
Abstract
Public health care policymakers and payers are increasingly investing in efforts to address patients’ health-related social needs (HRSNs) as a strategy for improving health while controlling or reducing costs. However, evidence regarding the implementation and impact of HRSN interventions remains limited. California’s Whole Person Care Pilot program (WPC) was a Medicaid Section 1115 waiver demonstration program focused on the provision of care coordination and other services to address eligible beneficiaries’ HRSN. In this study, we examine pilot-level variation in impact on acute care utilization and identify factors associated with differential outcomes. The majority of pilots reduced emergency department (ED) visits for enrollees relative to matched controls; however, only four pilots reduced both ED visits and hospitalizations. Coincidence analysis results highlight the importance of cross-sector partnerships, field-based outreach and engagement, and adequate program investment in differentiating pilots that reduced acute care utilization from those that did not.
Keywords
Introduction
Over the last decade, health care policymakers and payers have increasingly focused on addressing patients’ health-related social needs (HRSNs) as a strategy for improving health while controlling or reducing costs (Alley et al., 2016; Fichtenberg et al., 2020). In 2023, 25 states and the District of Columbia approved Medicaid Section 1115 waivers that included efforts to address beneficiaries’ HRSN (Chuang & Safaeinili, 2024), such as housing or nutrition assistance. Many states also include provisions related to identifying or addressing HRSN in their contracts with managed care plans (Gifford et al., 2021; Shin et al., 2021), although plan uptake of services to address HRSN remains low (Crook et al., 2021; Jin et al., 2022; Meyers et al., 2022).
Identifying and addressing patients’ HRSN requires significant investment in infrastructure and partnership development (Berkowitz, 2023; McConnell et al., 2023; Murray et al., 2020). However, the evidence base regarding implementation and health impacts of HRSN interventions remains limited and mixed, with some studies demonstrating reduced acute care utilization and costs (Johnson et al., 2012; Pourat et al., 2023), and others finding mixed or no impact (Brown et al., 2022; Finkelstein et al., 2020). Most studies also do not include detailed information on program implementation such as patient engagement strategies used, staffing, or caseload, limiting replicability even if proven effective (Albertson et al., 2022; Chuang & Safaeinili, 2024). As a result, uptake of HRSN interventions by managed care plans and health care providers remains limited due to concerns about financial risks and sustainability (Chisolm et al., 2019; Gottlieb et al., 2017; Kushner & McConnell, 2019).
California’s Medi-Cal Whole Person Care Pilot Program
The current study contributes to the literature by drawing on mixed methods evaluation data from California’s Medi-Cal Whole Person Care (WPC) Pilot Program to identify implementation strategies that differentiated pilot programs (pilots) that successfully reduced acute care utilization from those that did not. WPC was a Medicaid Section 1115(a) waiver program implemented from 2016 to 2021 by 25 pilots representing the majority of counties in California. Under WPC, all eligible beneficiaries received patient-centered care coordination of health, behavioral health, and social services. Beneficiaries also received housing assistance, benefits assistance, transportation assistance, and other services to address any identified HRSN. WPC-eligible populations included Medicaid beneficiaries who were high utilizers of acute health care services; experiencing homelessness or at-risk of homelessness; affected by serious mental illness, substance use disorders, or both; recently released from jail or prison; and/or affected by multiple chronic conditions.
Pilots were subject to certain requirements (e.g., in types of partners involved and services provided) but otherwise had flexibility in tailoring their programs to local needs and resources (Chuang et al., 2020). All pilots were implemented as cross-sector partnerships that included county agencies, Medicaid managed care plans, and community-based providers; however, program funds were funneled through pilot-designated lead entities, typically a county health agency, rather than through Medicaid managed care plans. Pilots were also encouraged to develop delivery system and data sharing infrastructure needed to improve cross-sector collaboration and integration of care but varied in investments and changes made.
Statewide evaluation results showed that WPC reduced emergency department (ED) use, hospitalizations, and overall costs of care for enrollees relative to a matched comparison group (Pourat et al., 2022). However, the evaluation did not assess whether program impact varied across pilots. The current study addresses this gap by assessing variation in pilots’ impact on acute care utilization and by identifying program implementation strategies and other factors associated with differential program outcomes.
Conceptual Framework
Our study of factors affecting WPC program outcomes is anchored by a conceptual model (Figure 1) informed by the cross-sector alignment framework (Landers et al., 2020), frameworks assessing determinants of implementation effectiveness (Aarons et al., 2011; Damschroder et al., 2022), and the logic model for the WPC evaluation (Pourat et al., 2022). The cross-sector alignment framework highlights the importance of partnership-level factors such as shared purpose, data, financing, and governance to system alignment efforts, while frameworks assessing determinants of implementation effectiveness such as the Consolidated Framework for Implementation Research (CFIR) and the Exploration, Preparation, Implementation, and Sustainment (EPIS) framework inform systematic identification of intervention characteristics and factors in the inner (organizational) and outer context (partnership, community) that may influence program implementation. Finally, the logic model for the WPC evaluation describes the mechanisms through which WPC is hypothesized to impact enrollee outcomes (e.g., strengthened delivery system and data sharing infrastructure resulting in increased care coordination and access to care, which in turn, will result in improved enrollee health).
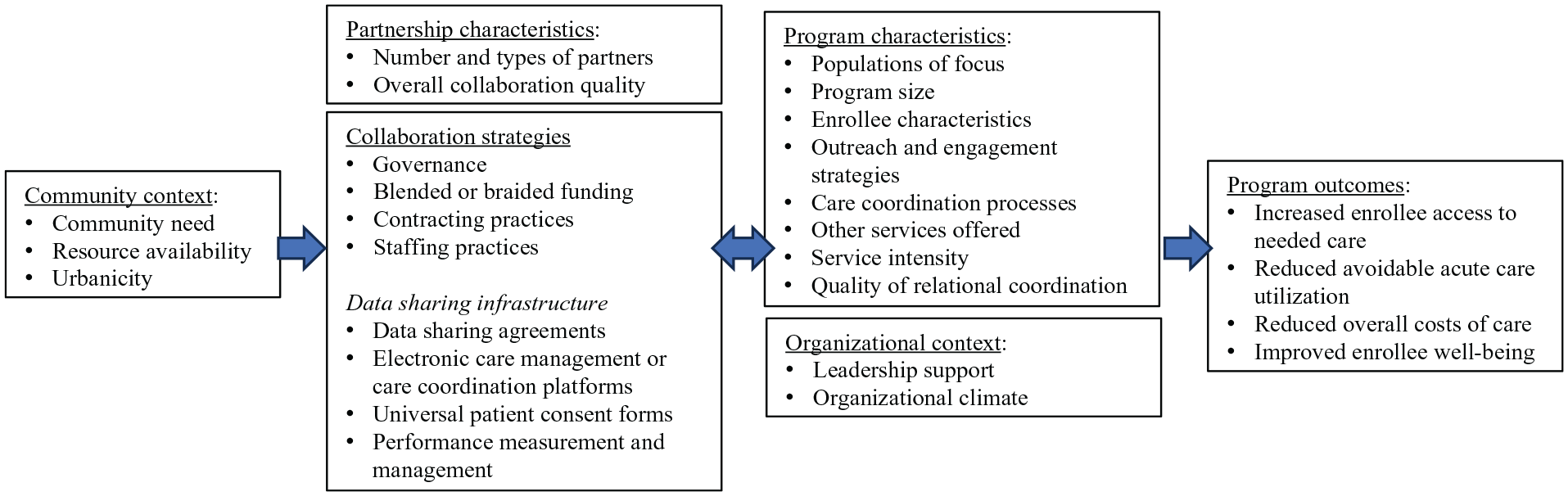
Factors Hypothesized to Influence Medi-Cal Whole Person Care Pilot Outcomes.
Informed by these frameworks, we hypothesize that WPC impact was influenced by partnership characteristics, collaboration strategies, program characteristics, and factors in the local community and organizational context. Partnership characteristics reflect the number and types of partners involved and their overall relationship quality, while collaboration strategies refer to specific policies and practices (e.g., governance arrangements, contracting practices) used to align operations or services across partners (Bunger et al., 2020). Governance arrangements refer to rules or processes for determining authority and accountability for program activities (Ansell & Gash, 2008; Bianchi et al., 2021); these arrangements can either focus all authority and accountability on a single entity or deliberately engage a broader range of cross-sector partners. Contracting practices include decisions made regarding whether to directly provide or outsource services, and whether any formal arrangements between partners included financial incentives linked to achievement of prespecified deliverables or outcomes (Lambright, 2009).
Program characteristics reflect unique program attributes hypothesized to impact program outcomes. In WPC, these program characteristics included variation across pilots in populations of focus, program size, enrollee characteristics, engagement strategies (i.e., strategies for identifying and building trust and rapport with eligible beneficiaries), care coordination processes (Chuang et al., 2019), and services offered. For example, while all pilots enrolled individuals experiencing homelessness, only about half of pilots (56%; 14 of 25) explicitly developed their programs with this population in mind (Pourat et al., 2021). Pilots also varied in their use of field-based outreach to identify and enroll eligible beneficiaries in WPC and in their use of staff with prior lived experience similar to that of enrollees.
Finally, we also included factors in the local community and organizational context known to influence implementation, such as community need, resource availability, and leadership support or buy-in (Aarons et al., 2011; Damschroder et al., 2022; Weiner, 2009).
New Contribution
In the United States, an increasing number of state Medicaid programs have adopted new state plan benefits or obtained Section 1115 waivers to cover services addressing HRSN for a wide range of medically and socially complex populations (Hinton & Diana, 2024; McConnell et al., 2023). However, currently little is known about program implementation (e.g., infrastructure developed, program staffing, and other characteristics), or its impact on acute care utilization, costs, or other health outcomes for enrolled members (Chuang & Safaeinili, 2024). To address this gap, we draw on data from the statewide evaluation of a Medicaid Section 1115(a) waiver program focused on identifying and addressing members’ HRSN to examine local variation in program impact on acute care utilization and by identifying program implementation strategies and other factors associated with differential program outcomes.
Method
Study Design
We used a convergent mixed methods approach (Creswell & Clark, 2017), in which quantitative and qualitative data from the statewide evaluation of WPC were collected and integrated during analyses. Analyses proceeded in multiple stages. First, we examined each pilot’s impact on acute care utilization by implementing a pre-post study design, in which separate difference-in-difference multivariate regression models were developed to assess each pilot’s impact on enrollee ED visit and hospitalization rates relative to a matched comparison group. A key assumption of this design is the parallel trends assumption, that is, that in the absence of WPC, outcome trends for enrollees and matched controls would have been parallel (Wing et al., 2018). In this study, we used propensity score matching to strengthen the validity of this assumption.
Next, we used a type of configurational comparative method (CCM) known as coincidence analysis to identify program implementation strategies and other conditions that differentiated pilots who successfully reduced acute care utilization from those who did not. CCMs represent formal, mathematical approaches to conducting cross-case analyses based on Boolean algebra and set theory (Rihoux & Ragin, 2009); a key analytic objective is to identify conditions that uniquely differentiate one group of cases from another. An advantage of CCMs over correlation-based methods is that analyses allow for causal complexity (when several conditions must jointly appear for an outcome to occur) and equifinality (multiple pathways to an outcome) (Whitaker et al., 2020). In CCMs, positive models (solutions explaining when an outcome is present) are run separately from negative models (solutions explaining when an outcome is absent).
Currently, the two most prominent types of CCMs are qualitative comparative analysis (QCA) and coincidence analysis (CNA). The two methods are both based on Boolean algebra and set theory but differ in the central algorithm used to identify necessary and sufficient conditions. QCA applies the “top-down” Quine-McCluskey algorithm developed in the field of electrical engineering, while CNA uses a bottom-up algorithm custom-designed for application in social sciences research (Swiatczak, 2022). In the current study, we chose to use CNA because it does not require the use of counterfactuals, that is, making assumptions about configurations not observed in our data, and because CNA is the only CCM with a systematic routine to assist with initial factor selection (Yakovchenko et al., 2020).
Study Context and Sample
WPC was implemented by 25 unique pilots that collectively served a cumulative total of 247,887 unique enrollees between 2017 and 2021 (Pourat et al., 2023). In the current study, to ensure adequate power, we restricted our sample to pilots that served at least 1,000 enrollees (n = 16 of 25; 64% of participating pilots). These 16 pilots collectively served 244,248 enrollees, or 98.5% of all WPC enrollees. The service area of each of these 16 pilots corresponded to that of a single county. Additional information about these 16 pilots is available in Supplemental Appendix 1.
Data Sources
Data used in this study were collected as part of the statewide evaluation of WPC and included 2015–2021 Medicaid claims and enrollment data; documents submitted by participating pilots to the California Department of Health Care Services (e.g., applications, biannual narrative reports, quarterly enrollment and utilization reports, annual invoices); surveys of all WPC-participating entities (lead entities and partners) and of frontline staff; and key informant interviews.
We used Medicaid claims and enrollment data to obtain information on demographic characteristics, health status, service utilization, and costs for WPC enrollees and a matched comparison group. Quarterly enrollment and utilization reports and invoices were used to identify WPC enrollees, average length of enrollment, and expenditures. Applications and narrative reports submitted by pilots to the state between July 2016 and December 2021 provided insight into pilots’ governance structure, goals, activities, and local community context. Content in all remaining domains identified in Figure 1 was assessed using qualitative data collected by the evaluation team, including a partner database, organizational surveys, a frontline worker survey, and key informant interviews. The partner database identified all WPC-participating entities in 2018 and 2020 and also included lead entities’ rating of extent to which partners were actively engaged in WPC.
We fielded two types of organizational surveys: surveys of pilot lead entities administered in 2018, 2020, and 2021 (response rates 96%–100%) and network surveys administered to all WPC-participating entities in 2018 and 2020 (response rates 55% and 46%). Lead entity surveys addressed collaboration strategies and program characteristics, while network surveys assessed the perceived quality of collaboration as well as multiplexity and density of ties between WPC-participating entities within each pilot. The frontline worker survey was administered in 2020 (mean response rate 56%; range 20%–100% per pilot) and addressed workers’ perceptions of their role, quality of coordination, leadership support, and organizational climate. All surveys were administered online, using SurveyMonkey (2018) or Qualtrics (2020 and 2021); data were subsequently cleaned and analyzed using Stata 16.0.
Key informant interviews were conducted September 2018–May 2019 and June–August 2021 with organizational leaders from different WPC-participating entities, managers, and frontline staff involved in WPC implementation. Interviews were conducted either in-person or via video conference (Zoom) by at least two members of the research team using semistructured interview guides tailored to respondents’ role in WPC. Interview guides addressed a broad range of topics, including organizations’ motivations for participating in WPC, program characteristics, collaboration strategies, local community and organizational context, and key facilitators, barriers, and lessons learned in implementation. With respondents’ permission, all interviews were recorded, professionally transcribed, and coded using a codebook reflecting key content domains of interest. Additional information about these data are also available elsewhere (Pourat et al., 2023).
Assessing Pilots’ Impact on Acute Care Utilization
We measured whether pilots reduced both ED visits and hospitalizations for WPC enrollees (=1 if yes, =0 if no). To assess the impact of WPC on acute care utilization, we used a quasi-experimental difference-in-difference design (Wing et al., 2018), in which we followed each beneficiary and matched controls for 2 years before WPC enrollment and up to 3 years after enrollment. For these analyses, our study population included Medicaid beneficiaries enrolled in WPC at any point between January 2017 and December 2021.
We used propensity scores to identify controls, that is, Medicaid beneficiaries that did not receive services from any WPC pilot but otherwise had similar demographic characteristics, health status, service utilization, cost profiles, and county of residence as enrollees. Within each pilot, we grouped WPC enrollees into cohorts based on the quarter in which they enrolled in WPC, and then matched to controls using data from 2 years prior to the quarter of their WPC enrollment. Each enrollee was matched to two controls; controls were sampled with replacement. Additional information regarding our propensity score matching approach is available in Supplemental Appendix 2.
To evaluate the impact of WPC on ED visits and hospitalization rates per 1,000 beneficiaries per year, we ran multilevel generalized linear models, using the Poisson distribution to account for the skewed distribution of our outcomes. All models controlled for enrollee demographics (gender, age, race/ethnicity, primary language, months of Medi-Cal enrollment), program characteristics (pilot, year of enrollment), baseline acute care utilization, and health status indicators (baseline Chronic Illness and Disability Payment System risk scores, specific chronic conditions, total count of chronic conditions). The exposure option within the Stata—glm—package was used to adjust for the number of months that beneficiaries were enrolled in full-scope Medi-Cal. Random intercepts for beneficiaries were used to accommodate within-patient correlation. To test the parallel trends assumption, we ran multilevel models with individual random intercepts and an interaction term that allowed for potentially different pretrends in the baseline years between WPC enrollees and matched controls. Additional information regarding our approach to testing the parallel trends assumption is provided in Supplemental Appendix 2.
In our study, we considered Pilots to have reduced acute care utilization if they significantly reduced both emergency department visits and hospitalizations for WPC enrollees relative to controls.
Coincidence Analyses
Analyses of data from pilot-reported documents, surveys, and key informant interviews resulted in an initial list of 92 potential explanatory factors across all key domains identified in Figure 1 (community context, partnership characteristics, collaboration strategies, program characteristics, and organizational context). We calibrated all explanatory factors for use in CNA, meaning they were recoded as binary (yes/no) or categorical variables (maximum value range 1–5). Supplemental Appendix 3 describes all of these factors, how they were operationalized, and the data source(s) used. Data were entered into an Excel spreadsheet in which rows represented each pilot and columns reflected specific variables of interest.
The next step was to reduce the number of conditions in our data. Specifically, we applied the “minimally sufficient conditions” (“msc”) function within the R coincidence analysis (“cna” package) (Baumgartner et al., 2023) to identify configurations of conditions with particularly strong connections to our outcome variables. We considered all one-, two-, and three-condition configurations that met predesignated thresholds for consistency and coverage. Consistency indicates how often a solution results in the outcome when present, and coverage indicates an empirical prevalence of the solution within the sample (i.e., number of cases with configuration and outcome present divided by the total number of cases with the outcome). Per CNA convention, we started with a minimum consistency threshold of 75% and assessed all configurations that satisfied coverage thresholds of 75%, 80%, 85%, 90%, and 95% to compare output at different thresholds (Rich et al., 2022).
We generated a condition table listing all configurations of conditions that met these thresholds. A review of this table resulted in identification of smaller subsets of conditions to model (see Table 1). During this phase, we also further reduced the dimensionality of selected factors, using mathematical output from the -msc- function together with subject matter knowledge to identify specific value levels at which individual factors linked to an outcome (Miech et al., 2021); this process resulted in dichotomizing certain variables (e.g., data sharing infrastructure, program intensity) rather than preserving their original, categorical format.
Explanatory Conditions Included in Final Coincidence Analysis Model.
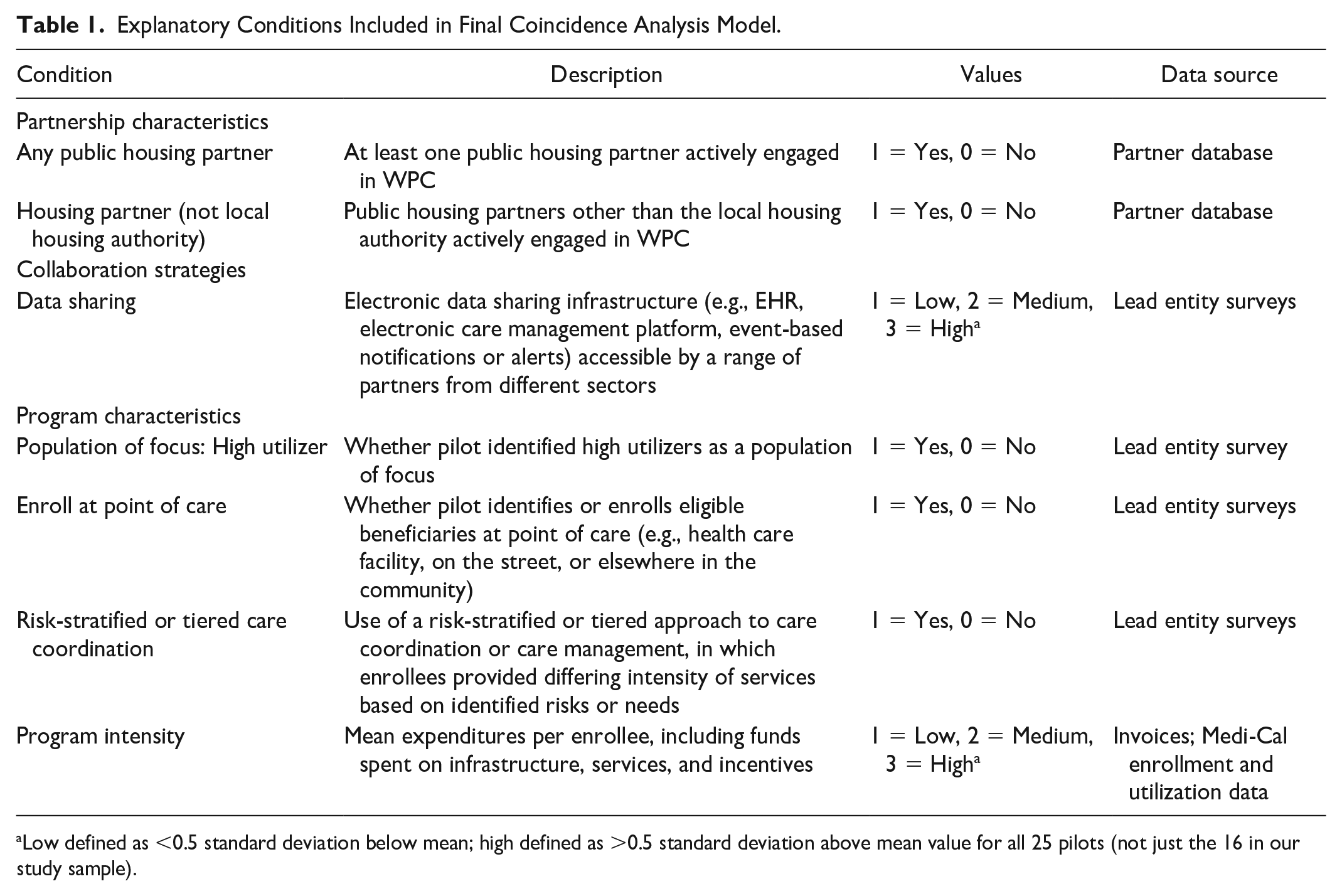
Low defined as <0.5 standard deviation below mean; high defined as >0.5 standard deviation above mean value for all 25 pilots (not just the 16 in our study sample).
Finally, we performed coincidence analysis using appropriate functions within the R “cna” package (e.g., -mvcna-, -frscored_cna-) (Baumgartner & Thiem, 2015). Models were developed iteratively based on our assessment of overall consistency and coverage of identified solutions and potential model ambiguity (i.e., when competing models explain the outcome equally well based on their consistency and coverage scores). We initially prioritized configurations with high consistency, lower complexity (fewer conditions), higher coverage scores, and for which different values of the same conditions explained whether or not a pilot reduced acute care utilization. To address potential model ambiguity, we reviewed exhaustiveness and faithfulness scores and fit-robustness (FR) scores. To mitigate the risk of overfitting, that is, inclusion of causally irrelevant factors (Parkinnen & Baumgartner, 2023), final model selection was based on the highest FR scores, followed by the highest consistency, highest coverage, lowest complexity, and exhaustiveness and faithfulness scores (Baumgartner et al., 2023).
All CNA analyses were conducted using the R “cna” package, R Studio, and Excel. Study activities were conducted with the approval of the California Committee for the Protection of Human Subjects.
Results
Table 2 provides an overview of key characteristics of the 16 pilots in our sample. Briefly, pilots served a mean of 15,266 and a median of 4,173 enrollees. Over half of enrollees (51%) experienced homelessness, over a third had serious mental illness (35%), and close to a third were diagnosed with substance use disorder. In addition, about a third had multiple chronic conditions, that is, 3+ chronic conditions per Chronic Condition Warehouse criteria in the 2 years prior to WPC enrollment, and over a third (35%) were high utilizers, that is, 3+ ED visits or inpatient stays in 12 months prior to WPC enrollment. Approximately 63% of pilots (10 of 16) identified high utilizers as a primary population of focus for their programs and over half (56%; 9 of 16) identified individuals experiencing homelessness as a primary population of focus.
Characteristics of California’s Whole Person Care Pilots, 2017–2021.
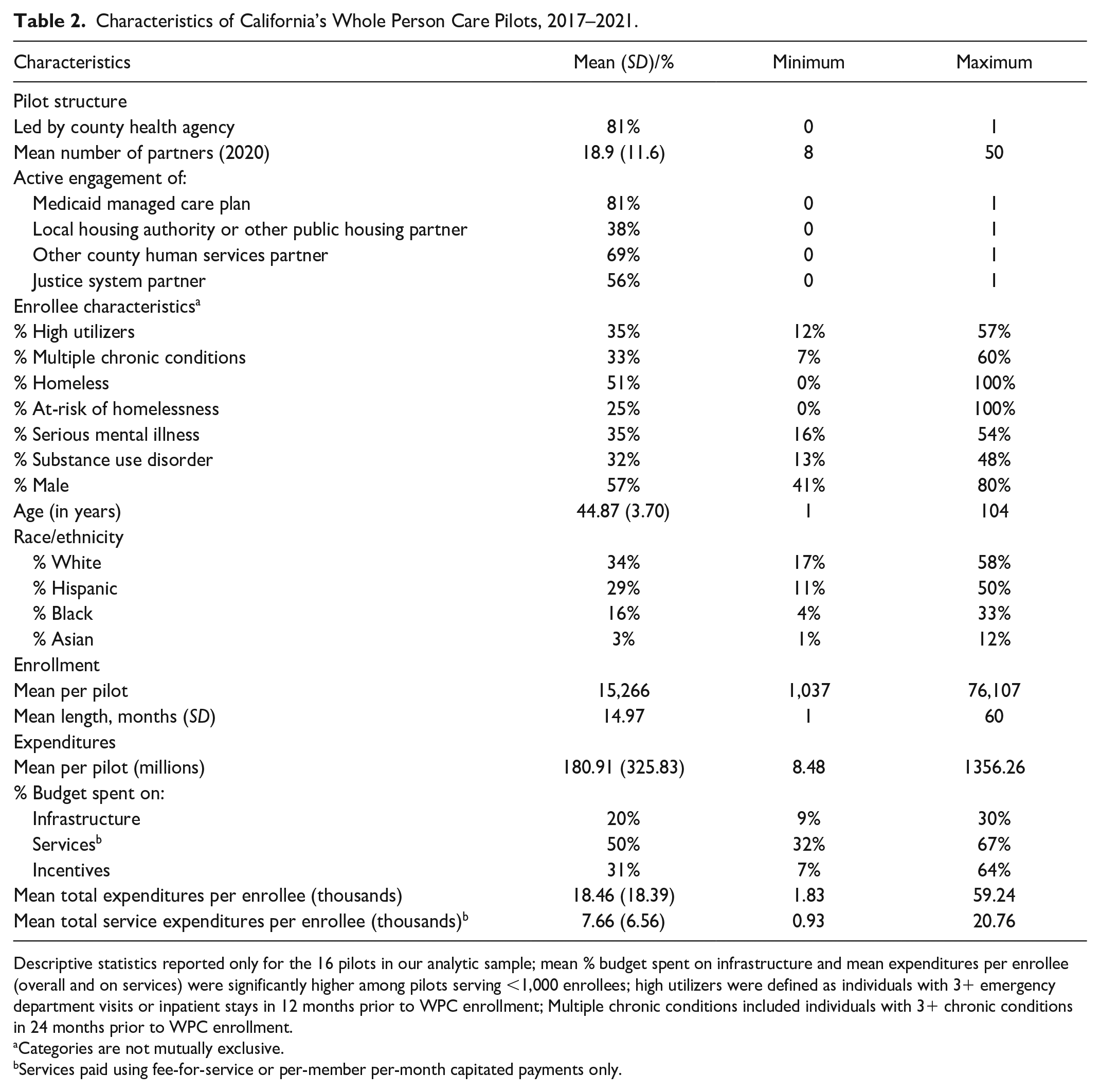
Descriptive statistics reported only for the 16 pilots in our analytic sample; mean % budget spent on infrastructure and mean expenditures per enrollee (overall and on services) were significantly higher among pilots serving <1,000 enrollees; high utilizers were defined as individuals with 3+ emergency department visits or inpatient stays in 12 months prior to WPC enrollment; Multiple chronic conditions included individuals with 3+ chronic conditions in 24 months prior to WPC enrollment.
Categories are not mutually exclusive.
Services paid using fee-for-service or per-member per-month capitated payments only.
Difference-in-Difference Analysis Results
Regression analyses confirmed that WPC enrollees in the 16 pilots collectively had lower acute care utilization than comparable Medicaid beneficiaries that did not participate in the program (Table 3). Overall, ED visits and hospitalizations decreased by 7.22% and 1.89% per 1,000 beneficiaries per year more, respectively, for WPC enrollees than their matched controls. Pilot-level findings revealed significant heterogeneity in impact across pilots. Of the 16 pilots, three did not reduce either ED visits or hospitalizations; eight pilots only reduced ED visits, one pilot only reduced hospitalizations, and four pilots reduced both ED visits and hospitalizations for WPC enrollees relative to controls. For the purposes of coincidence analysis, we coded the four pilots that reduced both ED visits and hospitalizations as reducing acute care utilization and the remaining 12 pilots as not reducing acute care utilization.
Difference-in-Difference Results: Change in Acute Care Utilization in WPC Versus Non-WPC Enrollees.
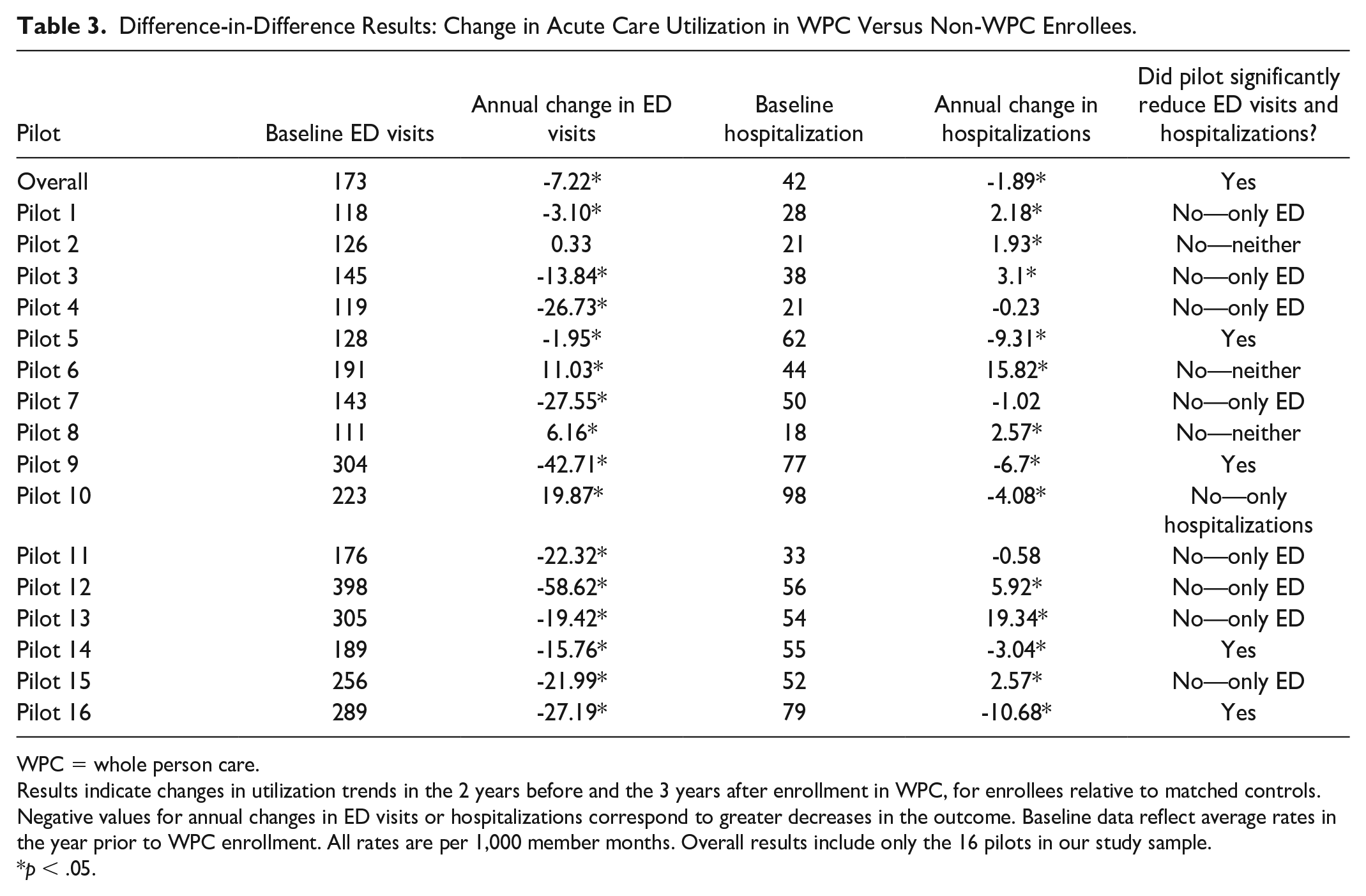
WPC = whole person care.
Results indicate changes in utilization trends in the 2 years before and the 3 years after enrollment in WPC, for enrollees relative to matched controls. Negative values for annual changes in ED visits or hospitalizations correspond to greater decreases in the outcome. Baseline data reflect average rates in the year prior to WPC enrollment. All rates are per 1,000 member months. Overall results include only the 16 pilots in our study sample.
p < .05.
We also conducted a number of sensitivity analyses (see Supplemental Appendix 4 for detailed results). First, we ran a sensitivity analysis to determine if the results differed based on populations served. Specifically, in 9 of 16 pilots that identified individuals experiencing or at-risk of homelessness as a population of focus, we reran analyses restricting our sample to enrollees experiencing or at-risk of homelessness (~75% of enrollees in these nine pilots). While the magnitude of effect size changed, overall model results did not differ significantly from those presented in Table 3.
Second, due to differences in the matching process used for these individuals, we reran analyses excluding WPC enrollees without prior Medicaid enrollment or claims data (~2% of enrollees). Conceptually, we felt it was important to include these enrollees in our analyses because their presence reflected some pilots’ commitment to identifying and engaging “hidden populations” in care, for example, chronically unhoused people who were eligible for but not enrolled in Medicaid or that may have multiple needs but historically disaffiliated from and mistrusting of care. In one pilot that focused exclusively on serving individuals experiencing homelessness, individuals without prior Medicaid enrollment or claims data accounted for ~6% of enrollees; once these enrollees were excluded from the sample, results indicated that this pilot did successfully reduce both ED visits and hospitalizations for enrollees relative to matched controls (as opposed to just ED visits).
Finally, to determine if results changed based on length of exposure to WPC, we reran analyses with our sample restricted to enrollees who participated in WPC for at least 1 month (96% of enrollees), and then again with our sample restricted to enrollees who participated in WPC for at least 6 months (70% of enrollees). Results did not significantly change in any of the pilots when we restricted our analyses to enrollees who participated in WPC for at least 1 month.
When we restricted our analyses to enrollees who participated in WPC for at least 6 months, results changed in two pilots. Specifically, we found that one pilot no longer significantly reduced acute care utilization for enrollees who participated for at least 6 months, while another pilot did. In the first pilot, most WPC services were designed to be short-term (e.g., 30 days or less) and focused on improving transitions of care posthospitalization or postincarceration. In this pilot, less than half of enrollees participated in WPC for at least 6 months, and the pilot reduced hospitalizations but not ED visits for these enrollees. The second pilot was the same one previously described as exclusively serving individuals experiencing homelessness and as including a high percentage of enrollees without prior Medicaid enrollment or claims data. In this pilot, 93% of enrollees participated for more than 6 months; results suggest that this pilot successfully reduced acute care utilization for enrollees who participated in WPC for at least 6 months but did not reduce hospitalizations for those who engaged for a month or less.
Coincidence Analysis Results
Coincidence analysis identified conditions whose presence or absence differentiated pilots that reduced acute care utilization from those that did not (Table 4). Specifically, in our positive solution model, the four pilots that reduced both ED visits and hospitalizations either (a) had a public housing partner other than the local housing authority actively engaged in WPC and identified or enrolled eligible beneficiaries at the point of care or (b) medium to high electronic data sharing infrastructure and medium to high program intensity. These conditions explained reduced acute care utilization in all four pilots (100% coverage) with 100% consistency. Brief examples of these conditions are provided in Table 5. Two of the four pilots met criteria for both solution pathways.
Coincidence Analysis Results: Conditions That Differentiated Pilots That Reduced Acute Care Utilization From Those That Did Not a .
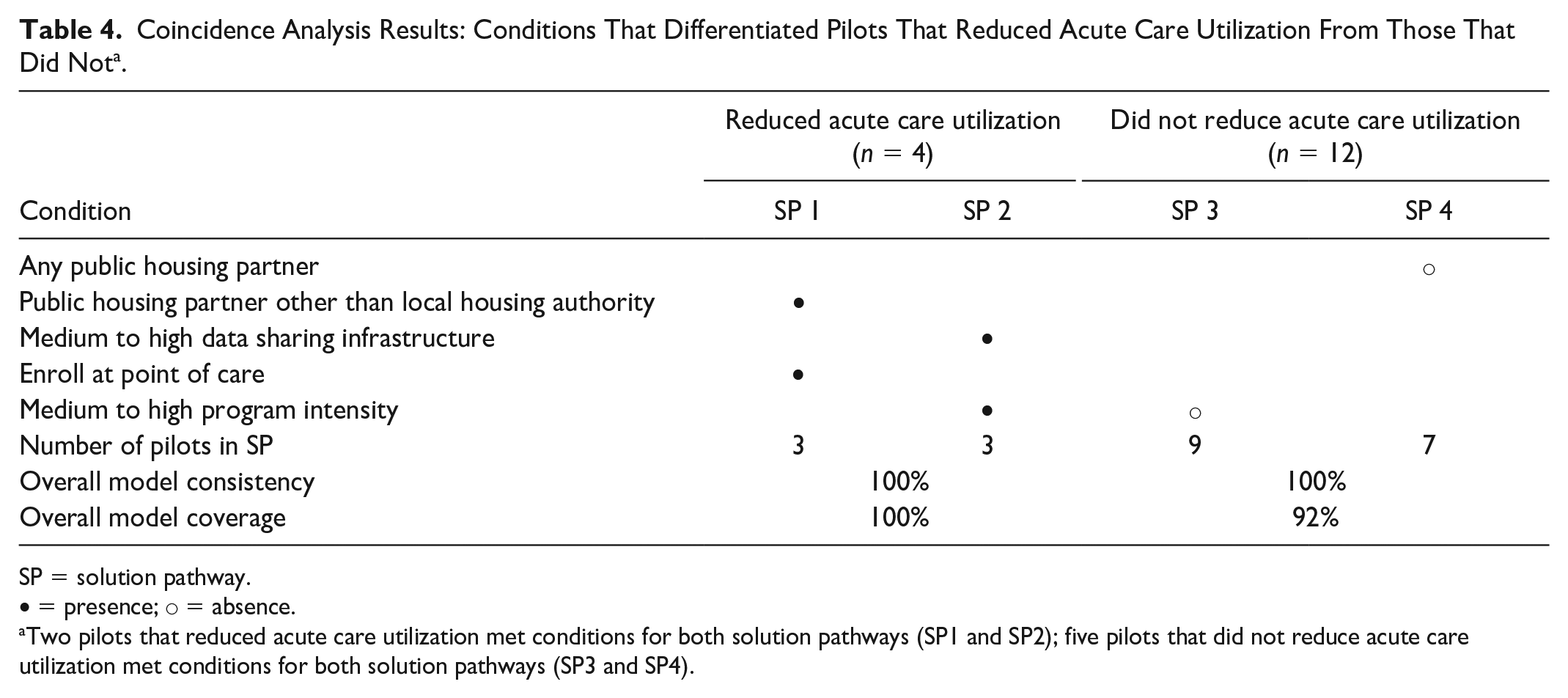
SP = solution pathway.
• = presence; ○ = absence.
Two pilots that reduced acute care utilization met conditions for both solution pathways (SP1 and SP2); five pilots that did not reduce acute care utilization met conditions for both solution pathways (SP3 and SP4).
Illustrative Examples of Difference-Making Conditions in Pilots That Successfully Reduced Acute Care Utilization.
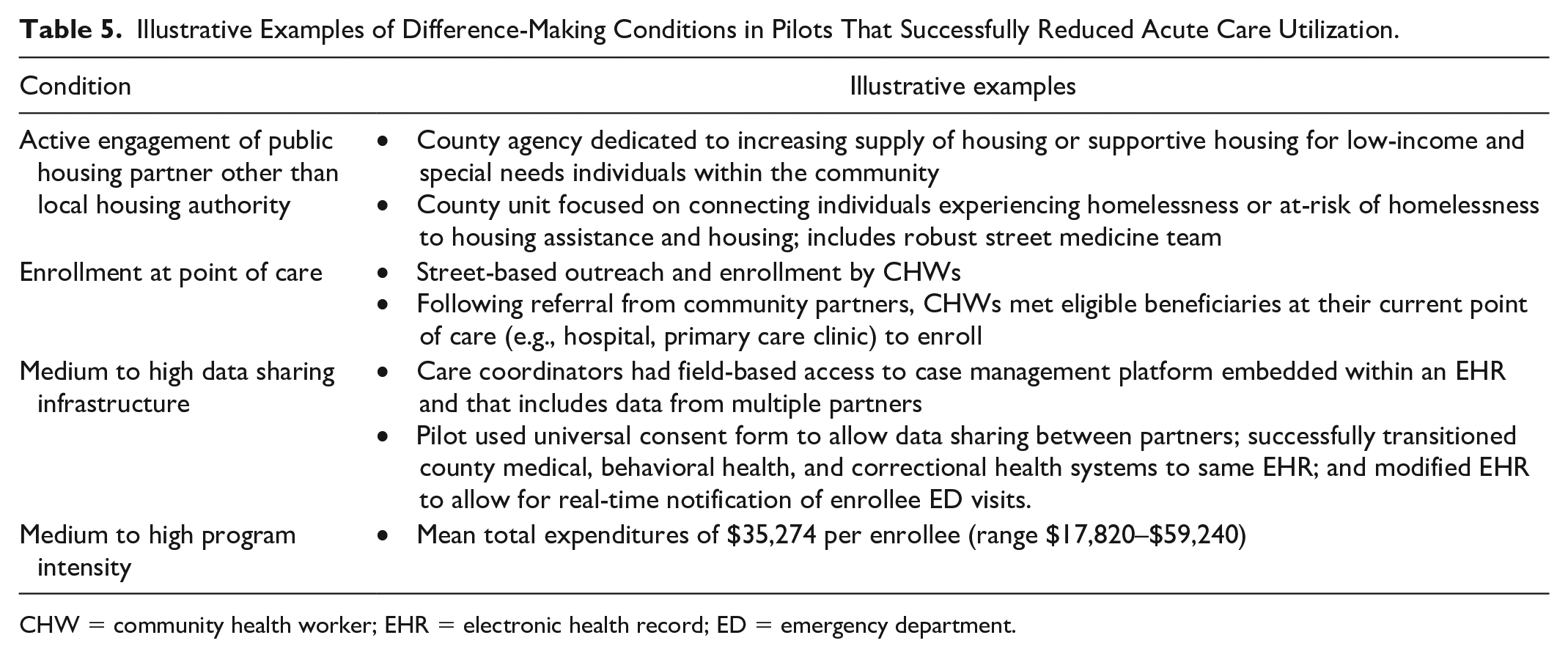
CHW = community health worker; EHR = electronic health record; ED = emergency department.
By contrast, in the negative solution model, the 12 pilots that did not reduce acute care utilization either (a) did not have any public housing partners actively engaged in WPC or (b) had low program intensity, that is, below average expenditures per enrollee (
To determine whether conditions that explained reduced ED visits differed from those that explained reduced hospitalizations, we also conducted a sensitivity analysis in which we modeled reduced ED visits and reduced hospitalizations as separate outcomes. A detailed overview of explanatory conditions and model results is provided in Supplemental Appendix 5. Briefly, we found that the primary conditions that differentiated pilots that reduced ED visits from those that did not were active engagement of housing partners, use of field-based strategies for identifying and engaging eligible members in WPC, and pilots’ infrastructure development needs. When examining hospitalizations, we found that data sharing infrastructure and program intensity, that is, average expenditures per enrollee, were the primary conditions that differentiated pilots that significantly reduced hospitalizations from those that did not.
Discussion
Study findings confirm considerable heterogeneity across pilots in program impact on acute care utilization. Most pilots significantly reduced either ED visits or hospitalizations for enrollees relative to matched controls. However, only four pilots reduced both ED visits and hospitalizations.
Study findings also provide insight into factors that may have contributed to pilot success in reducing both ED visits and hospitalizations for enrollees relative to matched controls. These factors included either actively engaging a public housing partner and enrolling eligible beneficiaries at the point of care, or developing a robust electronic data sharing infrastructure and implementing more intensive programs. Conversely, two factors that may have contributed to lack of success in reducing both ED visits and hospitalizations were failure to actively engage a public housing partner or implementing less intensive programs.
These findings are consistent with previous literature suggesting the importance of cross-sector partnerships and field-based outreach and engagement strategies for the successful implementation of care coordination and other interventions designed to address HRSN (Chuang et al., 2020; Fichtenberg et al., 2022; McConnell et al., 2023; Murray et al., 2020). Specifically, in our study, we found that successful pilots engaged public housing partners experienced in how to best connect clients to supportive or affordable housing in their communities. Although WPC was not solely focused on populations experiencing homelessness, the majority of enrollees experienced homelessness or were at-risk of homelessness (Pourat et al., 2022); thus, in our study, inclusion of these partners, alongside field-based enrollee outreach and engagement strategies, could have played a critical role in engaging enrollees in care coordination services and in ensuring their HRSN were identified and met. It is also possible that the presence of these public housing entities was indicative of communities already committed to making upstream systems changes needed to meaningfully address social determinants of health, for example, via local tax increases needed to create and support the existence of these agencies and develop other resources within the community (Castrucci & Auerbach, 2019; Thompson et al., 2021).
Study findings related to the importance of program intensity (as measured by average per-enrollee expenditures) and of having robust infrastructure in place for reducing acute care use also further reinforce prior literature suggesting the importance of adequately resourcing HRSN interventions, including upfront infrastructure investments needed for successful implementation (Gold et al., 2023; Murray et al., 2020). Specifically, in our study, we found that pilots with higher program intensity and strong electronic data sharing capabilities successfully reduced acute care utilizations, particularly hospitalizations. Similarly, we found that pilots’ infrastructure development needs (indicated by percent of budget the pilot needed to allocate to delivery system and data sharing infrastructure development to successfully implement WPC) was one of the conditions that differentiated pilots that significantly reduced ED visits for WPC enrollees from those that did not.
Several limitations must be taken into consideration in interpreting study results. First, our regression methods were observational rather than based on experimental design. However, we used robust difference-in-difference methods to estimate WPC program impact on acute care utilization. Second, our decision to restrict our analytic sample to pilots that served at least 1,000 enrollees resulted in the exclusion of smaller pilots and those located in rural areas; as a result, we were unable to identify program implementation strategies associated with reduced acute care utilization in these settings. In prior research, we found that smaller pilots and those located in more rural areas typically had less delivery system and data sharing infrastructure needed to support effective care coordination or address members’ HRSN in place at baseline, that is, prior to WPC implementation (Pourat et al., 2022). Future research could assess whether these pilots’ need to focus more on infrastructure development in the early years of the pilot may have impacted their ability to reduce acute care utilizations for enrollees. Third, although response rates on surveys of pilot lead entities was high (96%–100%), response rates on network surveys of partners was lower, particularly among partners not actively engaged in WPC, and may have affected the quality of our three network-based measures of the strength or quality of collaboration. We attempted to mitigate this limitation by symmetrizing the data (e.g., if one organization reported a tie with another organization, we assumed the tie was reciprocated) (Borgatti et al., 2018). Still, the fact that these measures were not identified in the final coincidence analysis solutions could have been due to measurement error rather than because they were not important. Similar concerns applied to our measures of organizational climate within pilots (e.g., staff role overload, perceived supervisor support, voice climate), due to modest response rates on the frontline worker survey (~56%). In addition, while coverage of the final coincidence analysis solution model was high, one pilot that did not reduce acute care utilization was not included in any of the identified solution pathways, indicating a possible role for additional factors beyond those included in the model. Finally, we did not include individual-level data from WPC enrollees. Enrollee perspectives on extent to which services were client-centered, integrated, or meaningfully improved well-being could also provide important insights.
Despite these limitations, our findings have implications for future efforts to address HRSN in Medicaid. Specifically, our findings demonstrate the potential value proposition of care coordination and other services to address HRSN as strategies for reducing acute care utilization. Study findings also highlight key factors that may be critical for program success, including the importance of robust electronic data sharing infrastructure, adequate program investment, meaningful inclusion of cross-sector partners, and field-based outreach and engagement strategies.
As health care policymakers and payers’ interest in addressing patients’ unmet social needs as a strategy for improving health while controlling or reducing costs continues to grow, there is a need for additional evidence regarding which intervention and implementation strategies are most effective. Our study contributes to the literature by drawing on data from the statewide evaluation of a Medicaid Section 1115 waiver demonstration project focused on addressing HRSN to identify factors that differentiated programs that successfully reduced acute care utilization from those that did not. Findings highlight several partnership and program characteristics that may be important for reducing enrollee acute care utilization. Future research could assess factors associated with a broader array of program outcomes, such as program reach, cost, utilization of other services, or other health outcomes.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587241273404 – Supplemental material for Program Implementation Strategies Associated With Reduced Acute Care Utilization for Medicaid Beneficiaries in California’s Whole Person Care Pilot Program
Supplemental material, sj-docx-1-mcr-10.1177_10775587241273404 for Program Implementation Strategies Associated With Reduced Acute Care Utilization for Medicaid Beneficiaries in California’s Whole Person Care Pilot Program by Emmeline Chuang, Dahai Yue, Brenna O’Masta, Leigh Ann Haley, Weihao Zhou and Nadereh Pourat in Medical Care Research and Review
Footnotes
Acknowledgements
The authors thank Kelly Royan Rozier, Nadia Safaeinili, and Ammar Bhaiji for their assistance with conducting or analyzing key informant interviews and narrative reports used in this study, and Christine Lo for her assistance with compiling PY6 invoice data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the California Department of Health Care Services (DHCS) and by the Robert Wood Johnson Foundation Systems for Action program (RWJF S4A; #78115). The views expressed in the article are solely the opinion of the authors and do not necessarily reflect the official policies or endorsement of DHCS or RWJF S4A.
Research Ethics and Patient Consent
Study activities were approved by the Committee for the Protection of Human Subjects (Protocol ID #2018-030-UCLA), which serves as the Institutional Review Board for the California Health and Human Services Agency.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.