
Abstract
Health care organizations face growing pressure to improve their patients’ social conditions, such as housing, food, and economic insecurity. Little is known about the motivations and concerns of health care organizations when implementing activities aimed at improving patients’ social conditions. We used semi-structured interviews with 29 health care organizations to explore their motivations and tensions around social care. Administrators described an interwoven set of motivations for delivering social care: (a) doing the right thing for their patients, (b) improving health outcomes, and (c) making the business case. Administrators expressed tensions around the optimal role for health care in social care including uncertainty around (a) who should be responsible, (b) whether health care has the needed capacity/skills, and (c) sustainability of social care activities. Health care administrators could use guidance and support from policy makers on how to effectively prioritize social care activities, partner with other sectors, and build the needed workforce.
Background
Recognizing the links between social risk factors and health outcomes, policy makers have relied, de facto, upon health care organizations to deliver social care (Alley et al., 2016). Social care is when health care organizations aim to improve their patients’ social conditions (DeVoe et al., 2016; Gottlieb et al., 2019; Gurewich et al., 2020). Social care includes activities such as screening for social risks, providing referrals to community-based organizations (CBOs), assisting patients with accessing referrals, and partnering with CBOs to develop needs-based programs (National Academies of Sciences, Engineering, and Medicine, 2019). Increasingly, health care leaders report that it is important to integrate data on social needs into patient care (Eisenson & Mohta, 2020). Furthermore, more than two-thirds of primary care practices report screening patients for at least one social risk factor (Brewster et al., 2020; Fraze et al., 2019). At the same time that momentum is growing for health care organizations to implement social care (Eisenson & Mohta, 2020; Gottlieb et al., 2016, 2019; Gurewich et al., 2020; Maani & Galea, 2020; National Academies of Sciences, Engineering, and Medicine 2019), others have raised concerns that many social care activities have not yet been rigoursly tested (Abir et al., 2019; Berkowitz & Kangovi, 2020).
One significant challenge faced by health care organizations attempting to implement social care is that care transformation requires upfront investments by health care organizations (Leutz, 1999; Shortell, 2020). Developing and implementing social care likely requires health care organizations to significantly adapt clinic workflows, identify and train staff on social care delivery, and identify CBOs. Even if highly impactful, these investments still come at a cost. Opportunity costs are steep because health care leaders are faced with a constellation of evidence-based care transformation activities, spanning clinical decision-making, disease management, care management, and social care, which they can choose to implement at any given time (Berkowitz et al., 2017; Gottlieb et al., 2017; Kilsdonk et al., 2017; Lau et al., 2016; McCarthy et al., 2015). Furthermore, leaders may be hesitant to implement time or staff-intensive care delivery transformation activities as the health care workforce is already stressed (De Marchis, Knox et al., 2019; Farmer et al., 2014; Levesque et al., 2015; O’Malley et al., 2015; Weiner et al., 2019; Willard-Grace et al., 2014).
Another noteworthy integration concern centers around the impact of the organization spearheading the effort as organizations that lead integration efforts may hold more influence than those who participate in the integration effort (Leutz, 1999; Shortell, 2020; Steenkamer et al., 2020). Many social care activities, such as social risk screening and subsequent referrals to CBOs for assistance, may be predominantly driven by health care organizations while also relying on the expertise of others. These social care efforts may create an imbalance of influence between health care and local CBOs. Some scholars have highlighted concerns around health care driven activities creating a “savior-designed system” where the preferences of health care organizations are prioritized over the needs of patients and CBOs (National Institute for Children’s Health Quality, 2020b). As a result of these concerns, many have advocated for robust cross-sector collaborations that are cocreated by key organizations in the community, including, but not limited to, health care organizations (Bye & Ghirardelli, 2016; Fichtenberg et al., 2020; Hogg-Graham et al., 2021; Robert Wood Johnson Foundation, 2016; Towe et al., 2016). Meaningful cross-sector community-wide collaboration may be even more challenging than traditional care integration (and social care) efforts for health care organizations in terms of staff and leadership time, up-front investments, and ongoing efforts (Petchel et al., 2020). Even when community-wide, cross-sector collaborations are formed, health care may still spearhead efforts because social service sectors may lack the investment and support needed to lead collaboration efforts (Monroe, 2020).
New Contribution
Calls for health care organizations to deliver social care have grown as the coronavirus disease 2019 (COVID-19) pandemic has surfaced, highlighted, and heightened inequalities (Burström & Tao, 2020; Cartier et al., 2020a; Fichtenberg & Gottlieb, 2021; Kreuter et al., 2020; Peretz et al., 2020; Rangel et al., 2020; Rollston & Galea, 2020; Singu et al., 2020). At the same time, health care organizations are under unprecedented stress during the pandemic, given increasing patient needs and revenue shortfalls (American Hospital Association, 2020; Basu et al., 2020). Despite the momentum among policy makers and health care organizations to deliver social care, little is known about health care organizations’ motivations and tensions around social care delivery. Prior research has largely focused on specific efforts made by health care organizations (e.g., social risk screening or implementation of social care programs; Berkowitz et al., 2018; Cartier & Gottlieb, 2020; De Marchis, Torres, et al., 2019; Emengo et al., 2020; Fraze et al., 2019; Gottlieb et al., 2017; Schickedanz, Sharp et al., 2019) or has evaluated the perspective of clinicians and patients on the integration of social care into medical care (Byhoff et al., 2019; De Marchis, Hessler, et al., 2019; Hamity et al., 2018; Hsu et al., 2020; Schickedanz, Hamity et al., 2019). A deeper understanding of why health care organizations choose to deliver social care can help policy makers identify and refine optimal policy levers aimed at incentivizing social care. In this study, we address these gaps by interviewing a diverse, national set of health care organizations to learn about their motivations, concerns, and challenges to integrating social care into medical care.
Method
Data Collection
We conducted 33 semi-structured interviews with 29 health care organizations from April to July 2019. All interviewed organizations had known about social care programs that addressed food, housing, transportation, utilities, or other economic insecurity. This study was approved by the institutional review board at Dartmouth College.
We used two methods to identify organizations: (a) We randomly selected organizations that responded to the National Survey of Health Care Organizations and Systems (NSHOS) and indicated they screened patients for social risks, and (b) we conducted internet searches to identify organizations that were publicizing their social needs efforts (Dartmouth College, 2021). NSHOS is a suite of nationally representative surveys that were conducted from 2017 to 2018. For this study, we selected organizations from the NSHOS primary care practice and health care delivery system surveys because they uniquely included information on social risk screening from a diverse, nationally representative set of organizations. (Brewster et al., 2020; Briggs et al., 2019; Dartmouth College, 2021; Fisher et al., 2020; Fraze et al., 2019; King et al., 2020; Ouayogodé et al., 2020). For this study, we sampled respondents to the NSHOS practice and health care system surveys.
We emailed leaders at sampled organizations and asked them to connect us with the individual at their organization who was best suited to speak with us about their efforts to address patients’ social needs. While interviewees had varying titles, we aimed to interview the individual responsible for administering implementation of social care activities (Table A1 includes information on interviewees). We conducted outreach in waves to ensure a diverse sample and, in total, contacted 64 organizations of which 29 organizations replied and participated (Tables A2, A3, and A4 summarize all sampled organizations and provide characteristics of participating organizations). In some organizations, the initial interviewee connected us with an additional interviewee (usually frontline staff) for more detailed information; we conducted four such additional interviews (Table A4).
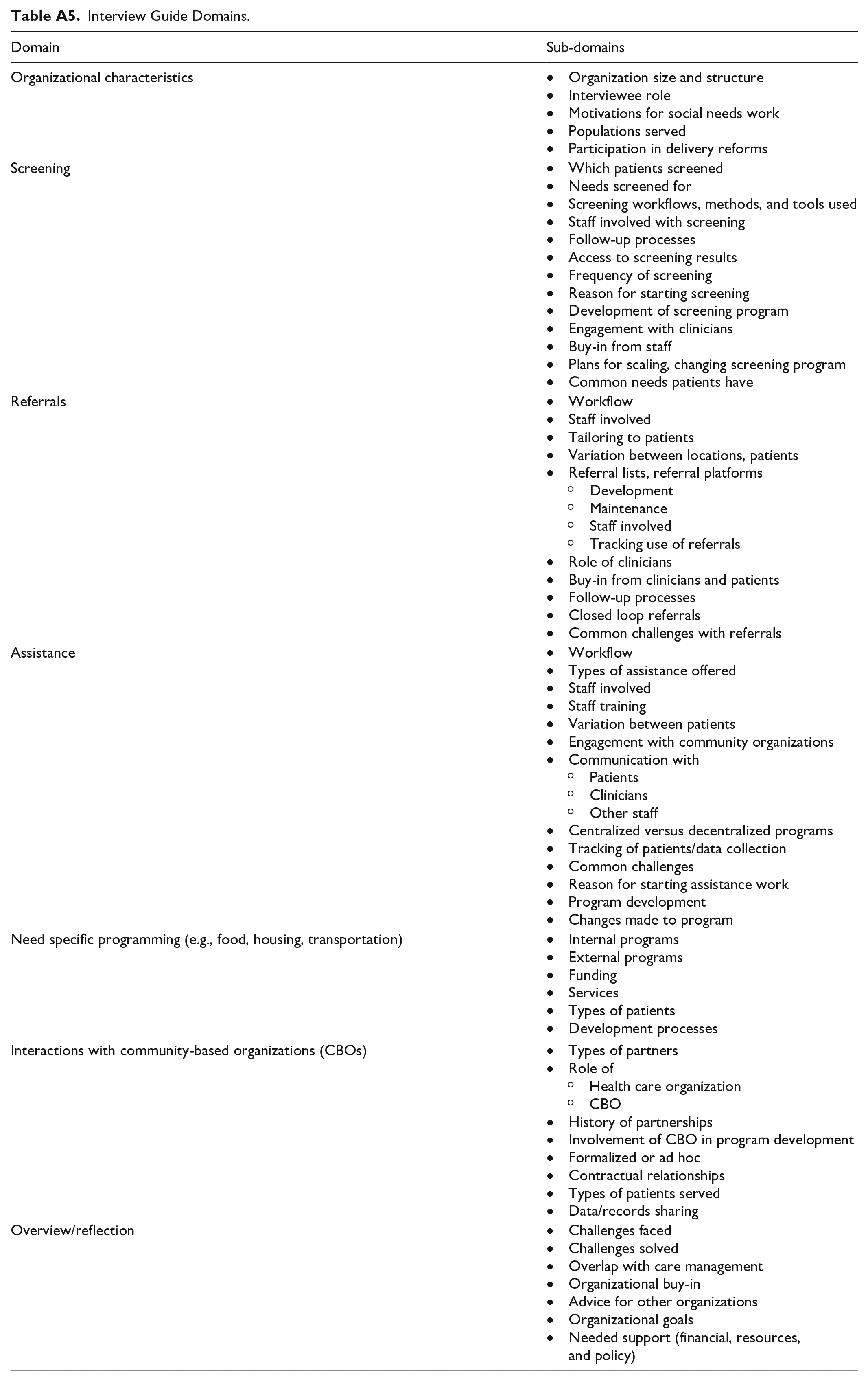
Interviews focused on activities that aimed to identify and address patients’ social needs. Semi-structured interviews followed an interview guide that included topics related to (a) organizational characteristics, (b) social risk screening, (c) referrals, (d) other activities for patients with social needs, and (e) interactions with CBOs (Table A5). All interviews lasted approximately 60 min, were conducted through telephone and recorded, and then were professional transcribed.
Data Analysis
Trained qualitative researchers coded transcripts, using an established codebook that was aligned with domains in the interview guide and used a grounded approach (Scott & Howell, 2008). All coding was conducted using QSR NVivo (QSR International Pty Ltd, 2014). All coders (T.F., L.B., and a trained research assistant) conducted iterative double coding until all coders and lead author agreed and were confident about the consistency between coders (Miles et al., 2014). Then, for all transcripts, the research assistant conducted initial coding and L.B. conducted an unblinded second pass at coding. For this article, we conducted analysis-specific coding on the motivations and concerns that administrators reported about their social care programs. One team member (L.B.) sub-coded all transcripts and the lead author (T.F.) reviewed the sub-coded data. We (L.B. and T.F.) met weekly to discuss coding. We analyzed coded data using an iterative approach and created a detailed memo that explored the motivations and tensions within each organization. We used the matrix coding approach to examine how each organization fit within each theme (Corbin & Strauss, 2008; Glaser, 2014; Scott & Howell, 2008). Figure A1 provides an overview of our analytic approach.
Results
Overview
Interviewed organizations were diverse in size, ownership, and geography (Tables A3 and A4). All interviewed health care organizations had specific organizational efforts that aimed to improve patients’ social conditions.
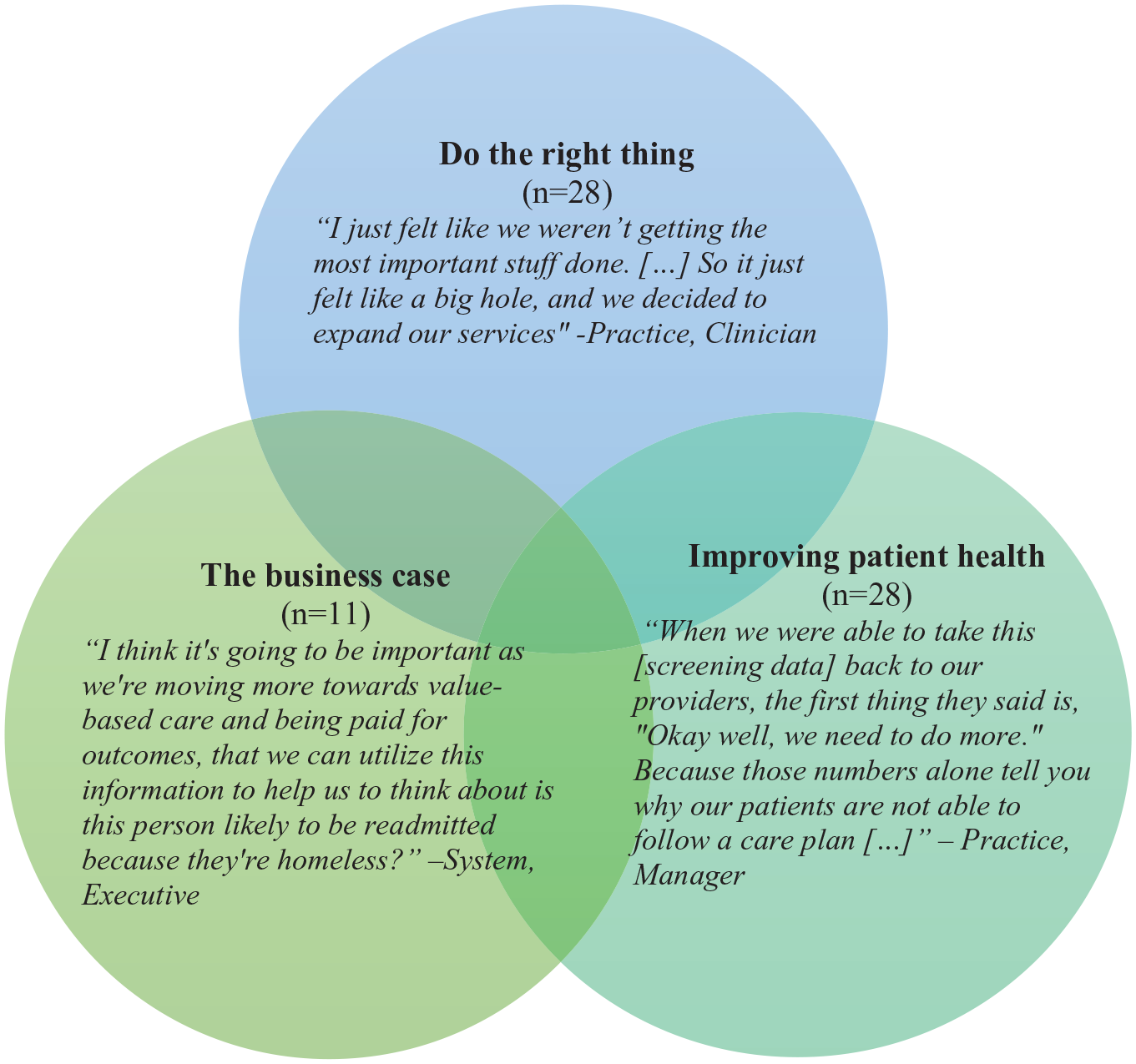
Administrators and frontline staff alike recognized the impact of social needs in their patients’ lives and on their health outcomes. Administrators described a complex and interwoven set of motivations for acting on that recognition, including (a) doing the right thing for their patients, (b) improving health outcomes, and (c) making the business case (Figure 1). This set of interconnected motivations likely interacted to catalyze organizations into developing social care programs. As one administrator explained, “it’s not just the right thing to do, but it’s a survival tactic” (System, Executive). At the same time, despite having compelling motivations for delivering social care, administrators expressed tensions around the optimal role for health care in delivering social care, including uncertainty in terms of (a) who should ideally be responsible, (b) whether health care has the needed the capacity or appropriate skills, and (c) whether their social care activities were sustainable (Table 1). We did not observe differences in either motivations or tensions by organizational type (e.g., size, rurality, ownership, or geography).
Motivations for Health Care Organizations When Delivering Social Care.
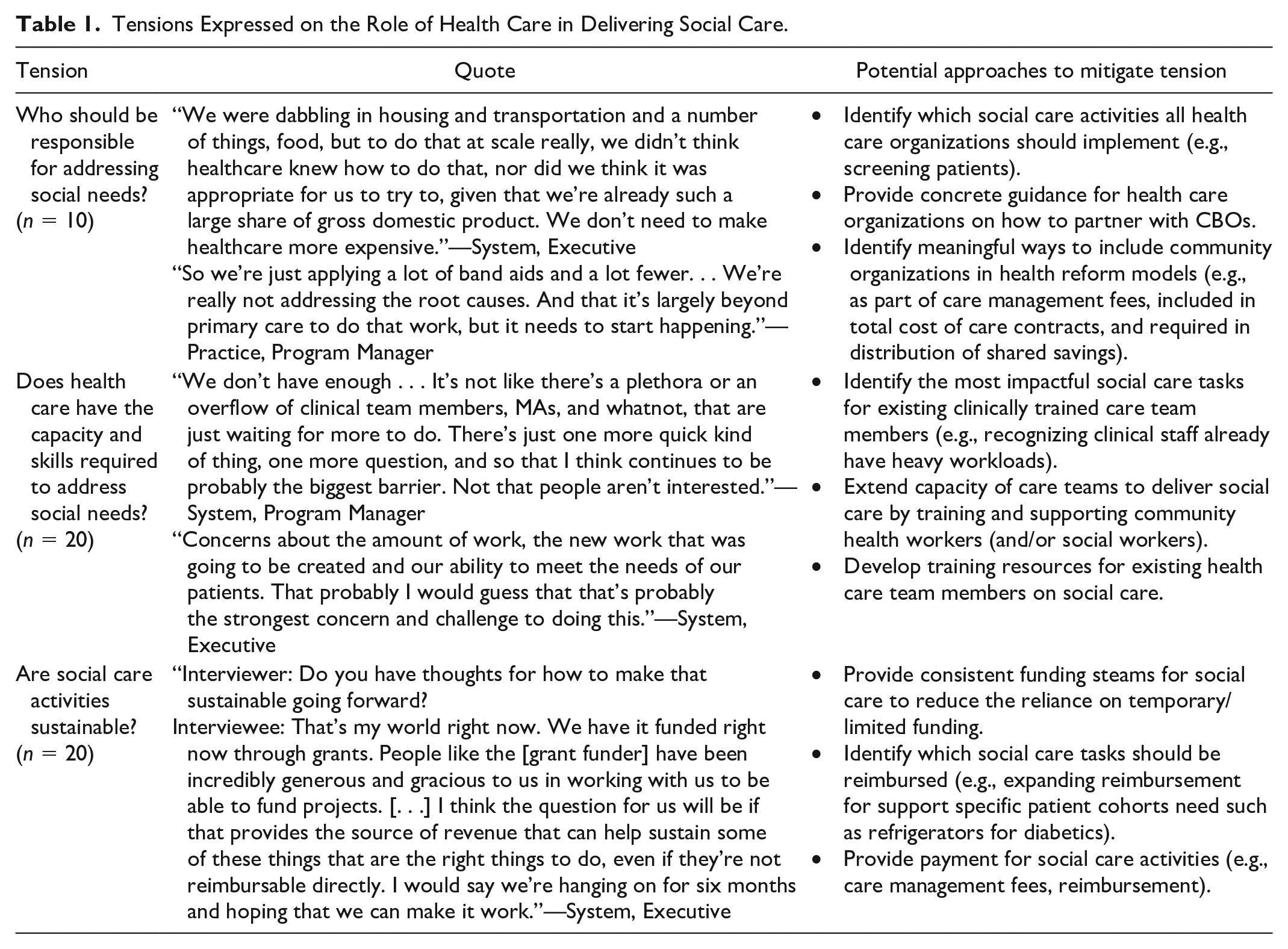
Tensions Expressed on the Role of Health Care in Delivering Social Care.
Motivation: “Doing the Right Thing”
A strong motivator for health care organizations to engage in social care was the desire to do what was right for their patients (n = 28). Administrators saw needs in their patients’ lives and felt compelled to help. Their intentions to provide holistic, patient-centered care drove their efforts to address social needs. As one administrator explained, “We knew that it was going to take more than great health care to really address the needs for the population” (System, Executive).
Administrators often felt there was a gap in that a patient’s needs were not being effectively met by another organization and, as a result, they felt compelled to “do something” and help fill that gap: Someone needs to be the quarterback. Someone needs to organize and make sure that needs are being met, referrals are happening, that there’s a response system in place if things go wacky. (System, Executive)
This coordination often fell to care managers or other primary care staff, and administrators often emphasized that staff embarked on this work out of a sense of compassion for their patients.
Motivation: Improving Health Outcomes
Along with the ethical motivation to help patients, administrators also emphasized that addressing the social needs of their patients was key to improving patients’ overall health (n = 28). In some instances, social needs were viewed as directly impairing the patient’s ability to adhere to their care plan. For example, addressing transportation gaps were seen as important for patients who required frequent care, and addressing food insecurity was highlighted as a priority when caring for patients with diabetes or other chronic diseases. Administrators noted that patients might not adequately manage health conditions until social needs were first addressed: If there is something that is preventing a person from a good quality health, or preventing them from getting to their physician’s appointments, getting to tests, getting to their medications, if they have financial difficulties. . . in other words what we’re doing is financially, socially, health-wise. What we want to do is help fill those gaps. (Practice, Case Management Staff)
Motivation: Making the Business Case
The final motivation revolved around the potential business case for social care (n = 11). Interviewees recognized that their motivations were multifaceted. Administrators not only wanted to “do the right thing” and improve patients’ health outcomes, but they also noted that the business case was also imperative. As one administrator explained, We’re having to introduce this as a business imperative, that it’s not . . . Yes, it’s the right thing to do on any given day and I wish I could have done it 20 years ago. But we are now talking about what are the things that we’re going to have to do so that we can make sure that we are covering all the bases as we’re looking at moving towards being paid for outcomes. (System, Executive)
While there are currently few financial incentives for health care organizations to address social needs, many hoped that their social care efforts would become financially sustainable. Some organizations that participated in alternative payment contracts believed that the up-front costs associated with implementing social care might be offset by reductions in total costs of care. For example, one administrator described potentially using hotels to house patients who did not require costly hospital care but could not be discharged because they did not have an adequate home environment. This would improve hospital flow and free up hospital beds for patients with greater needs.
Administrators were hopeful that their investments in social care activities would be offset in the future through payment and delivery reform (e.g., enhanced care management fees or other adjustments to payment due to patients’ social risks/complexity). For example, one organization used Z codes, which are International Classification of Diseases, Tenth Revision (ICD-10) diagnosis codes that allow clinicians to document social needs such as housing, because they hoped that these codes would eventually be leveraged by payers: We also recognize that there’s great value in that at least being able to describe our patient population well. If we have these less than desirable clinical outcomes, what else was going on here and to be able to actually risk adjusted according to income and other social determinants is very helpful. Also in terms of negotiating with payers, Medicare and increasingly the commercial payers are looking into the stuff. (System, Manager)
Tension: Who Should Be Responsible for Addressing Social Needs?
While concern for patients’ social needs compelled health care organizations to act, they also described their role in delivering social care as one born out of necessity (n = 10). Health care administrators described their actions in delivering social care as “stepping up” and filling a critical gap that could improve their patients’ lives. Some struggled to reconcile their desire to improve patients’ social conditions with concerns on when and how health care should optimally be involved. As one administrator explained, when their organization considered providing housing support, And I’m like, so a delivery system solving the housing problem would be the most expensive way and the stupidest way because we know nothing about housing, but there are these community-based organizations that know and have the wherewithal. (System, Executive)
Many administrators recognized that CBOs have deep expertise in addressing social risks and were likely better positioned to improve social conditions. However, CBOs also face significant challenges, given they have limited resources and are often chronically underfunded. Recognizing the limitations of CBOs, some administrators wondered whether it would be more effective for them to provide financial support to local CBOs. For example, one administrator noted that they were purchasing computers to help CBOs engage with referral platforms. Another brainstormed that it would be ideal to partner with local CBOs and provide them with financial support to meet patients’ social needs. She described this idea by saying that the CBO “works with the patient, the patient then identifies stable housing. They achieve stable housing solution for three months and then we pay [partner CBO]” (System, Executive).
Tension: Does Health Care Have the Needed Capacity and Appropriate Skills to Address Social Needs?
On a more pragmatic level, health care administrators worried about their capacity and ability to effectively address social needs (n = 20). Administrators frequently noted that primary care teams have limited time, knowledge, and experience to deliver social care because care teams were already overburdened and sometimes hesitant to assume new responsibilities.
In addition, some administrators faced resistance from care team members around social care. Care team members may be reluctant because of their lack of expertise or they may be uncomfortable discussing patients’ personal social situations. Clinicians were sometimes hesitant to conduct social risk screening when they felt that health care’s ability to resolve social needs was inadequate. One clinician leader described their discomfort: The problem is if you screen for it there’s an inherent accountability in responding to that. That is terrifying for all of us who take care of patients. If I screen for the fact that you’re homeless and I have, what am I supposed to do as a primary care doctor to get you a home? You know, I’m not trained to do that and you can say refer to a social worker, but many of our clinics don’t have the community health workers or the social workers in supply that are needed to meet patient needs. (System, Executive and clinician)
Tension: Are Social Care Activities Sustainable?
Finally, administrators were particularly concerned about whether their social care activities were sustainable (n = 20). They described concerns around sustainability in terms of (a) isolating which aspects of social care health care should lead versus other community organizations, (b) identifying which social care activities to prioritize while the business case solidifies, and (c) determining which social care activities they should continue.
Balancing the role of health care in social care programming was important to administrators—they grappled with determining which programs they should spearhead and which programs they should support but not manage. They wanted to build programs that were impactful and sustainable, but effectively focusing their role was a key challenge. As one leader described, For me, what I’m always constantly looking for is if there is somebody that’s in the community that’s doing the work, and it’s meeting the needs of the patient, then I don’t need to duplicate what’s existing in the community. If there is a gap in what our patients need, then that’s a potential place for us to step forward and lean in. (System, Executive)
While health care administrators were hopeful that investing in social care would be offset in the future, they struggled to justify programs in the interim. One administrator emphasized this by saying, “I think the key thing is how do we pay for this. I think that’s got to be on the top of everyone’s list right now” (System, Executive).
Finally, health care administrators were weighing which social care activities to continue. With a few notable exceptions, most social care programs were not proactively developed as part of a larger organizational (or community-based) strategy but were more typically reactively developed to respond to pressing patient needs. Administrators tried to balance their desire to care for their communities, the health benefits of social care, and the financial viability of programs.
Discussion
Interviewed health care administrators described a complicated and interwoven set of motivations for delivering social care. Our study suggests that health care administrators have found research demonstrating the links between social risk factors and health outcomes compelling. Administrators described social care as aligned with their mission and the “right thing” to do for their patients. Importantly, administrators were also strongly motivated to ensure there was a sufficient business case for social care delivery.
Health care administrators’ concern around ensuring there was a sufficient business case for social care was not surprising, given limited options for reimbursement. In a largely fee-for-service world, the business case is hard to make in isolation because any savings associated with reduced utilization is passed on to the insurer and the patient, whereas the cost of any intervention is covered by the delivery system. Health care administrators argued that delivering social care is a forward-thinking measure and that payers would eventually support their efforts.
Indeed, health care organizations’ early investment in developing and implementing social care programs may pay off. In 2018, the Department of Health and Human Services signaled their interest in expanding the role of health care in delivering a much broader range of services to combat social adversity (Azar, 2018; Joszt, 2018). And, as of 2020, Medicare Advantage plans have greater flexibility to improve patients’ social conditions through supplemental benefits, such as home modifications and meal delivery services post-discharge (Meyers et al., 2020). The American Medical Association recently announced significant modifications to outpatient evaluation and management codes (American Hospital Association, 2019). Beginning in 2021, clinicians can consider a patient’s social risk factors when determining medical complexity (American Hospital Association, 2019; American Medical Association, 2019; Gottlieb & Desilvey, 2020). Less than 2% of hospital admissions from 2016 to 2017 were coded for social risk factors (Truong et al., 2020), but these changes may serve as a significant motivator for health care organizations to screen patients for social risk factors across care settings.
Yet our study suggests that even with aligned financial incentives, significant uncertainty will remain around how to optimally integrate social care into medical settings. Health care could benefit from greater guidance on how to prioritize and implement social care activities: Should their early efforts focus on ways clinicians can adjust treatment plans for patients with social risk factors, should they serve more of a connector role between patients and CBOs, or should they consider standalone programs to directly impact social conditions (e.g., providing meals, transportation)? Policy makers can help health care focus these efforts.
A significant concern about social care within medical settings is ensuring a sufficient workforce. Health care teams, especially within primary care, already report high levels of burnout amid increasing workloads caring for patients with complex needs (De Marchis, Knox et al., 2019; Kung et al., 2019; Olayiwola et al., 2018). Community health workers and social workers have served as a bridge between health care delivery and CBOs (Kangovi et al., 2014, 2020; Ross & de Saxe Zerden, 2020). Policy makers could consider how to support the pipeline and integration of community health workers (or social workers) through training or certification programs and reimbursement for their social care activities. If existing care team members—from medical assistants to nurses to clinicians—are to deliver social care, then training for these team members is needed as well. Care teams are typically clinically trained with limited expertise on how to respond to and address patients’ social needs. A recent survey found that most clinicians did not feel confident they could address patients’ social needs (Schickedanz, Hamity et al., 2019). There are efforts to fill this gap in training; for example, the new Kaiser Permanente School of Medicine has incorporated required service-learning experiences as part of its medical school curriculum (Kaiser Permanente Bernard & Tyson School of Medicine, 2020).
Alternatively, should policy makers instead invest directly in the needed public health and social welfare efforts that focus on wellness and health of the population? The United States chronically spends less on social sectors, more on health care delivery, and has poorer outcomes compared with other countries (Bradley & Taylor, 2013; McCullough et al., 2020). Upstream investments in social welfare would address one significant concern—that health care directed interventions are targeted at patients with access to sick care, leaving out individuals with limited interaction with the health care system. One support could be to invest in community-wide systems to centralize information about community resources (Cartier et al., 2020b). Furthermore, administrators recognized that centering social care activities in medical settings is likely costly, inefficient, uneven, and potentially less effective than having other sectors (i.e., CBOs) lead efforts. Policy makers could catalyze cross-sector efforts such as the anchor institution movement where health care delivery systems and universities have recognized their community influence and have committed to investing in local economies (Koh et al., 2020). These efforts not only leverage the influence of health care organizations but also acknowledge that the health care delivery sector should be part of larger efforts to improve health, well-being, and economic security within communities (Koh et al., 2020). At the same time, health care organizations could benefit from guidance on how to deliver social care in a manner that squarely centers their efforts on the needs of the local community, as defined by the community, rather than on health care’s perceptions of community needs (National Institute for Children’s Health Quality, 2020a).
Our study had key limitations. First, most of our data was from the perspective of the administrators and may not represent the view of all clinicians at the organization. Health care administrators are well-poised to provide details on the organizational strategy and approach to formal social care efforts. Although NSHOS provided a robust sample of organizations, some organizational types may not have been included. In addition, interviews should not be generalized to all health care organizations, rather they should provide context on how health care organizations view their role in providing social care.
Although we have not yet determined the optimal role for health care in helping to improve patients’ social adversity, increasingly, there is agreement among policy makers and health care leaders that social risk screening should be integrated into medical care (Alley et al., 2016; Azar, 2018; Bees, 2020; Eisenson & Mohta, 2020). The pandemic spurred by COVID-19 has dramatically increased poverty as unemployment, and, in the face of mandatory distancing efforts, social isolation, has soared, which will likely have lasting effects (Banerjee & Rai, 2020; DeParle, 2020). Given these growing needs, it is likely that health care will increase their efforts to address patients’ social risks. Yet health care’s efforts to deliver social care may not be sustainable, given limited and developing funding streams and a lack of guidance on how to implement social care activities in partnership with communities. Understanding the motivations and uncertainties that health care leaders experience when implementing social risk interventions will help policy makers and payers refine their approaches.
Footnotes
Appendix
Interview Guide Domains.
| Domain | Sub-domains |
|---|---|
| Organizational characteristics | • Organization size and structure • Interviewee role • Motivations for social needs work • Populations served • Participation in delivery reforms |
| Screening | • Which patients screened • Needs screened for • Screening workflows, methods, and tools used • Staff involved with screening • Follow-up processes • Access to screening results • Frequency of screening • Reason for starting screening • Development of screening program • Engagement with clinicians • Buy-in from staff • Plans for scaling, changing screening program • Common needs patients have |
| Referrals | • Workflow • Staff involved • Tailoring to patients • Variation between locations, patients • Referral lists, referral platforms ° Development ° Maintenance ° Staff involved ° Tracking use of referrals • Role of clinicians • Buy-in from clinicians and patients • Follow-up processes • Closed loop referrals • Common challenges with referrals |
| Assistance | • Workflow • Types of assistance offered • Staff involved • Staff training • Variation between patients • Engagement with community organizations • Communication with ° Patients ° Clinicians ° Other staff • Centralized versus decentralized programs • Tracking of patients/data collection • Common challenges • Reason for starting assistance work • Program development • Changes made to program |
| Need specific programming (e.g., food, housing, transportation) | • Internal programs • External programs • Funding • Services • Types of patients • Development processes |
| Interactions with community-based organizations (CBOs) | • Types of partners • Role of ° Health care organization ° CBO • History of partnerships • Involvement of CBO in program development • Formalized or ad hoc • Contractual relationships • Types of patients served • Data/records sharing |
| Overview/reflection | • Challenges faced • Challenges solved • Overlap with care management • Organizational buy-in • Advice for other organizations • Organizational goals • Needed support (financial, resources, and policy) |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was provided, in part, by the Robert Wood Johnson Foundation (Grant ID: 75770). This work was supported, in part, by Agency for Healthcare Research and Quality’s (AHRQ) Comparative Health System Performance Initiative under Grant No. 1U19HS024075, which studies how health care delivery systems promote evidence-based practices and patient-centered outcomes research in delivering care. The views expressed here do not necessarily reflect the views of the Robert Wood Johnson Foundation or AHRQ.