
Abstract
The quality of teamwork in Child Advocacy Center (CAC) multidisciplinary teams is likely to affect the extent to which the CAC model improves outcomes for children and families. This study examines associations between team functioning and performance in a statewide sample of CAC teams. Multidisciplinary team members (N = 433) from 21 CACs completed measures of affective, behavioral, and cognitive team functioning. Team performance was assessed with three measures: team member ratings of overall performance, ratings of mental health screening/referral frequency, and caregiver satisfaction surveys. Linear mixed models and regression analyses tested associations between team functioning and performance. Affective team functioning (i.e., liking, trust, and respect; psychological safety) and cognitive team functioning (i.e., clear direction) were significantly associated with team members’ ratings of overall performance. Behavioral team functioning (i.e., coordination) and cognitive team functioning were significantly associated with mental health screening/referral frequency. Team functioning was not associated with caregiver satisfaction with CAC services. Aspects of team functioning were associated with team members’ perceptions of overall performance and mental health screening/referral frequency, but not caregiver satisfaction. Understanding associations between team functioning and performance in multidisciplinary teams can inform efforts to improve service quality in CACs and other team-based service settings.
Child Advocacy Centers (CACs) are designed to provide coordinated interagency responses to allegations of sexual abuse and other maltreatment (Elmquist et al., 2015; Herbert & Bromfield, 2016, 2019). The CAC model has been shown to improve criminal justice outcomes, use of medical and mental health services, and caregiver satisfaction (Herbert et al., 2020; Herbert & Bromfield, 2016, 2017; Nwogu et al., 2015). CAC accreditation standards require a team-based approach, with the team containing individuals from diverse disciplines including law enforcement, child welfare, prosecution, medicine, mental health, and victim advocacy (National Children’s Alliance, 2017, 2021). The use of a multidisciplinary team (MDT) is intended to improve knowledge and information sharing across agencies and increase collaboration and coordinated case planning, with the goals of reducing distress and increasing support for children and families (Herbert et al., 2020; Herbert & Bromfield, 2019).
In the CAC model, MDT members participate in forensic interviews, case review meetings, and collaborative efforts to assess family needs and provide ongoing support (Herbert & Bromfield, 2019). Team members continue to complete their discipline-specific tasks (e.g., child welfare investigations, medical exams). MDT activities are theorized to impact outcomes by increasing knowledge and information sharing, coordination and collaboration, child-friendly and trauma-informed practices, and support for families (see Herbert & Bromfield, 2019 for a theory of change and logic model). The extent to which MDT activities activate these theorized mechanisms and impact outcomes is likely to be affected by the functioning of the MDT. Effective teamwork requires team members to agree on goals, understand members’ roles and responsibilities, cooperate with one another, and coordinate their actions. The importance of teamwork in this setting is reflected in a new requirement for accredited CACs to have a dedicated MDT coordinator/facilitator who supports information sharing, case coordination, and team functioning (National Children’s Alliance, 2021).
Team functioning can be defined as how teams and their members think, feel, and act, and includes processes (e.g., coordination) and emergent states (e.g., trust) that may be affective, behavioral, or cognitive (Kozlowski & Bell, 2003; Kozlowski & Ilgen, 2006; Mitropoulos & Memarian, 2012). Affective aspects of team functioning capture how group members feel about one another and the team, and include trust, respect, cohesion (i.e., closeness within the team), and collective efficacy (i.e., shared belief in the team’s ability to make a positive impact). Behavioral processes include intra-team communication, coordination, learning behavior, conflict resolution, and decision-making. Cognitive aspects capture team members’ individual and collective knowledge, including shared mental models (i.e., common knowledge and understanding) and diversity in members’ expertise (Kozlowski & Bell, 2013; Mathieu et al., 2017; Mitropoulos & Memarian, 2012; Salas et al., 2008; Shuffler et al., 2011).
Teams are dynamic and adapt over time as members interact and context changes (Bisbey & Salas, 2019; Marks et al., 2001; Mathieu et al., 2017). Affective and cognitive states emerge from behaviors and interactions between team members and have reciprocal effects on these behaviors. For example, respect, an affective state, emerges from interactions between team members (e.g., professional communication) and in turn influences how team members interact with one another (e.g., increases information sharing). The importance of affective, behavioral, and cognitive team functioning has been demonstrated in diverse work teams (Kozlowski & Bell, 2003; Mathieu et al., 2017, 2019; Mitropoulos & Memarian, 2012; Salas et al., 2017).
Little research has specifically examined team functioning in CACs. However, the broader literature on multidisciplinary approaches to child maltreatment suggests that team functioning is likely to impact performance and outcomes for children and families served by CACs (Herbert & Bromfield, 2017; Jackson, 2012). A recent scoping review of facilitators and barriers to cross-agency collaboration in child abuse cases identified enabling factors (e.g., leadership, resources), processes (e.g., protocols, joint training), and individual factors (e.g., skills and knowledge, roles and priorities) associated with the quality of cross-agency collaboration and case outcomes (Herbert et al., 2020). Many of the factors identified in this research relate to dimensions of team functioning. For instance, differences in mandates, vision, roles, and priorities between team members challenge the development of shared knowledge and direction (i.e., cognitive team functioning). Trust and respect (i.e., affective team functioning) and communication (i.e., behavioral team functioning) were identified as indicators of the quality of collaboration and posited to be critical to the effectiveness of the multidisciplinary team approach (Herbert et al., 2020).
Although collaboration quality is assumed to affect outcomes, there is limited quantitative research testing associations between the functioning of CAC multidisciplinary teams and their performance. In other work settings, team functioning is positively associated with team performance (Bisbey & Salas, 2019; Cronin & Weingart, 2007; DeChurch & Mesmer-Magnus, 2010; Edmondson & Harvey, 2018; Kozlowski & Bell, 2013; Kozlowski & Ilgen, 2006; Mitropoulos & Memarian, 2012; Weingart et al., 2010). For example, in healthcare settings, better team functioning is associated with greater patient safety and better clinical outcomes (Dinh et al., 2020; Schmutz & Manser, 2013), and interventions that improve team functioning have been shown to improve patient safety and outcomes (Hughes et al., 2016; McCulloch et al., 2011; Miller et al., 2018; Weaver et al., 2014).
Team performance is multidimensional (e.g., efficiency, quality, productivity), context-specific, and can be measured subjectively (i.e., team members’ perceptions) as well as objectively (Mathieu et al., 2008, 2017). Because teams perform multiple functions, it is often appropriate to measure performance with multiple measures. In the context of CACs, subjective indicators include team members’ perceptions of collaboration and team performance, while objective indicators include client satisfaction, investigation and criminal justice outcomes, and service outcomes (Herbert & Bromfield, 2019).
Differences in the functioning of MDTs are likely to impact team performance and ultimately the extent to which the desired outcomes of the CAC model are realized. Figure 1 illustrates a conceptual model of team performance for CAC multidisciplinary teams based on the classic Input-Process-Output model of teams (Ilgen et al., 2004; Mathieu et al., 2008). Although variations in team characteristics may impact team functioning, team structure (i.e., who is on the team) and task demands (i.e., what teams are expected to do) are relatively constant across CACs in the United States because of national accreditation standards (National Children’s Alliance, 2017, 2021). Therefore, in this study, we focus on the influence of team functioning on performance (Courtright et al., 2015; Kozlowski & Ilgen, 2006; Kozlowski & Bell, 2013). Examining how different aspects of team functioning relate to team performance in CACs is needed to advance our understanding of multidisciplinary teams, inform efforts to improve team functioning, and ultimately, improve the quality of care in CACs and other services that rely on teams (e.g., integrated primary care, child welfare) (Fiscella & McDaniel, 2018; Lipton, 2009; Lewandowski & GlenMaye, 2002). Conceptual model of Child Advocacy Center multidisciplinary team performance. (Adapted from Mathieu et al., 2008; Mitropoulos & Memarian, 2012).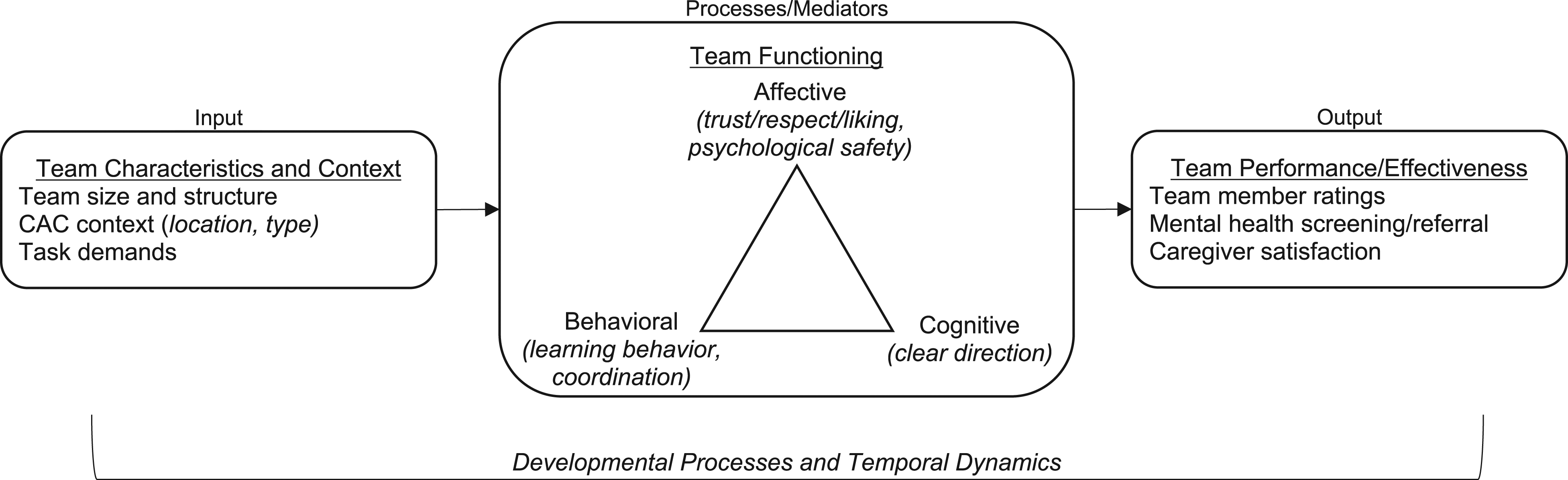
Current Study
The current study examines cross-sectional associations between multidisciplinary team functioning and team performance in a statewide sample of Child Advocacy Centers. Multidisciplinary team members completed multiple measures of affective, behavioral, and cognitive team functioning. We tested associations of team functioning with three dimensions of team performance: team members’ perceptions of performance, frequency of mental health screening/referral efforts, and caregiver satisfaction. We hypothesized that more adaptive affective, behavioral, and cognitive team functioning would be associated with better team performance.
Methods
Survey Participants and Procedures
We conducted an anonymous survey of CAC multidisciplinary team members in a single state. The 24 CACs in this state serve >6300 children annually; sexual abuse is the most frequent allegation (60% of cases) and physical abuse the second most frequent (30% of cases) (Utah Children’s Justice Center Program, 2022). The survey was constructed in REDCap, and survey invitations were emailed to all CAC directors with a request that they forward the invitation to their team members. One director, responsible for the three smallest CACs, did not respond to repeated invitations, resulting in the exclusion of these 3 CACs from data collection. These 3 CACs combined serve less than 1% of cases in the state. Participants who were part of the MDT at more than one CAC (e.g., a satellite CAC and its associated CAC) were asked to complete the survey separately for each CAC. Participants received a $5 Amazon.com gift card for completing the survey, and CACs with >75% participation received $150 in recognition of their time. All participating CACs received a final report summarizing the results for their CAC. The study was approved by the University of Utah Institutional Review Board.
Measures
Background information and child advocacy center characteristics
Participants reported their discipline, CAC, and years of experience in their current CAC and with any CAC. Participants also reported their gender, race, ethnicity, and age. CAC directors reported the number of team members. We estimated survey participation rates by dividing the number of surveys by the number of reported team members. CACs were classified as urban or rural/frontier based on their county’s population density (Utah Department of Health, Office of Primary Care & Rural Health, 2018) and as independent locations or satellite locations.
Affective team functioning
Two dimensions of affective team functioning were assessed: affective integration (i.e., extent to which team members like, trust, and respect one another) and psychological safety (i.e., perceptions that team members will not be punished for interpersonal risk taking). Affective integration was assessed with 11 items from Cronin and colleagues (2011). Participants rated their agreement with each item on a 5-point Likert scale (1 ‘Strongly Disagree’ to 5 ‘Strongly Agree’). Internal consistency was excellent (Cronbach’s α = 0.91). Psychological safety was assessed with seven items from Edmondson (1999). Participants rated the accuracy of each statement for their team on a 7-point Likert scale (1 ‘Very Inaccurate’ to 7 ‘Very Accurate’). Internal consistency was good (α = 0.84).
Behavioral team functioning
Two aspects of behavioral team functioning were assessed: learning behavior and coordination. Team learning behavior (i.e., how much the team tries to keep learning and improving) was assessed with seven items from Edmondson (1999). Participants rated the accuracy of each statement for their team on a 7-point Likert scale (1 ‘Very Inaccurate’ to 7 ‘Very Accurate’). Internal consistency was good (α = 0.75). Team members’ coordination about mental health was assessed with the Relational Coordination Survey (Gittell et al., 2019). Participants rated seven items assessing the quality of team coordination to meet families’ mental health needs (e.g., communication frequency, timeliness) on a 5-point Likert scale. Internal consistency was excellent (α = 0.90).
Cognitive team functioning
Clear direction (i.e., extent to which team members have a shared understanding of the team’s purpose and goals) was assessed with three items from Edmondson (1999), each rated on a 7-point Likert scale (1 ‘Very Inaccurate’ to 7 ‘Very Accurate’). Internal consistency was excellent (α = 0.90).
Team performance
Team member-rated performance
Participants rated the overall quality of work done by the team using five items from Edmondson (1999). Participants rated the accuracy of each statement for their team on a 7-point Likert scale (1 ‘Very Inaccurate’ to 7 ‘Very Accurate’). Internal consistency was good (α = 0.77).
Mental health screening/referral
Team members reported how often their team connected families with community resources, provided referral assistance to connect families with specialty mental health services, and used a standard protocol to identify children for mental health referrals. Items were rated on a 5-point Likert scale (0 ‘None (0%)’ to 4 ‘All the time (100%)’). Items were highly correlated with one another and combined into one scale reflecting the frequency of mental health screening/referral (α = 0.81).
Caregiver satisfaction
CACs collect anonymous satisfaction surveys from caregivers at the end of the family’s CAC visit as part of routine operating procedures. Caregivers rate 10 items (e.g., “The staff members at the Center were friendly and pleasant; My questions were answered to my satisfaction”) on a 4-point scale from 1 ‘Strongly Disagree’ to 4 ‘Strongly Agree.’ To obtain enough caregiver surveys for each CAC, we used caregiver surveys completed during the 2-year period prior to the team survey. The average rating across all surveys was used as a CAC-level performance measure.
Statistical Analyses
First, we examined associations between CAC characteristics, survey participation rates, and outcomes of interest to determine which variables should be included as covariates in our multivariable models. We conducted independent samples t-tests to test for differences by location (rural/frontier vs. urban) and CAC type (independent vs. satellite) and estimated correlations to assess the association between participation and team size. Multivariable linear mixed models tested the contribution of team size, location, and participation rate to each measure of team functioning, team member-rated performance, and mental health screening/referral frequency. Because caregiver satisfaction was measured at the CAC-level (i.e., one score for each CAC), associations between caregiver satisfaction and team size, location, and participation rate were tested using regression analyses.
Next, we tested associations of team functioning with performance. Each performance outcome (i.e., team member ratings, mental health screening/referral frequency, caregiver satisfaction) was examined individually. The first set of analyses for an outcome tested each dimension of team functioning separately (Model 1: affective; Model 2: behavioral; Model 3: cognitive). The second set of analyses included all measures of team functioning. Linear mixed models were used for analyses of team member-rated performance and mental health screening/referral, both of which were rated at the individual-level. All mixed models included a random effect to account for clustering within CACs. Caregiver satisfaction was rated at the CAC-level; for these analyses, team members’ ratings were aggregated to the CAC level and hypotheses were tested using regression analyses. For all analyses, we assumed a Type 1 error rate of α = 0.05 and made no adjustments for multiplicity.
Before aggregating team members’ ratings, we assessed within-team agreement on each survey measure using the Average Deviation index (AD) (Burke et al., 1999; Burke & Dunlap, 2002; González-Romá et al., 2009). The ADMd index quantifies the average deviation from the median and is preferable to r wg because it provides an estimate of within-team agreement in the metric of the original response scale and does not require assumptions about the distribution of expected null responses (Burke et al., 1999). 1 An ADMd value of 0 indicates perfect agreement, and higher values indicate greater disagreement. ADMd values less than c/6, where c is the number of response categories, indicate acceptable interrater agreement (Burke & Dunlap, 2002). For each measure in this study, the median ADMd value across teams was below the upper limit, indicating acceptable levels of agreement. We created aggregate scores reflecting the median of team member scores for each CAC; we used median scores rather than means to reduce the potential influence of outliers within each team. Aggregated team scores were used in regression analyses examining associations with caregiver satisfaction.
Results
Survey Participation
Team members from 21 of 24 CACs participated in the survey. Participating CACs included six urban, 10 rural, and five frontier CACs; four were satellite CACs associated with another CAC. Teams ranged in size from 9-110 members (M = 29; SD = 22; interquartile range [IQR] = 16–37), and participation rates ranged from 33-100% (M = 78%; IQR = 54–97%). A total of 433 team members participated in the survey, 382 (88%) of whom completed the entire survey. Using directors’ reports of team size as the denominator, 72% of team members in the 21 CACs participated. Seventeen CACs had more than 50% participation, and 14 had more than 75% participation. There were no significant differences in participation between rural/frontier and urban CACs or between independent and satellite CACs. The correlation between team size and participation rate was significant (r = −.57, p < .05); larger teams had lower participation. 2
Participant Background
Participants reported a variety of backgrounds, most commonly law enforcement (33%) and child protective services (19%). See Figure 2 for a complete breakdown by discipline. Overall, participants were fairly experienced with the CAC model; 15% had less than 1 year of experience, 34% had 1–3 years of experience, 20% had 4–6 years of experience, and 32% had seven or more years of experience. Most participants (83%) had been at their current CAC for more than 1 year. Participants who provided demographic data (>75%) were primarily non-Hispanic white (90%); 7% identified as Hispanic or Latino/a/x and 2% as belonging to other racial or ethnic groups. Participants identified as female (56%), male (43%), and nonbinary or not specified (1%). Most participants (84%) were between 26 and 55 years old; the most common age group (36%) was 36–45 years of age. Participant disciplines.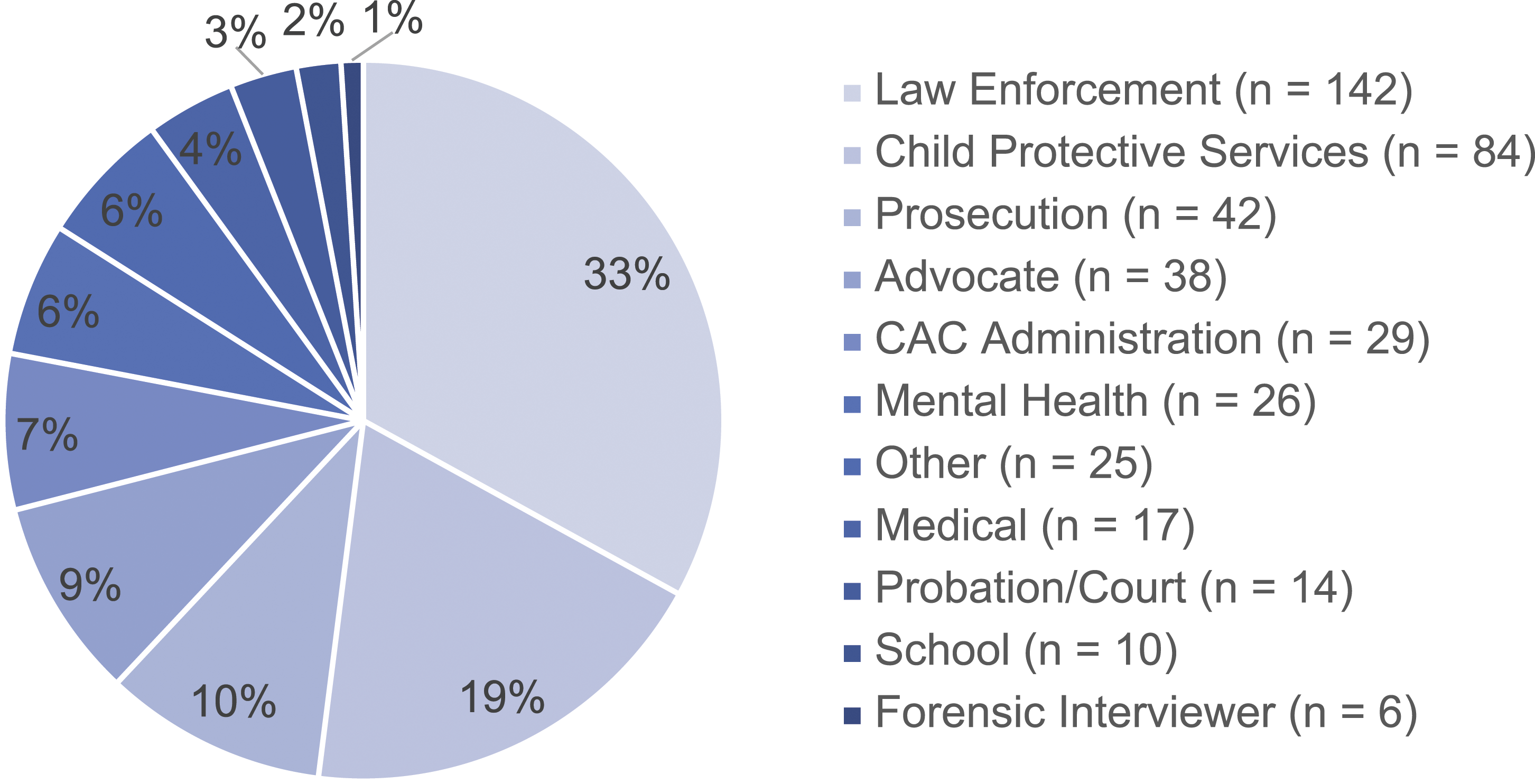
Descriptive Data
Descriptive Statistics and Correlations among Individual-Level Team Measures (N = 376–416).
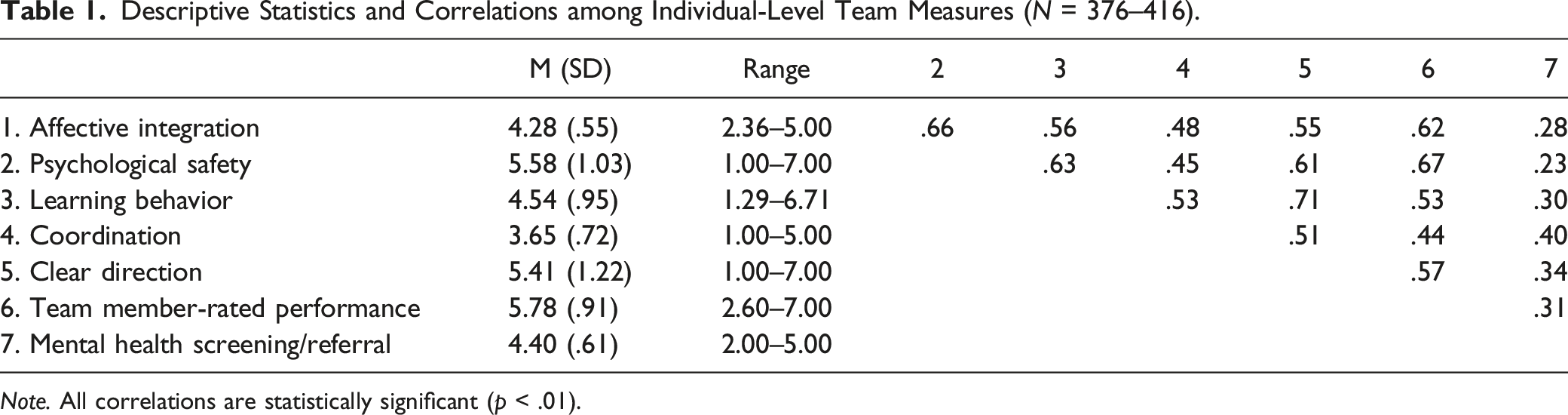
Note. All correlations are statistically significant (p < .01).
Descriptive Statistics and Correlations among Aggregated Team Measures (N = 21).
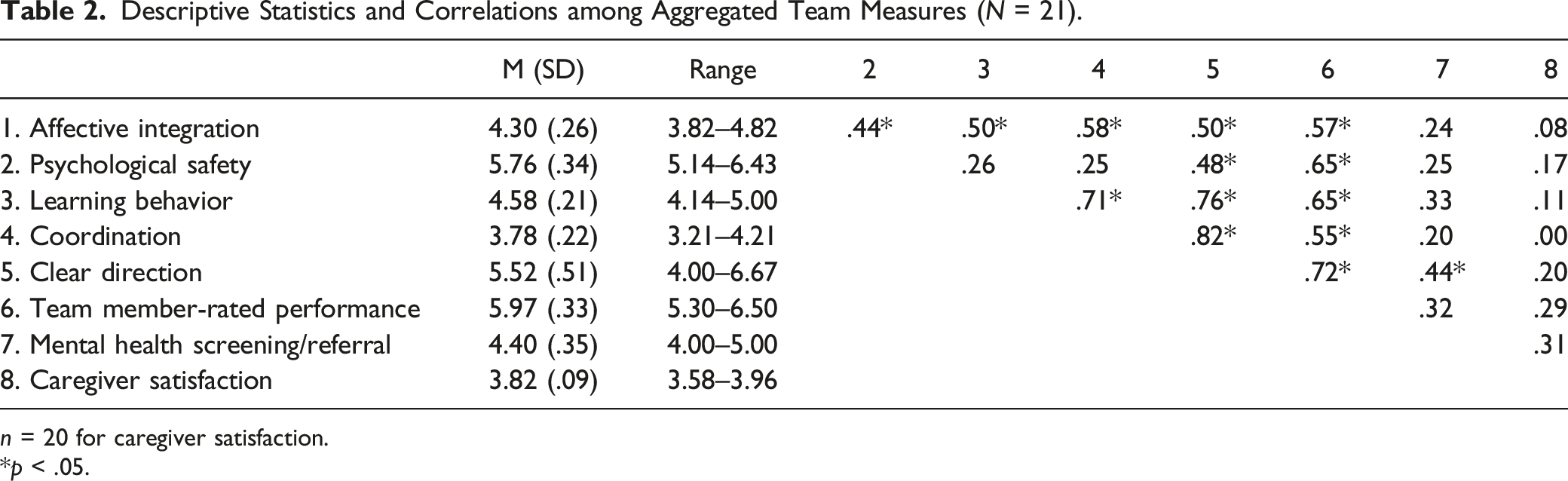
n = 20 for caregiver satisfaction.
*p < .05.
Associations Between Child Advocacy Center Characteristics and Team Measures
CAC characteristics (i.e., rural/frontier vs. urban location, team size) and participation rates were not associated with any measure of team functioning, nor were they associated with team member-rated performance, mental health screening/referral frequency, or caregiver satisfaction. Given the lack of associations between CAC characteristics and team outcomes, no CAC characteristics are included as covariates in later models.
Associations between Team Functioning and Team Performance
Associations of Team Functioning with Team Member-rated Performance and Mental Health Screening/Referral Frequency.
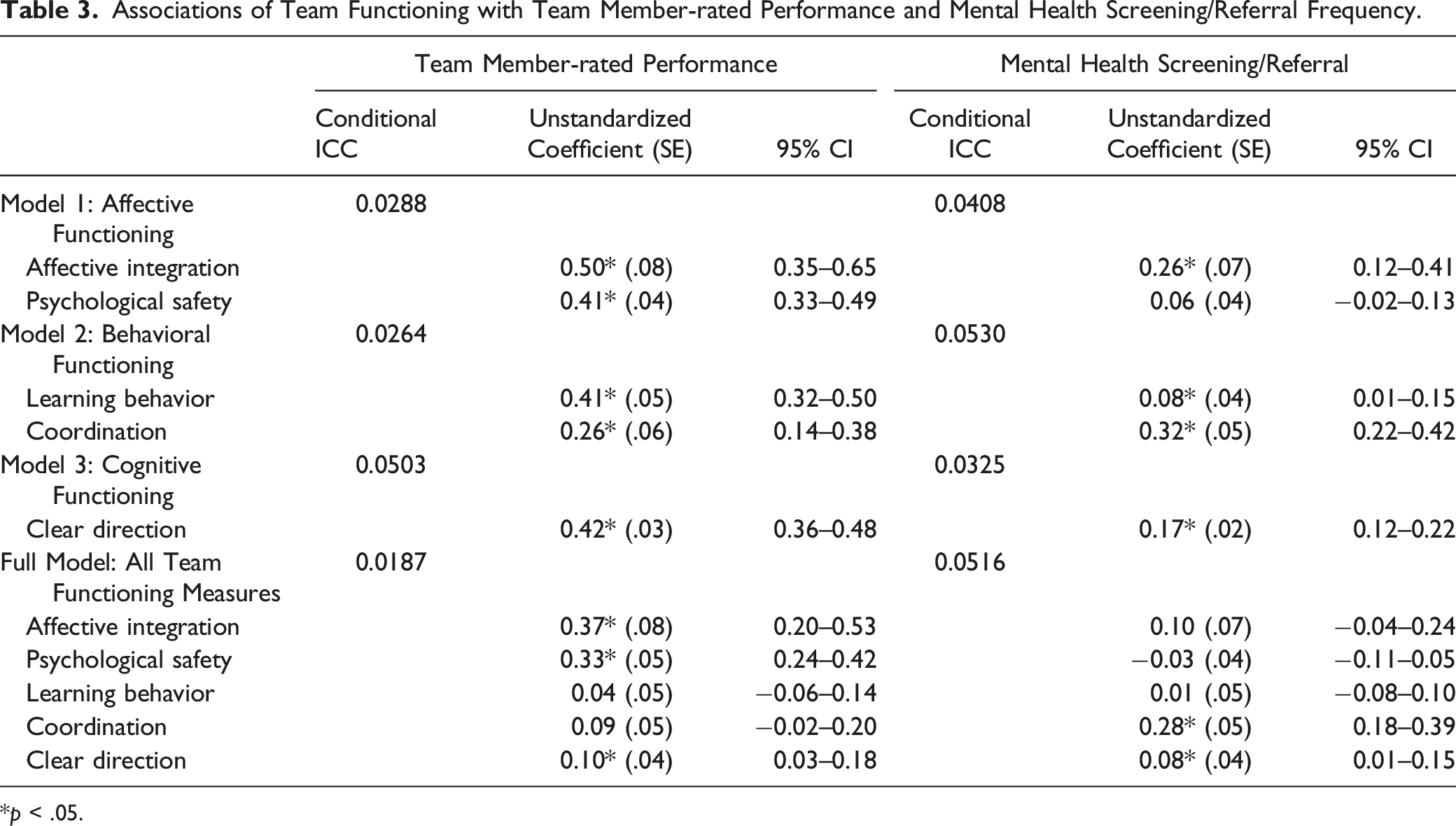
*p < .05.
Our final set of models included all measures of team functioning (i.e., affective integration, psychological safety, learning behavior, coordination, and direction). Results for the full models are presented in Table 3. When considering all dimensions of team functioning together, affective integration, psychological safety, and clear direction remained significantly associated with team member-rated performance; behavioral team functioning (i.e., learning behavior and coordination) was no longer significantly associated with performance. Coordination and clear direction remained significantly associated with mental health screening/referral frequency; affective integration and learning behavior were no longer significant when considering all aspects of team functioning. Team functioning was not significantly associated with caregiver satisfaction (results not shown; available on request).
Discussion
This study examined associations between team functioning and multiple measures of team performance in a statewide sample of 21 Child Advocacy Center multidisciplinary teams. We assessed affective, behavioral, and cognitive dimensions of team functioning and tested associations with team members’ perceptions of performance, the frequency of mental health screening/referral provided by the CAC, and caregiver satisfaction with CAC services. The high response rate in this study is a strength and increases the generalizability of our findings.
Affective integration (i.e., liking, trust, and respect) and psychological safety were significantly associated with team members’ perceptions of overall team performance. These results suggest that high-quality relationships among team members are associated with better performance. Affective integration was also associated with mental health screening/referral frequency in models including only affective functioning, but this association did not remain significant when considering other aspects of team functioning. Good affective functioning may be necessary but insufficient for improving objective performance outcomes. Some research suggests that building cohesiveness is an early stage of team development that provides a foundation for communication and clarification of roles and goals (Stock et al., 2013). It is possible that liking, trust, and respect among team members may indirectly affect service quality by facilitating more frequent and timely communication and improving coordination (Grossman et al., 2017). Affective functioning may also interact with other team characteristics to affect outcomes. For example, affective functioning may be more strongly associated with objective outcomes when team members work together more closely (Beal et al., 2003).
Both measures of behavioral team functioning (i.e., learning behavior, coordination about mental health care) were associated with overall performance and mental health screening/referral frequency when only behavioral team functioning was considered. When affective and cognitive functioning were included in models, only the association between coordination about mental health care and mental health screening/referral frequency remained significant. Consistent with hypotheses, greater coordination about mental health needs was associated with more frequent efforts to identify children with mental health needs and connect families with services. We conceptualized coordination as leading to more frequent screening/referral, but it is also possible that use of mental health screening/referral protocols leads to greater team coordination. Longitudinal research is needed to test the directionality of this association.
Cognitive team functioning, specifically the extent to which team members have a shared understanding of the team’s purpose and goals, was significantly associated with both perceived performance and mental health screening/referral frequency even when considering other dimensions of team functioning. These results are consistent with prior, primarily qualitative, research findings that unclear or competing mandates, visions, roles, and priorities contribute to increased conflict, less trust, and reduced information sharing in multidisciplinary teams (Herbert et al., 2020; Svedin et al., 2020). Clear shared team goals appear to be a critical contributor to multiple dimensions of MDT performance in CACs.
We did not find any significant associations between team functioning and caregiver satisfaction with CAC services. Satisfaction ratings were high overall. In addition, caregiver satisfaction ratings were obtained immediately following the family’s visit to the CAC and may be more strongly associated with factors specific to the visit (e.g., location of center, wait time, interactions with staff) than the work done by team members. Team functioning may have a greater impact on caregiver satisfaction for families engaged in extended investigations and ongoing services who have more interactions with team members.
Overall, we found that aspects of affective, behavioral, and cognitive team functioning in MDTs were associated with perceptions of overall performance and the frequency of mental health services provided by CACs. In our full models, affective functioning was most strongly associated with team members’ perceptions of effectiveness, while behavioral functioning was more strongly associated with the frequency of mental health screening/referral. Cognitive team functioning was associated with both measures of performance even after accounting for the contributions of affective and behavioral functioning. These associations were found despite limited range in measures of team functioning, suggesting that efforts to improve teamwork may improve performance even among teams that are already functioning well. The consistent pattern of findings for cognitive team functioning, specifically clear direction, suggests that shared team goals may be a particularly critical target for interventions that aim to improve team performance in CACs.
Limitations
Key limitations of this study include its cross-sectional nature and shared method variance. Longitudinal data is needed to determine the directionality of associations and make causal inferences. Because most measures were rated by team members, common method variance and self-report biases could have artificially inflated or deflated the observed associations (Podsakoff et al., 2003). Biases may have been reduced by the anonymous nature of the survey and use of validated measures with varying response scales. Another limitation is the limited variability in caregiver satisfaction ratings across CACs (range 3.58–3.96 on 1–4 scale). We used ratings across a 2-year period to increase the number of surveys per CAC, which may have contributed to decreased variation. In addition, because caregiver satisfaction was measured at the CAC-level, our sample of 21 CACs was likely underpowered to detect associations. Regional or national samples of CACs may be needed to test associations between teamwork and CAC-level outcomes. Finally, dimensions of team functioning were correlated with one another, making it challenging to distinguish their unique contributions to team performance.
Future Directions
Teams are complex, adaptive, dynamic systems, and processes and performance are likely to influence one another over time (Hackman, 2012; McGrath et al., 2000). Longitudinal research exploring potential mediators and moderators of team performance is needed. In addition, team performance is multidimensional, context-specific, and often subjective (Rosen & Dietz, 2017). Future research should utilize multiple methods to assess team functioning (e.g., team member ratings, supervisor or expert ratings, administrative data, qualitative data) and examine how team functioning is associated with more objective measures of team performance, such as observer ratings of team interactions or investigation and service outcomes, as well as the ultimate outcome of child and family well-being.
Because teams perform multiple context-specific functions, performance should be assessed with multiple measures. It may be helpful to consider MDT performance alongside indicators of CAC quality, such as adherence to accreditation standards, to better understand how team performance and the effectiveness of the CAC model are related. MDT performance and other components of the CAC model are theorized to impact investigation and service outcomes that should be examined in future research. Potentially relevant outcomes include quality of forensic interviews and disclosures, referrals for medical exams, prosecutions and convictions, efficiency of case resolution, children’s comfort and satisfaction with their experience, and family engagement in recommended services (Herbert & Bromfield, 2019). However, CACs vary in the extent to which they collect measures of quality and their methods of doing so. In addition, it should be noted that investigation and service outcomes are quite diverse and may be only weakly associated with one another. Some of these outcomes may be more strongly related to other standards of the CAC model than to teamwork. For example, the quality of forensic interviews may be more strongly associated with the training and experience of the interviewer and their adherence to protocols than with team functioning. Specifying the critical tasks and functions of MDTs in the context of CACs may help establish objective performance metrics that can be compared across teams.
Future research should evaluate associations between team functioning and caregiver satisfaction over time. Team functioning may impact caregivers’ experiences more strongly for children and families who have ongoing interactions with team members following their visit to the CAC. In addition, ensuring that children and families receive needed care and supports to ameliorate the long-term sequalae of maltreatment is likely to require coordination with external service providers and other professionals who are not part of the multidisciplinary team. Future research should examine how coordination and teamwork within this larger network affect child and family outcomes.
Another potentially fruitful area for research is the influence of team functioning and performance on outcomes for individual team members in the demanding and high-stress professions associated with CACs (e.g., child welfare, law enforcement, victim advocacy). One dimension of team performance is the extent to which the team contributes to members’ learning and development (Hackman, 2012). Well-functioning teams may provide a buffer against negative outcomes such as vicarious trauma, burnout, and turnover and improve team members’ competence and job satisfaction. Effective multidisciplinary teams are critical to realizing the promised benefits of the CAC model and improving outcomes for children and families served by CACs.
Footnotes
Author’s Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Acknowledgments
Thank you to every team member who took the time to complete the survey. We would also like to thank the directors of participating Children’s Justice Centers for their assistance distributing the survey and the University of Utah Pediatric Integrated Post-Trauma Services team and Utah Office of the Attorney General for their support of this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the SAMHSA [1U79SM080000-01] and the National Institutes of Health [TL1TR001858; MH018951; MH123729]. The REDCap platform at the University of Utah is supported by Center for Clinical and Translational Sciences grant support (8UL1TR000105 (formerly UL1RR025764) NCATS/NIH).