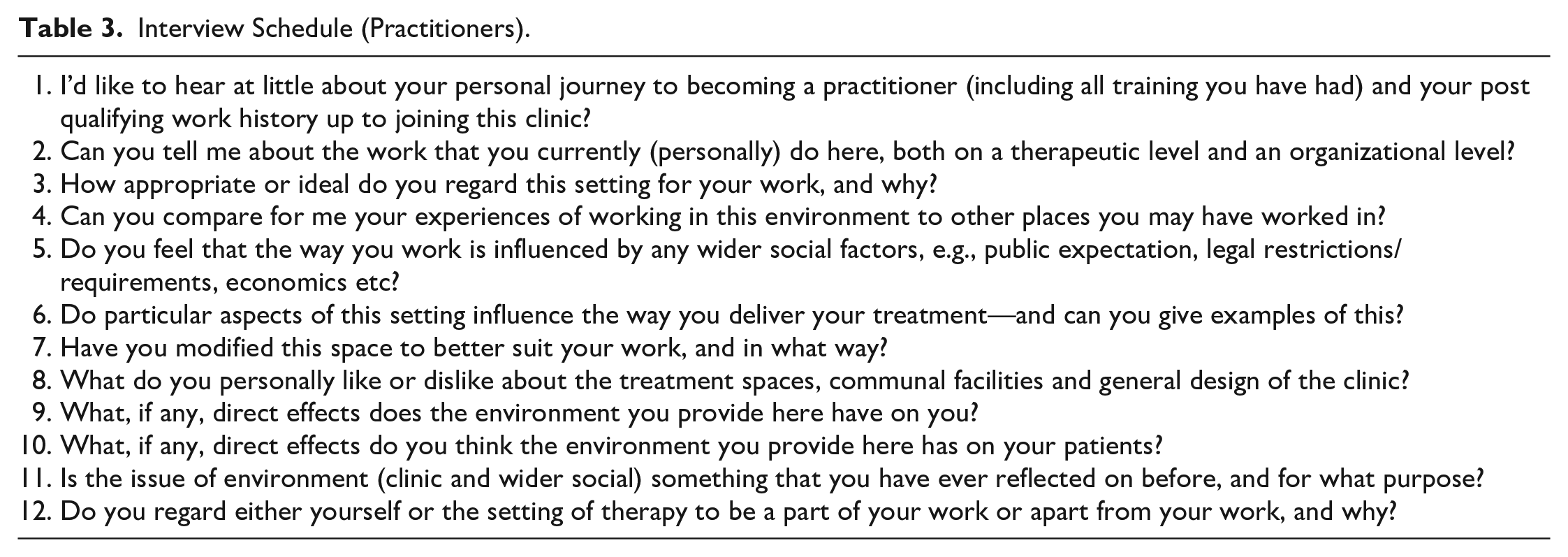
Patient interviews lasted a maximum of 30 minutes and practitioner interviews lasted a maximum of 60 minutes. Timings varied across the sample with participants for whom English was not their first language often taking longer to articulate their meanings, or employing other communication techniques (such as metaphors or mime) to ensure a clear understanding of their intention. When these schedules were flexibly applied, participants first volunteered the information they felt it most important to share or wanted to share. They were brought back, where necessary, to specific items or issues that had been captured and/or otherwise required clarification, if these were not addressed in initial responses. Any gaps were filled to ensure that findings could be comparable across different individuals and the different settings. Each interview concluded with an opportunity for participants to share anything they regarded as important that had not been previously covered. This proved a great source of “gems” with some inclusions enriching the data beyond expectation. The volume and depth of personal perspectives this revealed about the role and value of health care context and settings to the whole experience of therapy uncovered a clear sense of how these influence both the experiences of delivering and receiving therapeutic treatments.
Fieldwork in Action
Fieldwork was constructed in four phases and designed to immerse the researcher within the clinical and wider lived environment. Phase one was conducted at a single-site U.K. clinic, phase two was with a split-site Holland clinic, phase three was at a single-site Cyprus clinic and phase four was with two separate Denmark clinics. Researcher living arrangements for each phase were within reasonable proximity to clinic sites and played a crucial role in framing the research performance, providing a mindful insight to the wider social context and experiences of participants. This embodied experience supported dialogue and engagement with other characters and their stories (i.e., comparing experiences of the local setting, travel modes to attend the clinics). It also provided a means of comparing the impact of different contexts and settings on the research process (i.e., recruitment, data collection, analysis, and reflexivity). During each phase, the researcher attended clinical sites on each weekday, and explored the wider social aspects and locations on weekends.
In this generation, interpretation, reflection, analysis, and synthesis of the data set, we crafted the opportunity for appraisal of the whole performance of therapy and revealed a different side to the phenomenon usually overlooked. Basing therapeutic experience not on externally measurable outcomes, but on internally subjective ones also raised an “intrinsic transferability” (Avis & Freshwater, 2006:223) that meant we could identify commonalities and contrasts between practitioners and patients of different therapy approaches, in different places.
Performative Criticism as Holistic Analysis
We introduced and used “Performative Criticism” as a novel approach to data analysis, to appraise this holistic data set. A term first suggested by Toporisic (2011), to identify a potential new method of heuristic analysis (Moustakas, 1990), it embraces the whole experience as a “unique spatio-temporal event” and “performance as a kind of cultural participation” (Toporisic, 2011:1). Repositioned here as a form of critical inquiry, we explored the potential for this to “become specialised in the area of analysis of cultural and artistic phenomena” (Toporisic, 2011) as it requires the researcher to critique events from within as a co-actor or participant, rather than as an outsider or “foreign afar.” This approach gave us permission to widen the “space” for relating to and with the data in a more real and subjective way than any previous understanding of either reflexivity or reflective practice. It allowed entry into the data.
We devised a data extraction sheet (Table 4) to provide assistance in identifying and locating live interview commentary regarding the setting, plot, characters, and dramatic experiences. We then evaluated this in relation to our other data forms (images, descriptive notes, and observational records), to evidence and construct whole therapy experience as more than the sum of its parts.
Data Extraction Sheet.
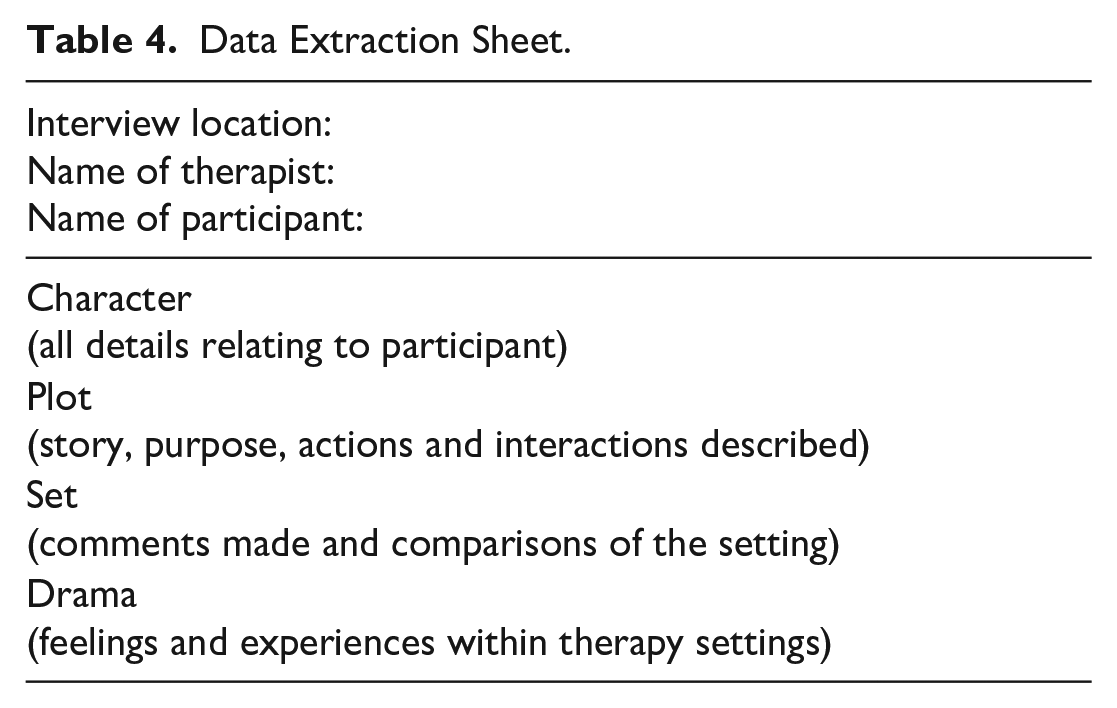
Interpreting and extracting interview data as a live medium was a cogent approach with the “performative criticism” method proposed (whereby the critic engages within the performance data) and what Shapiro and Hunt (2003:923) call the “uniquely compelling emotional quality” of participant experiences not always present within silent text, resulting data and analysis. This added dimension of meaning in the “human voice” (Smith & Gallo, 2007) directed appreciation to not only what people said but also how they said it, and illuminated a vitality of words that can be absent within dry text.
Theatricality as Methodology
Theatricality methodology is proposed as a novel approach for studying complex social practices including CIM which, as a therapeutic system, is characterized by an innate variability in practices and raises significant challenges that is increasingly shared across other health care disciplines. Use of a theater concept provides unique potential as both CIM and Theater represent global worlds where everything inside is a vital part of the whole event and, as a framework for researchers, can offer the opportunity to engage creatively and holistically with the complexity of CIM practice, its’ characters, and settings. Read (2005) argues that viewing space not as an art of composition or engineering but as a “performing art,” creates the possibility of reflecting “real situations, characters, and places . . . in real time, at a real scale, and with real people” (Read, 2005:53). Delivered as an adjunct to ethnography, this approach may provide a discrete, sensitive, and creative observation where the researcher is also a character/actor in the drama, opening a space for noting unique or complex matters and weaving these (setting, props, or costume detail) into the narratives (Goodall, 2000).
The theatrical metaphor, while not usually applied in clinical care, is well established. Its historical use has been common within the fields of philosophy, psychology, anthropology, ethnology, and sociology (Fischer-Lichte, 1995b:85), with examples also evident within Business (Anderson, 2005), Marketing (Fisk & Grove, 1996; Goodwin, 1996), Organizational Management (Gardner, 1992; Graham-Hill & Grimes, 2001; Harvey, 2001; Oswick et al., 2001; Walker & Monin, 2001; Wood, 2002), and Politics (Mazzone, 2022; Moulaert & Paris, 2013). More recently, examples have been seen within medicine, with Helman (2001:5) directly comparing spaces such as a doctor’s office, hospital ward or holy shrine “to a theater set, complete with scenery, props, costumes and script,” and Hall-Flavin (2020:15) describing how the experience of “medicine contains a substantial theatrical element, with representational scenery, roles (doctors, nurses, patients), costumes (white coats, indiscrete patient gowns), performance (lectures, bedside rounds, Morbidity and Mortality conferences), and simulation of mentoring models.”
Applying the theatrical metaphor as holistic research methodology brings a fresh dimension to these whole events, and creates the opportunity for “doing CIM,” just as Glass (2012) talks of “doing scene,” to go beyond observing the practices and effects of any interventions and seek understanding of the factors that underpin how space, identity, and power contribute to and manifest within these. As Mazzones (2022) theatrical conception of power is a product of blending Goffman’s (1959) dramaturgical perspective with Actor Network Theory (Müller, 2015) and Burke’s (1955) dramaturgy, so does Theatricality methodology offer a further development of these concepts.
Theatricality Concept 1: Setting the Scene
Congruent with theater semiotics, Myers (2010) describes setting the “scene” for therapy as perhaps the most embodied and yet overlooked part of clinical productions, relating much within “healing” to “the performance.” This active backdrop supports and enables all presentations and performances, and so can be considered worthy of capture and exposition, to evidence the underlying discourse of the place and/or those who work there. Containing both cues and clues to the intent and expectations of any characters, and influencing multiple aspects of the whole production including therapy experience, “the design contribution may be limited to the functionalistic or merely decorative. Conversely, it may be integral to the realisation of the text, counterpointing theme and ideology, image and symbol, in pictorial terms.” (Aston & Savona, 2013:144). This means it should be considered a vital element within the whole context of the performance (Glass, 2012).
Theatricality Concept 2: Finding the Plot
Storytelling is a powerful means of generating research data, and can be a useful way for people to “make sense of their lives and construct their versions of reality and identity” (Holloway & Freshwater, 2007). Within each story, the elements of past, present, and future mean that data are never limited to only the immediate observations, but rather to a series of single events or episodes within a much larger story, locating “their ‘now’ experience in a context of ‘back then’ and ‘not yet’” (Holloway & Freshwater, 2007). Together, these “individual narratives [and] the cultures within which they are told” (Kirkman, 2002) can be said to constitute the “plot” and provide “the means by which narrative events are structured, organised and presented” (Aston & Savona, 2013:21). The plot, whether constructed or improvised, will direct the action and help each story to flow to its natural conclusion. Events with a “shape” are observed and compared between productions and/or sites. Typical aspects within therapeutic encounters may be: the purpose of the visit; a detailed account of the interactions or interventions that are applied; interpretation of both spoken and unspoken dialogue; and any responses that are achieved from these within each individual scene. That is the plot of therapy.
Theatricality Concept 3: Dramatic Data
The drama in therapeutic performances results from the multi-level and multi-dimensional experiences of each character and can provide unique depth to the data. Capturing this in “live performances” and original interviews creates the potential for participants to communicate directly with audiences, through and beyond the researcher (Jones, 2002). For maximum effect, the researcher should also listen and engage with all the different sounds, smells, and feelings of each conversation as they occurred “in the moment,” wherein each creates different possibilities for response. Honoring the use of inflection in participant voices, any repetition and searching for the correct “word,” or the emotive choice of language can help direct analysis toward the most important replies and observations and reveal a different “drama” than is possible when transcribing and coding “dead” text alone. Synthesizing and crafting the data into character monologues makes it possible to (re)present the beliefs, intentions, and experiences of the individual therapies and therapists into the final performance.
Theatricality Concept 4: Performing Research
The “Theatricality” proposed here is different in application from other arts-based and dramaturgical research approaches, which may focus on recording and noting behaviors in “space” and attribute outcomes to either the characters or plot (fitting the four key dramaturgical concepts of comedy, tragedy, melodrama, and farce). It goes beyond the “performance turn” described by Denzin (2003) that seeks to make lived experiences “visible” by creating performances from field notes and textual data. Our method prospectively engages the key scenographic categories of scenery, set-design, lighting, properties, costumes, make-up and sound as living dimensions within the holistic performances, and records the characters stories and experiences within these in interviews, to provide a novel and holistic clarity about how characters engage with and take/make meaning from such composition.
This raises a parallel between society and “theatre” as heuristic and constructed cultural models with the “capacity of constructing reality” (Fischer-Lichte, 1995b:89). Viewing one as a reflection of the other, each constructed setting can each be regarded a result of complex components that create a space for performances within which a deeper, nuanced engagement may facilitate better critical reflection on the “process of construction and the conditions underlying it” (Fischer-Lichte, 1995a:104). This fits with the distinct “spatial turn” also seen in the humanities and social sciences, which emphasize “the connections between self, space and place” (Filmer & Rossmanith, 2011:228) and the use of theater semiotics beyond traditional boundaries, as in Pantidos et al.’s (2010) study of the materiality in teaching spaces. As a concept, theater is a “world” where different systems of thought, practice and knowledge production combine to become matter and meaning, in a reality where we are both subjects in our own little worlds and at the same time part of a pulsing, quickening whole of affect, body, story, light and space (Hartnell, 2021).
Discussion
CIM is a complex health care intervention and social phenomenon. Surveys from several European countries suggest increasing use over the recent decades with up to 70% of citizens having used some form of CIM (Nissen et al., 2012) and the most recent U.K. data showing prevalence of 26.3% (Harris et al., 2012). This trend raises the need for a quality CIM evidence base. Members from the Whole Systems Research (Langevin et al., 2011; Ritenbaugh et al., 2008) and CAMbrella research (Weidenhammer & Brinkhaus, 2012) groups have shown the diverse range of contextual variables present within real-world CIM, which raises a challenge for researchers wishing to engage these complex, often unfamiliar worlds. To meet this challenge, we proposed a holistic route to future study of CIM, honoring this inherent diversity; micro enough to gain real depth of meaning but macro enough to be transferable to wider practice and research communities.
Following the examples of Goffman (1959) and Burns (1972), who each used the concepts and terminology of theater to make “unfamiliar social worlds” accessible to others, we developed and tested Theatricality as a novel research methodology and method in CIM. We used Burns (1972) definition of Theatricality as a mode of perception, where behavior and social situations can appear theatrical to an onlooker and thus be described using the language of theater, to translate this concept into practice. We breathed new life into the definition of Theatricality within performance theory, as “the result of a perceptual dynamics linking the onlooker with someone or something that is looked at” (Féral, 2002:105), into an immersive and applied research method, and confirmed Denzin’s (2003:12) view of “performative representations” as a viable means of studying cultural experiences. This novel use, and the methods described here, offer the possibility to conceive and capture complex and diverse study data, which represents a small but significant step to improve the quality across complex health care research, including CIM. Applying the concepts of holism and theater to study distinct health care episodes has also illuminated a number of issues within our research, uniquely exposing and exploring the nature of therapy and of researching therapy—two concepts that are inextricably linked. In doing so, it revealed a larger, interconnected whole of findings and responses that speak of more than the places and performances witnessed.
Applied as an adjunct to ethnography, a research process based on fieldwork but includes engagement in the lives of those being studied (Davies, 2008:5), Theatricality methodology brings a new potential for capturing, analyzing and communicating situations, societies and environments in an embodied way, that adds to the range of explanatory models available. In observing behavior in context, it provides an intimate potential to question the meanings of that behavior and the values assigned to customs, artifacts, knowledge and experiences subject to both geographical and cultural influences (Moerman, 2002). Theatricality as methodology, with the associated methods developed and described, enabled our researcher to step inside a variety of clinics, inside the experiences of the practitioners and patients there, and into their own research performance, to examine the ways each connects to the whole.
Our attempt to bring contextual variables of a setting into the foreground, allowing the interventions to take a background position, and create a “space” for the human dimension to occupy “centre stage” ultimately evolved into a “production” where the performance of research became equally valuable to the overall appraisal and critique as the topic being explored. A complex process to enact, engagement with each setting was subject to the influence and impact of the different contexts, as much as the performances of therapy witnessed. This observation shares similarity to Steven Spielberg’s revelation that Dartmoor was a “third character” in his acclaimed movie War Horse (Groscop, 2012). Here, the result saw the researcher appraising how they experienced the different spaces and engaged with and within these, supplementing each subjective story. It also holds important lessons and encouragement for others wishing to devise, test, and apply methods appropriate to the needs they perceive, and the value of creating appropriate “space” for this.
Conclusion
The novel research method and methodology proposed in this article, and the study that provided the opportunity to develop and trial this, did not set out to determine the effect or effectiveness of different contextual variables on patient outcomes. It only aimed to develop a critical-subjective frame that would enable health care researchers to engage holistically with these alternate worlds or demonstrate how to see into these complex health care performances—from the whole staging, to composition and “acts” experienced within.
Findings from the original study (Croke, 2015) showed that CIM practices and practitioners appeared equally bound by their context and space, which created or limited the potential for relationships between therapists and their therapies/patients. It also evidenced that CIM research (and researchers) can be similarly bound, creating a potential for new relationships, as described here. This is part of the “messy business” that Freshwater and Rolfe (2001) allude to in their appraisal of qualitative research. Engaging with this milieu of “confusion” was as integral to the research outcomes as the stories of participants. This is something that all complex intervention researchers can learn from, and we encourage creating appropriate “space” to explore this.
Footnotes
Acknowledgements
I acknowledge the intermediaries, clinics, practitioners, and patients who welcomed me into their spaces to conduct the research where this novel methodology and method was first applied.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author conducted this work as part of their PhD, which was supported by a University of Leeds scholarship. There was no financial support for the authorship and/or publication of this article.