
Abstract
The present study examined the effectiveness of Family Group Conferencing (FGC) in child welfare. Effects were operationalized in terms of child safety (child maltreatment, supervision order, and out-of-home placement), number of professional services used, parental empowerment, and social support in a 1-, 3-, 6-, and 12-month follow-up. Furthermore, the influence of family characteristics and the level of FGC completion were examined. A total of 328 families were included, randomly assigned to an experimental group (n = 229) and a care as usual (CAU) group (n = 99). FGC was equally effective as CAU in improving child safety but resulted in more out-of-home placements. Furthermore, FGC resulted in a longer duration of child welfare involvement, a marginally higher number of professional services used, and increased parental empowerment and social support. Family characteristics did not moderate the results. Level of FGC completion was in general low. Higher levels of completion were related to a larger social network, a higher number of professional services used, and, marginally, less parental empowerment. In conclusion, although some beneficial results marginally support the use of FGC, it is the question whether these effects outweigh FGC costs, a longer duration of child welfare involvement and a higher number of professional services used.
Keywords
Family Group Conferencing (FGC) is currently a popular decision-making model in child welfare. Whereas in regular care, the child welfare worker is responsible for designing a care plan to reduce the risk of child maltreatment, the idea of FGC is that the family, together with its extended network, makes its own care plan that enhances and supports active responsibility (Merkel-Holguin, 1996). The basic premise of FGC is that families have the right to be involved in important decisions about their children and have the right to make these decisions themselves. Furthermore, it has been argued that a care plan, developed and supported by the family and its social network, is more likely to be carried out and successful than a plan developed by professionals (Burford & Hudson, 2000), probably because families feel that they have a voice in matters that concern them (Merkel-Holguin, 2004).
Although the implementation of the FGC model has shown a rapid growth in many countries (Nixon, Burford, Quinn, & Edelbaum, 2005), several authors have pointed out that the popularity of FGC is more based on client satisfaction than on the results of effectiveness studies that demonstrate the positive effects of FGC on child welfare outcomes (Barth, 2002; Maluccio, Ainsworth, & Thoburn, 2000). Robust prospective experimental studies examining the effectiveness of FGC are scarce. To illustrate, in a recently published meta-analysis on the effectiveness of FGC in child welfare, only 14 controlled studies, most of which using a retrospective design, could be included (Dijkstra et al., 2016a). This stresses the need for more prospective, controlled studies, allowing causal inferences on the effectiveness of FGC in child welfare.
In the present study, we, therefore, examined the effectiveness of FGC in child welfare by means of a randomized controlled trial (RCT). Given that FGC is used as an alternative approach in child welfare, we first focused on the ultimate goals of child welfare to enhance child safety and reduce the duration of child welfare involvement and professional service use. Previous research on the effectiveness of FGC in improving child safety and reducing the duration of child welfare involvement has yielded inconsistent results (i.e., Berzin, 2006; Crampton & Jackson, 2007; Pennell & Burford, 2000; Pennell, Edwards, & Burford, 2010; Sundell & Vinnerljung, 2004). Overall, a meta-analysis showed that FGC does not outperform regular care in reducing child maltreatment, out-of-home placements, and involvement of child welfare (Dijkstra et al., 2016a), which was confirmed in a more recent study by Hollinshead and colleagues (2017). In addition, previous research did not find FGC to be more effective than regular care in reducing professional service use (Sundell & Vinnerljung, 2004; Weigensberg, Barth, & Guo, 2009).
Furthermore, we focused on the effectiveness of FGC in terms of improving parental empowerment and social support. It has been argued that FGC increases parental empowerment and provides new sources of social support (Burford & Hudson, 2000; Merkel-Holguin, 2004), which contribute to improved child safety and less involvement of child welfare services (MacLeod & Nelson, 2000; Moore & McDonald, 2000). Indeed, results from the small number of studies focusing on these outcomes point toward an increase in parental empowerment (Oosterkamp-Szwajcer & de Swart, 2012; Sheets et al., 2009) and social support (Wijnen-Lunenburg, van Beek, Bijl, Gramberg, & Slot, 2008) following FGC. However, because the studies of Oosterkamp-Szwajcer and de Swart (2012) and Wijnen-Lunenburg, van Beek, Bijl, Gramberg, and Slot (2008) did not use a comparison group, results cannot be attributed to FGC.
In addition to studying the overall effectiveness of FGC, we examined which families are most likely to benefit from the FGC approach. Intervention research has demonstrated that certain family characteristics, such as socioeconomic and single parent status, affect treatment response to parent trainings (Lundahl, Risser, & Lovejoy, 2006). With regard to FGC, knowledge on moderators of effectiveness is scarce, and results of the few available studies are inconsistent. For instance, whereas Sheets et al. (2009) showed greater effectiveness of FGC for ethnic minority families in terms of family reunification, other studies found that FGC resulted in more extended supervision orders and re-referrals to child welfare in minority families when compared to ethnic majority (native) families (Dijkstra et al., 2016b; Hollinshead et al., 2017). To examine which families benefit most from the FGC approach, we studied several family characteristics that may moderate its effectiveness, including ethnicity, family situation, education level of parents, parental intellectual disability, and referral reason.
Finally, we focused on the influence of level of FGC completion, as an indicator of program fidelity. Pennell (2005, p. 110) described program fidelity as “the degree to which an intervention is carried out in a manner that is true to its key principles and its practices.” When program fidelity is not taken into account, it is unclear whether results can be attributed to an ineffective model or an ineffective implementation (Rauktis, Bishop-Fitzpatrick, Jung, & Pennell, 2013). Berzin, Thomas, and Cohen (2007), Marcynyszyn et al. (2012), and Rauktis, Bishop-Fitzpatrick, Jung, and Pennell (2013) examined program fidelity of FGC. However, none of them expressed program fidelity in a level of completion score and linked this to the results of FGC. Therefore, in this study, we not only assessed the level of FGC completion but also examined the influence of level of completion on the results of FGC.
The Present Study
The present study aimed to improve the knowledge on the effectiveness of FGC in child welfare. Since randomized experiment is preferred above alternative research designs as this allows for unbiased inferences on effectiveness (Farrington, 2003) and since LaBrenz and Fong (2016) argued that the absence of RCTs in the field of FGC makes it difficult to determine any impact that could be attributed to FGC itself, we conducted an RCT including 328 families referred to child welfare services. The aim of the current study was to examine the effectiveness of FGC in child welfare. We posed the following research questions: (1) Is FGC effective in improving child safety, reducing the involvement of professional services, and improving parental empowerment and social support? (2) Do ethnicity status, family situation, education level of parents, parental intellectual disability, and referral reason moderate the effectiveness of FGC? and (3) Is the level of FGC completion related to the effectiveness of FGC?
Method
Participants
All families that were referred to a child welfare agency in Amsterdam, the Netherlands, in the period of January 2014 until December 2014 were approached to participate in this study (see study protocol of Asscher, Dijkstra, Stams, Deković, & Creemers, 2014). The target group of this child welfare agency consists of families with multicomplex problems across various domains, such as child maltreatment, mental health problems, alcohol abuse and other drug problems, high-conflict divorce, and child behavior problems. For all families, child safety is at stake and in most families, risk factors for child maltreatment are present. The care, that is, offered to the families is compulsory, and in some families, a supervision order has been imposed.
Since in the Netherlands, FGC is believed to be suitable for all families, there were no exclusion criteria for participation in this study. A total of 527 families were approached (see Figure 1). Of these 527 families, 346 families (66% of total) gave informed consent and were randomly assigned (ratio 2:1) to the FGC group (n = 242) or the control group (care as usual [CAU], n = 104). Nonresponse analyses showed that the nonresponse group consisted of more non-Western families, χ2(1, 527) = 16.71, p = .000, and more intact families, χ2(1, 527) = 7.55, p = .02, than the response group. No differences between the nonresponse and response groups were found on mean age of the children, t (342, 27) = −0.61, p = .54. Of the 346 families, 18 families were excluded from the study because they did not belong to the target group of the child welfare agency, as determined by the child welfare worker (FGC group, n = 5; CAU group, n = 5) or because an FGC was not offered (FGC group = 8). The final sample of 328 families (FGC group, n = 229; CAU group, n = 99; Table 1) consisted of 529 children with a mean age of 10 years old (M = 10.04, standard deviation [SD] = 4.96, range = 0–19). More than half of the families had a non-Western background (53%, n = 175). A majority of the biological parents were divorced (76%) and were low educated (77%), meaning that they finished primary education or lower levels of secondary or tertiary education. Almost half of the families were referred to the child welfare agency because of parental problems (49%, i.e., psychopathology or substance abuse), as opposed to child-related problems (24%, i.e., delinquency or school problems) or family-related problems (27%, i.e., child maltreatment and neglect). Since families in the FGC group did not differ from families in the CAU group on any of the background characteristics at baseline, randomization of the sample seems to have been successful.
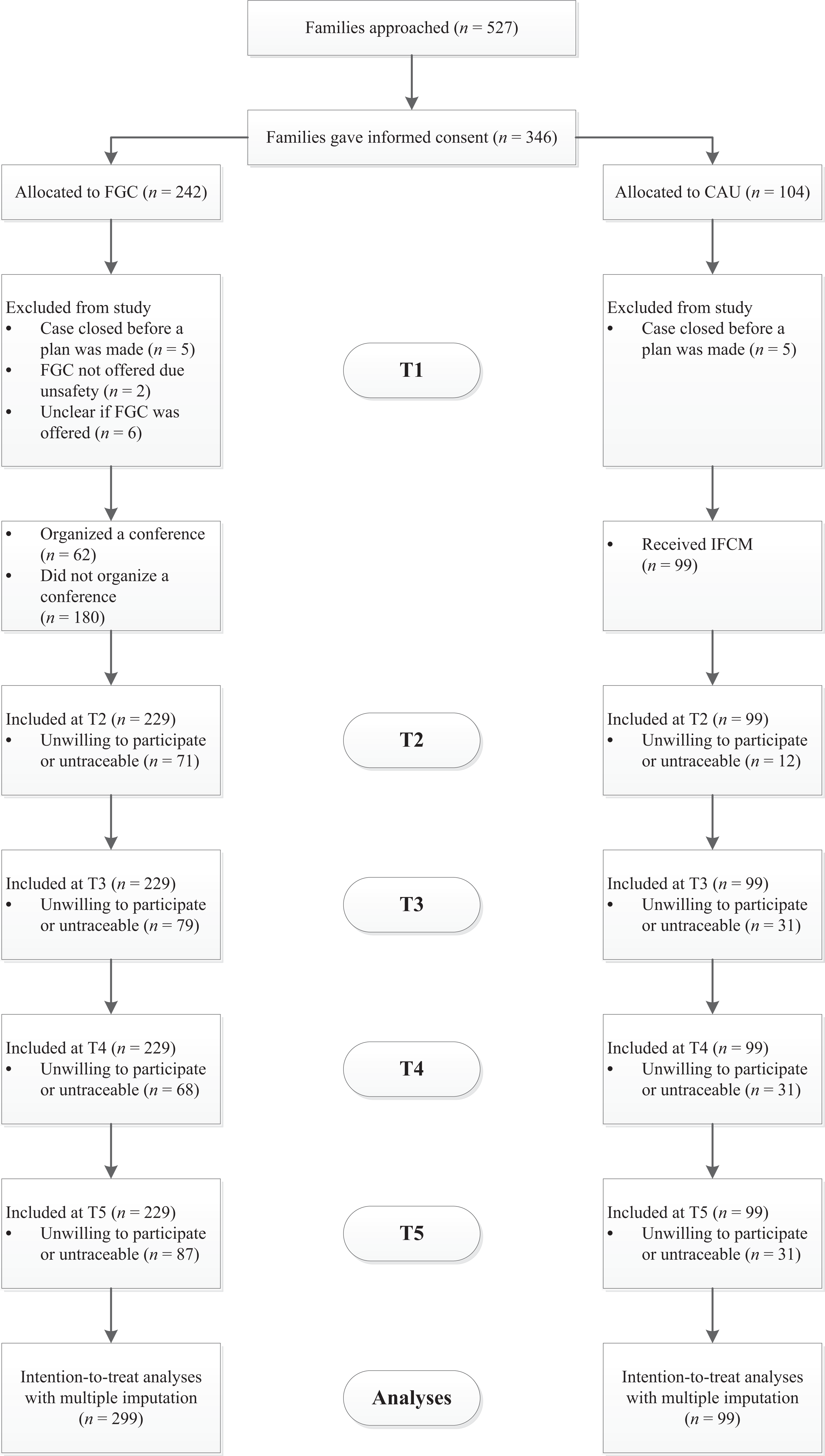
Flow diagram of the Family Group Conferencing effect study.
Background Characteristics of the FGC Group and the CAU Group at Pretest (T1).
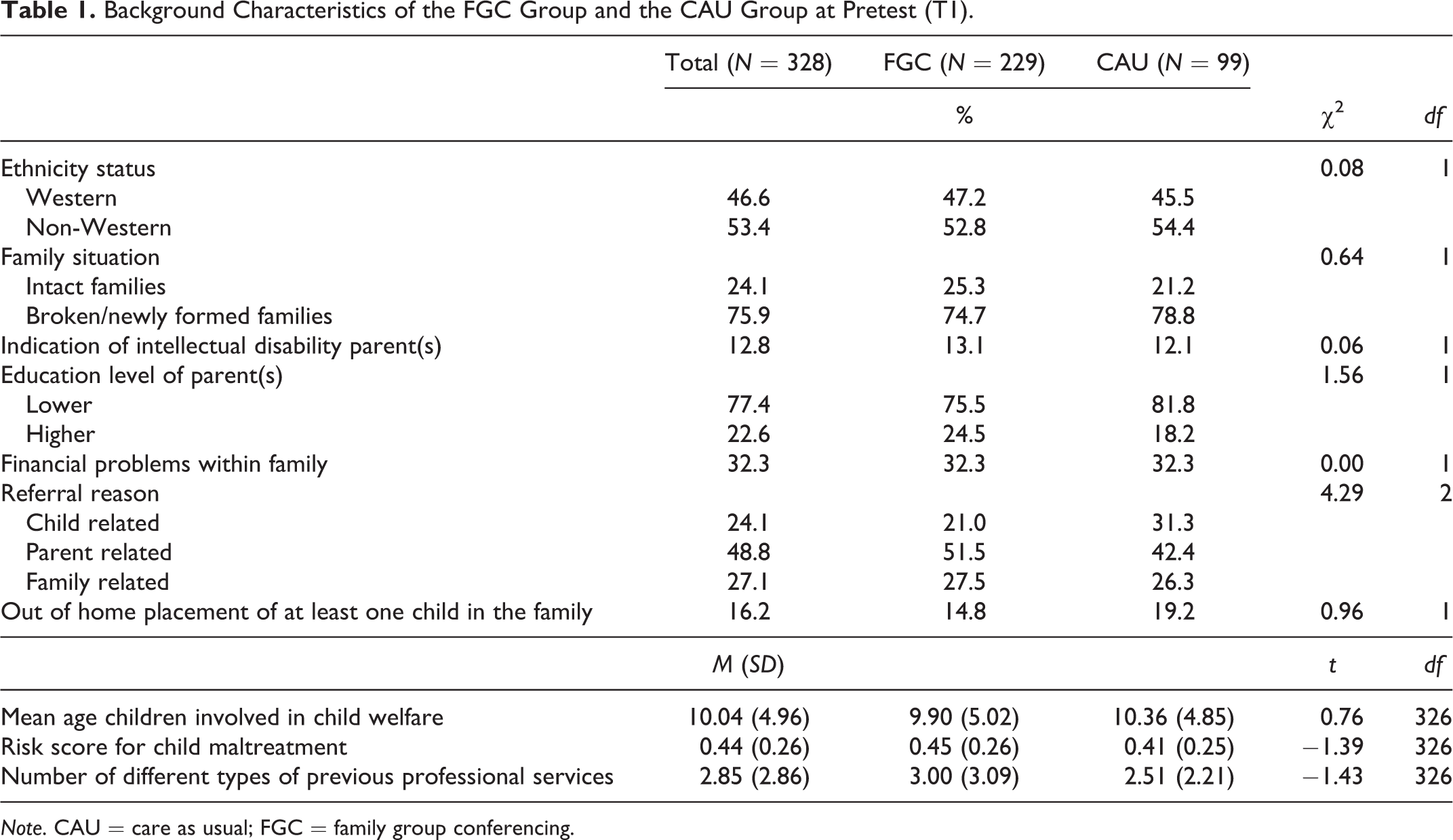
Note. CAU = care as usual; FGC = family group conferencing.
Family and child welfare worker reports were collected at five measurement occasions: as soon as possible after referral to the child welfare agency (pretest [T1]) and at assessments 1 month (T2), 3 months (T3), 6 months (T4), and 12 months (T5) after a care plan had been made. In addition to questionnaires, information about family characteristics, occurrence of out-of-home placement and supervision order, and duration of child welfare was extracted from case files by one research assistant. Although almost all families completed the baseline assessment (with the exception of n = 26 families), 25% did not respond at T2 (n = 83), 34% did not respond at T3 (n = 110), 30% did not respond at T4 (n = 99), and 36% did not respond at T5 (n = 118). For 13% of the families at T2, we had no child welfare worker data (n = 43, including n = 26 families where the child welfare worker was no longer involved due to case closure). This was also the case for 14% of the families at T3 (n = 46, including n = 43, families where the child welfare worker was no longer involved due to case closure), 20% of the families at T4 (n = 64 families where child welfare worker was no longer involved due to case closure), and 38% of the families at T5 (n = 123 families where child welfare worker was no longer involved due to case closure).
Families with missing data did not differ from the families with complete data in terms of background characteristics. With regard to outcome measures, we found that families with indications of child maltreatment at T1 were more likely to have missing data than families without indications of child maltreatment. Other outcome variables were not related to missingness. When there are indications that data are not missing completely at random, analyses based on complete cases may be biased (Sterne et al., 2009). Therefore, we replaced missing values with multiple imputation (Graham, 2009). Multiple imputation was performed in LISREL 8.80. When a case was closed during the data collection, missing child welfare workers data were not imputed.
Conditions
All families received Intensive Family Case Management (IFCM; Busschers, Boendermaker, & Dinkgreve, 2016), the standard procedure of the child welfare agency. This is a supervision and case management method, based on Functional Family Parole Services (Alexander & Robbens, 2010), for engaging, motivating, and working with high-risk youth and multiproblem families. It starts with the engagement and motivation phase in which a care plan is made. Subsequently, the care plan is implemented under intensive case management. When the goals in the care plan are achieved, the child welfare worker prepares the family for case closure. Although the child welfare worker is responsible for all phases, collaboration with the family and, if present, with the extended social network is an important element of the method (Busschers & Boendermaker, et al., 2016).
Families randomly assigned to the control group (from now on referred to as CAU-group) received only IFCM. Families randomly assigned to the experimental group (from now on referred to as FGC group) received IFCM and were offered an FGC. This means that, instead of making a care plan under responsibility of the child welfare worker, families were offered an “Eigen Kracht-conferentie” (Own Strength conference), the Dutch translation of the original model of FGC, to make a care plan. The FGC model consists of four phases: the referral phase, the preparation phase, the conference itself, and the implementation phase. In the referral phase, the child welfare worker gives the family the opportunity to organize an FGC together with their extended network. In this phase, an independent coordinator, who is not affiliated with the child welfare agency, is matched to the family (Marsh & Crow, 2000). In the preparation phase, the FGC coordinator visits the family and extended network and prepares the conference. The conference itself consists of (1) an information part in which professionals share information on the needs and care options and provide, if necessary, conditions for the plan, (2) a family-deliberation part (private part) in which the care plan is developed (no professionals or coordinator is present), and (3) a presentation part in which the family and the extended network present the care plan to the FGC coordinator and the professionals. When the care plan is approved by the child welfare worker, the family and extended network start implementing the care plan and monitor the implementation (see Table 2 for an overview of the key elements of the FGC model).
Level of FGC Completion.
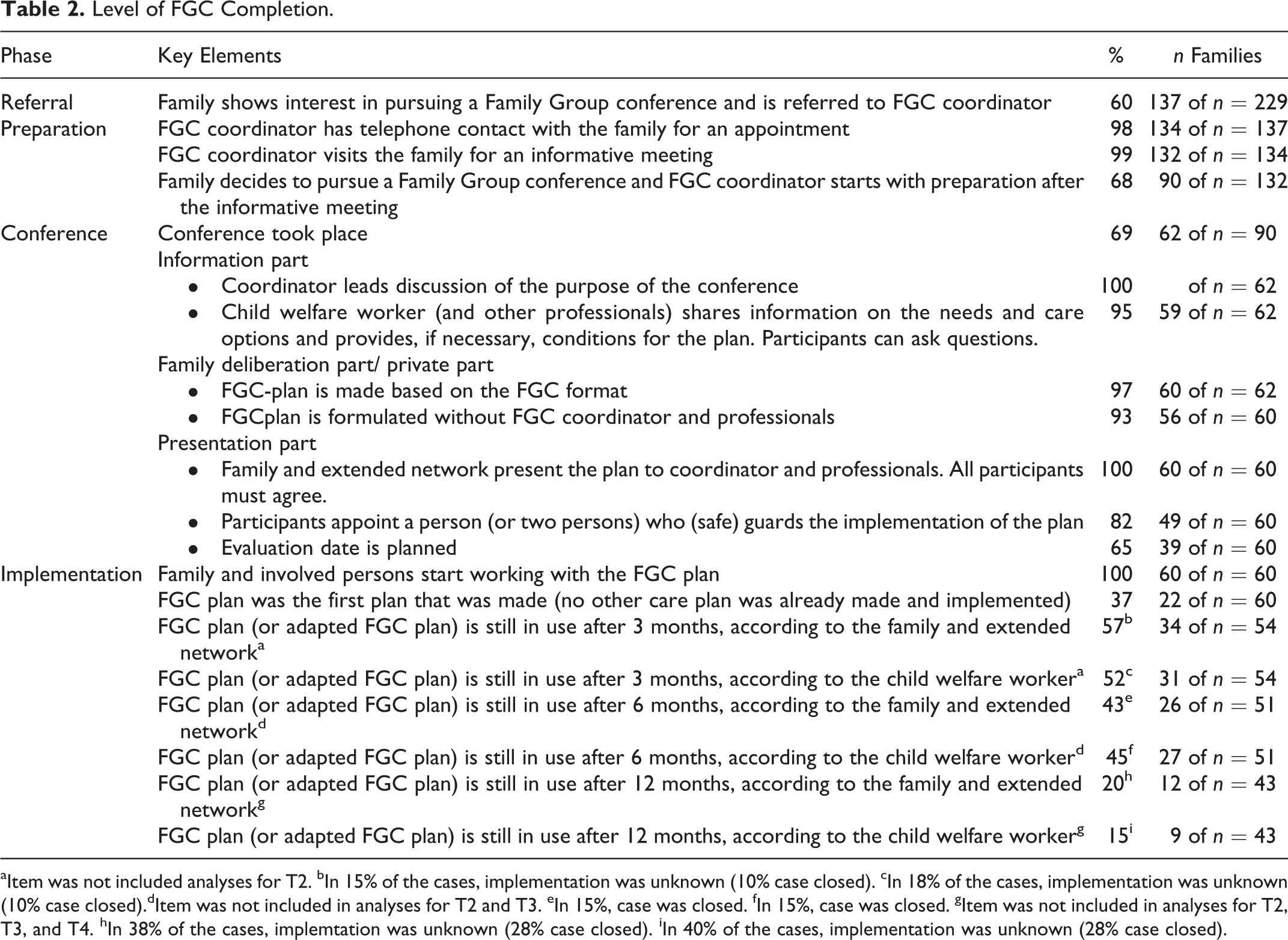
aItem was not included analyses for T2. bIn 15% of the cases, implementation was unknown (10% case closed). cIn 18% of the cases, implementation was unknown (10% case closed).dItem was not included in analyses for T2 and T3. eIn 15%, case was closed. fIn 15%, case was closed. gItem was not included in analyses for T2, T3, and T4. hIn 38% of the cases, implemtation was unknown (28% case closed). iIn 40% of the cases, implementation was unknown (28% case closed).
Procedure
During the first visit with the family, the child welfare worker introduced the study and asked the family permission to share their contact details with the research team. When families agreed, the research team contacted the family, further explained the study, and asked for participation. When families agreed with participation, they filled out an informed consent form, completed the pretest assessment, and their child welfare worker was invited to complete a pretest questionnaire. If two parents were involved, the primary caretaker was asked to participate. Following the pretest, the child welfare worker introduced FGC in the experimental group and informed the research team whether or not the family was interested in FGC. Families who were interested in FGC were contacted by an FGC coordinator who visited the family for an informative meeting. After that meeting, the FGC coordinator notified the research team whether or not families decided to pursue an FGC or not. When a care plan was made, on average 27 weeks (SD = 15.37) and 18 weeks (SD = 14.66) after the start for FGC and CAU group, respectively, the child welfare worker notified the research team. Then, in the FGC group, child welfare workers and FGC coordinators completed an FGC process questionnaire, with questions about the preparation of the conference (for both child welfare worker and FGC coordinator) and about the conference itself (only for FGC coordinator). In addition, for families in both groups, assessment dates for T2–T5 were determined. At T2–T5, questionnaires were completed by phone unless parents could not be reached. In that case, research assistants visited the homes of the families, hoping to reach them. Families received a compensation of 25 euros for participation in the study. A more detailed description of the procedure and design can be found in Asscher and colleagues (2014).
Instruments
Child safety was operationalized into a child safety score, child maltreatment, out-of-home placement, and supervision order. The child safety score was obtained from the child welfare worker at all time points. As part of their regular risk assessment procedure, child welfare workers register a child safety score after all their home visits on a 10-point scale (0 = highly unsafe to 10 = very safe).
Three measures of child maltreatment were distinguished, namely, risk of child maltreatment, assessed by the family and the child welfare worker, and indication of child maltreatment, assessed by the child welfare worker. On T1, T3, and T5, parents completed the short version of Child Abuse Potential Inventory (CAPI-short form; Grietens, Groenewegen, Hellinckx, Baartman, & Weglewski, 2000). The CAPI-short form is a screening tool for the prediction of child physical abuse and consists of 40 items. For the present study, only the subscale “child abuse” was used, consisting of 24 items to be answered on a 2-point scale (0 = disagree and 1 = agree). As risk factors for physical abuse mostly overlap with risk factors for other types of child maltreatment (Mulder, Kuiper, Van der Put, Stams, & Assink, 2018), we used this scale for measuring risk factors for all child maltreatment. Higher mean scores on this measure indicate a higher risk of child maltreatment. Cronbach’s α was .85 at T1 and .83 at T3 and .87 at T5. At all time points, child welfare workers filled out the risk assessment scale of the “Actuarial Risk Assessment Instrument Youth Protection” (ARIJ; Van der Put, Assink, & Stams, 2016), as standard procedure in child welfare. This scale, assessing parental risk of child maltreatment in the future, consists of 23 items to be answered on a 2-point scale (0 = absent and 1 = present). For the present study, we selected the 10 items assessing dynamic risk factors (1 = concerns about offering protection and safety; 2= basic care needs; 3 = rules and restrictions; 4 = stability; 5 = presence of parental psychiatric problems; 6 = parental substance abuse problems; 7 = parental relationship problems; 8 = high level of conflicts; 9 = financial problems; and 10 = low social support) and calculated a mean score (Cronbach’s α was 0.70 at T1, .71 at T2, .67 at T3, .68 at T4, and 0.70 at T5). Indication of child maltreatment was assessed at all time points with items of the ARIJ that focused on indications of child maltreatment, namely 5 items that assess current physical abuse, sexual abuse, emotional abuse, neglect, and domestic violence. Answers on these 5 items were dichotomized (0 = no indication of child maltreatment; 1 = indication of child maltreatment).
Finally, out-of-home placement and supervision order were extracted from case file reports. At pretest, we scored if out-of-home placement or supervision order was present, which was the case in, respectively, n = 53 (16%) and n = 30 (9%) families. For the families where children were not placed out of home or where no supervision order was imposed, we determined whether out-of-home placement or supervision order of one or more children took place at any time prior to the end of the data collection period (T5).
Professional services use was operationalized into the number of professional services used and duration of child welfare involvement. Number of professional services used was measured by the Questionnaire Intensive Care for Youth: health-care utilization and productivity loss (Bouwmans et al., 2012), completed by parents at T4 and T5. Families were asked about their use of professional services in the last 6 months. For the present study, we counted the number of different professional services families used (i.e., psychiatrist, psychologist, psychiatric nurse, social worker, general practitioner, school doctor, paediatrics, medical specialist, and alternative healer). Duration of child welfare involvement was extracted from case files and expressed in days. We determined duration at T2–T5 by subtracting the date of case closure or date of T2, T3, T4, and T5 when the case was not closed, from the date of start with child welfare services.
Parental empowerment was measured by the subscale Family of the Family Empowerment Scale (FES), completed by families at T1, T3, T4, and T5. The subscale Family of the FES consists of 12 items rated on a 5-point Likert-type scale (1 = not true at all to 5 = very true) and assesses parents’ perception of empowerment in parenting situations (Koren, DeChillo, & Friesen, 1992). An example of a question is: “I feel I am a good parent.” Cronbach’s α was .90 at T1, .89 at T3, .90 at T4, and .91 at T5.
Social support was operationalized into two domains: number of different social support sources and perceived social support. Number of different social support sources was assessed by the Parental Support Questionnaire (Dekovic, Gerrits, Groenendaal, & Noom, 1996), completed by parents at all time points. From a list of 15 resources of support, parents indicated the sources they feel supported by. For the present study, only the sources representing the informal social network were included, that is, partner, parents, other family members, neighbors, friends, and babysitter.
Perceived social support was measured by the short version of the Interpersonal Support Evaluation List (ISEL-short form; Cohen & Hoberman, 1983), completed by families at T1, T4, and T5. The ISEL-short form consists of 12 items rated on a 4-point Likert-type scale (1 = definitely false to 4 = definitely true). A lower score means that families perceived limited social support in their life. An example of a question is: “When I feel lonely, there are several people I could call or talk to.” Cronbach’s α was .82 at T1, .86 at T4, and .86 at T5.
Family characteristics
Ethnicity status was assessed with self-reports of parents and defined by the birth country of the parents. If one or both of the parents was/were born in a non-Western country, ethnicity status was coded non-Western (0 = Western status, 1 = non-Western status). Family situation was retrieved from case files of the family at the child welfare agency and was coded as intact families (biological parents married/together) or broken and/or newly formed families (0 = intact families, 1 = broken and/or newly formed families). Indication of parental intellectual disability was assessed by 1 item of the ARIJ (Van der Put et al., 2016), filled in by the child welfare worker (0 = no indication of intellectual disability for one or both parents, 1 = indication of intellectual disability for one or both parents). Education level of parents was assessed by self-reports of parents (0 = low education level [finished primary education or lower levels of secondary or tertiary education], 1 = high education level [finished higher levels of secondary or tertiary education]). Referral reason was assessed from case files and categorized into referral to the child welfare service because of problems related to the parents (e.g., substance abuse or psychopathology), problems related to the child (e.g., delinquency or school-related problems), or problems related to the family system as a whole (e.g., child maltreatment and child neglect).
Level of FGC Completion
As we were not aware of any standardized instruments to assess the level of FGC completion, we used the studies of Berzin et al. (2007), Marcynyszyn et al. (2012), Rauktis et al. (2013), and the Guideline for FGDM in Child Welfare (American Humane Association, in Olson, 2009) to construct an instrument to assess the level of FGC completion. To reach consensus on the included key elements, we organized a Delphi round (Hsu & Sandford, 2007) in which we asked six experts in the field of FGC for their opinion about the included key elements and their importance. We used their feedback to improve our instrument (Table 2). For each of the families, we scored the presence of the key elements in the four phases of the FGC model. For the referral and preparation phase, information was obtained from, respectively, the child welfare worker and the FGC coordinator (see Procedure section). Information about key elements in the conference phase was obtained from the FGC plan and from the FGC process questionnaire, completed by the FGC coordinator. An example item in the FGC process questionnaire is: “Did the child welfare worker share information about the needs of the family.” Information about working with the FGC plan after the conference was obtained with the T2–T5 questionnaires for parents and child welfare workers. All 20 key elements were scored on a binary scale (0 = absent, 1 = present). Then, mean scores were calculated per phase, and the four mean scores were summed to obtain an overall indication of the level of FGC completion at T2, T3, T4, and T5, ranging from 0 to 4. The final six key elements in the implementation phase, about use of the FGC plan at 3, 6, and 12 months after the conference, were only taken into account at the measurement occasions to which they applied. Furthermore, when a case was closed, items pertaining to use of the FGC plan after case closure were not taken into account when calculating the FGC completion score.
Analytic Strategy
Since the decision of the family to pursue a Family Group conference is part of the process of FGC, an intention-to-treat design was applied following the principle of Montori and Guyant (2001). This method was used to eliminate potential confounding effects of treatment motivation. Therefore, all families were included in the analyses, irrespective of their level of completion of the FGC process. 1 To examine the effectiveness of FGC in terms of the continuous outcome measures (child safety score, risk of child maltreatment, parental empowerment, and social support), we performed separate repeated measures analyses of variance to examine differences among the groups at each time point and over time. We conducted ANOVAs for the outcome measures, such as duration of child welfare involvement and number of professional services used. Furthermore, logistic regression analyses were performed to examine the dichotomous outcome measure indication of child maltreatment at each time point, accounting for pretest scores. Additional logistic regression analyses were performed to examine new out-of-home placements and supervision orders during the data collection period. In the latter analyses, we excluded the families in which at pretest one or more children were placed out of home or in which a supervision order had been imposed.
Moderator analyses were conducted to examine whether ethnicity status, family situation, education level of parents, indication of parental intellectual disability, and referral reason affected the effectiveness of FGC. For the repeated measures ANOVAs, we included an interaction between time, condition, and the specific moderator and for the ANOVAs and logistic regression analyses, we included an interaction between condition and the specific moderator. For the dichotomous outcome measures, moderator analyses were only performed when categories were filled with at least 10 families (Peduzzi, Concato, Kemper, Holford, & Feinstein, 1996).
To examine the level of FGC completion, we first calculated descriptive statistics to get more insight in the implementation of the key elements in each phase of the FGC model. To examine the relation between the level of completion and outcome variables, we performed linear regression analyses in the FGC group for the continuous outcome measures and logistic regression analyses for the dichotomous outcome measures, accounting for pretest scores.
Results
Child Safety and Professional Services Used
Families in the FGC group did not differ from families in the CAU group on any of the pretest indicators of child safety and professional services used. At each of the time points and over time (see Table 3), FGC was equally effective as CAU in improving child safety, Wilks’s Λ = 0.99, F(4, 200) = 0.77, p = .55, and reducing the risk of child maltreatment reported by the child welfare worker, Wilks’s Λ = 0 .99, F(4, 199) = 0.48, p = .75, and the parents, Wilks’s Λ = 1.00, F(2, 325) = 0.07, p = .94. Furthermore, indications of child maltreatment were equally prevalent in the FGC and CAU group at all time points. During the data collection period, in 8.7% of the families in the FGC group (17 of 195 families) and in 1.3% of the families in the CAU group (1 of 80 families), one or more children were placed out of home, which was a significant difference (odds ratio [OR] = 7.55; 95% confidence interval [CI] [1.00, 57.68]). With regard to imposed supervision orders, no differences between FGC and CAU were found; in 12% of the families in the FGC group (26 of the 213 families) and in 11% of the families in the CAU group (9 of the 85 families), a supervision order was imposed during the data collection period.
Effects of FGC (n = 229) Versus CAU (n = 99), Child Safety Outcomes.
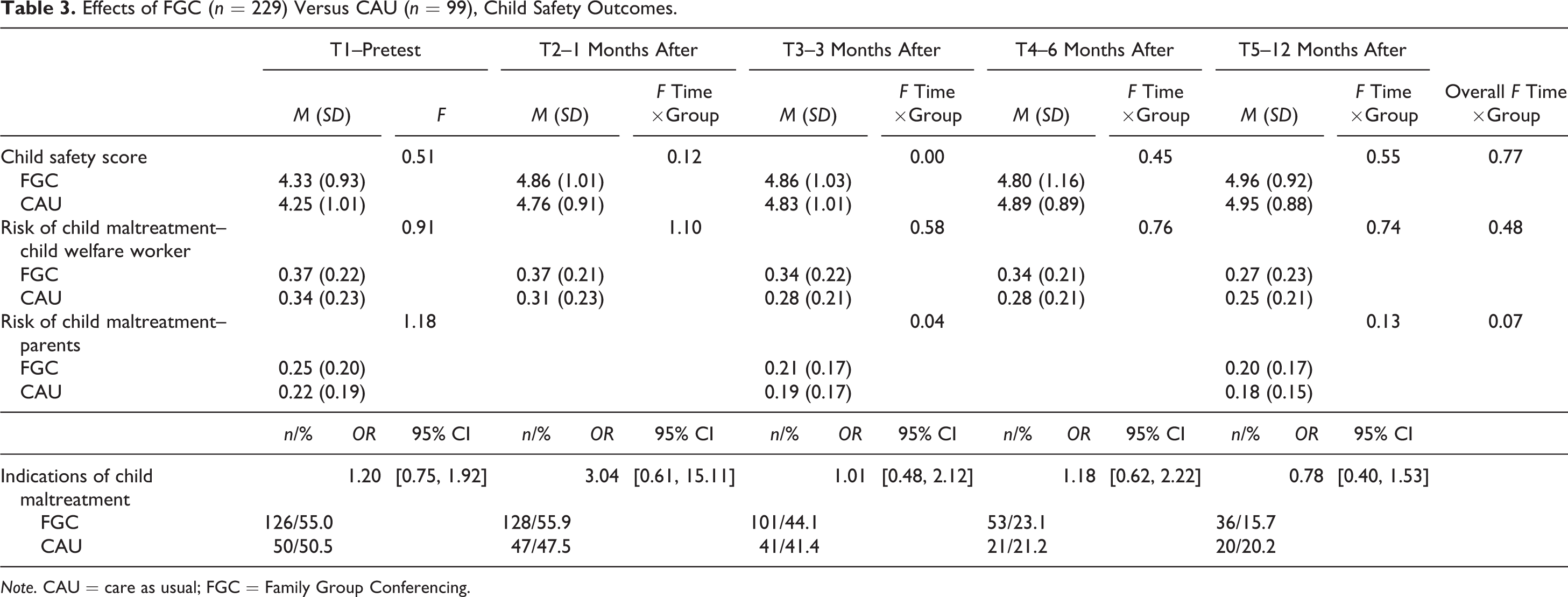
Note. CAU = care as usual; FGC = Family Group Conferencing.
Regarding professional services used (see Table 4), families in the FGC group did not differ from the CAU group in the number of professional services used at T4. However, at T5 families in the FGC group used—at trend level—a higher number of professional services than families in the CAU group, F(1, 326) = 3.48, p = .06, d = −0.22. With regard to the duration of child welfare involvement, families in the FGC group received more days of child welfare services than families in the control group at T2, F(1, 326) = 20.09, p = .00, d = −0.54; at T3, F(1, 326) = 8.59, p = .004, d = −0.40; and at T4, F(1, 326) = 12.87, p = .00, d = −0.44. At T5, differences in duration of child welfare involvement between families in the FGC and families in the control group were no longer significant, F(1, 326) = 2.42, p = .14.
Effects of FGC (n = 229) Versus CAU (n = 99), Involvement of Professional Services Outcomes.
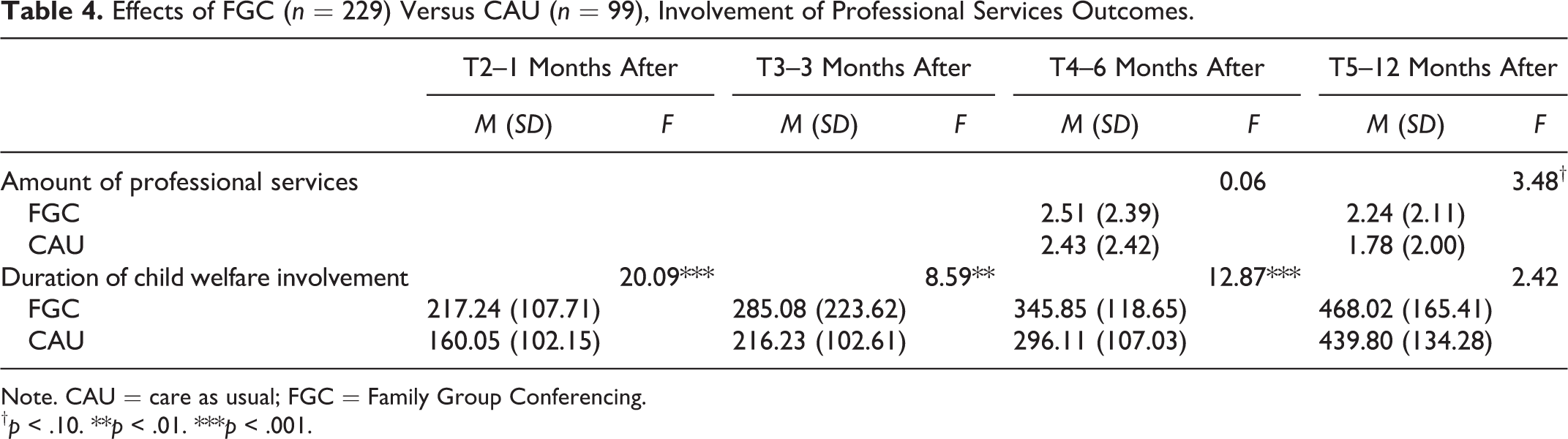
Note. CAU = care as usual; FGC = Family Group Conferencing.
† p < .10. ** p < .01. *** p < .001.
Self-Reported Parental Empowerment and Social Support
At pretest, families in the FGC group did not differ from families in the CAU group on parental empowerment and social support (see Table 5). Over time, families in the FGC group differed at trend level from families in the CAU group in the level of parental empowerment, Wilks’s Λ = 0.98, F(3, 324) = 2.25, p = .08. For the FGC group, the level of parental empowerment increased from T1 (M = 4.10, SD = 0.60) to T3 (M = 4.24, SD = 0.46), p < .01, 95% confidence interval [CI] [−023, −0.04], from T1 to T4 (M = 4.26, SD = 0.49), p < .001, 95% CI [−0.23, −0.07], and from T1 to T5 (M = 4.23, SD = 0.49), p < .01, 95% CI[−0.23, −0.02]. However, in the CAU group, the level of parental empowerment did not increase over time. In addition, 6 months after the start of the implementation phase, families in the FGC group reported a significantly higher level of parental empowerment compared to families in the CAU group, Wilks’s Λ = 0 .99, F(1, 326) = 4.46, p = .04, d = 0.08. At T2, T3, and T5, no differences between the groups were found.
Effects of FGC (n = 229) Versus CAU (n = 99), Parental Empowerment and Social Support.
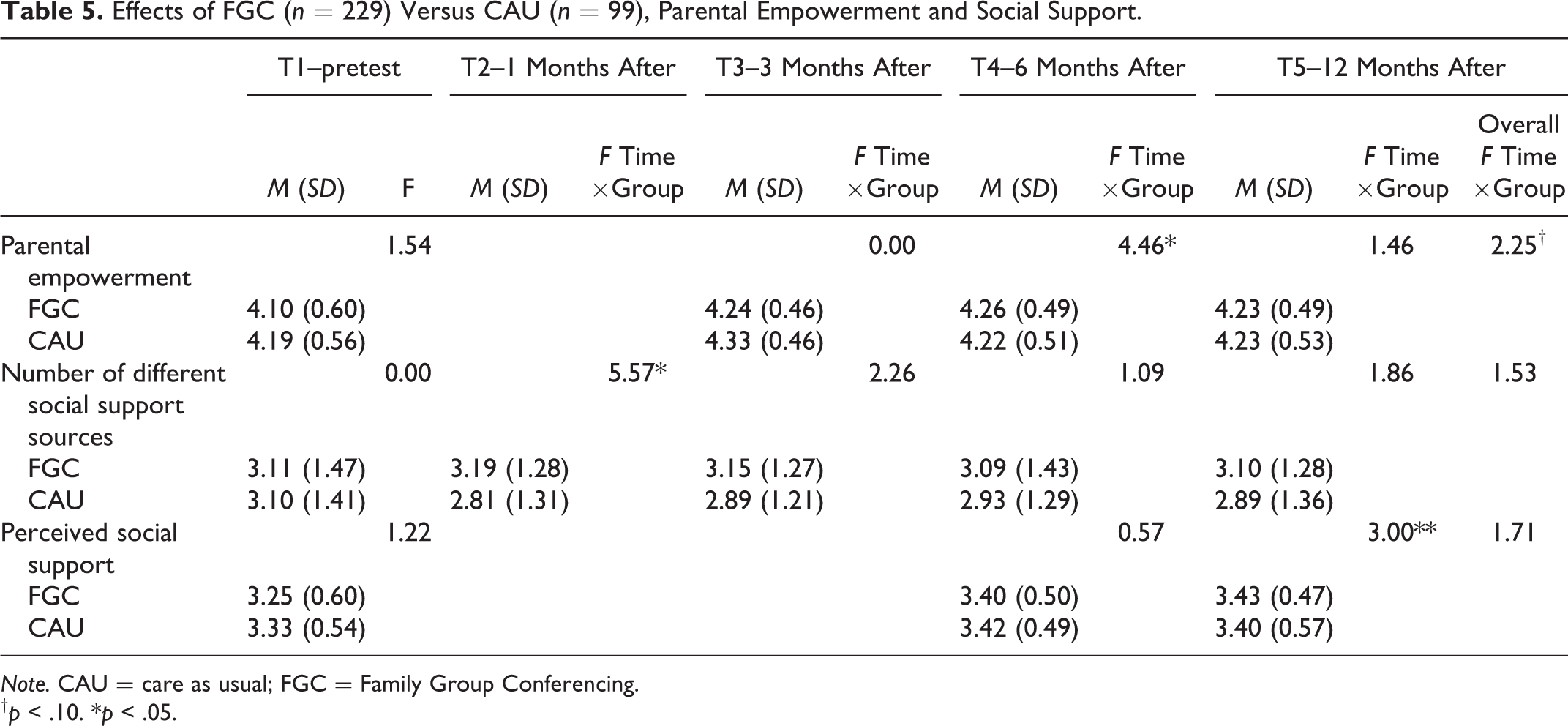
Note. CAU = care as usual; FGC = Family Group Conferencing.
† p < .10.* p < .05.
Over time, families in the FGC group did not differ from families in the CAU group in the number of different social support sources, Wilks’s Λ = 0.98, F(4, 323) = 1.53, p = .19, and perceived social support, Wilks’s Λ = 0.99, F(2, 325) = 1.71, p = .18. However, 1 month after the start of the implementation phase, families in the FGC group reported a higher number of social support sources than families in the CAU group, Wilks’s Λ = 0.98, F(1, 326) = 5.57, p = .02, d = 0.29. Furthermore, after 12 months, a trend was found suggesting higher levels of perceived social support in the FGC versus CAU group, Wilks’s Λ = 0.99, F(1, 326) = 3.00, p = .08, d = 0.05.
Family Characteristics as Moderator of FGC
To examine whether FGC was more likely to be effective for specific subgroups of families, we analyzed the influence of ethnicity status, family situation, education level of parents, parental intellectual disability, and referral reason. For the dichotomous outcomes indications of child maltreatment, out-of-home placement, and supervision order, categories of the moderators were insufficiently filled. Therefore, no moderator analyses were performed for these outcomes. The other potential moderators (ethnicity status, family situation, education level of parents, parental intellectual disability, and referral reason) did not moderate the effectiveness of FGC.
Level of FGC Completion
The average level of FGC completion was 1.48 (SD = 1.39, range = 0−4). In the referral phase, 60% (137 of the 229 families) showed interest in pursuing an FGC and were referred to an FGC coordinator. Eventually, for 27% of these families (62 of the 229 families), a conference took place, and for 60 families, a FGC plan was made. All 60 plans were approved by the child welfare worker. For most of the families that made an FGC plan, the different stages in the conference phase were completed successfully. However, for 11 of the 60 families, no safe guards for implementation of the plan were assigned, and for 21 of the 60 families, no evaluation date was planned. In addition, for 22 of the 60 families, the FGC plan was the first and leading plan and no other care plan, made by the child welfare worker, was in use. Twelve months after the conference, 12 of the 60 families and 9 of the 60 child welfare workers reported that the FGC plan (or adapted FGC plan) was still being used. For more detailed information about the level of FGC completion, see Table 2.
The relation between the level of FGC completion and each of the outcome variables is presented in Table 6. Higher levels of completion were related to a higher number of different social support sources at T2 (β = 0.13, p = .02), T3 (β = 0.13, p = .03), and T4 (β = 0.09, p = .08). In addition, higher levels of completion were related—at trend level—to lower levels of parental empowerment at T4 (β = −0.09, p = .09) and a higher number of professional services used at T5 (β = 0.21, p = .002). No other outcomes were related to the level of FGC completion.
Relation Between Level of Completion of FGC and Outcome Variables.
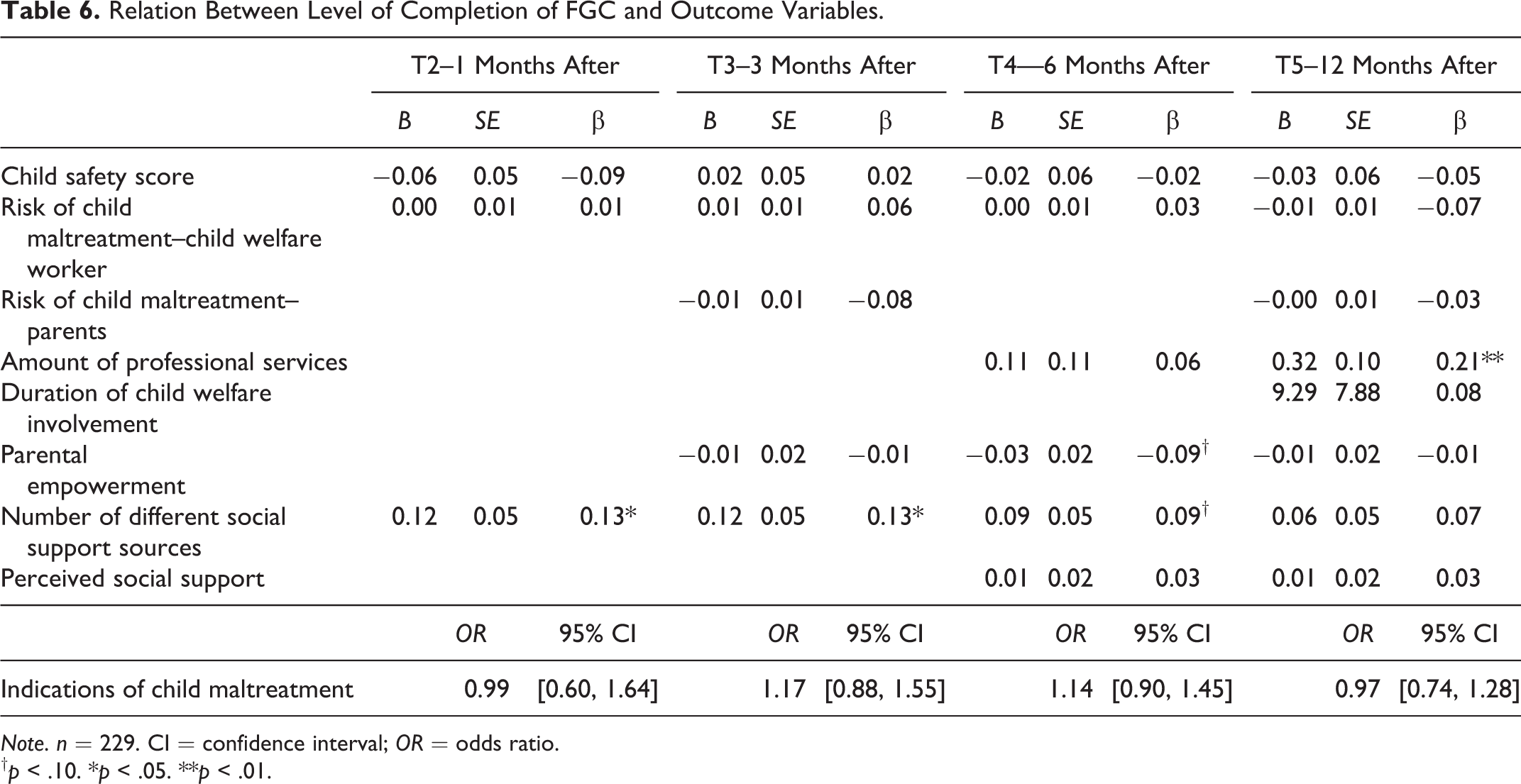
Note. n = 229. CI = confidence interval; OR = odds ratio.
† p < .10. * p < .05. ** p < .01.
Discussion
The present study aimed to examine the effectiveness of FGC in child welfare. In line with the findings of previous controlled studies), FGC did not outperform CAU in improving child safety, reducing child maltreatment and the risk of child maltreatment, and reducing the number of supervision orders. When compared to CAU, FGC resulted in more families in which children were placed out of home. However, due to the relatively small number of out-of-home placements, this result needs replication in a larger sample.
With regard to involvement of child welfare, we found that at T2, T3, and T4, FGC was associated with a longer duration of child welfare involvement compared to CAU. This may be explained by the relatively long period of time needed to prepare the conference, resulting in a later start of the implementation phase than is observed in regular care (27 and 18 weeks, respectively). As this may postpone the start of professional service use that is needed in some families, this longer period of decision-making might delay improvement in the family situation and extend the period of involvement of child welfare services. At the long term, the difference in duration of child welfare involvement between the FGC and CAU group disappeared. This finding suggests that for families with persistent problems that require long-term involvement of child welfare services, the FGC and CAU approach cannot be differentiated in terms of duration of care.
With regard to the number of professional services used, there were no short-term differences (6 months after the implementation phase) between FGC and CAU. However, at T5, our findings suggest that families in the FGC group used a marginally higher number of professional services than families in the CAU group, which was caused by a faster decrease in the number of professional services used in the CAU group. This result is in contrast to the expectation that FGC would lead to less use of professional services at longer terms (MacLeod & Nelson, 2000; Moore & McDonald, 2000). Whether this is a positive or negative outcome is not completely clear. On the one hand, it is positive when families use professional services if they need it. On the other hand, it is unclear if they need it because their needs are adequately identified or because the care to date has not been effective. Furthermore, it should be emphasized that the number of professional services used does not provide the complete picture of professional service use, as the frequency of use was not taken into account.
Regarding the effectiveness of FGC in terms of parental empowerment and social support, our findings suggest that over time and 6 months after the conference took place, families in the FGC group felt somewhat more competent than families in the control group. However, no effects for FGC on parental empowerment were found 1, 3, and 12 months after the start of the implementation phase.
With regard to social support, we found that FGC was minimally effective in improving perceived social support. However, we did find that, 1 month after the implementation period started, families in the FGC group reported a higher number of different social support sources than families in the control group. This difference between the FGC and CAU group was not observed after 3, 6, and 12 months. Our data indicate that this short-term difference is caused by a drop in the number of social support sources in families receiving regular care, rather than by an increase following FGC. Possibly, FGC may serve to reinforce strength and duration of existing social support while, without FGC, these supports may naturally drop off. It should be noted, however, that with this measure, we could only examine the number of sources of social support and not the total number of supporting people in the families network.
Possibly, the absence of significant differences between FGC and CAU in improving social support can be explained by the method that was used in the control group. About 10 years ago, the model of FGC was a new and innovative method in the child welfare system where own responsibility of the families and involvement of the extended social network did not receive much attention. Nowadays, in the whole child welfare system, including the child welfare agency where this study was performed, child welfare workers are trained to activate parents and to involve the extended network as a support system. Although FGC is a more progressive and concrete way to achieve these goals, by, for example, the involvement of an independent coordinator and a conference with a private part, CAU may result in nearly similar improvements in perceived social support. Based on these findings, we can conclude that, overall, FGC minimally outperformed CAU in increasing parental empowerment and social support. Our results do not provide support for a theory of change in which FGC leads to improved child safety and less involvement of child welfare through increases in parental empowerment and social support.
Beside examining outcome effects, we included moderators to determine which families are most likely to benefit from FGC. We did not find any influence of ethnicity, family situation, education level of parents, parental intellectual disability, and referral reason, which indicates that, based on these family characteristics, subgroups of families do not benefit more from the FGC model than other families. This is in line with results of the meta-analysis on the effectiveness of FGC (Authors’ citation, 2016a).
Furthermore, we examined the level of FGC completion and related it to the outcomes. The average level of FGC completion was relatively low, which could largely be explained by the high dropout rates in the first two phases of the FGC process and—to a lesser extent—by inadequate use of the FGC plans (another care plan was already in use, no stakeholders were assigned to monitor the implementation of the plan, no evaluation was scheduled, the plan was not used nor adapted). When the level of completion was linked to the results of FGC at 1, 3, 6, and 12 months after the start of the implementation phase, we found at all time points that higher levels of completion were related to a higher increase in the number of different social support sources. In contrast, 6 months after the start of the implementation phase, higher levels of completion were related to a higher number of professional services used. Furthermore, higher levels of completion were related to lower parental competence, which is remarkable since we did find that families in the FGC group felt more empowered than families in the CAU group 6 months after the start of the implementation phase. An explanation for this might be that many families referred to child protection services are not capable of addressing the required skills (i.e., taking own responsibility and problem-solving skills) to successfully complete FGC. For these families, carrying out the FGC model as intended—resulting in higher levels of completion—might be demanding, which may result in lower levels of parental competence. Alternatively, families with higher levels of FGC completion may feel more exposed, which may adversely affect empowerment.
When compared to CAU, we did find positive effects of FGC on parental competence. This combination of findings suggests that particularly families that did not complete all phases of FGC, resulting in lower levels of FGC completion, experienced an increase in parental competence. Berzin et al. (2007) stated, based on their program fidelity data, that the most important aspects of FGC are listening to the voice of the family and respecting their needs, which are aspects that are embedded in the first two phases of FGC. Possibly, offering FGC to the family might be enough to increase the levels of parental competence. Further research focusing on the relation between the levels of FGC completion and outcome variables is needed to confirm this hypothesis.
In conclusion, since the main goal of child welfare services is to improve child safety, the present study showed that FGC, as a more progressive and concrete way to achieve this goal by involving the social network with special focus on empowering families, did not outperform CAU. Although our findings on secondary outcome measures were small and inconsistent, they provide some support for Berzin’s suggestion (2006) that probably FGC may not be strong enough to effectively improve child welfare outcomes, but that it might be effective in terms of other beneficial and more intermediate outcomes, such as parental empowerment and social support.
Strengths and Limitations
Although the results of the present study are important for the field of child welfare where FGC is often used, some limitations of this study should be acknowledged. First, although participation rate at baseline was relatively high (66%) considering the target population of child welfare agencies, nonresponse analyses indicated that non-Western families and broken families were less likely to participate. Because of this participation bias, generalization to the entire population of child welfare should be done with caution. In addition, generalization to FGC models that hold specific exclusion criteria may be limited, as the FGC model under study was assumed to be suitable for all families.
Second, despite the inclusion of a large number of families, out-of-home placements and supervision orders were relatively uncommon, resulting in less robust results on these measures. Additionally, for indication of child maltreatment, the categories were insufficiently filled to conduct moderator analyses.
Third, during the data collection, there was high staff turnover. In 50% of the families in this study, 51.1% in the experimental and 47.5% control group, χ2(1, 328) = 0.36, p = .55, a new child welfare worker was assigned between T1 and T5, which has been shown to increase the duration of a supervision order in child welfare (Busschers, Van Vugt, & Stams, 2016). For these families, information reported by the child welfare worker was derived from different persons (who may have different perspectives on the family situation).
Fourth, it should be emphasized that results at 1, 3, and 6 months after a care plan was made were obtained after an, on average, longer period of child welfare involvement for families in the FGC group when compared to families in the CAU group. This is a result of the longer period of time needed to make a care plan using FGC.
Finally, the results for level of FGC completion may be affected by selective dropout during the FGC process. More specifically, drop out during the FGC process—resulting in a lower level of completion—may possibly be explained by characteristics that also affect the receptivity of families to child welfare support. Up to now, knowledge on predictors of FGC dropout is limited (Dijkstra et al., 2017). On the other hand, because dropout during the FGC process is part of FGC practice, we believe it is important to study the effectiveness of FGC by comparing families who are randomly assigned to the FGC and control condition. This study is one of few that examined the effectiveness of FGC by means of a randomized controlled trial. Most of the previous studies on the effectiveness of FGC focused on the select group of families who fulfilled Phase 3, the conference phase, which might lead to biased results. Therefore, the present results give more insight in the process of FGC.
Implications
The results of this study have some practical implications. First, since we did not find effects for FGC on improved child safety, the main goal of child welfare services, it is important for policy makers and clinical practice to consider the investments and costs of FGC compared with regular care. Second, since the longer period of time needed to establish a care plan in FGC may delay improvement in the family situation and extend the period of involvement of child welfare services, families may be offered additional support or guidelines to accelerate the process of FGC.
In addition, this study leads to various implications for future research. To further understand the influence of the decision-making model (FGC or CAU) on empowerment, social support, and eventually child safety, research with a strong focus on the start of child welfare involvement/FGC is needed. In such studies, short intervals between measurements allow for the identification of mechanisms of change. In addition, besides level of FGC completion, it would be interesting to examine the relative ease or difficulty that families encounter during the decision-making process, as well as the period that is needed to develop a care plan, and relate these to its outcomes. In such studies, child welfare worker and agency characteristics that may impact the decision-making process should not be overlooked (Allan, Harlaar, Hollinshead, Drury, & Merkel-Holguin, 2017). In addition, it seems particularly interesting to study how parental empowerment is affected by child welfare involvement and by sharing family problems with the extended social network.
Finally, cost-effectiveness analyses are recommended to determine whether the small and temporary positive effects on parental empowerment and social support compensate for higher costs associated with FGC, a longer duration of child welfare involvement and—to a smaller extent—a higher number of professional services used.
Footnotes
Authors’ Note
The authors declare that the manuscript has not been published elsewhere and is not under consideration by any other journal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by the Dutch organization for Health research and Development (ZonMW), grant number: 70-72900-98-13158.