
Abstract
Improving access to midwifery care has been identified as a strategy to address shortages of reproductive health clinicians and ensure person-centered, equitable care. This article describes findings from a new survey of licensed midwives (LMs) in California, who enter the profession without a nursing background. The data offer new insights into LMs’ demographics, training, client population, and practice experiences. LMs predominantly have their own practices, typically working with another midwife and/or an assistant or student, and have relatively small numbers of clients each year. Most of the births they attend occur in homes and birth centers. Many LMs report a lack of understanding of and support for their expertise by physicians and hospitals. Despite these challenges, most LMs are satisfied with their careers. LMs contribute to person-centered care, offering alternatives to hospital birth and expanding access to the midwifery model of care.
Introduction
In the United States, there is increasing interest from patients, community advocates, and policymakers in improving access to midwifery care to both address shortages of reproductive health clinicians and reduce inequities in birth outcomes by expanding options for holistic person-centered care (White House, 2022; Zephyrin et al., 2021). Midwifery recognizes pregnancy and childbearing as natural physiological processes that take place in a variety of settings, including clinics, birth centers, homes, and hospitals. The midwifery model of care considers the pregnant person as an active partner in care and strives to ensure that monitoring for the risk of complications does not preempt other important aspects of the pregnancy and birth experience (Rooks, 1999). Midwifery care is distinct from medical care; however, midwives often work in collaboration with and regularly consult with physicians, and they transfer patients to physician care when the need arises.
Midwives are common providers for prenatal and birth care in many countries, including most European countries, Canada, and Australia (Shaw et al., 2016). It is well-established that midwifery care is associated with lower rates of unnecessary medical interventions (e.g., labor induction, episiotomy, cesarean birth), higher rates of vaginal birth and breastfeeding, lower health care costs, and lower rates of maternal and neonatal mortality and morbidity (Altman et al., 2017; Attanasio & Kozhimannel, 2017; Renfrew et al., 2014; Sandall et al., 2024; ten Hoope-Bender et al., 2014). Moreover, midwifery-based birth center care for low-risk birth has been associated with lower rates of intervention, low birth weight, neonatal intensive care unit admission, and neonatal death, and higher rates of breastfeeding (National Academies of Sciences, Engineering, and Medicine, 2020; Wallace et al., 2024). Midwives can play a role in reducing racism-based health disparities through community-based models that provide respectful and culturally congruent care (Karbeah et al., 2022; Liese et al., 2022; Welch et al., 2022).
In the United States, there are three credentials for midwifery practice. Nurse-midwifery certification (“CNM”) became available from the American College of Nurse-Midwives in 1971, after being introduced to the United States in the early 1910s (Varney & Thompson, 2016). Interest in expanding and formalizing the field of direct-entry midwifery, without nurse licensure, led to the establishment of the Certified Midwife (CM) credential by the American College of Nurse-Midwives in 1994 and the Certified Professional Midwife (CPM) credential by the North American Registry of Midwives (NARM) in 1995. CM training and examination requirements largely mirror those of certified nurse-midwives, with programs offering graduate degrees, providing didactic instruction aligned with national standards, and providing clinical experiences through direct patient care and simulation. CPM education is achieved primarily through one of two routes: 3-year postsecondary education at an accredited program or apprenticeship with documented knowledge and skills verification by qualified midwives. CPMs’ clinical experience is supervised by a NARM Registered Preceptor and usually occurs in a birth center or home birth practice. All CPMs must successfully complete the national certification examination administered by NARM (Marzalik et al., 2018). In 2023, it was reported that there were 13,868 CNMs, 130 CMs, and 2,699 CPMs with active certification in the United States (AMCB, 2023; NARM, 2023).
As with other health professions, states regulate the practice of midwives. All states recognize and license nurse-midwives but there is variation in the licensure of CMs and CPMs (Jefferson et al., 2021): CMs are recognized in 12 states and CPMs have legal recognition in 38 states (ACNM, 2024; FeelingPushy.org, 2024). In California, only the CPM credential is recognized for direct-entry midwives, who are licensed as “licensed midwives” (LMs) and regulated by the Medical Board of California. Candidates for licensure must graduate from an accredited education program approved by the Medical Board and pass the certification examination offered by NARM. Alternatively, potential LMs who completed their midwifery education or previously worked as midwives outside of California can attain licensure by providing documentation that they have substantial midwifery clinical experience and education prior to coming to California, taking a challenge exam at a board-approved institution, and passing the NARM exam. In 2013, revised regulations gave LMs the freedom to practice without physician supervision.
While the number of nurse-midwives was stable in California between 2017 and 2023, the number of LMs increased 22% from 376 in 2017 to 458 in 2023. Between 2007 and 2017, the number of births attended by LMs in California increased from 929 to 2,908; in 2017, LMs attended 0.6% of births, with 21% of these occurring in freestanding birth centers and 74% occurring in residences (Kwong et al., 2019). Similar trends toward increased midwife-attended and community-based births have been reported nationally (MacDorman et al., 2022).
New Contribution
Rising interest in midwifery as a key strategy for reducing disparities in access to and quality of birth care in California led to the development of a survey by our research team of direct-entry midwives in the state. California’s large, heterogeneous population provided the opportunity to explore both the characteristics of the LM workforce and the diversity of the people for whom they provide care (called “clients” by CPMs). The American College of Nurse-Midwives has conducted several surveys of the CNM and CM workforce, most recently in 2020 (Thumm et al., 2023), but the last national survey of CPMs was conducted by NARM in 2011 (Cheyney et al., 2015). No survey had ever been fielded specifically to California LMs. This article describes the survey’s findings, offering new insights into the direct-entry midwifery workforce. We contribute to the literature by describing the demographic characteristics of LMs, their training, career intentions, job satisfaction, and burnout, as well as providing insights into their clients and practice settings.
Method
Results reported in this article were derived from the California Survey of Licensed Midwives, which was conducted by the authors and fielded from July 2022 through March 2023, supported by a grant from the California Health Care Foundation. The overarching study purpose was to understand the LM workforce in California, its contributions to improving access to care, and challenges faced by LMs that could be addressed through policy change. The survey questionnaire was based on prior surveys conducted of nurse-midwives in California and the 2011 NARM survey of CPMs. The questionnaire development was guided by an Advisory Committee, which included California-based midwifery leaders. The survey questionnaire included items about education and training in general and in midwifery, practice characteristics such as services offered and number of patients served, collaboration with other health professionals, experiences and relationships with hospitals, client population characteristics, precepting of students, satisfaction with numerous aspects of practice, employment intentions, and demographics. LMs were asked a series of questions to ascertain the extent to which they were experiencing burnout, which was measured using the nine-item Emotional Exhaustion and five-item Depersonalization subscales of the Maslach Burnout Inventory Human Services Survey (Maslach & Jackson, 1981). The draft questionnaire was cognitively tested with five LM volunteers, after which a pen-and-paper instrument and an online questionnaire were finalized. The specific questions used in this analysis are provided in the Appendix.
A list of all LMs was obtained from the Medical Board of California website, which included 437 people who had addresses in California. This list provided LMs’ mailing addresses and was matched with a roster of members of the California Association of Licensed Midwives, which included both mailing address and email address. The online version of the survey was sent to the 287 matching LMs using their email address, with three reminder emails. After the initial email fielding, the pen-and-paper instrument was sent via the U.S. Postal Service to nonrespondents and the remaining 150 LMs for whom we had only a mailing address. The paper mailings included the survey questionnaire, a postage-paid return envelope, and a link to the online survey. Three reminder postcards and one re-mailing of the full survey packet were used to increase response rates.
There were 229 usable responses for the LM survey, of which 179 were completed online and 50 were completed on paper. A total of 31 cases were classified as ineligible because the LM was unreachable at the address on record, resulting in an eligible population of 406 LMs and a 56.4% response rate for the eligible population. The pen-and-paper instrument responses were entered into a database and merged with the online responses. Post-stratification weights were developed to address differential response rates across nine regions of the state to ensure that analyses reflected the statewide population of licensed LMs. A public-use version of the dataset is available from the authors upon request.
The data were analyzed using descriptive statistics such as frequencies, tabulations, and cross-tabulations, and we assessed statistical differences among subgroups with t-tests for continuous variables and chi-square tests for categorical measures. Variables used for the analysis presented in this article were selected to provide insights into demographic characteristics of the LM workforce, their practice characteristics, the clients they serve, their job satisfaction, and burnout. Burnout was defined by a cut-off of ≥27 on the emotional exhaustion and ≥10 on the depersonalization scale (West et al., 2009). Stata MP 15.1 was used to prepare and analyze the data.
Results
Demographic Characteristics of Licensed Midwives
The mean age of California’s LM workforce was 49.5 years. Among LMs practicing as midwives, 46.2% were below 45 years and 26.2% were 55 years or older; among LMs not practicing, 20.8% were below 45 years and 49.8% were 55 or older (all statistics are available in a table in the Appendix). Overall, 76.5% of LMs identified as White, 12.2% as Latinx/Hispanic, 2.8% as Asian or Pacific Islander, 1.8% as Black/African American, and 6.6% as of mixed racial-ethnic identity. As seen in Figure 1, younger LMs more often identified as having a racial or ethnic background other than White (p < .01), with 16.1% of LMs aged 55 to 64 years and 26.2% aged below 35 years identifying as Black/African American, Latinx/Hispanic, Asian/Pacific Islander, Mixed, or another non-White identity.
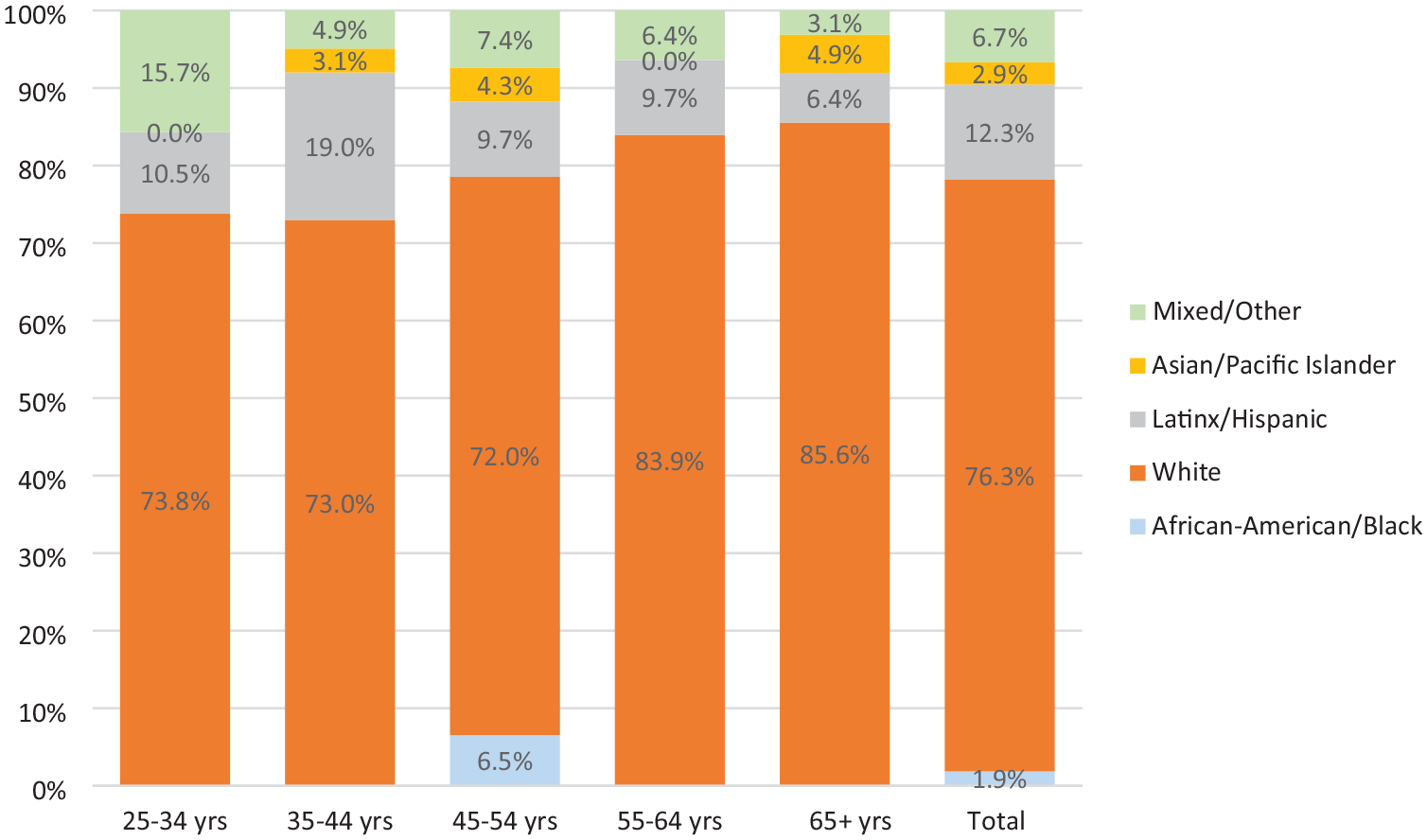
Race-Ethnicity of California Licensed Midwives, by Age Group.
Education Completed by Licensed Midwives
More than two thirds of LMs (67.3%) completed an education program approved by the Medical Board of California, 30.5% were qualified by documenting completion of training equivalent or greater than required for Medical Board approval, and 2.2% had California licenses granted based on licensure in another state. The average duration of LM training was 4.2 years, and the average age at completion of LM education was 37.4 years. Many LMs reported that they completed other postsecondary education in addition to their LM education: 49.4% reported that their highest education was a bachelor’s degree, and 12.9% reported that they held a master’s or doctoral degree.
Employment of Licensed Midwives
At the time of the survey, 78.6% of LMs reported that they were practicing midwifery, equating to an estimated 344 LMs practicing in California. Greater percentages reported they had practiced at some point in the past year (82.6%) and past 3 years (88.7%). Among those practicing midwifery, 21.1% indicated they also were employed outside a midwifery role. Among those who were not practicing midwifery, 54.2% were employed in another type of job.
Most LMs own their midwifery practice. As seen in Figure 2, 49.1% of practicing LMs reported their practice was a sole proprietorship. Another 5.8% operated a partnership and 23.8% operated some type of corporation. Relatively few were employees of an organization, with only 8.5% reporting they were regular employees and 7.5% were contract employees for their midwifery practice.
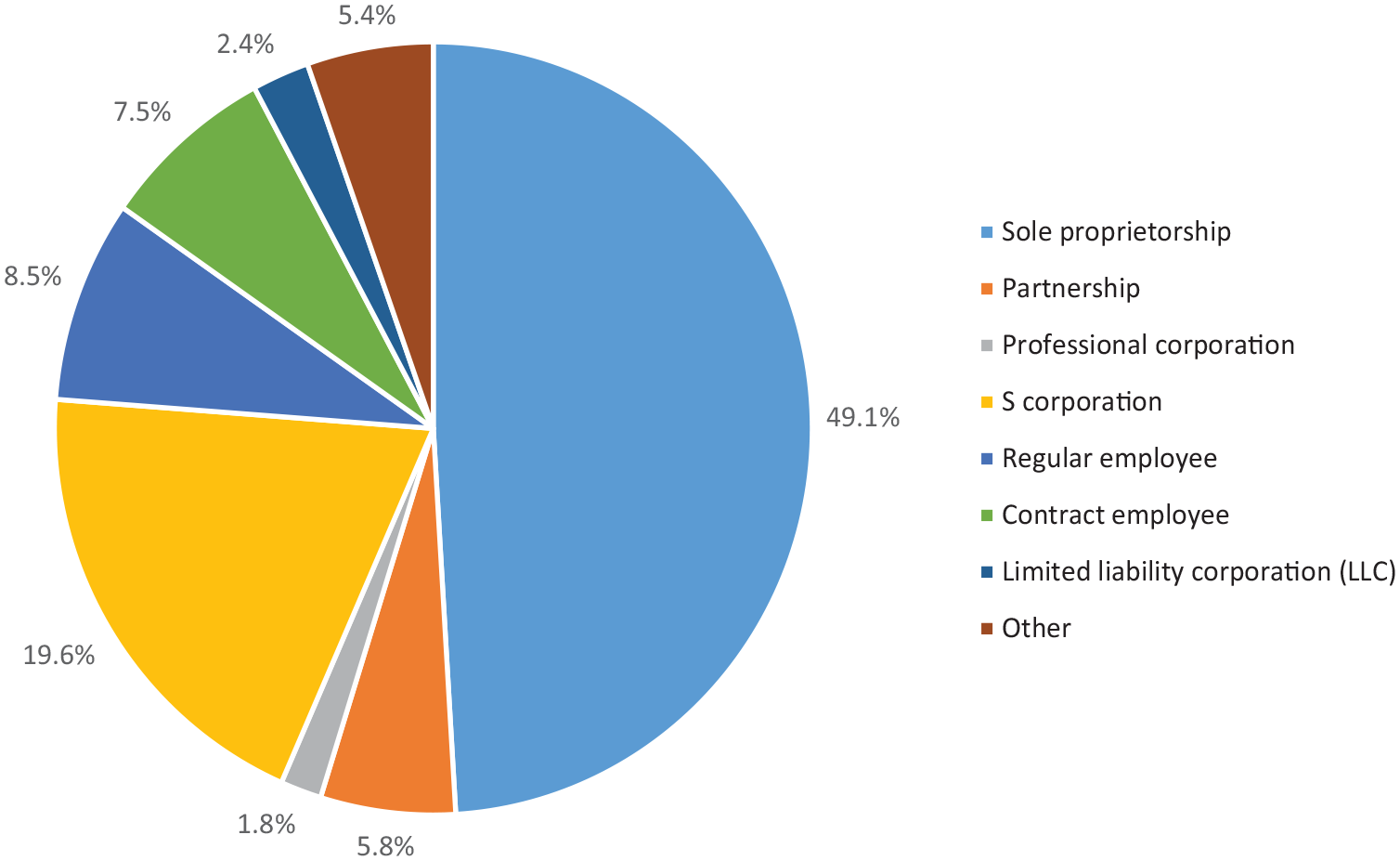
Licensed Midwife Employment and Practice Ownership.
Many LMs reported that they worked with other health professionals in their practice. Nearly two thirds (65.9%) worked with another LM and 11.3% worked with a nurse-midwife. Many worked with a midwife assistant (36.7%) or midwife student (46.6%), and some worked with a doula (8.3%). Only 12.8% reported that they worked alone in their midwifery practice.
Clients Served by Licensed Midwives
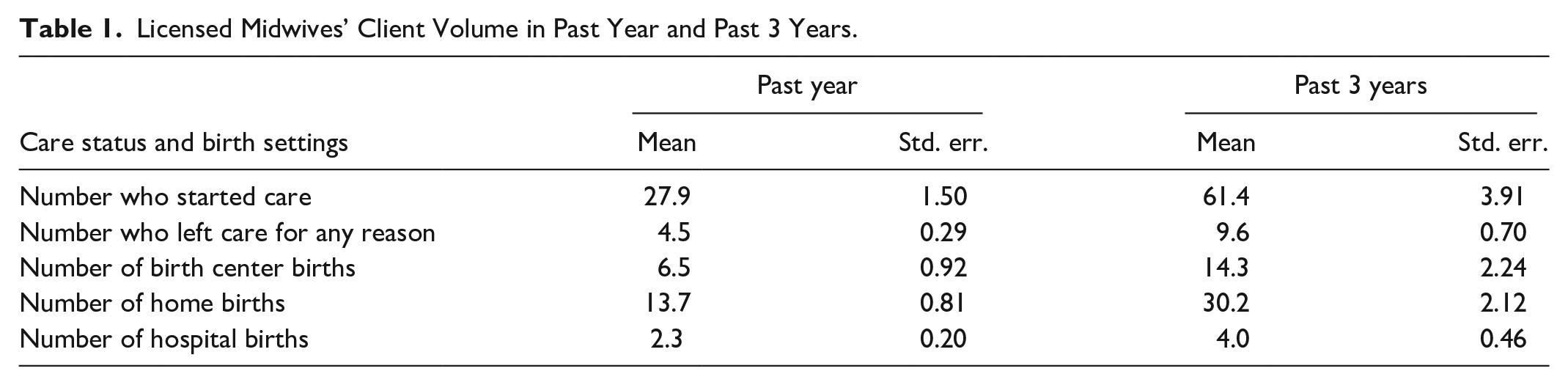
LMs were asked a series of questions about their client volume over the prior year and the prior 3 years. They reported an average of 27.9 clients who started care in the prior year and 61.4 clients over the prior 3 years, inclusive of clients for whom the LM attended birth, those whose pregnancies ended without birth (e.g., miscarriage), and those who transferred to another clinician (Table 1). Participants reported that an average of 4.5 clients left their care in the past year because the client had a higher risk profile than within LM scope of practice or for another reason. Births at home were the most numerous among LMs’ clients, on average, with 13.7 in the past year and 30.2 in the past 3 years. These were followed by birth centers, with an average of 6.5 in the past year and 14.3 in the past 3 years. Half of LMs indicated that at least one of their clients had given birth in a hospital, with a statewide average of 2.3 patients giving birth in a hospital in the past year.
Licensed Midwives’ Client Volume in Past Year and Past 3 Years.
The survey questionnaire asked LMs to estimate the racial-ethnic distribution of their clients. Figure 3 presents the averages of their estimates for each group, as well as the racial-ethnic distribution of mothers giving birth in California in 2023 (CDC Wonder, 2025). LMs reported that Black clients averaged 10.4% of their patients, which is notably greater than the statewide percentage of 4.9% of birthing mothers being Black. LMs’ clients were also more often White than birthing mothers in California (57.0% vs. 28.2%). A much smaller percentage of LMs’ clients were reported to be Latina/x compared with the state’s birthing women (17.4% vs. 48.7%); this was also true of Asian/Native Hawaiian/Pacific Islander women (6.8% vs. 15.4%).
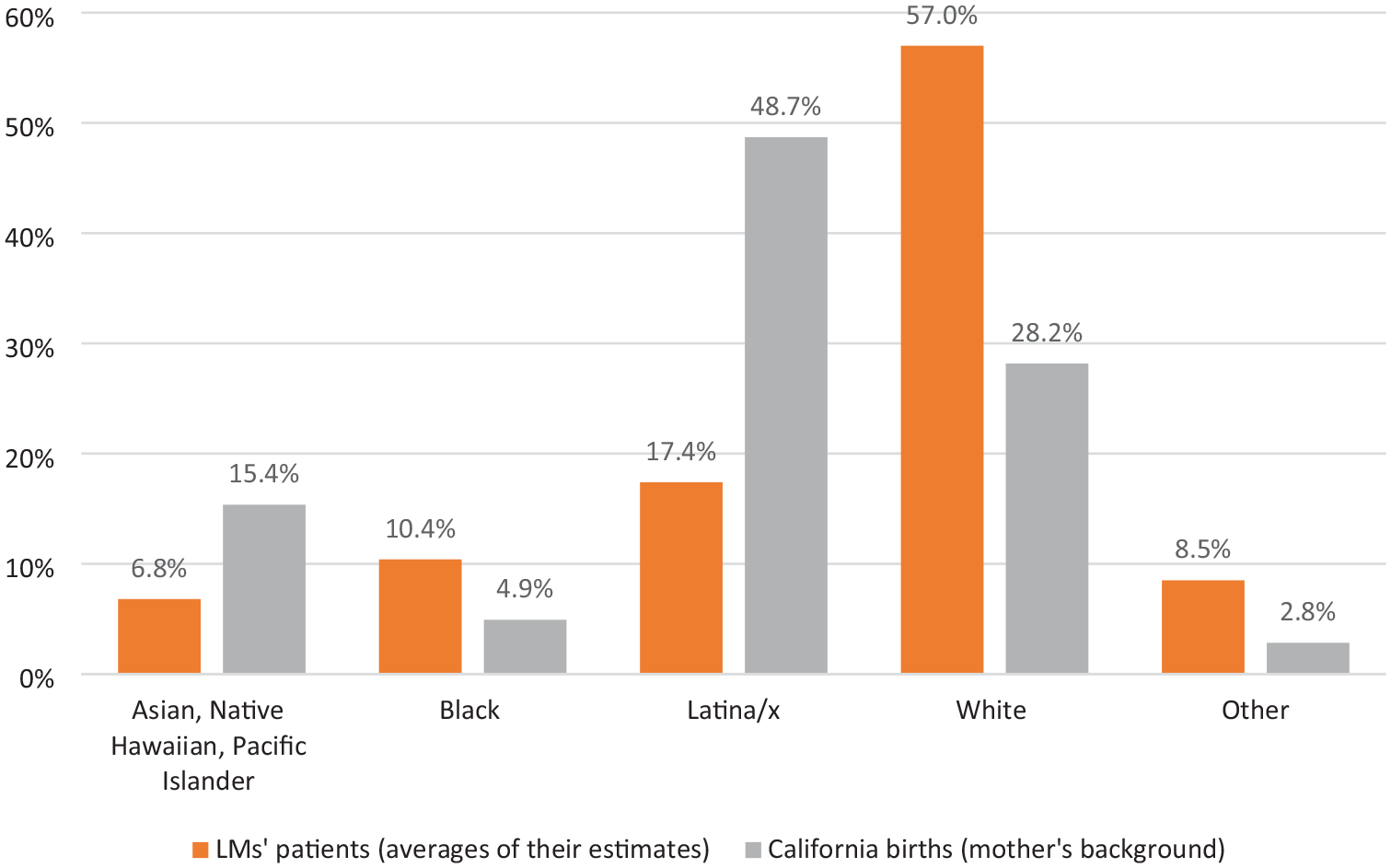
Race-Ethnicity of Licensed Midwives’ Patients and Mothers Giving Birth in California in 2023.
LMs estimated that an average of 54.2% of their clients were self-paying and an average of 32.9% would pay or be reimbursed by commercial insurance (Figure 4). Only 15.1% of LMs reported that they accepted Medicaid payments (not shown), and they estimated an average of 8.3% of their clients were insured by Medicaid. Among LMs who did not accept Medicaid, the most frequently cited reasons were that payment is not high enough to recoup the costs of providing care (69.6%), they do not want to deal with the bureaucratic process of becoming authorized (43.2%), and they do not have malpractice insurance (34.2%). Nearly two thirds of LMs reported they do not have malpractice insurance (65.0%), with the main reasons being that the cost is too high (83.1%), there is a lack of policies that offer coverage to LMs (48.0%), and a lack of administrative support to research and maintain malpractice insurance (27.1%). Some LMs reported that they are philosophically opposed to malpractice insurance (11.2%) and that they are willing to take the risk of a malpractice lawsuit (8.6%).
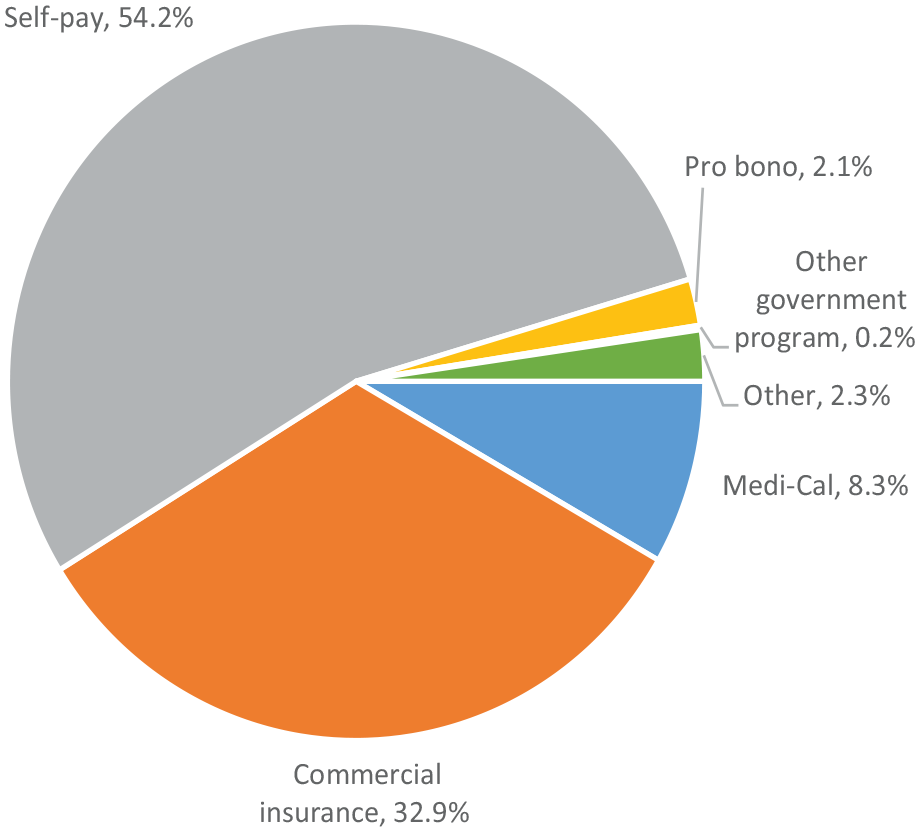
Insurance Coverage of Licensed Midwives’ Patients.
Relationships With Physicians and Hospitals
Approximately half of LMs reported that they did not have a physician with whom they provided collaborative care for their clients (51.1%). This is associated with their perceptions of the lack of support for midwifery by physicians. Only 26.2% of LMs somewhat, mostly, or strongly agreed that local physicians understand the midwifery model of care, and only 14.5% agreed that local physicians advocate for the midwifery model of care. Two thirds of LMs reported they had experienced unprofessional or hostile behavior from a physician at least one time in the past 3 years and, among those who had any such experiences, there was an average of 6.8 incidents.
Given these poor relationships with physicians, it is not surprising that LMs also perceive that many hospitals are not supportive of their practice. More than two thirds reported they had bypassed the nearest hospital in the past 3 years (67.8%). The most commonly reported reasons for bypassing a hospital were that the nearest hospital was hostile to midwifery care (72.8%) and client preference (54.2%).
Career Satisfaction and Burnout
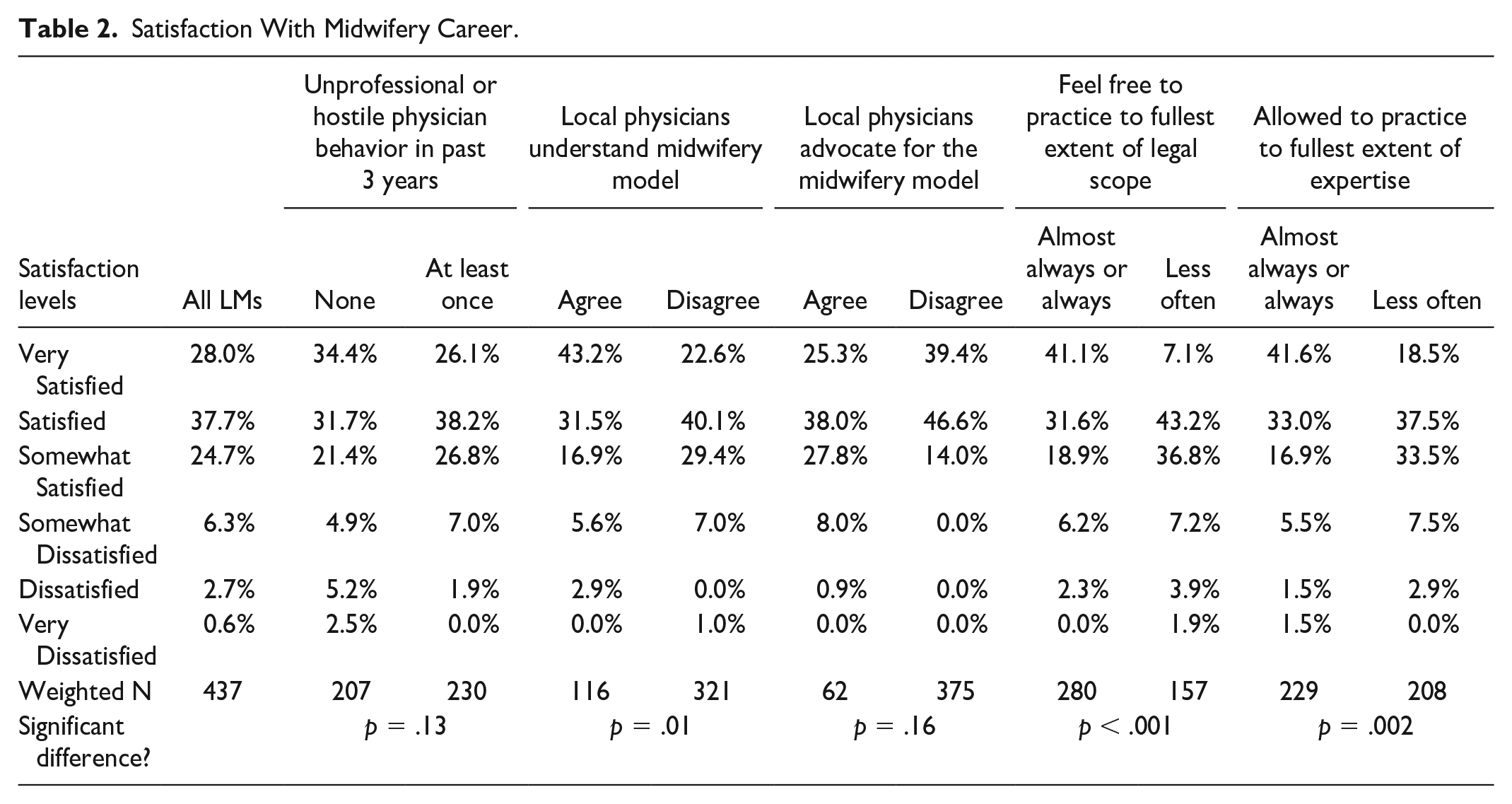
The vast majority of LMs indicated that they are satisfied with their midwifery career, as seen in Table 2. Among all LMs, 90.4% are at least somewhat satisfied with their career, and 28.0% are very satisfied. There was not a statistically significant difference in career satisfaction between LMs who had versus had not experienced at least one unprofessional or hostile physician behavior in the previous 3 years (p = .13). There also was not a statistically significant difference between LMs who agreed versus disagreed that local physicians advocate for the midwifery model of care (p = .16). However, LMs who agreed that local physicians understand the midwifery model of care had a significantly different pattern of reporting they were satisfied with their careers versus those who did not agree; 43.2% of those who agreed were very satisfied with their career versus 22.6% of those who did not agree. LMs who reported they almost always or always felt free to practice to the fullest extent of legal scope were significantly more satisfied than those who felt able to do so less often (p < .001). Similarly, LMs who perceived that they almost always or always could practice to the fullest extent of their expertise were significantly more satisfied than those who could do so less often (p = .002).
Satisfaction With Midwifery Career.
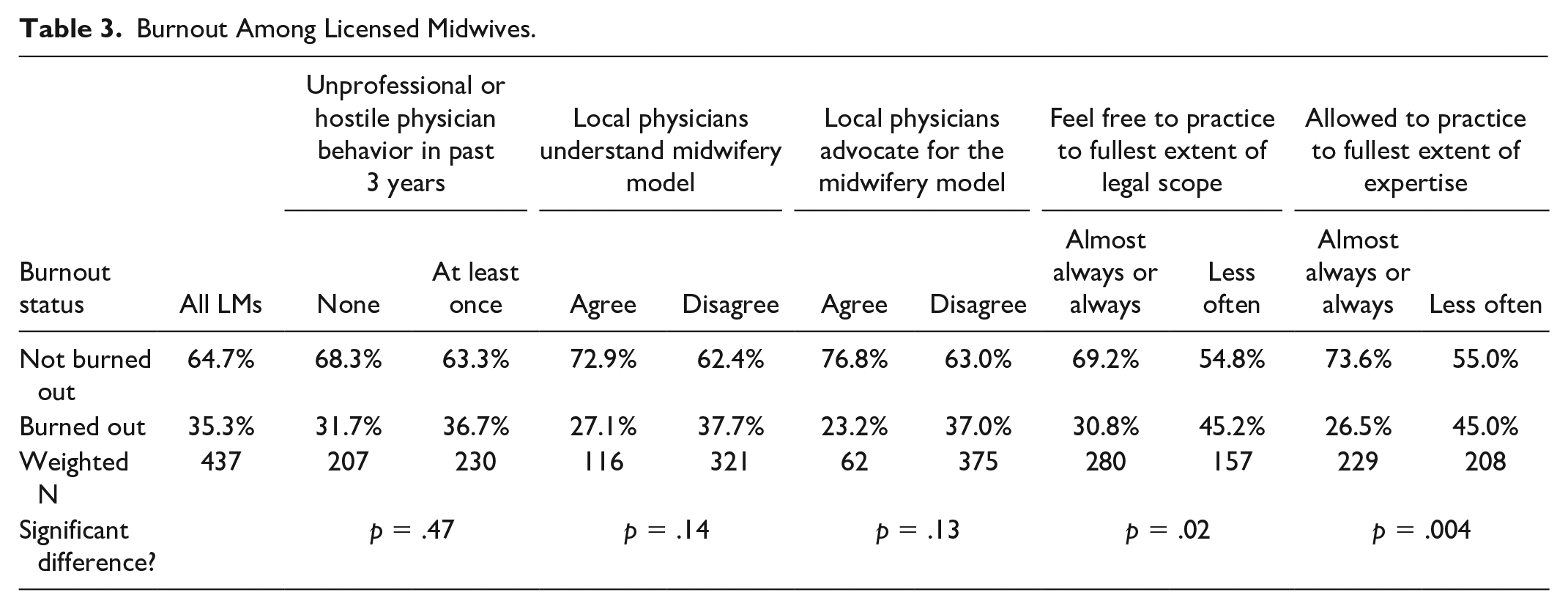
As seen in Table 3, 35.3% of LMs’ responses to the Emotional Exhaustion and Depersonalization subscales of the Maslach Burnout Inventory indicated that they were experiencing burnout. There were no statistically significant differences in rates of burnout between LMs who had versus had not experienced unprofessional or hostile physician behavior, who agreed versus disagreed that local physicians understand the midwifery model of care, or who agreed versus disagreed that local physicians advocate for the midwifery model of care. However, LMs who reported that they almost always or always feel free to practice to the fullest extent of their legal scope, and to practice to the fullest extent of their expertise, were significantly less burned out than other LMs (p = .02).
Burnout Among Licensed Midwives.
Discussion
This study described the demographics, training, client population, and practice experiences of LMs in California, providing new information that can guide policies to advance equitable care for birthing people in California and nationwide. Most LMs are practicing midwifery, and one fifth of those are also employed in a non-midwifery position, which is notably different from California nurse-midwives, of whom 85% are employees of an organization (Joynt et al., 2024). They are predominantly small business owners, usually practicing with another midwife and often with an assistant or student. They provide personalized care to relatively small numbers of clients each year, with most births occurring in homes and birth centers. California LMs report high rates of career satisfaction, with 90.4% at least somewhat satisfied with their career, which is similar to the satisfaction rate among California nurse-midwives (Joynt et al., 2024). LMs in California have lower rates of burnout than rates reported for nurse-midwives (35% for LMs and 54% for nurse-midwives; Dau et al., 2025).
A large study of women’s childbearing experiences in California reported high rates of negative birth experiences among Black women, and 66% of Black women reported they would want a midwife for a future birth (Sakala et al., 2018); LMs are stepping up to meet this need. California LMs care for a disproportionately high percentage of Black clients in California. However, they rarely accept Medicaid reimbursement, attributing this to low payment rates, bureaucratic enrollment processes, and a lack of malpractice insurance. LMs point to costs and administrative barriers as reasons they do not have malpractice insurance. The low rate of acceptance of Medicaid among California LMs may explain the low representation of Latina/x people among their clients. More than half of California’s Medi-Cal enrollees are Latinx (California Health Care Foundation, 2024), and people who identify as Latina/x comprise 49% of the state’s birthing women.
LMs’ focus on community-based care, including delivering babies at home and in birth centers, is aligned with research that shows that this approach to maternal care can improve maternal health outcomes, particularly for Black, Hispanic/Latinx, and Native American people (Zephyrin et al., 2021). However, national data have found that Medicaid enrollees have less access to birth centers than privately insured women, because birth centers face administrative challenges in participating directly in Medicaid, barriers to contracting with managed care organizations, and payment rates that are insufficient to support the costs of independent facilities (Courtot et al., 2020). Payment reforms that remove barriers to birth centers being reimbursed by Medicaid, requiring equitable payment to midwives for their services, and using value-based payments that support holistic models of care could help expand options for families who would benefit from community-based care (Sakala et al., 2022; Zephyrin et al., 2021).
While LMs make significant contributions to expanding choice in reproductive health care, they perceive that their skills and roles are not well appreciated. Most LMs think that physicians do not understand the midwifery model of care and even fewer believe they have advocates in the physician community. Many have experienced unprofessional or hostile behavior from physicians, and most have bypassed the nearest hospital when a transfer was needed, often due to perceiving that the hospital was hostile to midwifery care. LMs are much less likely than nurse-midwives to report that they think local physicians understand the midwifery model of care (26.2% vs. 67.7%; Dau et al., 2025), which might be associated with LMs’ primarily practicing in birth centers and homes (where physicians are not usually present) versus nurse-midwives primarily attending births in hospitals (Joynt et al., 2024). Our findings suggest that the lack of understanding of LMs’ model of care among physicians and the inability of LMs to use all of their skills and practice to the fullest legal scope contribute to burnout and dissatisfaction with midwifery as a career. There is a need for integrated educational programs that provide midwifery students, medical students, and obstetrics-gynecology residents opportunities to practice collaboratively and develop mutual trust and role appreciation (Avery et al., 2020). Health care systems can evaluate the workplace for a supportive midwifery practice climate and identify ways to improve it (Thumm & Flynn, 2018). They also can implement programs to improve transfers to hospitals from community-based birth settings, such as those described in the Alliance for Innovation on Maternal Health’s (AIM, 2024) Community Birth Transfer Resource Kit and the “Drill Kits” to train health care team to respond to emergencies in community settings published by the organization Step Up Together (2024).
Limitations
Our analysis has several limitations. First, is the potential for nonresponse bias. Although we received a response rate of over 50% and weighted the data to account for differential response across regions, there is a risk that the findings may not be fully representative of the entire population. Second, the survey data are self-reported and thus may contain errors. We conducted checks for consistency, outlier values, and values that were inconsistent when preparing the data, but errors might remain. Our study was conducted in California, a geographic region where LM regulations are distinct from other states and where other direct-entry midwives (i.e., certified midwives) are not recognized.
Conclusion
Ongoing racial and ethnic disparities in maternal morbidity and mortality point to the urgency of implementing multiple strategies to expand the reproductive health workforce and ensure person-centered, racially equitable birth care (National Conference of State Legislatures [NCSL], 2024). Direct-entry midwives, such as California’s LMs, can play a key role in providing person-centered care and offering clients a choice of birth setting and the model of care provided. States should support direct-entry midwife practice, establish policies that support birth center and home births, and develop strategies to improve interprofessional collaboration between physicians and midwives.
Footnotes
Appendix
Weighted frequencies and means of variables used in the study.
Q: In what year were you born?
Q: What is your racial/ethnic background? Check all that apply.
Q: Over the past year, what percentage of your clients do you think had the care you provided paid for / reimbursed by each of the following methods?
Q: Do you have malpractice insurance? If no, why not? Check all that apply.
Acknowledgements
We appreciate editorial contributions from Jennifer Joynt and Stephanie Teleki. We also appreciate the guidance of an Advisory Committee: Rosanna Davis, LM, CPM, California Association of Licensed Midwives; Kathleen Dowd, CNM, California Nurse-Midwives Foundation; Tanya Khemet Taiwo, CPM, MPH, PhD, Bastyr University / Skyline Foundation; and Holly Smith, CNM, MPH, FACNM, California Nurse-Midwives Foundation / Midwifery Access California.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the California Health Care Foundation.
Ethical Approval and Informed Consent Statements
This research was approved by the UCSF Committee for Human Research.
Data Availability Statement
Public-use files from the surveys are available upon request.