
Abstract
Primary care practitioners (PCPs) are the first point of contact for most patients with suspected dementia and have identified a need for more training and support around dementia diagnosis and care. This qualitative study examined the Alzheimer’s Disease–Extension for Community Healthcare Outcomes (AD-ECHO) program. AD-ECHO was designed to strengthen PCP capacity in dementia through bimonthly virtual meetings with a team of dementia experts. We conducted 24 hr of direct observations at AD-ECHO sessions and interviewed 14 participants about their experiences participating. Using thematic analysis, we found that participants valued the supportive learning environment and resources; knowledge gained empowered them to take more action around dementia; they identified ways of disseminating knowledge gained into their practice settings, and many desired ongoing AD-ECHO engagement. However, most identified time as a barrier to participation. AD-ECHO has the potential to strengthen the primary care workforce’s knowledge and confidence around dementia care.
Introduction
More than 6 million people live with Alzheimer’s disease and related dementias (ADRDs) in the United States, a number that is expected to triple by 2050 (“2023 Alzheimer’s Disease Facts and Figures,” 2023). Primary care practitioners (PCPs) are the first point of contact for most patients with suspected ADRD, yet as many as 66% of patients in primary care are not diagnosed in the early stages of the disease (Boustani et al., 2003). PCPs report a lack of familiarity with evaluation tools, issues of time, difficulty accessing specialists, difficulty getting reimbursement, difficulty connecting with service agencies, and lack of confidence managing patient and family preferences, as barriers to providing quality dementia care (Bernstein, Rogers, Possin, Steele, Ritchie, Kramer, et al., 2019; Bernstein, Rogers, Possin, Steele, Ritchie, Miller, & Rankin, 2019; Borson et al., 2013; Bradford et al., 2009). One study found that only about 20% of PCPs feel confident in recognizing dementias, and only 20% feel comfortable using and interpreting standardized tests to assess cognitive complaints and discuss the diagnosis and management with patients (Bernstein, Rogers, Possin, Steele, Ritchie, Kramer, et al., 2019; Bernstein, Rogers, Possin, Steele, Ritchie, Miller, & Rankin, 2019). Furthermore, there is a shortage of neurology and geriatrics specialists compared with the size of the population needing evaluation and care for these diseases. More work is thus needed to build and strengthen primary care workforce capacity to manage the rising number of patients with ADRD.
One approach to addressing this workforce challenge is Alzheimer’s and Dementia Care–ECHO (Extension for Community Healthcare Outcomes), or AD-ECHO, a certified Project ECHO training program developed as a collaboration between University of California, San Francisco (UCSF) and the Alzheimer’s Association. Project ECHO was established in 2003 in New Mexico to support PCPs, including rural clinicians, who have limited access to specialists, to provide quality care to their patients with Hepatitis C. Project ECHO involves a hub-and-spoke model of education and consultation, with a central group of specialists supporting a group of community practices through synchronous moderated virtual meetings. During these meetings, specialists typically provide didactics, or brief educational sessions, alongside the presentation of de-identified cases by primary care participants. Cases are discussed by the specialists and primary care participants, and PCPs receive recommendations and resources (Arora et al., 2007, 2017a, 2017b; Robert Wood Johnson Foundation, 2014; Sequist et al., 2011). The program has now expanded to a multitude of disease areas and patient populations and is a nationally renowned model of specialty care in rural, low-income, and underinsured areas of the United States.
In March of 2021, the Alzheimer’s Association initiated a California-based Project ECHO for dementia program in collaboration with the UCSF. AD-ECHO recruitment targets primary care practices caring for underserved populations and enables primary care teams to provide dementia expertise within their practice settings. Participants are PCPs from multiple disciplines, including physicians, nurses, social workers, psychologists, and physical therapists. The purpose of this study was to use qualitative research to assess the primary care workforce implications of participation in AD-ECHO. Building PCP capacity in dementia diagnosis and care is a major priority for improving access to quality dementia care.
AD-ECHO Program Description
UCSF’s AD-ECHO was developed in coordination with the Alzheimer’s Association Project ECHO team. The hub team of specialists in neurology, geriatric psychiatry, neuropsychology, social work, and nursing developed a series of 12 didactic presentations focused on content areas ranging from the biology of dementia to red flags and referrals and management of behaviors (see Table 1 for full list of topics). Community primary care practice partners formed the spokes, participating, for free, in twice monthly sessions conducted through Zoom videoconferencing over the course of 6 months. Each AD-ECHO session began with a 10-min didactic lecture followed by a 50-min discussion of real cases that were submitted by PCPs to highlight challenges they faced in practice. The team of specialists and community practice participants reviewed and discussed the cases together, identified recommended approaches for management, and jointly identified strategies for implementing the standard of care. The AD-ECHO program manager, in coordination with the Alzheimer’s Association, shared a curated set of resources, with additional tailored resources provided after each session based on questions that arose during the case review. These resources included the Alzheimer’s Association Toolkit and the Assessment of Cognitive Complaints Toolkit for Alzheimer’s Disease (ACCT-AD), developed by the California Alzheimer’s Disease Centers. Participants received 1 CME credit for their participation.
Alzheimer’s and Dementia Care ECHO Topics.
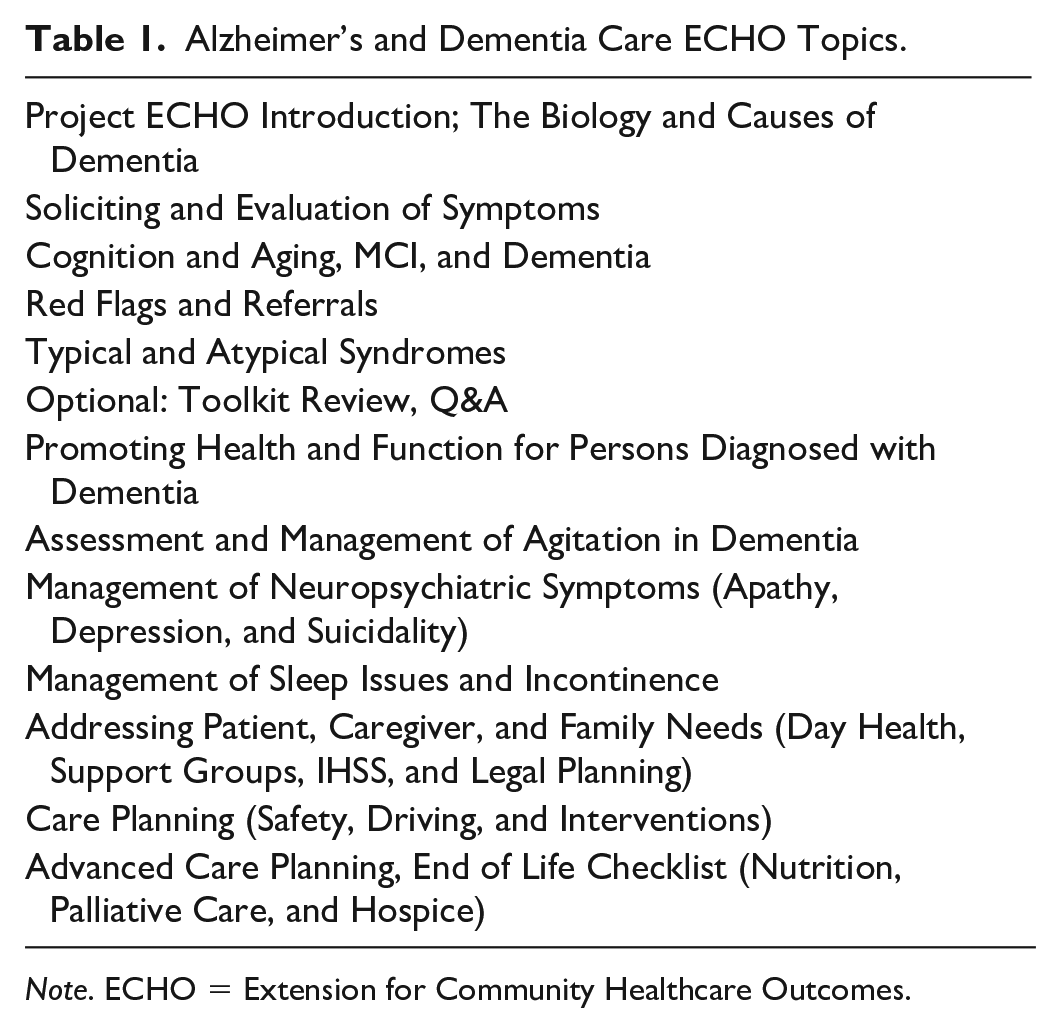
Note. ECHO = Extension for Community Healthcare Outcomes.
New Contribution
Although Project ECHO has been studied across multiple different clinical settings, this study examines a more recent iteration, AD-ECHO, focused specifically on ADRDs, at a time when the population with dementia is rapidly growing and new FDA-approved disease-modifying treatments have just become available (Cummings et al., 2022, 2023). Using qualitative methodology, including direct observations of 24 AD-ECHO sessions and in-depth interviews, this study provides insights into the content of the AD-ECHO program, its operations in practice, and the experiences of PCPs who participated. Understanding these aspects of AD-ECHO can provide a framework and recommendations for improving and expanding this and other similar training programs to address the critical health workforce needs surrounding the primary care of dementia.
Conceptual Framework
We draw on Moore et al.’s conceptual framework for assessing learning in clinician- and clinical-team–focused continuing education activities (Moore et al., 2009, 2018). This model was used in the development of Project ECHO to help define the structure for the continuing education approach, and for thinking about desired outcomes across several levels of clinician-focused learning. This model has also been used in prior studies of other Project ECHO programs (Agley et al., 2021; Arora et al., 2017b; Holmes et al., 2020; Sockalingam et al., 2018; Zhou et al., 2016). The AD-ECHO program set out to achieve a variety of outcomes for providers, including increases in knowledge, competence, and performance. Our results touch on aspects of several of Moore’s levels, including participation, satisfaction, learning, competence, and impact on performance in practice, with data from this qualitative study reporting participants’ perceptions and experiences. Table 2 identifies the ways we assessed each of these levels. Although the goals of Project ECHO programs are ultimately to affect patient health outcomes and population health, we did not explicitly measure these outcomes in this study.
Moore et al.’s Framework for Assessing Learning in Continuing Education Activities.
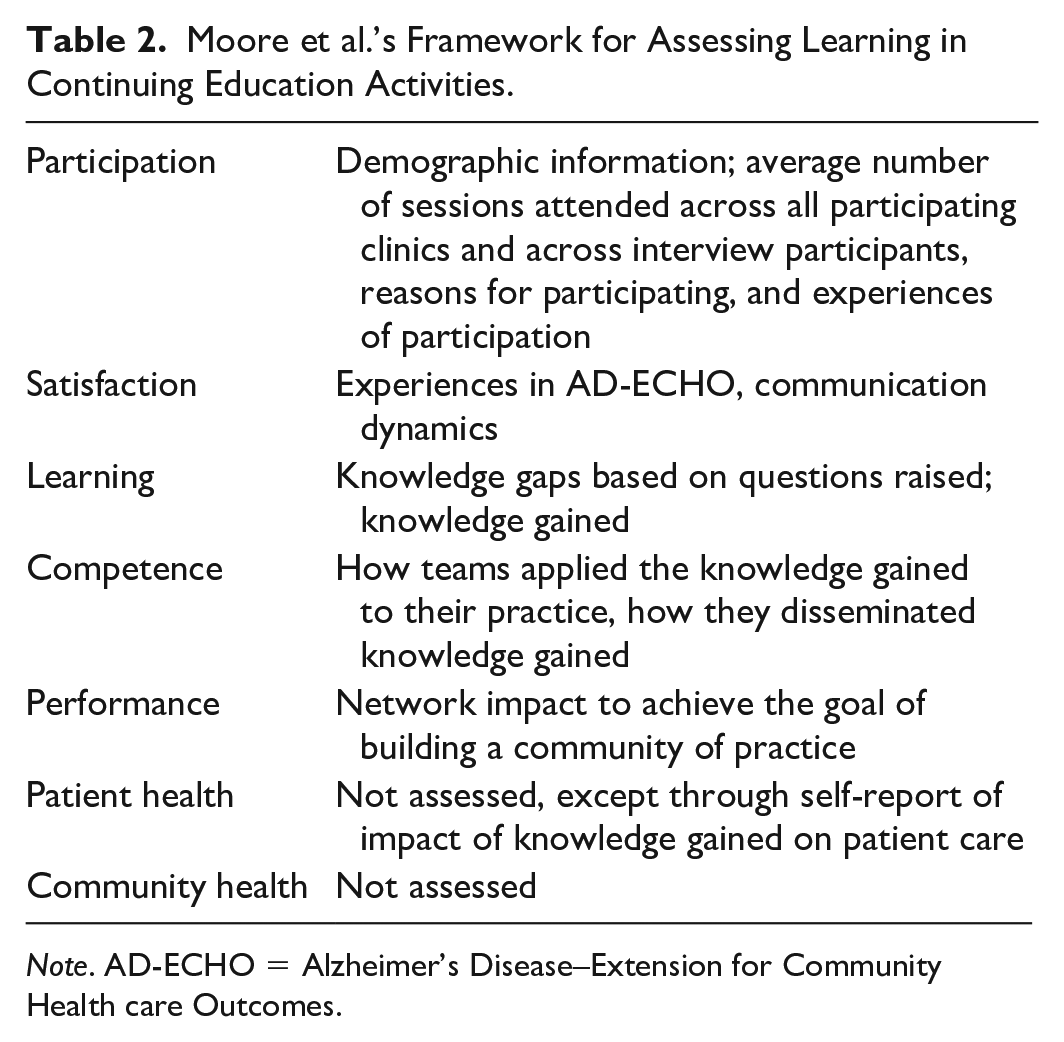
Note. AD-ECHO = Alzheimer’s Disease–Extension for Community Health care Outcomes.
Study Design and Method
The research protocol for this qualitative study was approved by the University of California San Francisco Institutional Review Board study no. 20-29974. We followed guidelines developed in the Standards for Reporting Qualitative Research (SRQR; O’Brien et al., 2014).
Observational Data Collection
We conducted 24 hr of direct observations during two AD-ECHO series comprising a total of 24 sessions that included 27 participating clinics and 149 participants (i.e., those who attended at least one session). Observers (AH, MM) took structured field notes during observations, using an observation template. The observation template asked observers to provide reflections on verbal and nonverbal dynamics, such as emotional responses, communication dynamics, specific topics discussed during case presentations, and reflections. The observers also documented every question raised by the community of PCPs during the sessions, both spoken and in the Zoom chat.
Interview Data Collection
Recruitment emails were sent by the Alzheimer’s Association and Project AD-ECHO coordinators to all 149 participants in the AD-ECHO trainings. Following oral consent, we conducted semi-structured interviews (n = 14) of 30 to 60 min with primary care participants. The same interview guide was used for all participants, and interview domains focused on their practice setting and experiences with AD-ECHO, including knowledge gained, impact on patient care, dissemination of what was learned, impact on clinician networks, communication dynamics during AD-ECHO sessions, challenges encountered, and future directions (see Supplemental Material for interview guide). Interviews were conducted by a medical anthropologist (ABS). Following each interview, a memo was created using a structured template to document notes summarizing respondent description and practice setting, big takeaways from the interview, and experience with AD-ECHO. The interviewer also documented initial ideas about patterns seen in the data that were used to develop the codebook. Interview participants self-reported demographic information.
Data Analysis
Observations
Two observers (AH, MA) compared and consolidated their observation notes from the 24 sessions and created a summary of reflections at the end of each session. From these observation notes and logs from the Zoom chat, they abstracted all questions asked to the specialists by primary care community participants. In this article, we focus on the questions documented during session observations and we triangulate interview findings with observational insights to provide additional context for these findings. The observers imported all questions from observations and chat into an Excel spreadsheet. They analyzed and categorized the questions by content (e.g., medical management, diagnostic workup). The study’s principal investigator (PI) (ABS) and observers (AH, MM) met weekly to discuss and refine the categories. The two observers developed a list of examples within each category and then calculated the frequency of questions within each category across all 24 sessions.
Interviews
Three researchers (ABS, AH, MM) familiarized themselves with the data by reviewing the interview memos and transcripts. They created a codebook of seven deductive codes to begin to develop findings. Deductive coding involved applying preexisting categories from our study’s goals and theoretical framework to designate overarching areas of interest. Deductive codes included the following: AD-ECHO experience, knowledge gained, impact on patient care, dissemination (existing or planned), network impact, communication dynamics, and challenges. The team conducted deductive and inductive coding of three interview transcripts together in ATLAS.ti, a qualitative data analysis software, to establish agreement in coding approach and code definitions. Inductive coding identifies codes from within the data and, for this project, were developed as subcodes under the deductive codes to help us refine and expand on the deductive coding framework. For example, under “AD-ECHO experience” we created inductive codes “support,” “empathy,” and “validation” to illustrate specific aspects of our participants’ experiences in AD-ECHO that were ultimately developed into the theme “the value of cultivating a supportive learning environment.” The researchers AH and MA divided the remaining transcripts and independently coded all data, double coding four transcripts. ABS reviewed coded data by extracting quote reports and reviewing reports for concordance with code definitions. The team met weekly to review coding and resolve discrepancies through consensus. The team reviewed all codes, quotes, and memos, and used these to develop key findings for the article and exemplary quotations, and then organized findings according to Moore et al.’s framework.
Results
Through analysis of interview and observational data, we report on PCP perspectives on participation AD-ECHO. We structure our results according to Moore et al.’s framework for assessing learning in continuing education activities. We found that, although PCPs had varied reasons for joining AD-ECHO, they greatly valued the cultivation of a supportive learning environment. Many were empowered to do more for their patients because of knowledge gained, and they identified specific areas of knowledge that were most valuable. They identified the values, and challenges, of resources provided, but most found creative ways to disseminate AD-ECHO knowledge learned into their practice settings. Many desired ongoing engagement with the AD-ECHO network although they found it challenging to fit AD-ECHO into busy practice schedules. We provide details of these findings and exemplary quotations below.
Participation
Engagement
Between March 2021 and April 2022, two consecutive series of AD-ECHO were held, with 12 sessions per series, or a total of 24 sessions. There were 27 participating clinics across both series, with 149 total participants, and 56 participants who attended 50% or more sessions. Cohort 1 involved 15 clinics with 99 registered participants and 36 who attended 50% or more sessions. Cohort 2 involved 12 clinics with 61 registered participants and 20 who attended 50% or more sessions. Interview participants attended an average of seven sessions, whereas participants across all participating clinics attended an average of nine sessions. Case presentation topics were determined by the presenting PCP. Topics primarily focused on medications, support for the family, behavior modification, and resources in the community (e.g., Adult Day Health, In-Home Supportive Services [IHSS] program support). A total of 24 cases were presented across the two cohorts (14 in Cohort 1, 10 in Cohort 2).
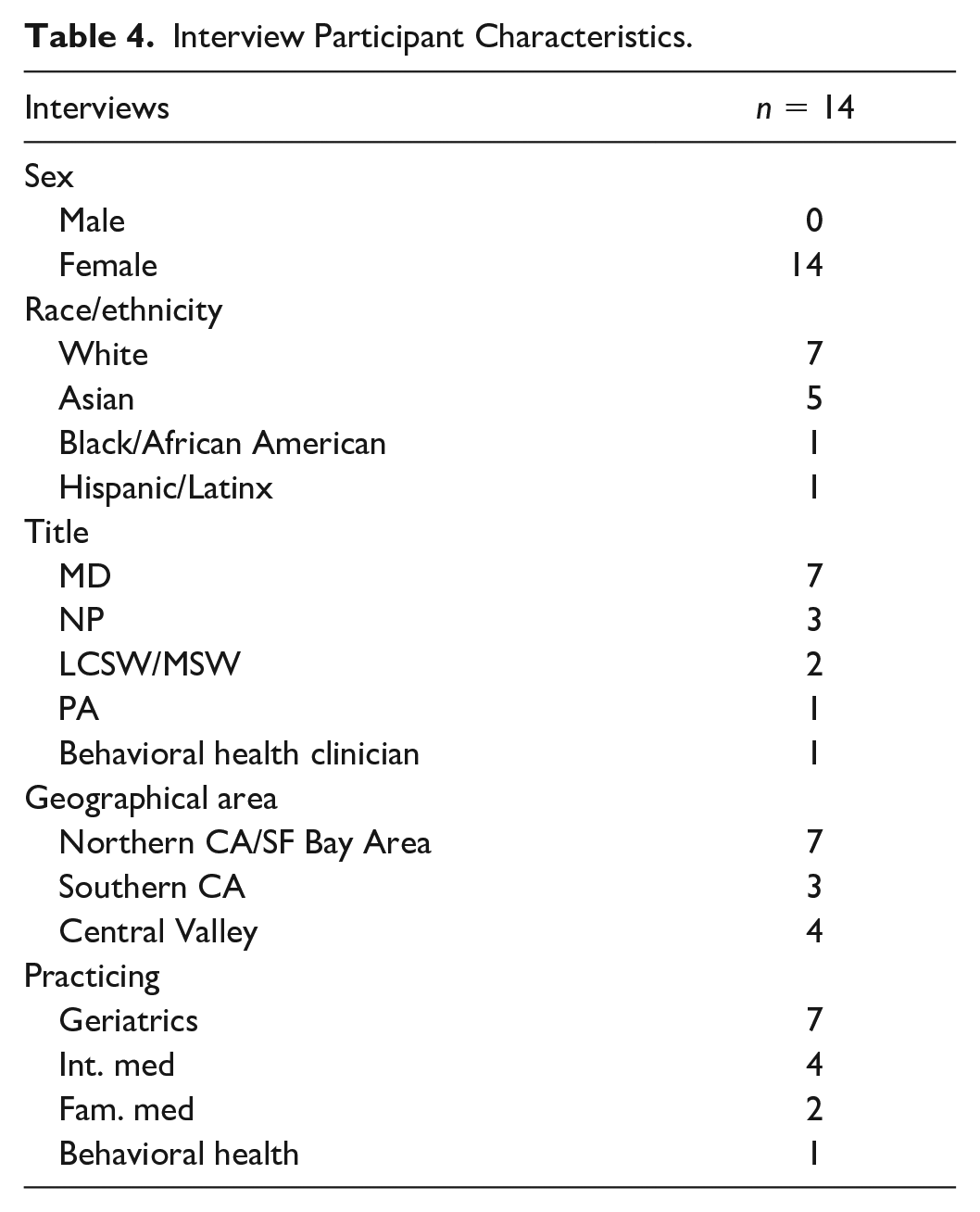
Participants
Of those who provided their title, most participants in the AD-ECHO sessions were MDs (50%), followed by LCSWs/MSWs (11%) and NPs (11%). Participating clinics represented a range of geographies and practice settings, including health maintenance organization (HMO), nonprofit, federally qualified health centers (FQHC), community health centers, Veteran Affairs (VA), and private (see Table 3 for participating practice characteristics). Our interview participants were all female. Similar to the full group of participants, of those who provided their title, most were MDs (57%) followed by NPs (21%), LCSW/MSWs (14%), and LCSW/MSWs (14%). Most (50%) practiced in a geriatric primary care setting (see Table 4 for interview participant characteristics).
Participating Practice Characteristics.
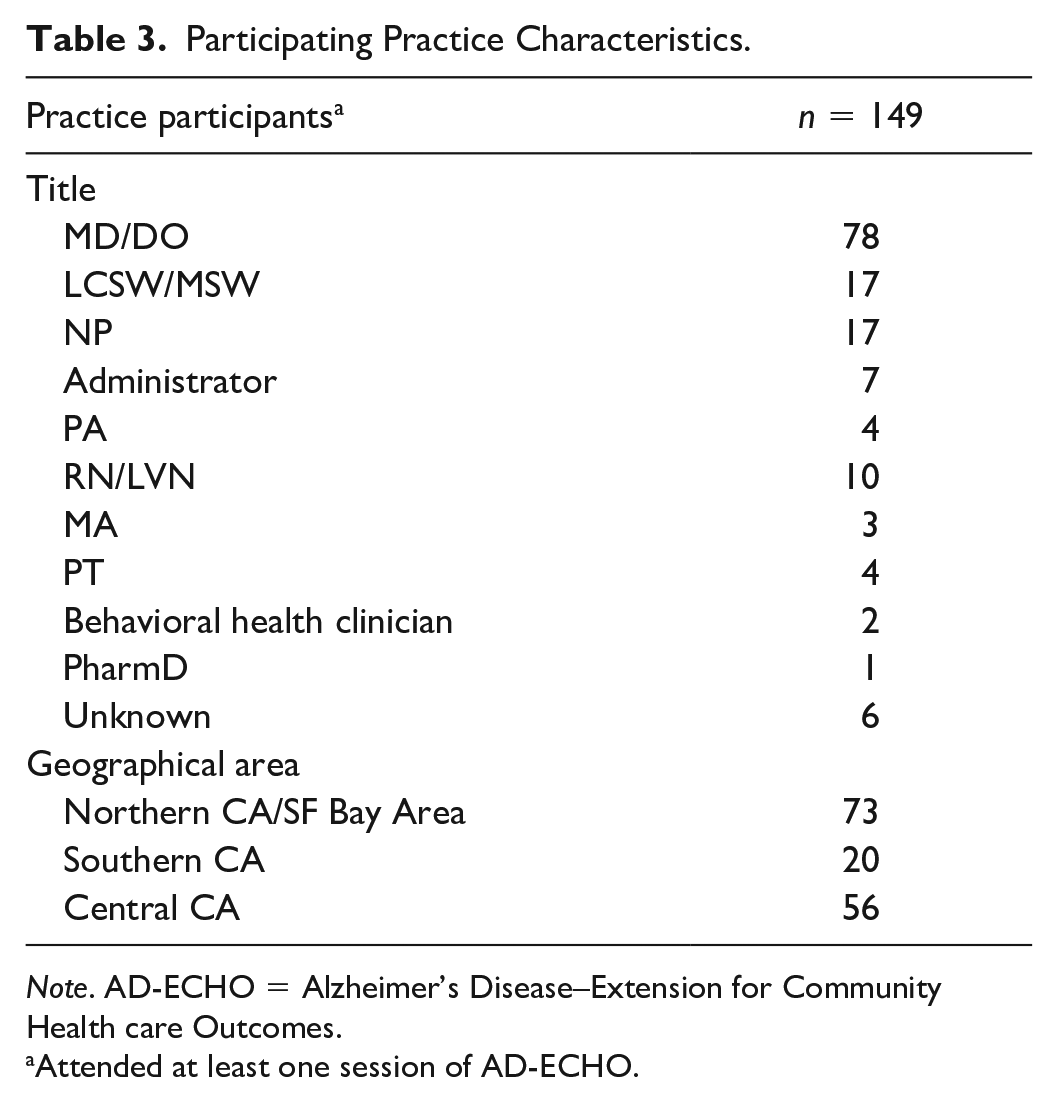
Note. AD-ECHO = Alzheimer’s Disease–Extension for Community Health care Outcomes.
Attended at least one session of AD-ECHO.
Interview Participant Characteristics.
Reasons for Joining AD-ECHO
Interview participants identified a variety of reasons for participating in AD-ECHO. These included the need for a refresher in dementia-related topics and the desire to learn about dementia due to the demographics of their patient population. For example, one participant explained, I wanted to learn about diagnosing and what other techniques were being used and what resources are out there and to see how people were handling mild cognitive impairment and if people were doing what we were doing in our clinic. (PCP6_LCSW)
Participants also identified a desire to expand what they could offer to better help their patients, with a specific focus on resources and the social aspects of managing dementia. For example, I have a few patients who come in, and then when they explain to me, “Oh, I have memory issues” . . . we know the basic stuff, but I don’t know extensively how to help this patient because I’m not sure is there any treatment available or what other resources I can give to them through the patient’s family. (PCP12_MD)
Furthermore, some participants valued joining a collaborative community due to experiences of isolation in their current setting or because they were interested in hearing how other clinics handled similarly challenging cases.
Satisfaction
The Value and Impact of Cultivating a Supportive Learning Environment
Many interview participants in AD-ECHO felt that the program cultivated a supportive learning environment. Specifically, they noted feeling supported by the empathy and reassurance they experienced from the specialist team and other participants in the program. Many felt that the empathy and reassurance were confidence-building and created a safe place to ask questions, learn, and discuss challenges. Some felt that this reassurance inspired them to take more action in their work with patients with dementia. Others felt especially supported by the approachable and collaborative environment created when focused on problem-solving during case review discussions. Through the support of specialists and the community, they learned how to think through a challenge and received supportive feedback about their strengths in working through that challenge. One nurse practitioner explained, Using words like, “We know this is a tough situation. We’ve been there in similar situations.” Just a sense of empathy from other providers is really valuable, because you can feel really isolated and unsure when you’re caring for people that are so vulnerable . . . it just lends another piece of confidence and credibility to your practice. (PCP2_NP)
A physician’s assistant articulated, It was a reassurance. To hear that what [the specialists] are doing is something that maybe I’m doing in my practice, it was great. I felt that I was on the right path. I mean what I’m doing is—it’s good, the right thing to do. (PCP8_PA)
This supportive learning environment also enabled some PCPs to experience improvement in their ability to communicate with specialists and other members of their teams and develop relationships with other community practices. For example, AD-ECHO’s supportive setting provided some with the confidence and knowledge to ask neurologists accurate and helpful questions to better engage in the dementia diagnostic process. Others felt more comfortable engaging in follow-up work with neurologists. Some reported feeling better able to ask the “right” questions because they developed an understanding of the specialist’s thought process regarding diagnosis. A few participants also felt that communication and sense of community within their own teams was also improved, for example, Being in the same project [with people who were in my group] helped strengthen that relationship, and so it makes me feel more comfortable asking for help, for advice within my own community. (PCP1_MD)
Observations similarly identified the way specialists empathized with PCPs and validated their struggles while providing concrete recommendations to overcome barriers during case review. Observers noted that PCPs appreciated having a forum to have their experiences, effort, and difficulties validated.
Struggle to Fit AD-ECHO Into Busy Schedules
Most PCPs felt that a major challenge regarding participation in AD-ECHO was fitting the sessions into their already busy schedules. Some participants struggled if they ran late and missed the didactics and felt that it was hard to catch up. Participants made recommendations about providing digital copies of the lectures and different formats, such as a daylong conference, as well as ways to catch up if they missed a lecture.
The lunchtime meetings were a little problematic for me since I have morning clinic that often ran over into the lunch hour; therefore, I would often join late, and this impacted my learning. (PCP1_MD)
Learning and Competence
The Knowledge Gained Empowered PCPs to Take More Action Around Dementia in Their Clinical Care of Patients
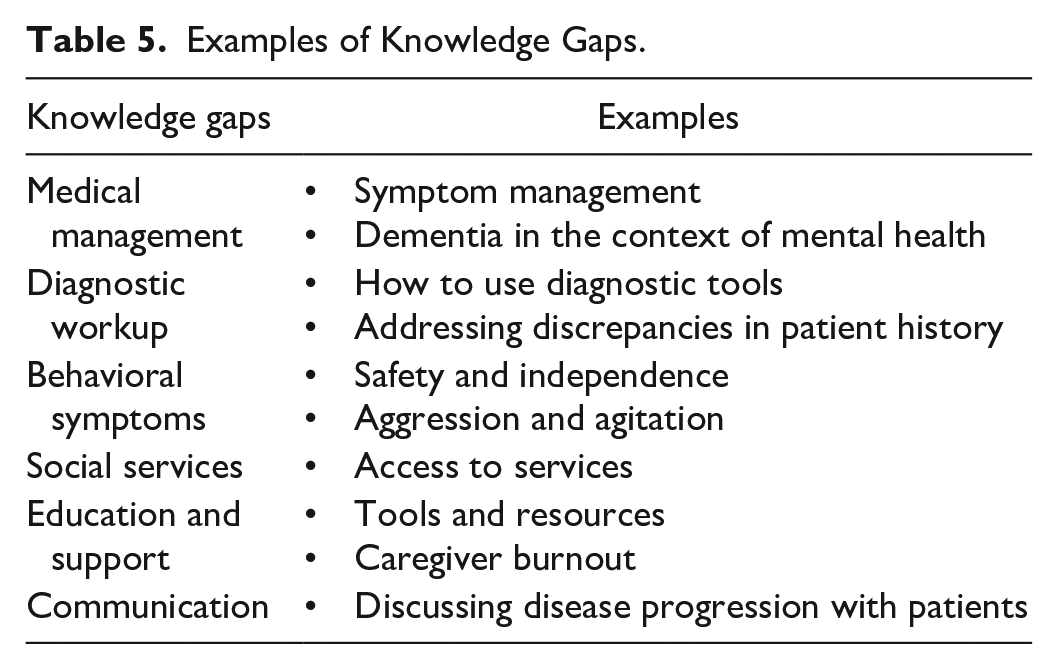
The most frequent questions raised by PCPs during observations of AD-ECHO sessions, indicating knowledge gaps, were in the following domains: (a) diagnostic workup (e.g., how to use diagnostic tools, addressing discrepancies in patient history), (b) medical management (e.g., symptom management, dementia in the context of mental health or substance abuse), (c) behavioral symptoms (e.g., safety and independence, aggression and agitation), (d) social services (e.g., access to services), (e) education and support (e.g., tools and resources, caregiver burnout), and (f) communication (e.g., discussing disease progression with patients). During sessions, PCPs raised the most questions about medical management, followed by diagnostic workup and behavioral symptoms. Observers noted that medication was a major topic of discussion that PCPs did not have much confidence or experience with, while managing behaviors came across as the most stressful and difficult topic and was the most frequent area about which PCPs turned to specialists for guidance and advice. See Table 5 and Figure 1 for question examples and frequencies.
Examples of Knowledge Gaps.
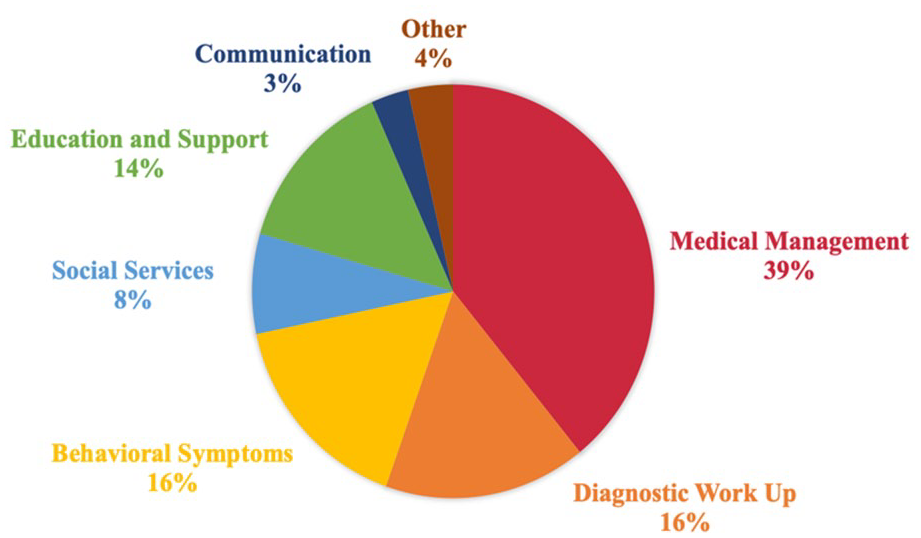
Types of Questions Raised by PCPs During AD-ECHO Sessions.
In interviews, many participants articulated that they gained important and actionable knowledge from participation in AD-ECHO. Most notably, they identified the value of learning about diagnostic tools, atypical dementias, behaviortx management, medications (both what to prescribe and how to manage polypharmacy), community resources, and learning about other clinicians’ approaches to care. The didactics provided participants with targeted information, while the cases provided them with practical knowledge from dementia experts and from the community.
When we went through some of the nuances of the other types of dementias, I think now actually from doing this, I’m more comfortable and confident at trying to look outside the Alzheimer’s label. Well, maybe there’s this. Maybe it’s this. Maybe we should have them see the neurologist. So I think it actually made me critically look at what they’ve been diagnosed with, as well, to make sure it’s accurate, so that we’re treating appropriately. (PCP4_NP) They helped us to differentiate patients, if it’s the depression or dementia. And I was able to get a lot of help with if they have behavioral issues or if they have depression . . . [the] other thing I learned was, other than medications . . . it’s their lifestyle modification, like a healthy lifestyle, physical activities, exercise, healthy diet. (PCP12_MD)
During observations, we found that specialists provided PCPs with knowledge and direct recommendations, helping them gain new perspectives on how to address patient cases, and how to utilize and expand their in-depth knowledge of and rapport with patients to facilitate individualized decision-making, difficult conversations, and planning. However, in interviews, some participants still noted the challenge of applying the knowledge gained during busy primary care practice days where they are constantly negotiating what to prioritize. Furthermore, some participants made recommendations for areas in which they would appreciate further education, including emerging disease-modifying treatments and other medications, more emphasis on caregiver support, content on levels and transitions of care, and how to address systemic barriers to long-term care.
Value of Dementia-Specific Resources Provided
Throughout AD-ECHO, resources from community and dementia specialist team members were shared based on the topics and cases discussed and requests for more information that came up during the sessions. Most interview participants endorsed the value of these resources. These included resources related to the diagnosis and care of people with dementia (e.g., an Alzheimer’s disease diagnostic tool kit) as well as resources focused on care planning (e.g., caregiver education, support groups, day care centers, long-term care options, and organizational connections). Some participants reported that they shared the resources provided with others in their practice.
It was really nice to have the resources listed out . . . Quite honestly, I haven’t really gone back to it very much, but I like knowing that it’s there in case I do need it. (PCP14_MD) I think getting familiarity with the toolkit. I enjoyed learning about it. . . I also recognize that it is not actually usable in regular practice. But I think as a learning tool, it’s actually quite good. And then, the dementia questionnaire, while not something I can do with most of my patients, having it available in Chinese to give to a smaller subset of my patients who complain of memory issues, I think that’s actually been real helpful. (PCP7_MD)
Others felt that the resources were valuable but that they were difficult to access, or that they would not have the time to engage with them more deeply. Some participants stated they did not use the resources actively, although they appreciated having the reference for when they needed it.
Performance
Dissemination of AD-ECHO Knowledge Into Primary Care Practice Settings
Many interview participants were actively involved in disseminating the knowledge and skills they had acquired through AD-ECHO into their practice settings. They were proactive in sharing what they learned with their colleagues and teams, or had plans to disseminate knowledge in the future. Some dissemination strategies included discussion of the topics covered in AD-ECHO during weekly and quarterly meetings, sharing resources and educational materials through email, updating protocols in their clinical practice, and implementing improved triage approaches. One participant was using the AD-ECHO model to develop approaches to training residents. Examples of dissemination approaches are as follows, With the residents and fellows, we did use the knowledge for lectures we have once a week, it’s a didactic for the fellows, and we give a special lecture to the family medicine and internal medicine residents. And the medical students, they come and rotate with us. So, we use this information with them for education. (PCP3_MD) We have meetings at least once a month for all the house call providers. We discuss any questions that anybody has. We all collaborate. We do have opportunities to spread the word and our new knowledge and material that we learned from [AD-ECHO]. (PCP8_PA) I think it’s just made me more excited as a clinician and confident to share information. And if someone comes to me to take [dementia] on, I may be a little bit more rigorous than I had previously to kind of help them problem solve it out, even if it’s my patient, to try to guide them, spend a little extra time having a conversation about it. (PCP4_NP)
Desire for Ongoing AD-ECHO Network Engagement
Many interview participants articulated wanting further opportunities to connect with AD-ECHO, although in a less time-intensive and structured format. Recommendations included an all-day conference, alumni group, networking opportunities, check-ins, a virtual forum, and opportunities for in-person contact. Participants explained, Just these connections are helpful . . . kind of knowing that you’re there to help me if I need it . . . Maybe a dream would be if my nurse and I came down [to the dementia expert center] with one of my patients. That would probably be the best way to learn, truly. One day. I’m sure we would learn so much. (PCP9_MD) I feel to continue to communicate with the whole team . . . if we have anything to follow through either once every three months, once every six months, something longitudinal . . . to be able to reach out with questions or resources or ask kind of random things that might come up. (PCP3_MD)
Discussion
This qualitative study examined the implementation of the AD-ECHO program and its implications for the primary care workforce. Building PCP capacity in dementia assessment and care is a major priority for improving access to quality dementia care, especially for at-risk patients from populations disproportionately impacted by health disparities.
The Project ECHO model has been highly successful, with studies showing that it can change practitioner behavior and patient outcomes, and that it is cost-effective (Zhou et al., 2016). The model has been expanded to several other clinical, and even nonclinical fields (Katzman et al., 2014; Koenig et al., 2016, 2019; Komaromy et al., 2016; Scott et al., 2012; Sockalingam et al., 2018). Prior qualitative studies of Project ECHO programs in different disease areas identified findings similar to ours regarding the experience of a supportive community developed during the sessions, the impact on patient care, and ways participants disseminated what they learned, as well as the challenges related to time (Carlin et al., 2018). Other Project ECHO programs have also been developed to support dementia care. In 2018, the Alzheimer’s Association implemented their first Project ECHO for dementia. A formal evaluation of the Alzheimer’s Association program by the Center for Evaluation of Applied Research indicated good engagement, high satisfaction, and high impact with respect to knowledge gained among participants. A Project ECHO for dementia program was also created in Washington State in late 2019, led by University of Washington faculty members, and currently serves more than 60 community practices. Given this increase in dementia-focused ECHO programs, our study identifies important areas of focus for the ongoing implementation and improvement of AD-ECHO. Some of the implications of this program and our work are outlined in the following.
Addressing Dementia Workforce Needs
Strengthening a primary care workforce that is capable of timely dementia diagnosis and quality dementia care is a major research priority, highlighted in the National Alzheimer’s Project Act (NAPA) Milestone 9K to support research on early detection of cognitive impairment (CI)/dementia in everyday settings (National Institute on Aging, n.d.) and in the U.S. Congress’s Building Our Largest Dementia Infrastructure for Alzheimer’s (BOLD) Act (Alzheimer’s Impact Movement, n.d.; Cummings et al., 2022, 2023; “2023 Alzheimer’s Disease Facts and Figures,” 2023). The emphasis on the primary care workforce in dementia is due to the expected growth in patients with dementia as the population ages, alongside recently approved and future disease modifying treatments for early stage ADRD. Primary care is the first point of contact for most people experiencing cognitive concerns and is where dementia diagnosis is most often missed or delayed (Amjad et al., 2018; Bernstein, Rogers, Possin, Steele, Ritchie, Kramer, et al., 2019; Boise et al., 1999; Bradford et al., 2009; Happich et al., 2016; Harris et al., 2009; Hunter et al., 2015; Koch & Iliffe, 2010; Lang et al., 2017; Ólafsdóttir et al., 2001; Thyrian et al., 2016; Volpe et al., 2020). Prior studies demonstrate that PCPs face barriers to diagnosing dementia and caring for these patients, including competing time demands, difficulty accessing and communicating with specialists, low reimbursement, difficulties connecting with service agencies, managing patient and family preferences, and lack of interdisciplinary teams (Boise et al., 1999; Boustani et al., 2006; Brayne & Fox, 2007; Cordell et al., 2013; Harris et al., 2009; Hinton et al., 2007; Iliffe & Wilcock, 2005; Russ et al., 2013; Sideman et al., 2022; Yokomizo et al., 2014). As our findings demonstrated, programs such as AD-ECHO have the potential to strengthen the primary care workforce’s knowledge and confidence around dementia care and to address knowledge gaps.
Building and Strengthening Community and Networks Through a Community of Practice
In interviews, participants noted the supportive learning community generated through AD- ECHO, which helped them feel validated in their work and less isolated in their roles. Observations also identified characteristics of this support, such as empathy and validation. In this way, the implementation of AD-ECHO created a Community of Practice by organizing and convening a group of people who attended a series of regular meetings, discussed and shared common goals and challenges, and emphasized a Project ECHO principle of “all teach, all learn”—everyone has something to contribute and take away. Community of Practice within this context involved convening a group of people with common goals and values who shared knowledge and expertise to improve practice (Raatz et al., 2023; Ranmuthugala et al., 2011; Seibert, 2015).
As part of this Community of Practice, the AD-ECHO approach promoted highly efficient communication between specialists and PCPs by allowing a small team of specialists to advise and educate multiple community practitioners simultaneously. Beyond its educational value, Project ECHO establishes new relationships between community practices and specialty centers, which can also facilitate referrals of patients to the specialty centers when needed for difficult or complex cases. In addition, by bringing together practitioners from the same region, Project ECHO leverages the expertise of community practitioners who can inform their colleagues about local resources to support care. These features distinguish Project ECHO from other educational venues, such as publications, conferences, and websites. To strengthen these ties, more work is needed to identify ways to provide ongoing participation in and interaction with AD-ECHO and the community after the completion of the session, as requested by participants in our study. To address this need, the AD-ECHO team is currently developing an alumni series for former participants who wanted to continue their learning and engagement with the community. This desire for ongoing connection with the AD-ECHO community also supports the aspect of a Community of Practice that involves maintaining a long-term level of engagement. Furthermore, there is a need to identify opportunities for more informal PCP-specialist communication and relationships.
Validating PCP Experiences and Knowledge Through Nurturing Learning Environments
Our findings identify a need to provide more opportunities for PCPs to get positive reinforcement about their work in dementia diagnosis and care, and to have supportive and empathetic interactions with specialists that bolster their confidence. Developing educational settings that create a positive atmosphere and nurture PCPs’ work may help to build confidence in dementia care and strengthen their willingness to engage in identifying patients with dementia and supporting their ongoing care.
Supporting Dissemination and Interprofessional Teamwork Within Practices
Many participants in AD-ECHO actively sought to share and integrate the knowledge gained into their clinical practice and professional development. Furthermore, many different professions were represented in the sessions, including MDs, NPs, social work, physical therapy, and behavioral health clinicians among others. Participants articulated the improvement in communication and work within their teams about dementia, which is another important way that AD-ECHO was disseminated into and affected the practice setting and not just individual clinicians. AD-ECHO facilitated dissemination of best practices and insights within teams and practices, strengthened because it was delivered in a digestible, thoughtful, and nurturing manner. Future AD-ECHO work may include structured recommendations for ways that PCP participants can circulate tools, resources, and lessons learned into their practices and beyond, and guidance for how to strengthen interprofessional teamwork around dementia care.
Responsive Course Content
To respond to the requests for additional didactic content, the AD-ECHO team is now working to develop and tailor more targeted sessions that focus on the areas where most questions were raised (e.g., medical management). As noted previously, they are also developing an alumni concept that would allow continued delivery of basic didactics to new ECHO participants while also offering sessions covering additional topics for practitioners who have previously heard these talks.
Limitations
This study has several limitations. First, participants chose to participate in the AD-ECHO program and in our interviews, which may result in selection bias. In addition, this AD-ECHO program only served PCPs in California, and therefore does not represent a diversity of experiences from across the United States, although both urban and rural settings and different types of health care systems were represented.
Conclusion
Findings from this study demonstrate that AD-ECHO has the potential to grow the dementia care workforce by expanding the reach of expert knowledge, as evidenced by the ways that PCPs identified direct impact of participation on their knowledge and patient care. Furthermore, AD-ECHO can lead to the development of a supportive and ongoing Community of Practice, providing validation and empathy among health care practitioners, particularly across discipline. Finally, there is a need to identify more ways to support dissemination of AD-ECHO knowledge within practices, with an emphasis on strengthening and supporting the work of interprofessional teams. AD-ECHO has the potential to lead to ADRD workforce enhancements, particularly in underserved primary care practices, and provide a policy framework for how to improve primary care training and engagement in ADRD.
Supplemental Material
sj-docx-1-mcr-10.1177_10775587241251868 – Supplemental material for Strengthening Primary Care Workforce Capacity in Dementia Diagnosis and Care: A Qualitative Study of Project Alzheimer’s Disease–ECHO
Supplemental material, sj-docx-1-mcr-10.1177_10775587241251868 for Strengthening Primary Care Workforce Capacity in Dementia Diagnosis and Care: A Qualitative Study of Project Alzheimer’s Disease–ECHO by Alissa B. Sideman, Alma Hernandez de Jesus, Cecilia Alagappan, Melissa Ma, Christopher J. Koenig, Loren I. Alving, Freddi Segal-Gidan, Rachel Goldberger, Dana Sohmer and Howie Rosen in Medical Care Research and Review
Footnotes
Acknowledgements
The authors thank Morgan Daven and Stella De La Pena for their contributions to this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Resources and Services Administration (HRSA) [Grant 1 U81HP26494-01-00] of the U.S. Department of Health and Human Services (HHS) as part of an award totaling US$543,300, with 0% financed with nongovernmental sources. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement by, HRSA, HHS, or the US Government. For more information, please visit HRSA.gov. This work was also supported by the National Institute on Aging (K01AG059840) and the California Department of Public Health Alzheimer’s Disease Program (no. 19-10614, no. 18-10612).
Supplemental Material
Supplemental material for this article is available online.
References
{kind=link}
{kind=link}
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.