
Abstract
Research shows care coordination contributes to integrated care experiences. Yet evidence from system-level initiatives is lacking. Using a survey of Veterans Health Administration (VHA) patients linked with clinical records, this nonrandomized, cross-sectional study compares perceived care integration among patients at high risk of hospitalization or mortality who did and did not receive care coordination services at 31 VHA sites during early implementation of a national initiative. Six validated dimensions included: knowledge about patient’s medical history among staff, providers, and specialists; provider support for self-directed care and for medication adherence and home care; and test results communication. Among 714 respondents, 48% had received care coordination services, 78% were 65 or older, and 95% were male. Regression models suggest little association between receipt of care coordination and perceived care integration. Implementation monitoring followed by responsive adaptations may be needed to boost patient perceptions of care integration.
Introduction
Improving care coordination and integration for people with complex care needs is a focus of health systems and policy makers, because their care is often fragmented due in part to seeing multiple providers (Bindman & Cox, 2018). Interventions intended to improve care coordination and integration and patient outcomes include accountable structures and processes for communication and implementation of a comprehensive plan of care across providers and that is patient-centered (Duan-Porter et al., 2022; Fryer et al., 2016). Despite widespread adoption, such interventions have produced mixed results (Duan-Porter et al., 2022; Fryer et al., 2016), including within the US Veterans Health Administration (VHA; Sjoberg et al., 2022; Swankoski et al., 2023). Similarly, measurement of patient perceptions of care integration have been examined and validated (Frean et al., 2021; Fryer et al., 2016; Kerrissey et al., 2017), including among US Veterans (Benzer et al., 2019, 2020; Charns et al., 2022). Yet these studies were conducted prior to implementation of new VHA care coordination and integration initiatives, passage of legislation expanding Veterans’ options to use care in non-VHA community settings, and the COVID-19 pandemic, which was accompanied by a marked uptick in telehealth. Given changes to health care delivery since these events, there is an opportunity to assess more current evidence regarding patient perspectives of care integration. In addition, with increased attention on incorporating physical as well as social needs into care coordination efforts (Bodenheimer & Berry-Millet, 2009; Kuluski et al., 2017; Renaud et al., 2023; Scholz Mellum et al., 2018), updated evidence will be informative for helping health systems to better understand the mechanisms through which care coordination services improve patient care and outcomes, and reasons why some care coordination interventions may not yield expected improvements.
The VHA is the largest national integrated health system in the United States, providing care at 1,255 health care facilities, including 170 VHA Medical Centers and 1,074 VHA outpatient clinics, and serving over 9 million Veterans, over one-third of whom have multiple chronic conditions (Veterans Health Administration, 2018). According to the latest VHA Enrollment and Health Care Projection models, this proportion is likely to remain higher than for the general population, with the aging of the Vietnam era Veteran population and the increasing number of enrollees being adjudicated for service-connected disabilities who require more services (Veterans Health Administration [VHA] Office of Enrollment and Forecasting, 2025). Comorbid mental health and physical health conditions are common among Veterans, which has led VHA to integrate primary care and mental health care teams, a change which has been associated with reduced hospitalization rates (Bohnert et al., 2013; Leung et al., 2018). Also, as the VHA has reorganized its purchased community care options, more Veterans are receiving some VHA-covered care from community-based providers, in particular for specialty care; assessing the extent of care integration with these changes may inform health system improvements (Singer, Sinaiko, et al., 2020; Sjoberg et al., 2022).
The VHA has undertaken initiatives to define, transform, and integrate case management and care coordination to support care integration across all facilities (Greenstone et al., 2019; Kilbourne et al., 2018). One of these health-system-level efforts underway at the time of our study is the Care Coordination & Integrated Case Management (CCICM) initiative, intended as a practice framework to implement integrated organizational processes and optimize care coordination efficiency by reducing duplication and fragmentation of service delivery (Care Coordination and Integrated Case Management [CCICM] Implementation Guide, 2024; Greenstone et al., 2019; Swihart & Hess, 2018). The CCICM was developed with engagement of subject matter experts, VA Offices of Nursing Services and Patient Care Services-Care Management and Social Work, and was intended to establish processes that would enable integration of safe, efficient, and cost-effective care coordination, case management, and care management (Care Coordination and Integrated Case Management [CCICM] Implementation Guide, 2024; Greenstone et al., 2019). It began with 12 test sites from 2017 to 2019 and proceeded to the early implementation phase in 2021 and has continued through a progressive deployment phase.
The CCICM practice framework comprises a multidisciplinary process, involving nursing and social work in collaboration with primary and specialty care, and with steps as depicted in Figure 1. Key process components include: (a) applying standardized risk stratification and predictive analytics using patient health records to proactively identify Veterans who would benefit from care coordination services; (b) review of patient risk stratification levels by a Care Coordination Review Team (CCRT) and assignment of a Lead Coordinator based on the level of a Veteran’s prominent care coordination needs being moderate to high; and (c) creation of one care plan to integrate communication, collaboration, and coordination along the continuum of care (Figure 1; Veterans Health Administration [VHA] Care Coordination and Integrated Case Management [CCICM], 2024). CCRTs comprise case managers supporting individual Veterans, care managers supporting a population of Veterans with a shared diagnosis, and care coordinators supporting Veterans across multiple care environments (Greenstone et al., 2019). With growing numbers of Veterans in the VHA with multimorbidity and social needs, attention to health care delivery integration across VHA and non-VHA providers with new initiatives like the CCICM, evidence regarding patient perspectives about care coordination and integration could help to inform areas for improvement in care needs assessment, communication, care transitions, and follow-up care.
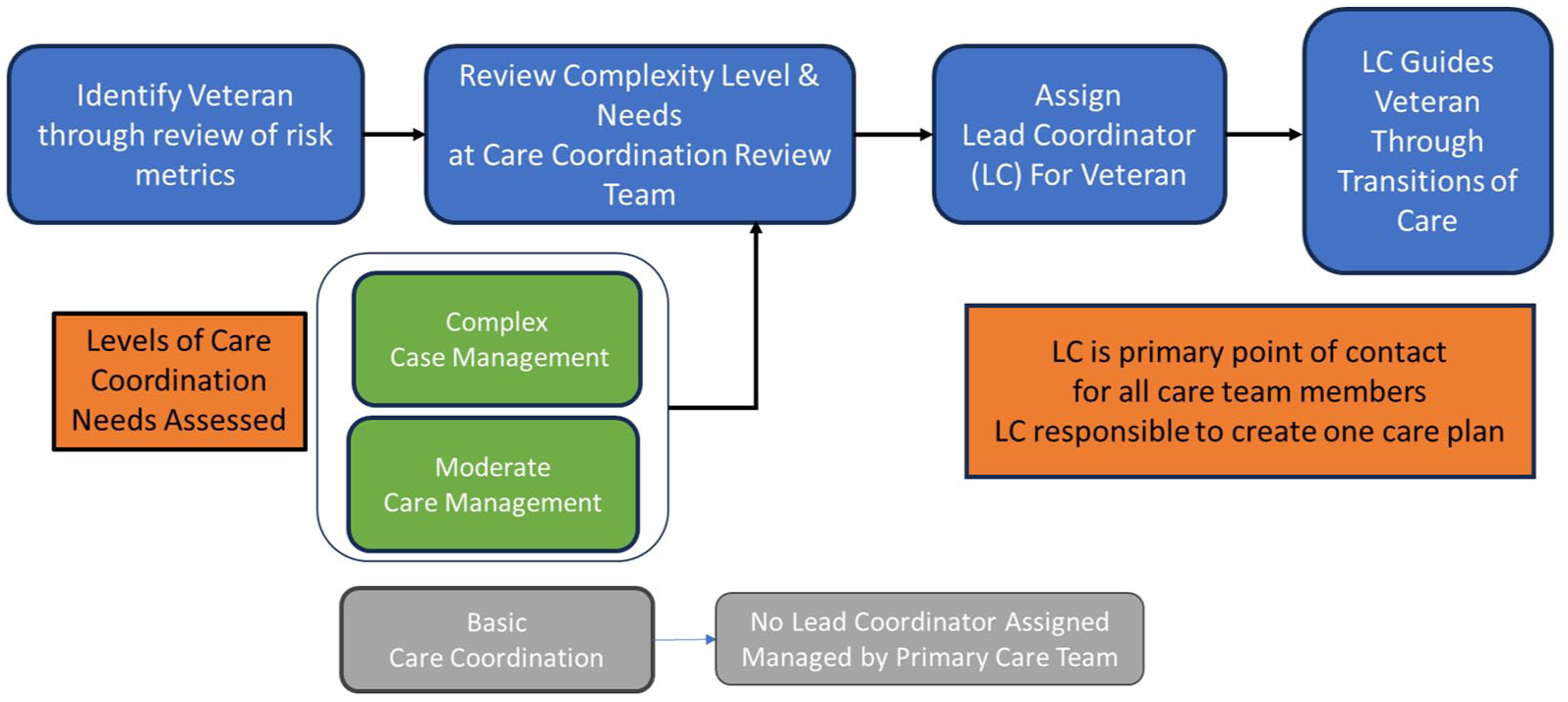
The Care Coordination and Integrated Case Management (CCICM) Practice Framework Key Process Components Include: (a) Applying standardized risk stratification and predictive analytics using patient health records to proactively identify Veterans who would benefit from care coordination services, such as by screening for Care Assessment Need (CAN) score for risk of hospitalization; limitations in activities of daily living; housing and transportation needs; frequency of ED visits, etc.; (b) Review of patient risk stratification levels by a care coordination review team (CCRT) and assignment of a Lead Coordinator for those identified as having complex case management or moderate care management level needs; and (c) Creation of one care plan by the Lead Coordinator to integrate communication, collaboration, and coordination along the continuum of care and to update the care plan as needed and guide the patient through care transitions.
The purpose of this paper is to describe perspectives about care integration dimensions reported by Veterans at high risk of hospital admission and/or mortality and the association with receipt of care coordination services. During a time when the CCICM initiative was undergoing early implementation, we sought to compare perspectives between Veterans who did and did not receive care coordination services at one of 31 VHA sites participating in CCICM’s first implementation phase. We hypothesized that Veterans who received care coordination services would have higher levels of perceived care integration than Veterans who did not. This work is part of a larger study focused on understanding the role of care coordination in Veterans’ health care delivery and outcomes (Hynes et al., 2023).
New Contribution
This study is the first to describe Veteran perspectives of care integration and their association with receipt of care coordination services during the commencement of a system-wide initiative intended to improve VHA care coordination services and care integration. Using validated measures of perceived care integration, we surveyed Veteran patients who did and did not receive care coordination services and compared their perspectives on six dimensions of care integration. We carried out robust multivariable analyses adjusting for patient, facility, and regional factors.
Method
Participants
In a prospective non-randomized cohort study, we identified Veterans receiving care in FY2021 (October 2020-September 2021) at VHA facilities, which self-selected to participate in the CCICM during the first implementation phase. Veterans were identified from electronic health records and classified as being at high risk of hospitalization or mortality based on having at least one Care Assessment Need (CAN) score of 85 or higher in FY2021 and being alive at the end of FY2021 (n = 262,169) (Ruiz et al., 2018; Wang et al., 2013).
Survey Data Collection
For selected sites, we used proportional sampling relative to patient volume at each site to randomly select eligible patients for study participation, split equally between those with and without receipt of care coordination services. Power analyses conducted in PASS v16.0.5 using n = 660 respondents (25% of the estimated sample n = 2,640 of survey recipients), a maximum standard deviation of 0.9, 96% power, and α = 0.05, detected a significant difference between group means as low as 0.3. Sample size was informed based on previous work by Benzer et al. (2020) using an adaptation of the Patient Perceptions of Integrated Care (PPIC) instrument on a cohort of Veterans. Patients were recruited using 1–2 mailings between November 2022-February 2023. Both paper and online data collection via mail and Research Electronic Data Capture (REDCap), respectively, were used (Harris et al., 2009).
Measures
Measures of integrated care were drawn from an adaptation of Singer’s integrated care framework (Singer et al., 2011) and the PPIC 2.1 survey instrument (Friedberg et al., 2021), which has been validated and psychometrically tested to evaluate patients’ perspectives about integration of care (Friedberg et al., 2021; Singer et al., 2013), including in the VHA (Benzer et al., 2019). Measures included the six dimensions of the PPIC 2.1 (Table 1): (a) provider knowledge of the patient’s medical history (5 items), (b) staff knowledge about the patient’s medical history (3 items), (c) specialist knowledge about the patient’s medical history (1 item), (d) provider support for the patient’s self-directed care (5 items), (e) provider support for medication adherence and home health management (4 items), and (f) test result communication (3 items). The survey instrument contained 68 items. Questions used a Likert-type response scale (e.g., 1 = never, 4 = always) and dimension scores were scored using all available responses, meaning if a factor’s items were not all answered, scores were based on the answered items, except for the specialist knowledge about the patient’s medical history, which comprised one item and was dichotomized from: “Yes, definitely,” “Yes, somewhat,” or “No” to “Yes” or “No.” (A list of all items included is in Supplemental Table 1). Higher scores indicate greater perceived integration.
Patient Perceptions of Integrated Care (PPIC) 2.1 Survey Dimensions and Sample Questions.
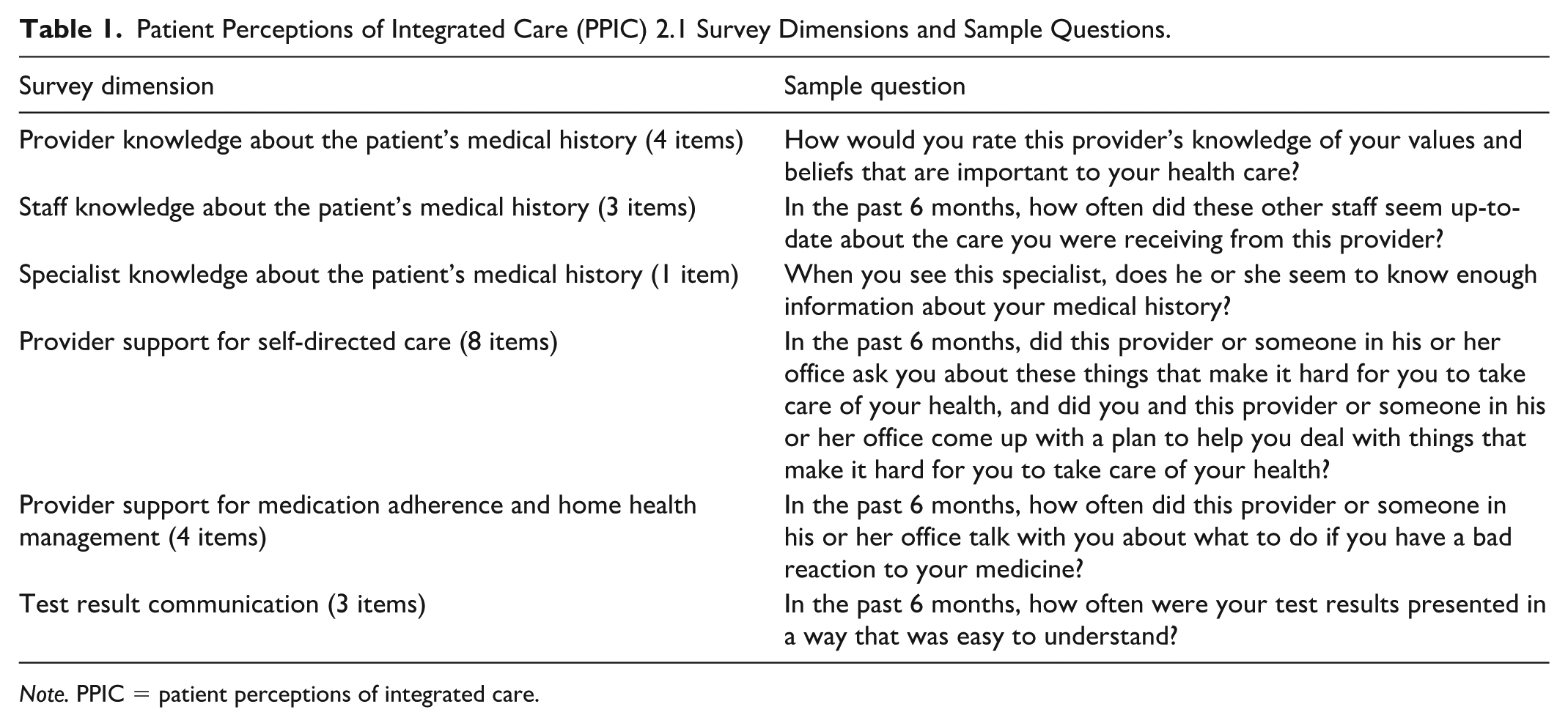
Note. PPIC = patient perceptions of integrated care.
The primary independent variable was documentation of receipt of care coordination services in VHA. Patients were categorized as having received care coordination services or not based on presence of a chronic care management or transitional care management CPT code (see Supplemental Table 2; Agarwal et al., 2020; Gardner et al., 2018; Rivera et al., 2018), and/or by completion of a care coordination needs assessment recorded in the electronic health record during FY2021, the year prior to survey administration. Since survey administration was delayed until November 2022, we also accounted for any services that occurred in the interim in sensitivity analyses.
Additional survey measures included the standardized life orientation test-revised (LOT-R) scale to account for potential differences in individual tendency to give more positive or negative responses (Glaesmer et al., 2012). Respondent characteristics from the survey also included sex (male, female), race (African American/Black, White, Asian, Native Hawaiian or other Pacific Islander, American Indian or Alaska Native, Other Race), Hispanic/Latino ethnicity (yes or no), marital status (married or living with a significant other/not), living situation (live alone/not live alone/unknown), help with survey (yes/no).
Other Data Sources
Data from respondents’ VHA-linked electronic health records from the Corporate Data Warehouse (CDW) were used for patient age, sex, race, Hispanic/Latino ethnicity, marital status, and zip code. CDW data was used to impute these demographics when survey responses were missing/unknown. Drive time to the nearest VA primary care site was also drawn from CDW. Respondents’ zip code of residence was categorized as urban or rural/highly rural based on the US Department of Agriculture Rural-Urban Commuting Area Codes. Respondents’ county overall social vulnerability index (SVI), was calculated from the Centers for Disease Control measures (CDC/ATSDR Social Vulnerability Index [SVI], 2022; Flanagan et al., 2018).
Respondents’ clinical characteristics and health care use variables were drawn from the CDW and Medicare claims data (US Department of Veterans Affairs, Health Services Research & Development, 2014). These included FY2021 total VHA outpatient visits, Medicare Fee-for-Service (FFS) outpatient visits, Elixhauser readmission score (Moore et al., 2017), individual Elixhauser comorbidity categories for mental health conditions (3 categories) and diabetes (2 categories), and VHA reliance, defined as the proportion of outpatient visits paid for by the VHA (either VHA-direct or VHA-purchased) relative to all outpatient visits (VHA and Medicare FFS) in FY2021.
Statistical Weighting
We calculated inverse probability of treatment weights (IPTW) to account for possible biases for receipt of care coordination services using characteristics found predictive of receiving said services based on previous research; these included age, gender, race, ethnicity, marital status, VHA copayment status, Medicare FFS outpatient use, rural residency, and drive time to closest VHA primary care (Govier et al., 2024). In addition, analytic survey weights to approximate a representative sample of the population were generated and used in all analyses. Finally, we generated nonresponse weights based on predictions from a logistic regression model estimating the probability of responding to the survey based on age, race, ethnicity, marital status, and an interaction between receipt of care coordination and the Veteran primary VA care site. These weights were combined and scaled to match the population total (described in the Participants section).
Statistical Analysis
We compared respondents’ characteristics by receipt of care coordination services (yes/no) using descriptive statistics, and calculated weighted absolute standardized mean differences (SMDs) between groups (Austin, 2009). To estimate associations between multi-item factor scores and receipt of care coordination services, we estimated weighted multivariable linear regression models, adjusting for participant characteristics (age, sex, race, Hispanic/Latino ethnicity, marital status, living situation, help with survey, rurality of residence, SVI, Elixhauser score, VHA outpatient use, VHA reliance). Specialist knowledge only had one item and was modeled with a weighted logistic regression model with the above patient characteristics (excluding race and living situation due to model boundary issues). Sensitivity analyses were performed using the same modeling strategy as above adding LOT-R score, self-reported health (very good/excellent or less than very good/excellent), and Elixhauser measures for mental health conditions and diabetes as covariates. In additional sensitivity analyses, since there was a delay from initial classification of patients care coordination group through September 2021 (FY2021) and the survey initiated in November 2022, we conducted the same modeling approach with revised care coordination group classification based on patient’s receipt of care coordination in the year before their survey was returned and recorded.
All analyses used complete cases and were performed using R version 4.4.1 (R Core Team, 2024). Statistical significance of coefficients was determined a priori at α = 0.05. For SMD, effect sizes were determined a priori at 0.2 = small effect, 0.5 = medium effect, 0.8 = large effect (Cohen, 1988).
Results
Among the 2,640 Veterans surveyed, 714 responded (response rate 27%, and varied across sites; see Supplemental Figure 1); 48% (n = 345) had documented care coordination services during FY2021, mean age in the overall cohort was 69 years (SD = 12), with 71% who were 65 years or older, 94% were male, 78% were White race, 94% were non-Hispanic/Latino, 47% were married, 38% lived alone, and 71% lived in urban areas (Table 2). Compared to those who had no care coordination, those who did receive care coordination had a higher Elixhauser readmission score (29.9, SD = 20.4 versus 37.1, SD = 24.7; SMD = 0.31), and more VHA visits in FY21 (25.5, SD = 16.1 versus 39.5, SD = 28.0; SMD = 0.62). Compared to nonrespondents, respondents included a higher percentage of older, male, White, and married Veterans (Table 2).
Characteristics of Survey Respondents.
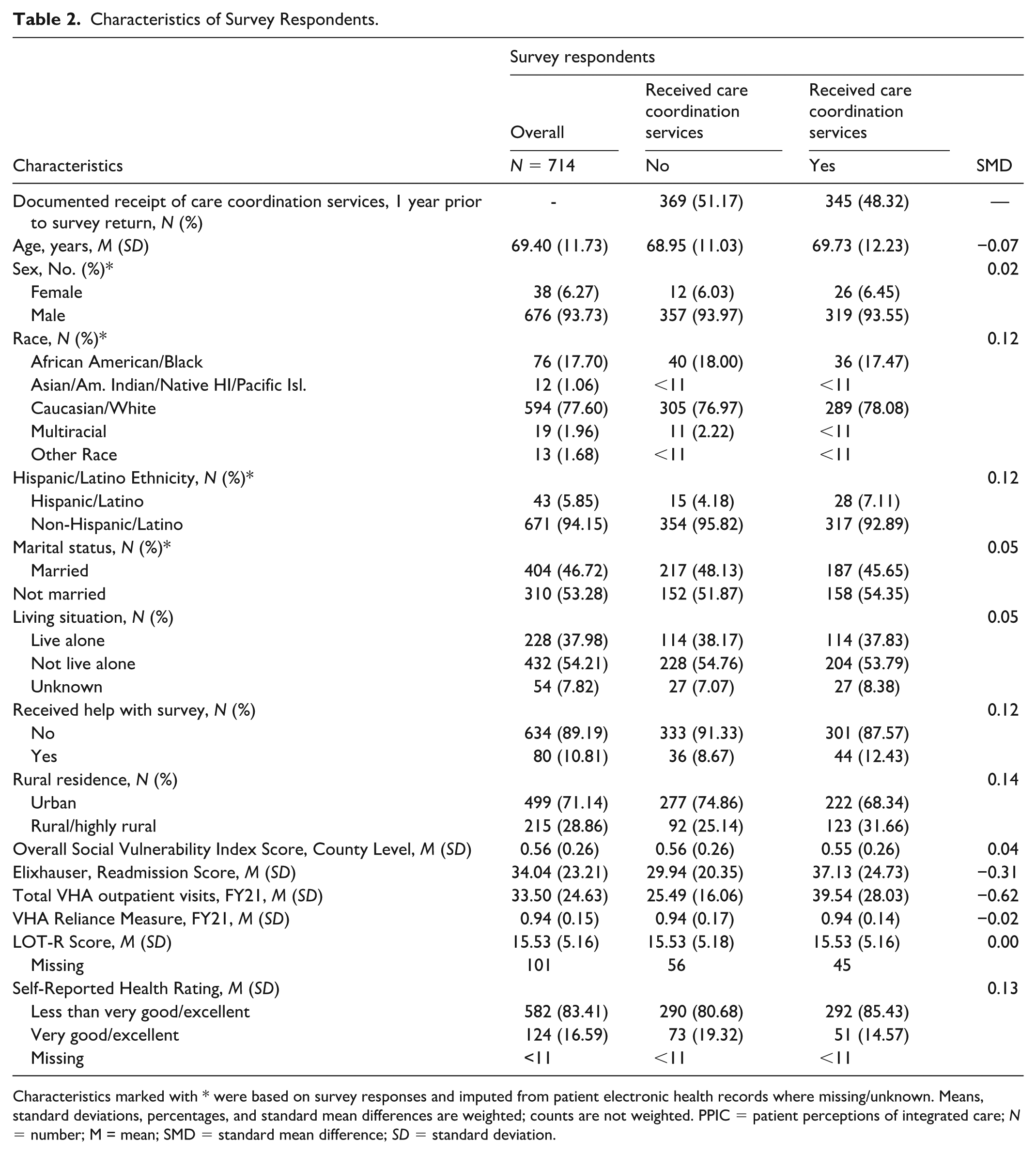
Characteristics marked with * were based on survey responses and imputed from patient electronic health records where missing/unknown. Means, standard deviations, percentages, and standard mean differences are weighted; counts are not weighted. PPIC = patient perceptions of integrated care; N = number; M = mean; SMD = standard mean difference; SD = standard deviation.
For the six PPIC outcome measures, overall mean dimension scores were highest for staff knowledge about the patient (mean 3.30; SD = 0.70), indicating relatively higher perceived integration than other domains and lowest for provider support for medication adherence and home health (mean 2.57; SD = 1.00) and test result communication (mean 2.74; SD = 0.49; Table 3). Most respondents (66.47%) reported definitely or somewhat yes that specialists had knowledge about the patient. In unadjusted analyses comparing scores between those with and without care coordination services, mean dimension scores for all factors were similar. Those with care coordination compared to those without care coordination had lower albeit statistically similar mean scores for provider knowledge (mean: 3.12 versus 3.19; difference 0.06, 95% CI: -0.04, 0.17); staff knowledge (mean: 3.28 versus 3.32; difference 0.05; 95% CI: -0.12, 0.21); support for self-directed care (mean: 2.88 versus 2.97; difference: 0.09; 95% CI: -0.08, 0.25); medication adherence (mean: 2.52 versus 2.63; difference: 0.11; 95% CI: -0.07, 0.28); and test result communication (mean: 2.72 versus 2.76; difference: 0.04; 95% CI: -0.04, 0.13).
Weighted Comparison of Unadjusted Patient Perceptions of Integrated Care (PPIC) Survey Dimension Scores Between VHA Patients With Versus Without Documented Care Coordination Services.
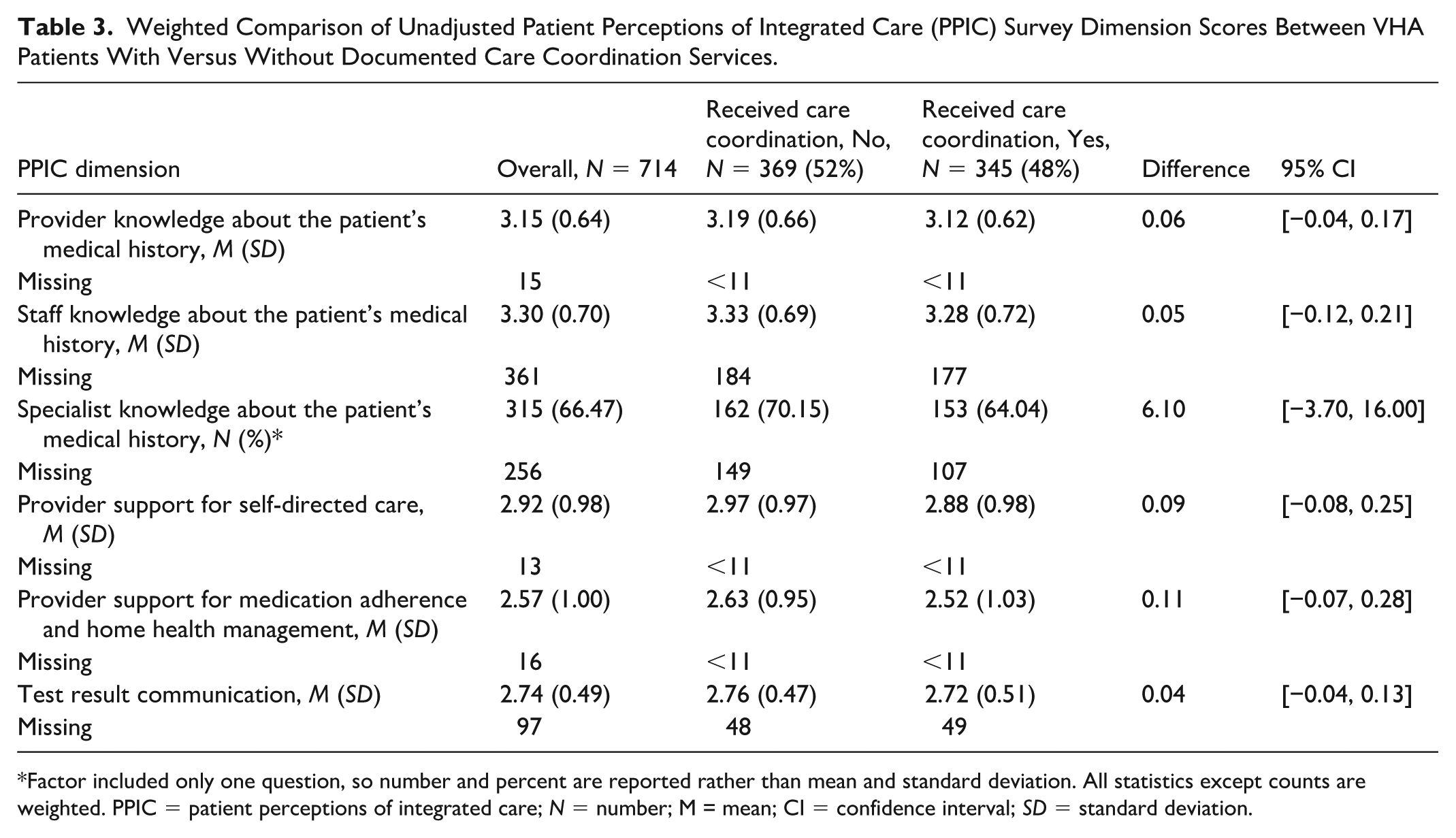
Factor included only one question, so number and percent are reported rather than mean and standard deviation. All statistics except counts are weighted. PPIC = patient perceptions of integrated care; N = number; M = mean; CI = confidence interval; SD = standard deviation.
In regression analyses (Table 4), we found that those with care coordination had lower mean provider support for adherence to medications and home health management scores (Coefficient -0.20; 95% CI: -0.37, -0.02). For the other PPIC dimensions, the differences were not statistically significant at the α = 0.05 level: provider knowledge about the patient’s medical history (Coefficient -0.06; 95% CI: -0.17, 0.06); staff knowledge about the patient’s medical history (Coefficient -0.08; 95% CI: -0.25, 0.09); specialist knowledge about the patient’s medical history (OR = 0.79; 95% CI: 0.49, 1.28); provider support for self-directed care (Coefficient -0.13; 95% CI: -0.30, 0.04); and test result communication (Coefficient -0.07; 95% CI: -0.17, 0.02).
Regression Models Comparing VHA Patients With Versus Without Documented Care Coordination Services.
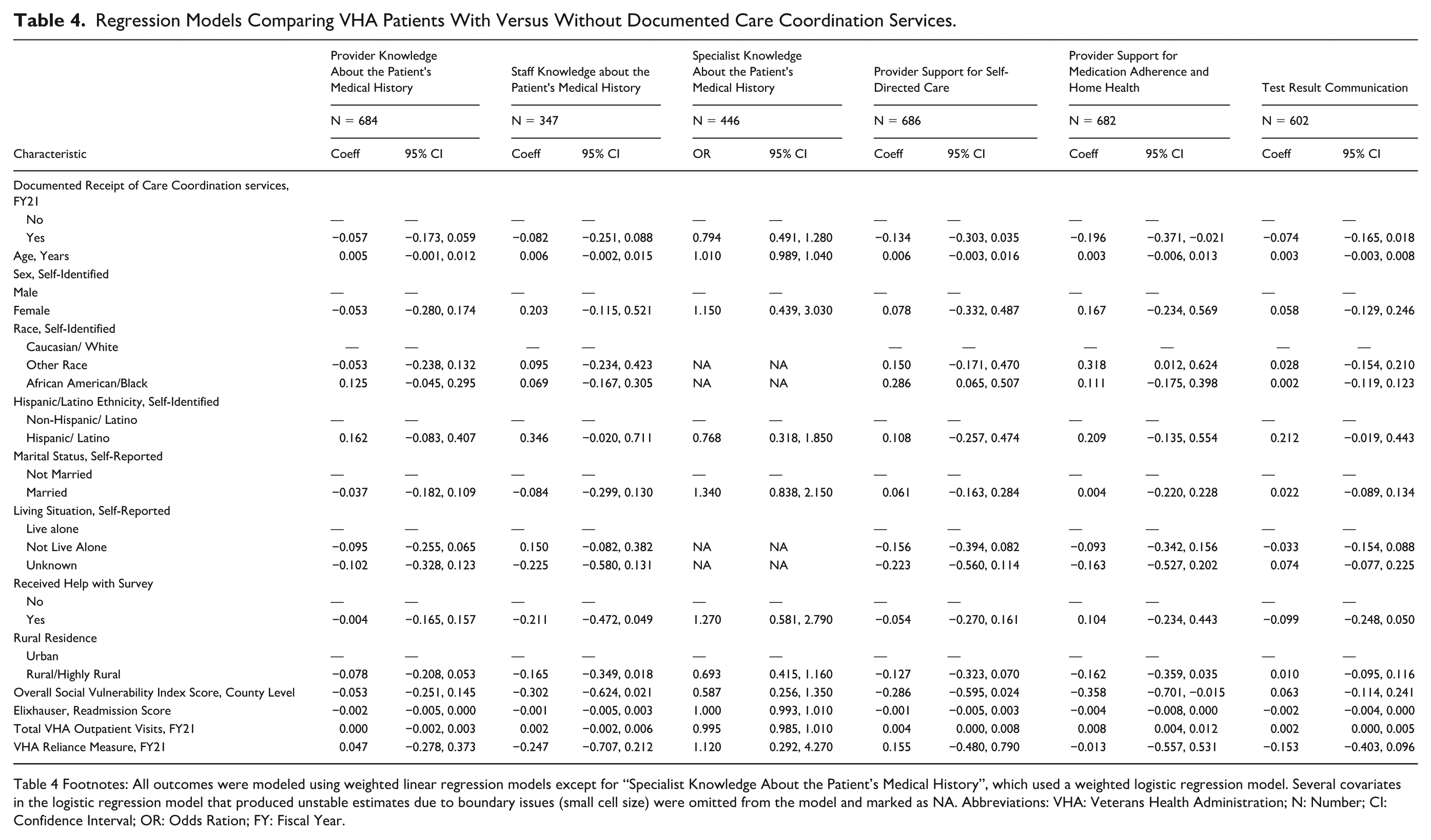
Table 4 Footnotes: All outcomes were modeled using weighted linear regression models except for “Specialist Knowledge About the Patient’s Medical History”, which used a weighted logistic regression model. Several covariates in the logistic regression model that produced unstable estimates due to boundary issues (small cell size) were omitted from the model and marked as NA. Abbreviations: VHA: Veterans Health Administration; N: Number; CI: Confidence Interval; OR: Odds Ration; FY: Fiscal Year.
Considering other patient characteristics and their associations with the PPIC dimensions, results were mixed (see Table 4). For provider knowledge about the patient’s medical history, scores increased with age (Coefficient 0.01; 95% CI: 0.00, 0.01). For the perceptions about staff knowledge of the patient’s medical history, those identifying as Hispanic/Latino had higher, though not statistically significant, scores than those of non-Hispanic/Latino ethnicity (Coefficient 0.35; 95% CI: -0.02, 0.71). And regarding specialist knowledge of patient’s medical history, there were no significant associations. There were no other significant differences among the knowledge dimensions (see Table 4).
Regarding provider support domains, for provider support for self-directed care, those identifying as African American/Black race had higher scores compared to those identifying as White (Coefficient 0.29; 95% CI: 0.06, 0.51). For provider support for medication adherence and home care, higher scores were observed for those identifying as other race (Coefficient 0.32; 95% CI: 0.01, 0.62) and those with higher total VHA use in FY21 (Coefficient 0.01; 95% CI: 0.00, 0.01), whereas those living in an area with high SVI had lower scores (Coefficient -0.36; 95% CI: -0.70, -0.02) as well as those who received care coordination (Coefficient -0.20; 95% CI: -0.37, -0.02).
Regarding communication about test results, those with higher total VHA use in FY21 had higher scores (Coefficient 0.002; 95% CI: 0.000, 0.005). There were no other significant associations.
Sensitivity analyses using LOT-R, selected survey questions, and health covariates (Supplemental Table 3), and with revised care coordination groups were similar to the primary results (Supplemental Tables 4, 5).
Discussion
In this study, we surveyed Veterans with high risk of hospitalization or mortality who were engaged in care at one of the 31 VHA facilities that were early adopters of the CCICM practice framework. We found that receipt of care coordination had little association with PPIC dimensions. These results suggest that the delivery of care coordination services in the context of the early implementation of a national care coordination practice framework did not improve patients’ perceptions of care integration. Although organizational and practice changes were underway, it is likely that it may have been too early in the implementation for patients to observe changes in care integration. It may also be that receipt of care coordination services alone may not be sufficient to influence such patient perceptions. Care coordination services may cover a wide range of activities that depend upon patient’s clinical and social needs at the time. Future research should explore whether patient perceptions of care integration improved after full deployment of this organizational change, including among a broad range of patients with different conditions and social needs.
Overall, respondents’ mean PPIC scores were relatively high (greater than 3 on a scale of 1 to 4) for two dimensions related to knowledge about patient medical history among staff and primary providers. In addition, PPIC scores were highest for staff knowledge about the patient, although ratings were similar for those who did and did not receive care coordination services. By virtue of their self-selection as early adopter sites in the first phase of the CCICM implementation, it is possible that sites may have already been providing highly integrated care beforehand or were better positioned to do so for these dimensions. On the other hand, mean PPIC scores were relatively low for provider support for self-directed care, provider support for medication adherence and home care, and test result communication. Even for early adopter sites, achieving higher patient perception scores for these dimensions may require deeper engagement with patients.
Our results differ from prior research assessing perceived care integration among VHA-enrolled Veterans with diabetes and using an earlier 8-dimensional PPIC version administered in 2016 (Benzer et al., 2019, 2020). Our cohort had higher ratings for staff knowledge about the patient (mean 3.30; SD = 0.70 versus 3.02; SD = 0.91) and lower ratings for provider support for patient self-directed care (mean 2.92; SD = 0.98 versus 3.00; SD = 0.85) and test result communication (mean 2.74; SD = 0.49 versus 3.38; SD = 0.79). These differences may be due to study design—disease-specific versus a general chronic disease population in our study, and emphasis of diabetes education that prioritizes specific aspects of self-care. In sensitivity analyses adjusting for the presence of diabetes, we saw no differences from our main results. Other factors that may contribute to these differences include study time frame, transformations in care delivery overall, the pandemic, growth in virtual care, and expansion of VHA community care. Notably, our lower ratings for test result communication align with a 2021 survey of Veterans who favored VHA-purchased care over VHA facility care, and rated communication and other experiences less favorably than those who favored VHA facility care (Slatore et al., 2024).
Our results indicating no significant associations between comorbidities and perceptions of integrated care among Veterans at high risk of hospitalization also appear to differ from prior research. However, specific measures used are not the same (Benzer et al., 2019, 2020; Kerrissey et al., 2017). Furthermore, compared to these prior studies, our cohort was older (mean age 72; SD = 10.84 versus 68; SD = 13.47), comprised a broader population, and had higher comorbidity levels (mean Elixhauser 34.25; SD = 23.76). Our findings suggest that there may be heterogeneity among Veterans in our study and that the care coordination services offered may not be distinguishable from usual care processes for patients. On the one hand, such standardization of practices does not appear to have been disruptive to care, based on the relatively high dimension scores. However, if improvement in patient perceptions of care integration is one of the goals of implementation of a new practice framework for care coordination, or care coordination more broadly, monitoring followed by responsive adaptations may be needed. Future research should consider if there are additional dimensions that are specific to care transitions and progression of multiple chronic conditions to optimize adaptations.
Among dimension ratings that were the lowest, there may be ways to improve. For example, to improve test result communication, Lead Coordinators might facilitate communication by alerting the relevant primary care provider and/or discussing with patients about their questions. Regarding potential improvement for provider support for self-care, perhaps the heterogeneity of patient needs requires a more tailored approach that considers time-varying functional and clinical aspects. Further, as CCICM early implementation has been primarily focused on the roles of nurses and social workers, consideration of expanded engagement with primary care physicians and PACT teams, as well as health care personnel who support VA community care, will also be important for ensuring effective communication and confidence in the team member roles.
It is also important to recognize that care coordination is not straightforward to capture in current data systems or to distinguish patients who did or did not receive it. Both within and external to VHA, care coordination may not be adequately captured. In the VHA, documenting care coordination through care management/transition services using CPT codes has been variably implemented, and there are no reimbursement or workload incentives to do so. In the private sector, care management/transition services are reimbursable, although there have been reports that the burdens of staffing and coding outweigh the work to deliver the service (Gardner et al., 2018). In both the VHA and in the private sector, care teams are increasingly multidisciplinary with dynamic roles, and documentation can be burdensome and siloed (Keenan et al., 2013). Therefore, better documentation, data capture, and understanding about how a team works and manages care are needed to know how to improve specific care elements. In our survey, it might have been helpful to specifically identify the role of the Lead Coordinator assigned to the patient and to include items to address communication and actions attributable to the Lead Coordinators’ support for patient care plans. Future versions of the PPIC might consider such modifications to address specific care elements. Future research should also address efficient methods to capture team dynamics, tasks, and their impacts on patients to inform practice enhancements that may be needed; process mapping may be one way to do so (Kerrissey et al., 2017, 2023; Singer, Kerrissey, et al., 2020).
There are limitations to this study. As a cross-sectional study, our results describe associations, not causal effects. We measured care coordination as a single service, which may or may not be sensitive enough for patients to perceive its effects. Additional qualitative research to understand why care coordination services may not be associated with patient perceptions of integrated care, and whether perspectives of providers, staff, or other care partners should be considered. More in-depth investigations to identify potential bright spots and reveal how success was attained may inform adaptations to ongoing and future interventions. Our study population included patients at high risk of hospitalization or mortality, and although we used methods to account for potential selection for receiving care coordination services, residual bias may exist. We focused on early adopter sites; therefore, results from our study might not apply to other VHA sites, which might have different patient population needs and staffing than the selected sites. Also, our response rate was somewhat low and while we accounted for nonresponse and adjusted for patient and facility characteristics, there may be potential confounding due to unmeasured factors that could be correlated with responding and with the PPIC responses. Furthermore, it is also possible that the degree to which care coordination services addressed care integration was limited during the early implementation phase of the CCICM. Finally, our results may not generalize beyond Veterans who receive care in the VHA.
Conclusion
Veterans’ perceptions about care integration did not correspond as hypothesized with receipt of care coordination services. Although results were similar for those with or without documented receipt of care coordination services, lower perceived integration regarding support for self-care and communications overall suggests specific dimensions to prioritize for improvement and with engagement among patients and across providers. As the implementation of VHA’s care coordination initiative progresses, assessment of patients’ perceptions should be conducted to monitor impacts and to identify opportunities for continued improvement. Efforts to improve consistent documentation of care coordination services are needed to identify potential gaps in care. Future research that interrogates the fit between patient needs and preferences for specific care coordination services may also inform practice enhancements.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587251413444 – Supplemental material for Patient Perspectives of Care Integration During Early Implementation of a Care Coordination Initiative
Supplemental material, sj-docx-1-mcr-10.1177_10775587251413444 for Patient Perspectives of Care Integration During Early Implementation of a Care Coordination Initiative by Denise M. Hynes, Alex Hickok, Holly McCready, Meike Niederhausen, Mazhgan Rowneki, Diana J. Govier, Sara J. Singer, Kristina M. Cordasco, Christopher G. Slatore, Matthew L. Maciejewski, Kathryn McDonald, Lisa Perla and Abby Moss in Medical Care Research and Review
Footnotes
Acknowledgements
The US Department of Veterans Affairs was not involved in the study design; collection, analysis, or interpretation of data; writing the manuscript; or the decision to submit the manuscript for publication. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the US Department of Veterans Affairs of the United States government. We appreciate the initial planning for this survey by Rebecca Young, Derek Nelson, and Avery Laliberte.
Consent to Participate
This project was reviewed and approved by the joint Oregon Health & Sciences University/VA Institutional Review Board and the Research & Development Committee of the Portland VA Healthcare System. Documentation of informed consent was waived, and all participants received an information sheet along with their mailed survey.
Consent for Publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the US Department of Veterans Affairs (VA) Health System Research (HSR) award (IIR 20-165) and for use of the VA-linked Medicare data (SDR 02-237; SDR 98-004). Drs. Hynes and Maciejewski were supported in part by VA Research Career Scientist Awards (RCS 21-136, RCS 10-391). Dr. Slatore was supported by resources from the VA Portland Health Care System and the National Center for Lung Cancer Screening. Dr. Govier was supported in part by a VA Office of Rural Health Career Development Award (VRHRC-IC 04246).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to Department of Veterans Affairs data restrictions prohibiting sharing. Contact the corresponding author, Denise M. Hynes, for data requests.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.