
Abstract
Objective
Currently, no comprehensive analysis of the risk factors for venous thromboembolism (VTE) in chronic obstructive pulmonary disease (COPD) patients has been reported. We aimed to explore the risk factors for VTE among individuals with COPD using meta-analysis.
Methods
PubMed, Cochrane Library, Web of Science and Embase were searched from database to February 2025 for case-control and cohort studies that assessed the risk factors for VTE among COPD patients. Pooled odds ratios (ORs), mean differences (MDs) and 95% confidence intervals (CIs) were calculated to determine the risk factors.
Results
A total of 23 clinical studies were included. Being female, atelectasis, prolonged immobility, invasive mechanical ventilation, neoplasia and chest pain (P < .05 for all) increased the risk of VTE in COPD. In addition, lower levels of PaO2 (MD: −2.12; 95% CI: −4.04, −0.19; I2 = 0%; P = .03), lower levels of PaCO2 (MD, −3.62; 95% CI: −6.96, −0.27; I2 = 65%; P = .03), higher levels of D-dimer (MD, 1.31; 95% CI: 0.13, 2.50; I2 = 75%; P = .03), increasing of age (MD: 2.05; 95% CI: 0.42, 3.68; I2 = 90%; P = .01) and having a history of venous thrombosis (OR, 4.87; 95% CI 1.91-12.41; I2 = 90%; P = .0009) were associated with VTE. However, diabetes was not identified as significant risk factors for VTE in COPD.
Conclusions
This review provides a comprehensive overview of the quality of the evidence base for the risk factors of VTE in patients with COPD. Healthcare professional should be aware of the risk factors for VTE when rehabilitating patients with COPD.
Highlights
VTE is a preventable cause of death in COPD patients.
This meta-analysis provides a comprehensive overview of the available evidence and informs clinical staff about the importance of screening for VTE in COPD patients.
The risk factors of VTE in patients with COPD included: females, atelectasis, prolonged immobility (≥3 days), invasive mechanical ventilation, neoplastic disease and chest pain. In addition, lower levels of PaO2 or PaCO2, higher levels of D-dimer, increasing of age and a history of venous thrombosis were associated with VTE.
Introduction
Chronic obstructive pulmonary disease (COPD) is a widespread condition characterized by persistent respiratory symptoms and systemic inflammation, resulting in airflow limitation and a progressive decline in lung function. 1 COPD significantly compromises the patient's quality of life, increases the probability of related complications and is associated with a substantial socio-economic burden.
Multiple risk factors contribute to venous thromboembolism (VTE), a common complication of COPD patients. The pathogenesis of COPD combined with VTE is complex, but is believed to result from prethrombotic states, inflammatory response, hypoxemia and increased oxidative stress. VTE is a preventable cause of death in COPD patients. The incidence of VTE in COPD patients is high, has a rapid progression and can be life-threatening. 2 Therefore, early assessment of the risk of VTE and preventive treatment can reduce mortality risk in COPD patients. However, symptoms such as coughing and dyspnea caused by VTE are unspecific and resemble the symptoms of acute exacerbation of COPD. Studies have shown that patients with COPD show a 2.5-fold increased risk of secondary VTE compared with patients with normal lung capacity.3,4 It is usually difficult to distinguish between VTE and COPD, resulting in a low diagnosis rate of VTE. Therefore, there is an urgent need to identify COPD patients at risk of VTE for effective prevention.
However, variables linked to VTE in patients with COPD have received little attention. There have been some reported discrepancies between the findings of earlier research on risk variables, which could be because of limited sample numbers and various inclusion criteria, so clinical practice cannot be guided by corresponding evidence. 5 There isn't yet a thorough examination of the risk factors for VTE in patients with COPD. Therefore, we aimed to explore the risk factors for VTE among individuals with COPD by meta-analysis. We present the following article by the CONSORT reporting checklist.
Material and Methods
Search Strategy
The search was performed on three databases (EMBASE, Cochrane Library, Web of Science and PubMed) from their inception until February 22, 2025. We attempted to identify eligible articles by developing search queries according to the characteristics of each database. The search approach is summarized in Supplementary Tables 1-3. The key concepts used for searching were “Chronic Obstructive Pulmonary Disease”, “venous thromboembolism”, “Deep Vein Thrombosis”, “Pulmonary Embolism” and “risk factor”. To make sure that other possibly suitable studies were included, we manually verified the references of the retrieved publications and tracked their references.
Study Selection
All the retrieved studies were reviewed for inclusion based on the following criteria: (1) Articles that were written in English; (2) observational studies, including case-control and cohort designs; (3) studies mentioning VTE among individuals with COPD. The exclusion criteria inlcuded: (1) Studies that did not report relevant risk factors. (2) Incomplete information or inability to conduct data extraction research; and (3) case reports, reviews, letters or commentary. Duplicate studies were removed after reading titles and abstracts. Two researchers further excluded studies that did not meet the eligibility criteria. Next, two researchers completed the full-text review and data extraction independently. In cases of controversy, the researchers compared the results and discussed them until a consensus was reached.
Data Extraction and Methodological Quality Assessment
Two researchers (Huang and Wu) independently completed the data extraction process. A third reviewer was consulted in case of any doubt or objection until a consensus was reached. The extracted data included author, publication year, country, study design, sample size, setting or source of participants, the prevalence of VTE and related risk factors (ie, gender, diabetes, hypertension, atrial fibrillation, history of drinking alcohol, smoking history, obesity, varicose veins, coronary heart disease, history of deep vein puncture, bed rest, heart failure, infection, anticoagulation therapy, rehabilitation treatment, age and cancer). Two researchers independently used the Newcastle-Ottawa Scale (NOS) 6 to assess the quality of all included literature, and they came to a consensus about the quality evaluation through discussion. Studies with an NOS score ≥6 that included appropriate statistical analyses were deemed to have high methodological quality.
Statistical Analysis
The RevMan 5.3 software (http://tech.cochrane.org/revman/download) was used for data analysis. For count data, odds ratio (OR) was used as the effective index, mean difference (MD) was selected for continuous variables and 95% confidence interval (CI) was used for interval estimation. If the heterogeneity test P ≥ .1 and I2 ≤ 40%, indicating homogeneity between the studies, the fixed-effects model was used for combined analysis; in contrast, if P < .1, I2 > 40%, indicating heterogeneity between studies, then the random-effects model was used for combined analysis. A funnel plot was used to screen for publication bias for the most reported outcome. Each study was symmetrical and within 95% CI, indicating no publication bias. Simultaneously, the publication bias was examined using the egger test, and the findings showed statistical significance (P < .05).
Results
A total of 1972 studies were found during the database search, as shown in Figure 1. After removing 82 duplicate studies and reading titles and abstracts, 300 irrelevant studies were excluded, and the remaining 58 records were examined. In addition, we excluded 35 articles that did not meet the eligibility criteria, five where data could not be extracted, and five with wrong data. Finally, 23 articles were eligible for this study, including 16 case-control studies and 7 cohort studies. The baseline characteristics of the 23 articles included are presented in Table 1.
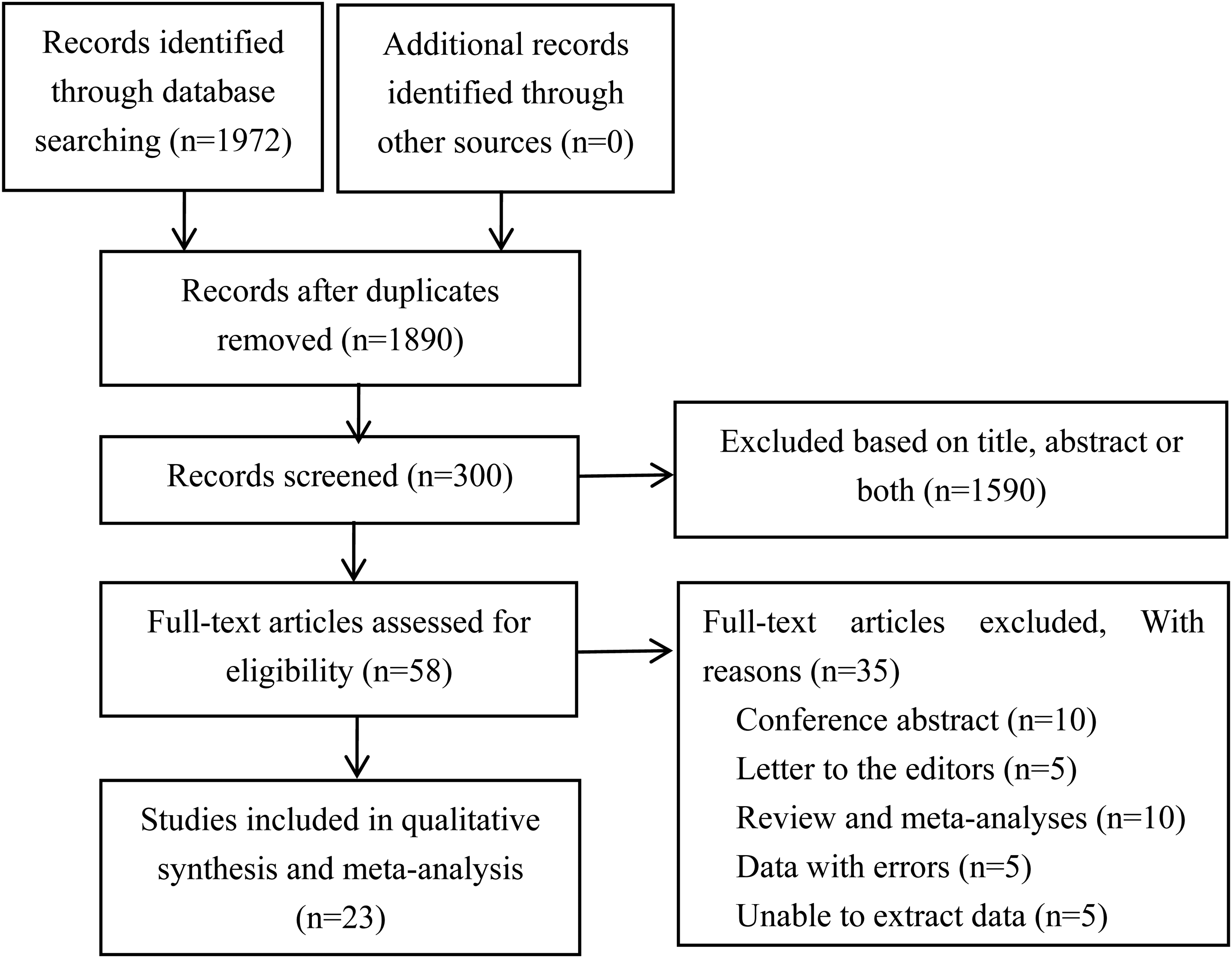
Flowchart Showing the Inclusion of Studies in the meta-Analysis.
Baseline Characteristics of the Included Studies.

Abbreviations: M, male; F, female; UK, United Kingdom; #, not reported.
Risk Factors for VTE among Individuals with COPD
Sex
Meta-analysis of 22 studies showed that being female was a risk factor for VTE in COPD patients (OR, 1.23; 95% CI, 1.02-1.49; P = .03) (Figure 2A), with significant heterogeneity among studies (I2 = 81%; P < .00001). After sensitivity analysis, the studies by Barba et al 23 and Morgan et al 13 were the main sources of heterogeneity. However, after removing those two large-scale crowd-based studies (n = 285,216), being female was still a significant risk factor (OR, 1.17; 95% CI, 1.02-1.35; I2 = 37%; P = .03) for VTE. The funnel plot analyzes the potential for publication bias (Figure 2B). The corresponding scatterplot is roughly symmetrical, indicating that the publication bias is small (Figure 2B). The results of the Egger test also showed that there was a low probability of publication bias for this indicator (P = .765) (Figure 3C).
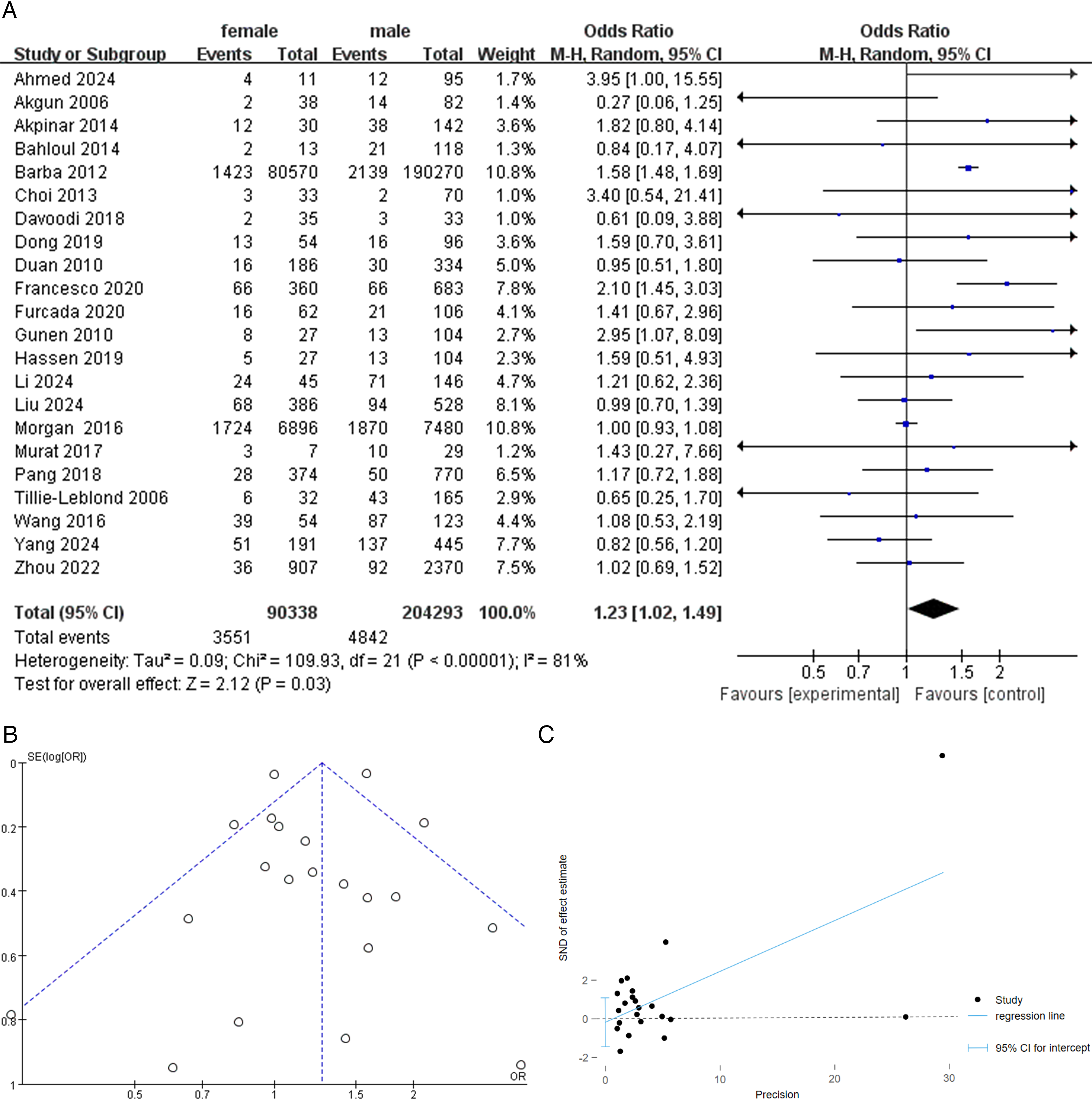
A: Forest Plot of Venous Thromboembolism for COPD Patients According to Sex. B: Funnel Plot of Venous Thromboembolism for COPD Patients According to Sex. C: Egger Plot of Venous Thromboembolism for COPD Patients According to Sex.

Forest Plot of Venous Thromboembolism for COPD Patients According to Atelectasis.
Atelectasis
The meta-analysis showed that the presence of atelectasis (OR, 5.27; 95% CI, 1.68-16.49; I2 = 0%; P = .004) was associated with a significantly increased risk of having VTE in COPD (Figure 3).
Immobility
Five studies provided data regarding the relationship between immobility and VTE in COPD patients. Prolonged immobility (≥3 days) (OR, 2.08; 95% CI, 1.36-3.18; I2 = 63%; P = .0007) was a risk factor for VTE in COPD (Figure 4).

Forest Plot of Venous Thromboembolism for COPD Patients According to Immobility.
Mechanical Ventilation Requirement
Five studies provided data on the relationship between mechanical ventilation and VTE in COPD patients. The need for mechanical ventilation among COPD patients was associated with a significantly increased risk of VTE. (OR, 2.65; 95% CI 1.32-5.34; I2 = 71%; P = .006) (Figure 5). Sensitivity analysis revealed that when the study by Akgun et al was omitted, the result was consistent with the main finding (pooled OR: 2.00, 95% CI: 1.22-3.29), and the heterogeneity was decreased (I2 = 42%, P = .006).
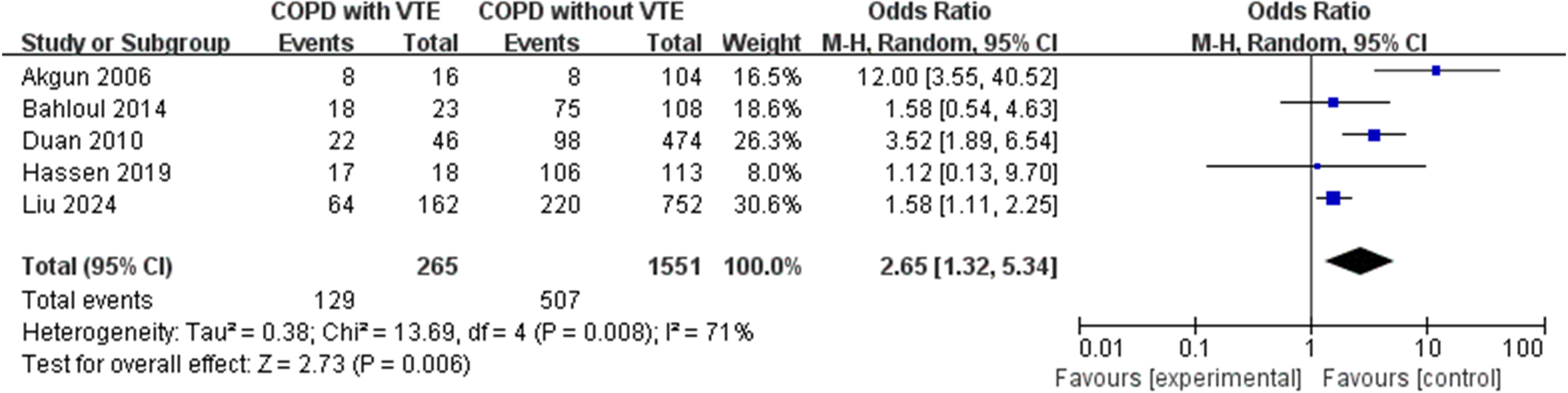
Forest Plot of Venous Thromboembolism for COPD Patients According to Mechanical Ventilation Requirement.
D-Dimer
Four studies provided data on the association between D-dimer concentration and VTE in COPD patients. The meta-analysis showed that higher levels of D-dimer among patients with COPD was associated with higher risks of VTE. (MD: 1.31; 95% CI: 0.13-2.50; I2 = 75%; P = .03) (Figure 6). Sensitivity analysis revealed that when the study by Gunen et al was omitted, the result (pooled MD: 0.83, 95% CI: 0.18-1.48; P = .01) was consistent with the main finding, and the heterogeneity between studies decreased (I2 = 25%, P = .26).
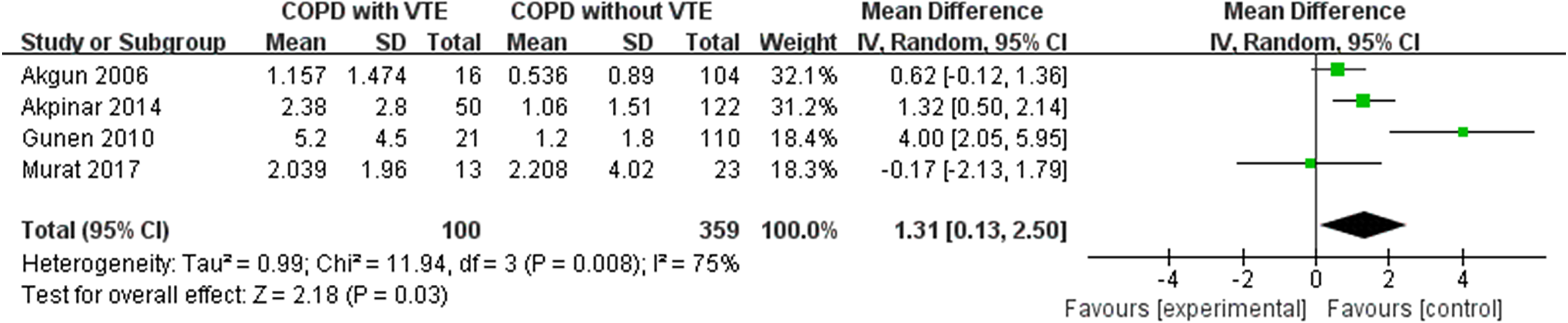
Forest Plot of Venous Thromboembolism for COPD Patients According to the Level of D-Dimer.
PaO2
A total of six studies provided data regarding the relationship between the level of PaO2 and VTE in COPD patients. Lower levels of PaCO2 among patients with COPD was associated with higher risks of VTE. (MD: −2.12; 95% CI: −4.04, −0.19; I2 = 0%; P = .03) (Figure 7).

Forest Plot of Venous Thromboembolism for COPD Patients According to PaO2.
PaCO2
A total of seven studies provided data regarding the relationship between the level of PaCO2 and VTE in COPD patients. Lower levels of PaCO2 among patients with COPD was associated with higher risks of VTE. (MD: −3.62; 95% CI: −6.96, −0.27; I2 = 65%; P = .03) (Figure 8). Omitting the study by Akgun et al in sensitivity analysis showed consistent results with the main findings (pooled OR: −5.12, 95% CI: −7.15, −3.09) with a lesser degree of heterogeneity between studies (I2 = 44%, P = .11).

Forest Plot of Venous Thromboembolism for COPD Patients According to PaCO2.
Neoplastic Disease
Eight studies provided data on the relationship between neoplastic disease and VTE in COPD patients. Having neoplastic disease was a risk factor for VTE in COPD (OR, 2.73; 95% CI, 2.54-2.93; I2 = 38%; P < .0001) (Figure 9).

Forest Plot of Venous Thromboembolism for COPD Patients According to Neoplastic Disease.
Chest Pain
Eight studies provided data regarding the relationship between chest pain and VTE in COPD patients. The meta-analysis showed having chest pain was a risk factor for VTE in COPD (OR, 1.87; 95% CI, 1.43-2.45; I2 = 29%; P < .00001) (Figure 10).

Forest Plot of Venous Thromboembolism for COPD Patients According to Chest Pain.
History of Venous Thrombosis
A total of six studies provided data on the relationship between a history of venous thrombosis and VTE in COPD patients. Compared to COPD patients without VTE, those with VTE had a history of venous thrombosis (OR, 4.87; 95% CI 1.91-12.41; I2 = 90%; P = .0009) (Figure 11). Excluding the study by Pang et al And Zhou et al on sensitivity analysis showed consistent results with the main finding (pooled OR: 2.41, 95% CI: 1.61-3.60; P < .0001) and decreased heterogeneity between studies (I2 = 4%, P = .37).

Forest Plot of Venous Thromboembolism for COPD Patients According to History of Venous Thrombosis.
Age
A meta-analysis of the fifteen studies reporting on the relationship between age and VTE revealed that age was a significant risk factor for VTE in COPD patients (MD: 2.05; 95% CI: .42, 3.68; I2 = 90%; P = .01) (Figure 12A). The funnel plot's uneven visual result raised the potential that some unfavorable outcomes were overlooked (Figure 12B). The funnel plot's asymmetry and possible publication bias were validated by the Egger test (P = .022) (Figure 12C).
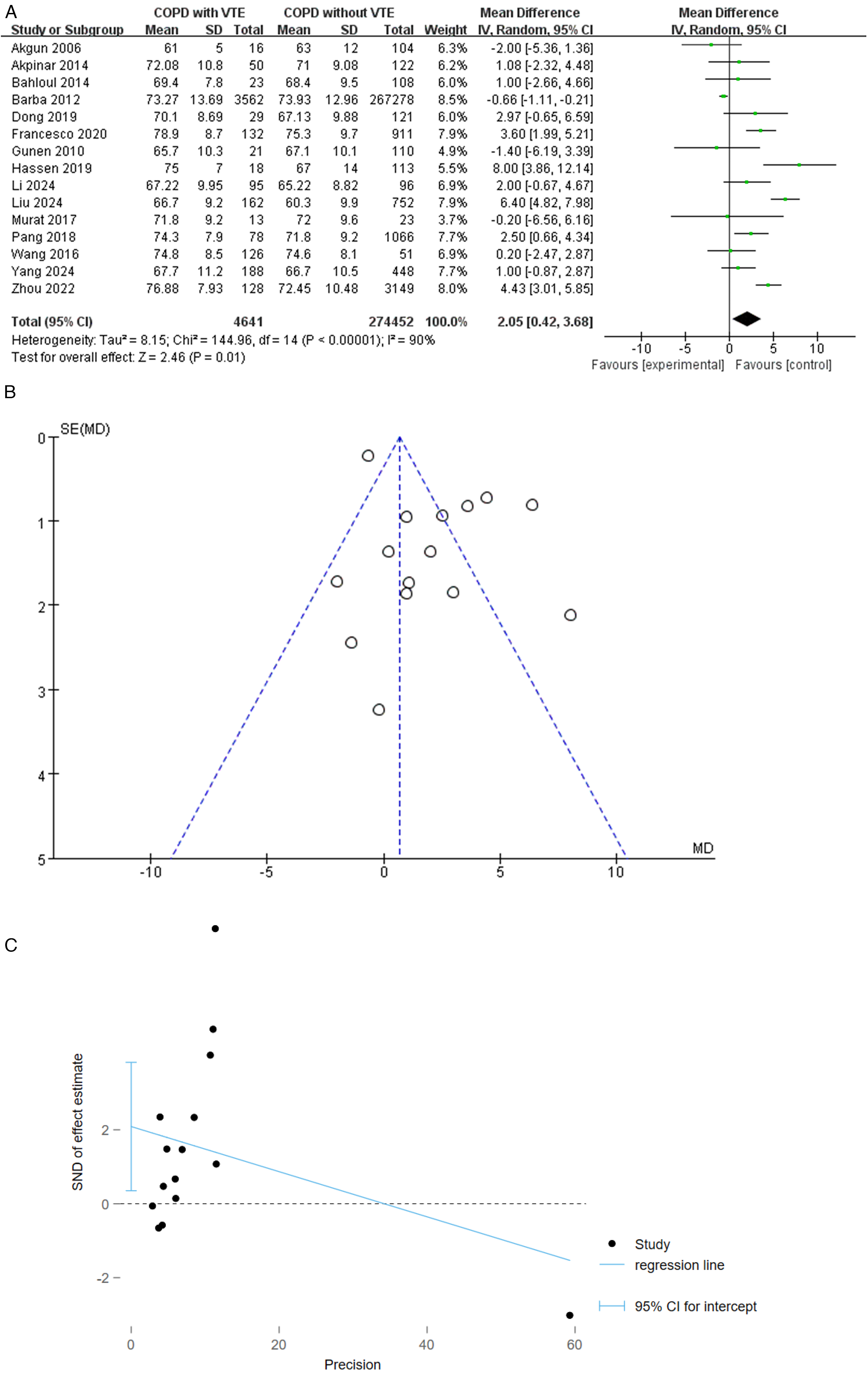
A: Forest Plot of Venous Thromboembolism for COPD Patients According to Age. B: Funnel Plot of Venous Thromboembolism for COPD Patients According to Age. C: Egger Plot of Venous Thromboembolism for COPD Patients According to Age.
Diabetes
Twelve studies reported the relationship between a history of diabetes and incident VTE in COPD patients. Meta-analysis suggested no significant association between a history of diabetes and VTE (pooled OR: 0.87, 95% CI: 0.70-1.08; I2 = 69%; P = .20) (Figure 13A). A funnel plot revealed that the majority of the studies were dispersed between the top and middle of the plot, suggesting minimal publication bias (Figure 13B). Additionally, the Egger test results indicated that the likelihood of publication bias was minimal for this indicator (P = .904) (Figure 13C).

A: Forest Plot of Venous Thromboembolism for COPD Patients According to Diabetes. B: Funnel Plot of Venous Thromboembolism for COPD Patients According to Diabetes. C: Egger Plot of Venous Thromboembolism for COPD Patients According to Diabetes. Note: Heterogeneity is Defined According to the I2 Statistic. Random-Effects or Fixed-Effect Meta-analysis Models Were Used Based on the Degree of Heterogeneity Across Studies.
Discussion
This study found that gender factors influence COPD complicated by VTE, and females are more likely to suffer from VTE, consistent with earlier studies.7,23 However, Barba et al 23 discovered that the male gender was a risk factor for VTE in hospitalized COPD patients (OR, 1.23; 95% CI, 1.02-1.49; P = .03). In addition, studies have shown that males tend to suffer from VTE,7,23 probably due to the gender ratio of the collected cases and differences in the studies’ inclusion criteria.
This study showed that immobility exceeding three days and the presence of atelectasis were associated with increased risks of VTE in COPD. COPD is a systemic disease that severely impairs functional abilities of patients, especially elderly patients suffering from respiratory failure. 30 As lung function declines, breathing difficulties may restrict daily activities, causing patients to remain bedridden for a long time. Immobility increases the possibility of a prethrombotic state (Prothrombotic state, PTS). 31 PTS makes COPD an airway or lung disease and a vascular disease, especially in senile patients with COPD and respiratory failure. The probability of being bedridden and for PTS to occur among COPD patients increases in the long term, exacerbating the risk of deep vein thrombosis and pulmonary thromboembolism. Sunnetcioglu et al 32 found that the percentage of thrombi in the main pulmonary arteries (MPAs) was greater in immobilized patients. Nevertheless, immobilization slows blood flow and favors thrombosis. Consequently, COPD patients with breathing difficulties and limited mobility have an increased risk of thromboembolism. The administration of anticoagulant drugs to prevent thrombosis among COPD patients with a clinical suspicion of VTE or who are bedridden for over three days is of great significance.
It is worth noting that in addition to patients who have been immobilized for a long time, most patients who used invasive mechanical ventilation were in the VTE group. This information often indicates that the patient who used invasive mechanical ventilation is in a critical state. As a product of fibrin degradation, D-dimer is elevated in thromboembolism and hospitalized patients with comorbidities, the elderly, patients with malignant tumors and pregnant women.33,34 However, the specificity of this test is low in hospitalized patients with more comorbidities. Therefore, choosing the appropriate method when evaluating COPD combined VTE is vital to exclude the influence of comorbidities on the results. It is important to study the significance of D-dimer to exclude VTE in patients with COPD and reduce the excessive use of CTPA and other radiological examinations as preliminary screening tools.
Lower levels of PaO2 were strongly associated with higher risks of VTE in COPD patients. Hypoxia causes microcirculation disorders in the body, damages vascular endothelial cells, releases various inflammatory mediators and cytokines, slows blood flow and increases blood viscosity. 35 The common result of arterial blood gas analysis in COPD patients is hypoxemia and hypercapnia. Blood gas analysis is not only a routine admission examination for patients with COPD, but the results of PaCO2 and PaO2 are important to identify patients at risk of thromboembolism, which cannot be easily ignored in clinical work. For patients suspected of pulmonary thromboembolism, it is crucial to monitor the changes in blood gases, especially the trend of partial pressure of CO2.
This study found that neoplastic disease was associated with the occurrence of VTE in COPD patients. The development of malignant tumors is often accompanied by abnormal coagulation function, which is closely related to tumor cells, tumor microenvironment, inflammatory factors and treatment. Due to the activation of the coagulation cascade system, thrombocytopenia and fibrinogen consumption, frequent bleeding complications can be observed in patients with malignant tumors. 36 Tumor cells activate coagulation through multiple mechanisms related to the expression of tissue factors, inflammatory cytokines and cancer procoagulant factors. Malignant tumors may also pose a risk of thrombosis due to compression or direct invasion of large blood vessels. In the treatment of advanced malignant tumor or surgery or catheter use, stasis may lead to hemodynamic disorder and activation of the coagulation cascade. Some studies36,37 have shown that chemotherapy drugs can damage the balance of the blood coagulation system by damaging the vascular endothelium and increase the risk of thrombosis. Tumor cells interact with and activate the blood coagulation system, which is conducive to tumor angiogenesis, progression, growth and metastasis. COPD patients with malignant tumors should not only take appropriate anti-tumor treatment, but also be alert to the risk of thrombosis and select appropriate preventive anticoagulation measures according to the actual condition.
We observed that patients with a history of venous thrombosis were 4.87 times more likely to experience VTE than those without a history of venous thrombosis. The main reason was that patients with a history of venous thrombosis generally had a high thrombotic state. When stimulated by factors such as hypoxia, infection and inflammation, those patients with a history of venous thrombosis were more likely to have thromboembolism and VTE. Therefore, COPD patients with previous pulmonary embolism or venous thrombosis should be counselled on the risk of pulmonary embolism and monitored regularly.
This study suggests that age is a risk factor for VTE in COPD patients. Older patients with COPD are more likely to develop systemic vascular diseases. 38 Meanwhile, increased age is associated with significant reductions in activity tolerance, relatively prolonged bedtime, increased blood stasis and hypercoagulability states, increasing the risk of VTE. However, this study did not observe an association between a history of diabetes and a higher risk of VTE in COPD patients. Diabetes is an established risk factor for thrombosis. 39 This discrepancy could be explained by the fact that these patients have better descriptions of adequate thromboprophylaxis, and most practitioners administer VTE prophylaxis to these patients. Therefore, further research is needed to explore this contradiction.
It is important to note the study's acknowledged shortcomings. First, publication bias was probably exacerbated by the exclusion of unpublished publications from our systematic evaluation. Second, the included studies’ sample sizes differed significantly, which would have added to the results’ heterogeneity. Notwithstanding these drawbacks, this study is the first meta-analysis to look at the risk variables for VTE in individuals with COPD.
The 23 studies selected for this were of good quality based on the NOS score. Other factors that have been reported to have some association with VTE in the literature could not be assessed in this study due to insufficient data or the inability to extract relevant data. There is still a need for more high-quality, large-sample, multi-center studies, and other unproven risk factors need to be further studied based on high-quality research.
Conclusions
This meta-analysis provides a comprehensive overview of the available evidence and informs clinical staff about the importance of screening for VTE in COPD patients. The risk factors of VTE in patients with COPD included: females, atelectasis, prolonged immobility (≥3 days), invasive mechanical ventilation, neoplastic disease and chest pain. In addition, lower levels of PaO2 or PaCO2, higher levels of D-dimer and a history of venous thrombosis were associated with VTE and patients with VTE were significantly older than those without VTE (P < .05). In contrast, diabetes was not associated with VTE in COPD patients. Monitoring and support should be strengthened for patients with the above-mentioned high-risk factors to improve prognoses and reduce complications.
Supplemental Material
sj-docx-1-cat-10.1177_10760296251388989 - Supplemental material for Risk Factors Associated With Venous Thromboembolism in Individuals With COPD: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-cat-10.1177_10760296251388989 for Risk Factors Associated With Venous Thromboembolism in Individuals With COPD: A Systematic Review and Meta-analysis by Jingjuan Huang, Binjing Wu, Zeyong Zhang and Li Wang in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Abbreviation
Acknowledgements
We wish to express our gratitude to YuYu Duan for his assistance with purely technical help. In addition, we would like to thank Biqian Liu for her help in polishing our paper.
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Authors’ Contributions
Conception and design: All authors; Administrative support: L Wang; Provision of study materials or patients: J Huang, B Wu; Collection and assembly of data: J Huang, B Wu; Data analysis and interpretation: All authors; Manuscript writing: All authors; Final approval of manuscript: All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Medical Science Technology Research Fund of Guangdong Province [grant number B2021194].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data are within the manuscript and its supporting Information files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.