
Abstract
Previous studies have identified ABO blood type as a risk factor for venous thromboembolism. However, the association between ABO blood type and pulmonary embolism (PE) has not yet been explored. The PubMed, Cochrane Library, Embase, and Web of Science databases were searched from inception to May 2025. Case–control/cross-sectional and cohort studies focusing on the effect of ABO blood type on PE were evaluated. Nine eligible studies were included for meta-analysis. The pooled risk of PE was 1.45 (95% confidence interval [CI] 1.23-1.72, I2 = 89.6%) for the non-O group compared with the O group, and there was significant heterogeneity. After the exclusion of two studies that may have produced unstable results, the risk was still significant (Relative Risk [RR] 1.39, 95% CI 1.22-1.59, I2 = 47.1%), but there was less heterogeneity and improved stability. Both the A (RR 1.29, 95% CI 1.08-1.55, I2 = 47.1%) and AB (RR 1.41, 95% CI 1.18-1.69, I2 = 0.0%) blood types conferred an increased risk of PE, whereas the risk for the B group was not significant (P = .089). With respect to origin, only studies from America (P < .001), but not from Europe (P = .064) or Asia (P = .102), showed increased PE risk. Regarding study type, the results were significant both in case–control/cross-sectional (P < .001) and cohort studies (P = .002). In conclusion, individuals in the non-O group were associated with an increased risk of PE compared with those in the O group both in case–control/cross-sectional and cohort studies.
Introduction
Venous thromboembolism (VT), encompassing deep venous thrombosis (DVT) and pulmonary embolism (PE), is the third most prevalent cardiovascular disorder. 1 While the annual incidence of PE in the general population remains at 1 case per thousand individuals, stratifying the data by age reveals striking disparities. 2 The prevalence increases eightfold across age groups, progressing from 1.4 cases per thousand in 40–49-year-olds to 11.3 cases per thousand among subjects aged 80 and older.3,4 PE shows a broad clinical spectrum, varying from acute catastrophic events such as sudden cardiac death to completely asymptomatic cases detected incidentally via radiological examination.5–7 Several risk factors have been associated with an increased risk of PE, such as chronic obstructive pulmonary disease (COPD), 8 pneumonia 9 and sickle cell disease. 10 Additionally, atrial fibrillation may be a risk factor for the occurrence of PE, particularly in the first few weeks after a recent diagnosis of atrial fibrillation.11,12
Previous meta-analyses have identified ABO blood group as a risk factor for venous thromboembolism (VTE). Wu et al reported that non-O blood groups, particularly the A1A1, A1B, and BB genotypes, contribute significantly to the development of VTE. 13 Another meta-analysis reported similar results, which identified non-O blood type as a candidate risk factor for VTE, 14 as well as in children with cancer. 15 However, the associations between ABO blood group and subtypes of VTE, including DVT and PE, remain obscure. Several studies have demonstrated that patients with non-O blood type have an increased risk for PE compared with patients with O blood type.16–22 Other studies have shown that ABO blood group subtypes are not associated with DVT with symptomatic PE, 23 with total knee arthroplasty or total hip arthroplasty. 24 These conflicting findings necessitate a comprehensive meta-analysis for further investigation.
Therefore, we conducted a systemic review and meta-analysis to confirm the association between ABO blood type and PE.
Methods
Search Strategy for Inclusion of Studies
We systematically searched the PubMed, Embase, Web of Science, and Cochrane Library databases up to May 2025. The search strategy was as follows: (“abo blood group system” OR (“abo” AND “blood group” AND “system”) OR “abo blood group system” OR (“abo” AND “blood” AND “group”) OR “abo blood group”) AND (“venous thrombosis” OR (“venous” AND “thrombosis”) OR “venous thrombosis” OR (“deep” AND “venous” AND “thrombosis”) OR “deep venous thrombosis”), (“abo blood group system” OR (“abo” AND “blood group” AND “system”) OR “abo blood group system” OR (“abo” AND “blood” AND “group”) OR “abo blood group”) AND (“pulmonary embolism” OR (“pulmonary” AND “embolism”) OR “pulmonary embolism”). This study was registered on PROSPERO (ID: CRD420251020637). The review protocol was not made public.
Inclusion and Exclusion Criteria
Case–control/cross-sectional and cohort studies published in English were deemed eligible if they included patients with ABO blood group and if the outcome was a clinical diagnosis of PE. The comparison included a non-O group and its subgroups versus the O group. Studies were excluded if they were duplicates, reviews, letters, guidelines, case reports or case series. Additionally, studies were excluded if they lacked original data or if the original data could not be effectively converted and utilized.
Study Selection
Two authors (ZH W and XD W) conducted literature searches of all potential studies across multiple databases. Additionally, the reference lists of relevant studies and systematic reviews were reviewed to ensure comprehensiveness. While there was no language restriction during the database search, only English studies were potentially eligible for this study. After removing duplicate studies, two independent researchers (XJ W and XD W) reviewed the titles and abstracts for further screening. The full texts were retrieved after careful screening according to the eligibility criteria. The above information was then crosschecked by ZH W, with discrepancies resolved by the senior author (ZH W). ZH W and XD W summarized the vital characteristics of all the studies in one table (Table 1). Study quality was assessed via the Newcastle–Ottawa Scale (NOS), with scores ranging from 7 to 9 indicating high quality, scores ranging from 4 to 6 indicating moderate quality and scores ranging from 0 to 3 indicating low quality.
Main Characteristics of the Included Studies.

Abbreviations: OR, odds ratio; RR, relative risk; CI, confidence interval; NOS, Newcastle-Ottawa Scale; BMI, body mass index; ARIC, Atherosclerosis Risk in Communities; CHS, Cardiovascular Health Study; CVD, cardiovascular disease; DVT, deep venous thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism; THA, total hip arthroplasty; TKA, total knee arthroplasty; DM, diabetes mellitus.
GRADE Assesement
GRADEpro software (https://www.gradepro.org/) 25 uses the following aspects to assess the quality of evidence: limitations in the study design, potential risk of bias, inconsistency among different studies, indirectness in the evidence, imprecision, and other pertinent factors. 26 Five degrees of evidence were identified, from high quality to no evidence.
Statistical Analysis
Statistical analyses were conducted using STATA 17.0 (StataCorp LLC, located at College Station, TX, USA), with relative risks (RRs), odds ratios (ORs) or hazard ratios (HRs), and the respective 95% confidence intervals (CIs) employed as pooled effect sizes. Subgroup analyses were performed according to ABO subtype, origin and study type. A funnel plot was used to detect publication bias. Heterogeneity was assessed by the I2 test (I2 < 50%). 27 Sensitivity analysis was also carried out to ensure the stability of the pooled analysis.
Results
Study Selection and Baseline Characteristics
Overall, 725 studies were retrieved from the four databases. Following the removal of 390 duplicates, 335 records were then screened. Studies were excluded for the following reasons: irrelevant objectives (n = 215), case reports/series, letters, reviews, guidelines (n = 43), congress abstracts (n = 17), records not English (n = 11), and basic science/experimental studies (n = 8). After further screening for full texts, 9 eligible studies were ultimately included in the meta-analysis (Figure 1). Details of all the selected studies are displayed in Table 1.
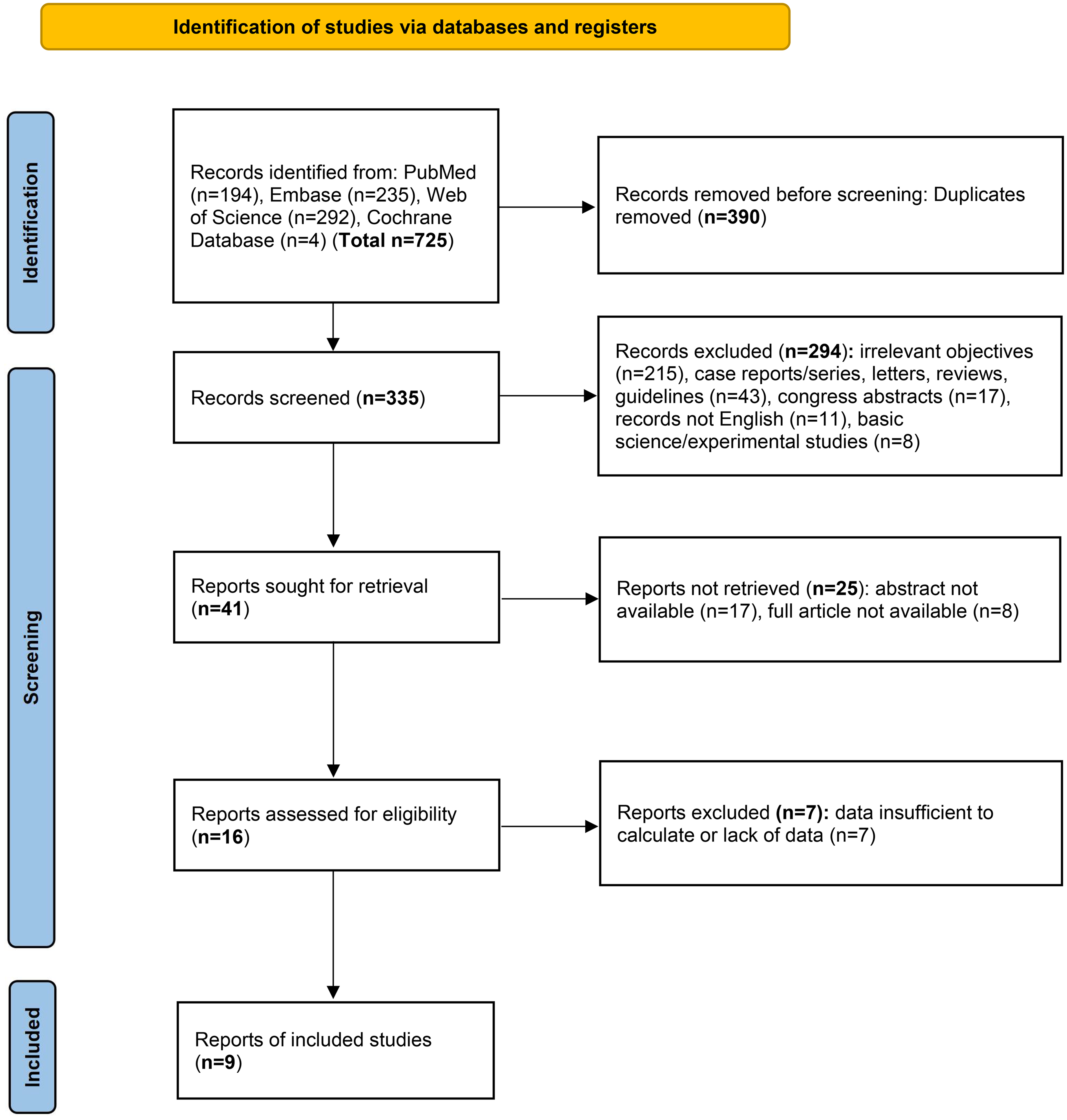
PRISMA Flowchart Showing the Study Selection Process.
PE Outcome Analysis
All nine studies reported the development of PE. The pooled risk of PE was 1.45 (95% CI 1.23-1.72, I2 = 89.6%, Figure 2) for the non-O group compared with the O group, indicating significant heterogeneity among them. The funnel plot analysis suggested rough symmetry (P > .05, Figure 3A). Sensitivity analysis revealed that two studies19,22 might have caused instability in the overall analysis (Figure 3B). To generate a more stable result, further analysis was conducted with the exclusion of the above studies. The results still indicated that the non-O group had an increased risk of PE compared with the O group (RR 1.39, 95% CI 1.22-1.59, I2 = 47.1%, Figure 4), with significantly decreased heterogeneity and improved stability.

Forest Plot Showing the Association Between ABO Blood Group and PE.

Funnel Plot (A) and Sensitivity Analysis (B) of the General Analysis.

Forest Plot Showing the Association etween ABO Blood Group and PE with Stable Results.
Subgroup Analysis
Subgroup analyses were performed according to ABO subtype, origin and study type (Figure 5, Table 2). Both the A (RR 1.29, 95% CI 1.08-1.55, I2 = 47.1%) and AB (RR 1.41, 95% CI 1.18-1.69, I2 = 0.0%) blood groups conferred an increased risk of PE, whereas the risk for the B group was not significant (P = .089, Figure 5A). Regarding origin, only studies from America (RR 1.42, 95% CI 1.18-1.72, I2 = 66.1%), but not from Europe (P = .064) or Asia (P = .102, Figure 5B), showed increased PE risk. Regarding study type, the results were valid in both case–control/cross–sectional (RR 1.29, 95% CI 1.15–1.46, I2 = 27.5%) and cohort studies (RR 1.58, 95% CI 1.18–2.12, I2 = 94.9%, Figure 5C).
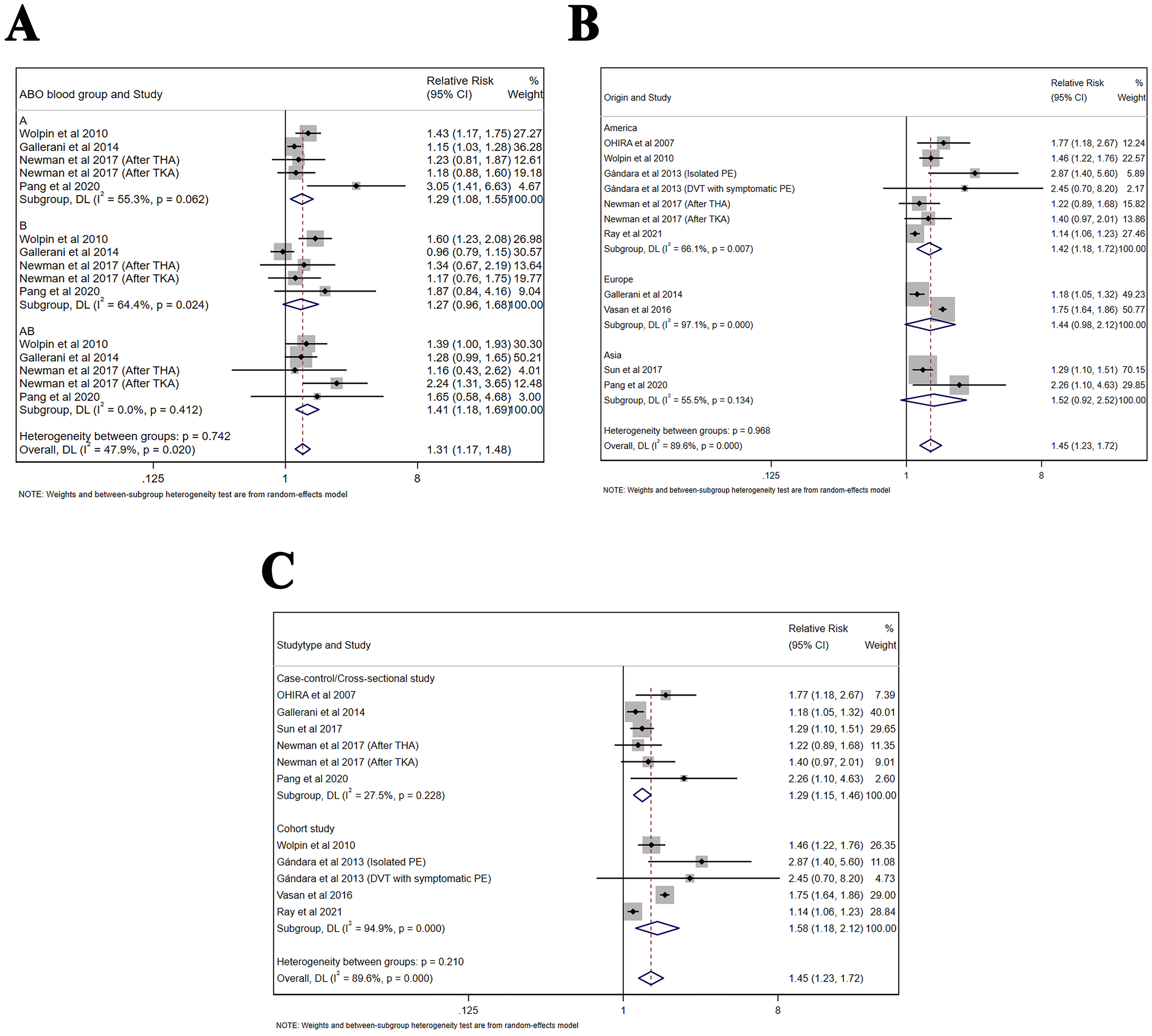
Subgroup Analysis of the Association Between ABO Blood Group and PE. (A) ABO Subgroup. (B) Origin. (C) Study Type.
Subgroup Analyses Stratified by ABO Subtype, Origin and Study Type.
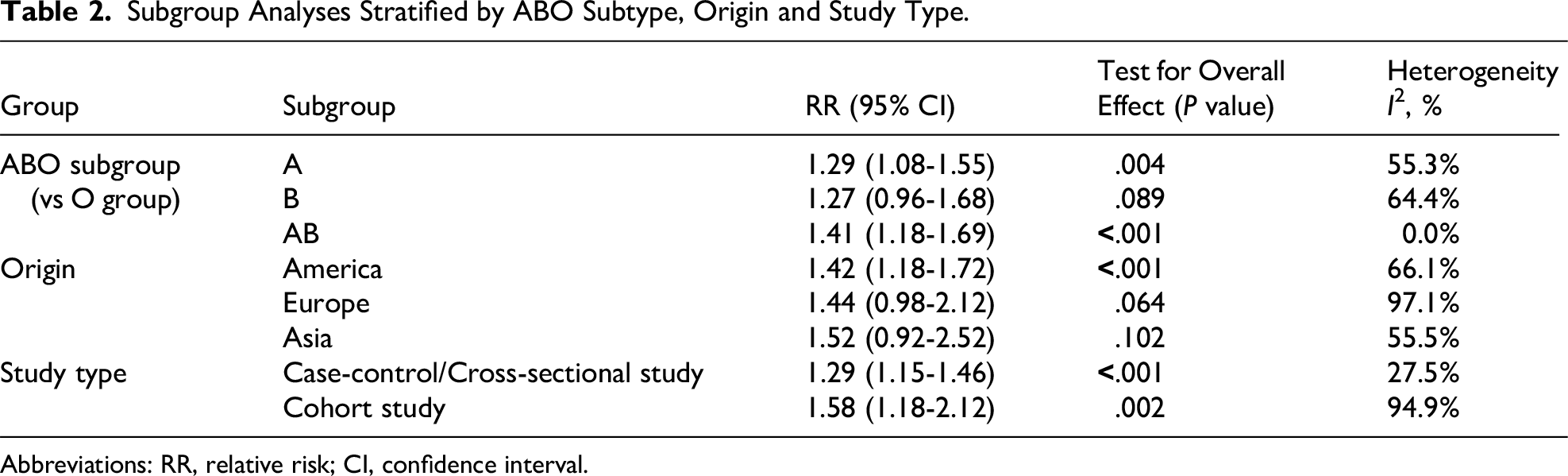
Abbreviations: RR, relative risk; CI, confidence interval.
Quality of Evidence
In the case of outcomes examined by both cross-sectional/case–control and cohort studies, the evidence quality was rated as “very low” (Table 3). There was no validation of high-quality evidence. The evidence was downgraded, mainly due to limitations stemming from nonrandomized controlled designs, substantial heterogeneity within the whole analysis, and the presence of publication bias.
Quality of Evidence.
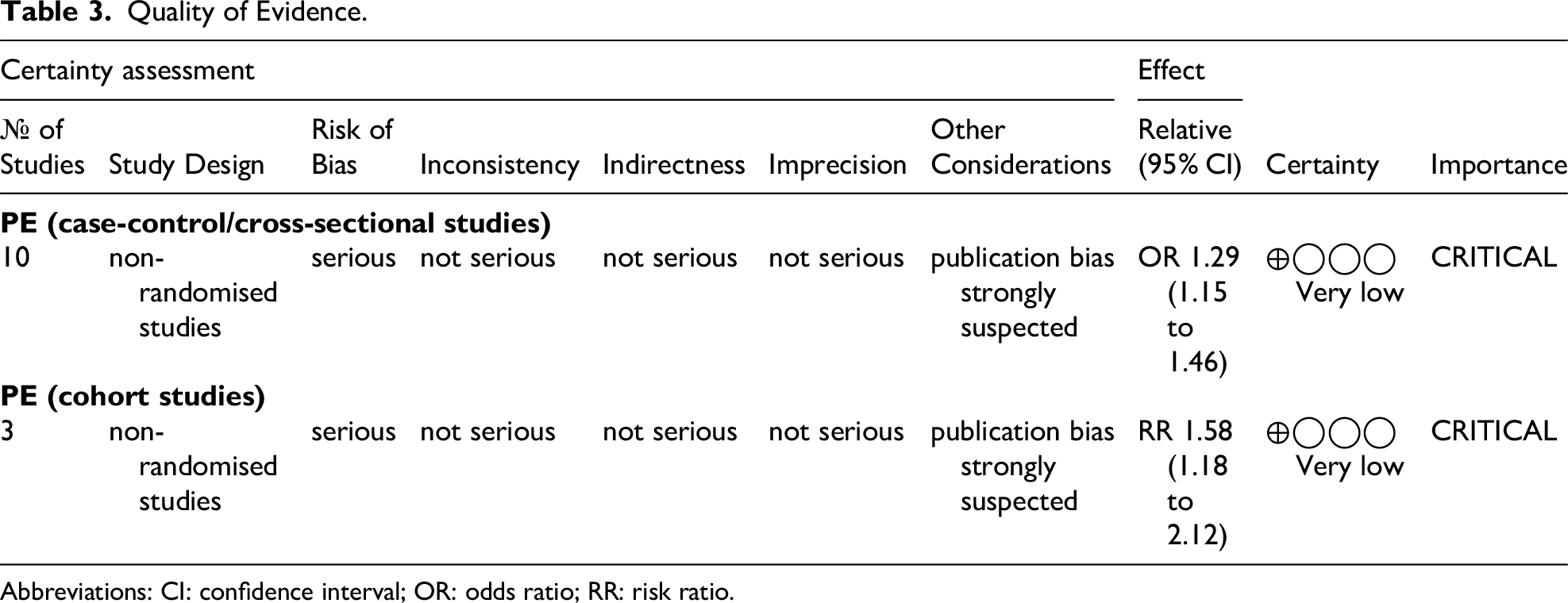
Abbreviations: CI: confidence interval; OR: odds ratio; RR: risk ratio.
Discussion
This meta-analysis of nine studies demonstrated a significant association between the non-O blood group and an elevated risk of PE in both case–control/cross-sectional and cohort studies. Despite the heterogeneity among the studies, sensitivity analyses indicated that the results were tenable. Only studies from America supported the above association. A and AB blood types, but not the B blood type, resulted in a statistically significant increase in the development of PE. However, the limited number of studies included in this meta-analysis prompted more population-based studies to verify this association.
The exact etiology for the increased risk for PE in patients with non-O blood type is still obscure. However, it has been estimated that the plasma concentrations of von Willebrand factor (vWF) and the level of the procoagulant factor VIII (FVIII) might be vital mediators of this association. Previous studies demonstrated that increased levels of vWF and FVIII were statistically significant in the third week of life in non-O neonates compared with type O neonates.28,29 Klarmann et al reported a significant increase in FVIII:C, VWF:Ag, and VWF:RCo in a non-O group population beginning in childhood and in adolescence and adulthood. 30 The levels of VWFpp proteins in non-O populations are much greater in aging individuals. 29 Similar results were also reported in other related studies, which demonstrated that blood group non-O was associated with higher VWF and FVIII levels than was blood group O.31–33
With respect to the associations among FVIII, VWF and thrombosis, it has long been recognized that higher levels of FVIII and VWF are associated with the risk of VT.34–36 The effect of VWF on the risk of venous thrombosis is mediated by the FVIII concentration. 37 Other studies have shown that VWF and FVIII are independently associated with VT in a dose-dependent manner. 38 High VWF levels also have a strong synergistic effect with low ADAMTS13 activity on DVT risk. 39 The biochemical mechanisms underlying FVIII levels and the risk of VT are only partially understood. One potential reason is that an increase in FVIII accelerates the formation of thrombin and fibrin, which is supported by the observation of the association between high FVIII levels and thrombin generation markers, namely, prothrombin fragments 1 + 2 and the thrombin-antithrombin complex. 40 Another possible mechanism is that FVIII could enhance the resistance of the anticoagulant effect of activated protein C (APC) through deactivation of activated factors V and VIII. 41
Our study had several limitations. Even after adjusting the estimates in all the included studies, various unmeasured confounding factors and biases remained. These included genetic variations, lifestyle-related factors, and the exclusion of articles written in languages other than English. Additionally, according to the GRADE assessment, the evidence was of extremely low certainty. This could be partly explained by the nonrandomized nature of the study design and the likelihood of publication bias. In specific subgroup analyses, the number of included studies was still limited. Hence, there is a need to carry out more population-based research to confirm these relationships.
Conclusion
Individuals in the non-O group were associated with an increased risk of PE compared with those in the O group, both in case–control/cross–sectional and cohort studies. Even with the exclusion of two studies that might have caused instability in the analysis, the association remained significant. Both A and AB, but not the B blood group, conferred an increased risk of PE. However, to offer more conclusive and trustworthy evidence, it is essential to conduct additional high-quality studies to validate our results.
Footnotes
Author Contributions
ZH W and XD W conceptualized the study and developed the protocol. ZH W and XD W conducted the literature search. XJ W and XD W selected the studies and extracted the relevant information. ZH W, XJ W, and XD W synthesized the data. XJ W and ZH W drafted the initial version of the paper, and all authors reviewed and made critical revisions to subsequent drafts of the paper. The final version was approved by all authors. The corresponding author confirms that all listed authors meet the criteria for authorship and that no eligible authors have been excluded.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the study are available from the corresponding author on reasonable request.