
Abstract
Create and evaluate a scoring system to detect early moderate/severe bleeding in acute promyelocytic leukemia (APL).
Methods
The study used 89 APL patients from Shanxi Bethune Hospital (2014/01-2024/10) for development and 48 APL patients from Tianjin Medical University General Hospital (2021/08-2024/08) for validation. Logistic regression was used to analyze independent risk factors and develop a scoring system based on odds ratios, with ROC curves assessing the AUC. Both sets were classified into low and high risk using the system's cut-off, and the incidence of moderate/severe bleeding in each group was calculated. The scoring system's relationship with the ISTH DIC score and their combined diagnostic efficacy for DIC and bleeding events in APL patients were evaluated using AUC, specificity, and sensitivity.
Results
In the development cohort, 15.7% (14 cases) had moderate/severe bleeding, while the validation cohort had 14.6% (7 cases). Multivariate logistic regression identified LDH levels ≥538 IU/L, fibrinogen <0.95 g/L, and D-Dimer ≥6865 ng/mL as independent risk factors for early moderate/severe bleeding in APL patients. The new warning scoring system had an AUC of 0.899 in the development group and 0.937 in the validation group. High-risk patients in both cohorts were significantly more likely to experience moderate/severe bleeding than low-risk patients (p < .001). The ISTH DIC score is significantly linked to both bleeding severity and the warning scoring system.
Conclusions
The warning scoring system shows potential for predicting the risk of moderate/severe bleeding in APL patients; however, further prospective validation studies are necessary to substantiate its efficacy.
Introduction
Acute promyelocytic leukemia (APL), a subtype of acute myeloid leukemia,
1
is characterized by the PML/RARα or RARα/PML fusion due to t (15;17) translocation. Despite being highly treatable with all-trans retinoic acid (ATRA) and arsenic trioxide (ATO) or chemotherapy,
2
early treatment failure often results from bleeding, particularly intracranial, within 30 days of diagnosis.3,4 About 80% of APL patients experience early-stage coagulopathy; Disseminated intravascular coagulation (DIC) can even occur at the onset of the disease.
5
The exact cause of early bleeding in APL patients is unclear but may involve high tissue factor levels, changes in the fibrinolytic system, and infections or inflammation.6,7 It's important to detect early severe bleeding in APL patients and provide timely treatment based on the underlying causes. Several studies have reported severe bleeding markers in APL patients, but no consistent predictors of fatal hemorrhage risk have been identified,4,8–16 as shown in Table 1. While DIC is often used to assess bleeding severity, its results remain inconclusive.10,13 Thus, there is an urgent need for a reliable risk assessment model for predicting fatal bleeding. This paper reviews the literature and, in cooperation with Tianjin Medical University General Hospital, develops a model and initiates a multicenter study with specific objectives:
Create a warning scoring system for moderate/severe bleeding in APL patients at our hospital Validate this scoring system using data from Tianjin Medical University General Hospital Analyze the relationship between the ISTH score, bleeding severity, and our warning score system for moderate/severe complications.
Key Findings from Studies on Predictors of Major or Fatal Bleeding in APL are Presented. Abbreviations: FIB, Fibrinogen; WBC, White Blood Cell; PLT, Platelets; FDP, Fibrin Degradation Product; ISTH, International Society on Thrombosis and Hemostasis; APTT, Activated Partial Thromboplastin Time; D-D, D-Dimer; DS, Differentiation Syndrome; LDH, Lactate Dehydrogenase.

Patients and Methods
Patients
We conducted a retrospective review of medical records for patients treated in the Hematology Department of Shanxi Bethune Hospital from 2014/01 to 2024/10 and Tianjin Medical University General Hospital from 2021/08 to 2024/08. We identified 89 newly diagnosed APL patients at Shanxi Bethune Hospital and an additional 48 cases at Tianjin Medical University General Hospital, diagnosed based on a reciprocal translocation between chromosomes 15 and 17 and/or PML/RARα rearrangements. 17 The exclusion criteria included, not meet APL diagnostic criteria, incomplete data, treatment for APL before admission, severe organ issues, certain diseases, malignancies, pregnancy, and end-stage disease. The research flowchart is shown in Figure 1. Demographic, laboratory, and clinical data were collected from our Hospital Information System using a standardized form. The study received approval from the Ethics Committees of Shanxi Bethune Hospital (YXLL-2024-200) and Tianjin Medical University General Hospital (IRB2024-YX-516-01).

Flowchart Showing the Patients Included in the Study.
Laboratory Procedures
After admission, we gathered lab data for all patients, including routine blood tests (white blood cell, neutrophil, lymphocyte, monocyte, platelet counts, hemoglobin), coagulation profile (D-dimer, prothrombin time (PT), activated partial prothrombin time, fibrinogen, plasma protamine para-coagulation test (3p test)), and serum biochemical tests (LDH). The international society on thrombosis and hemostasis (ISTH) scoring system was used to diagnosis DIC, which is based on four laboratory parameters and the presence of a predisposing condition. It includes elevations in D-dimer (or other fibrin-related markers), prolonged PT, and reductions in platelet count and fibrinogen concentration. 18
Assessment of Bleeding and Risk Stratification
Bleeding severity in newly diagnosed APL patients was assessed using the World Health Organization (WHO) grading system 19 within the first 30 day, as most fatal hemorrhages occur within four weeks of starting induction therapy, particularly in the first week. 3 WHO grades 0-2 denote no/mild bleeding, while grades 3-4 indicate moderate/severe bleeding. APL risk stratification follows Chinese guidelines: low risk (WBC <10 × 109/L, PLT >40 × 109/L), intermediate risk (WBC <10 × 109/L, PLT <40 × 109/L), and high risk (WBC >10 × 109/L). 20
Treatment Strategies
Patients diagnosed with APL via bone marrow examination should begin chemotherapy immediately. They are prescribed oral ATRA (25 mg/m2/day) with either intravenous ATO (0.16 mg/kg/day) or compound Huangdai tablet (60 mg/kg/day) until complete remission. If WBC exceeds 10 × 109/L, anthracyclines or cytarabine (Ara-C) may be used to manage hyperleukocytosis. 20 Dexamethasone (10 mg every 12 h) is given as a preventive measure for suspected or confirmed differentiation syndrome. To treat severe bleeding and anemia, transfusions of fresh frozen plasma, cryoprecipitate, blood components, and fibrinogen were administered.
The Development and Verification of the new Warning Scoring System for Bleeding Severity
89 cases recruited from Shanxi Bethune Hospital constituted the “development set” for the purpose of constructing the prediction model and scoring system. An additional 48 cases from Tianjin Medical University General Hospital were designated as the “validation set” to assess the predictive efficacy of the scoring system. Within the development set, independent risk factors for moderate/severe bleeding were identified through logistic regression analysis. Subsequently, these selected predictive variables were utilized to formulate a preliminary risk factor model, with the contribution of each risk factor represented as odds ratios (ORs), assigning a total score of 10. To validate the scoring system established from the development set, each APL patient in the validation set was scored based on these risk factors to obtain a total score. The sensitivity, specificity, and area under the curve (AUC) were then calculated to evaluate the accuracy and effectiveness of the bleeding warning score system. Patients with scores exceeding the cut-off value were predicted to have a high likelihood of moderate/severe bleeding, whereas those with scores below the cut-off value were predicted to have no/mild bleeding. Furthermore, the numerical characteristics of the warning score for each group of APL patients, categorized by varying ISTH DIC scores, were compared against the established cut-off value. This comparison aimed to ascertain the correlation between the ISTH DIC score and the newly developed early bleeding warning scoring system.
Statistical Analysis
Statistical analyses were performed with SPSS 27.0. Continuous variables were reported as mean ± SD or median (range), while categorical variables were shown as percentages. Differences between groups were assessed using the Chi-square test for categorical variables, the t-test for normally distributed continuous variables, and the Wilcoxon test for non-normally distributed continuous variables. A multivariate logistic regression analysis was conducted to identify independent risk factors and create a warning scoring system. The ROC curve analysis, including AUC, optimal cut-off values, sensitivity, and specificity, assessed the effectiveness of these factors and the scoring system in differentiating between APL patients with no/mild bleeding and those with moderate/severe bleeding. A p-value of less than .05 indicated statistical significance.
Results
Clinical and Laboratory Characteristics
The development set included 89 newly diagnosed APL patients, as detailed in Table 2. The median age was 42 years (range 13-73), with 55.1% male. Bleeding was the most common admission symptom (54 patients), followed by fatigue and fever (33 patients each). During induction therapy, 89.9% experienced infections, primarily respiratory system (73 patients). Within 30 days of starting induction therapy, 79 patients (88.8%) experienced bleeding, primarily ecchymosis (54 patients), gingival bleeding (36 patients), and epistaxis (14 patients). 4/14 (28.57%) of the severe bleeding cases resulted in fatality. Initial blood tests showed anemia and low platelets, with a median platelet count of 19.0 × 109/L and hemoglobin at 78 g/L. Coagulation tests indicated poor function, with a median PT of 14.6 s, mean APTT of 29.0 ± 3.1 s, median fibrinogen at 1.42 g/L, and median D-dimer at 5353 ng/mL. The LDH values closely related to tumor burden was 293.60 IU/L (94.70-2105.30 IU/L).
Baseline Characteristics of Patients with APL.

Abbreviations: WBC, White Blood Cell; PT, Prothrombin Time; APTT, Activated Partial Thromboplastin Time; FIB, Fibrinogen; D-D, D-Dimer; FDP, Fibrin Degradation Product; LDH, Lactate Dehydrogenase; 3p Test, Plasma Protamine Para-Coagulation Test.
Comparison of Baseline Characteristics of no/Mild and Moderate/Severe Bleeding Groups in APL Patients
In this study, 89 patients were included in the development set, with 14 (15.7%) experiencing moderate/severe bleeding. ROC curve analysis identified cut-off values for the laboratory indicators. Hemoglobin, platelet, and APTT with AUCs below 0.5 were excluded. The remaining indicators were grouped by cut-off values, and univariate analysis showed that in the development set, higher risk stratification, WBC count, lymphocyte count, PT, FDP, D-D, LDH, and early granulocyte ratio in bone marrow, as well as lower FIB levels were linked to moderate/severe bleeding in APL patients (P < .05). However, age, sex, time from onset to admission, monocyte count, 3p test, history of hypertension and diabetes, post-admission infection rate, and differentiation syndrome incidence showed no significant differences between the groups (all P > .05), as detailed in Table 3.
Characteristics of 89 APL Patients with no/Mild Versus Moderate/Severe Bleeding, with p < .05 Showing Significant Differences Between Two Groups. Abbreviations: WBC, white blood cell; PT, prothrombin time; APTT, activated partial thromboplastin time; FIB, fibrinogen; D-D, D-dimer; FDP, fibrin degradation product; LDH, lactate dehydrogenase; 3p test, plasma protamine para-coagulation test.

Analysis of independent risk factors and establish an early warning scoring system of moderate/severe bleeding in APL patients
A multivariate logistic regression analysis was conducted using indicators with significant results from the prior univariate analysis (see Figure 2). The model showed good fit (Hosmer-Lemeshow test: χ2 = 2.242, p = .524). Independent risk factors for moderate/severe bleeding in APL patients were identified as LDH ≥538 IU/L, FIB <0.95 g/L, and D-D ≥ 6865 ng/mL (p = .010, .022, .012). The odds ratios (OR) for each risk factor were collected and summed in the final model. The OR value proportion for each risk factor was calculated relative to the total OR values, assigning a total score of 10. This led to the creation of a warning scoring table for early moderate/severe bleeding risk in APL patients, as shown in Table 4.

Forest Plot Showing Multivariate Logistic Regression Analysis of Independent Risk Factors for Moderate/severe Bleeding.
Warning Scoring System for Moderate/Severe Bleeding in APL Patients.

Verification of early warning scoring system
We first examined the ROC curve for three independent risk factors and the new early warning scoring system, as shown in Figure 3. The new system had an AUC of 0.899 (0.791-1.000) in the development set, with 78.6% sensitivity and 93.3% specificity, and an AUC of 0.937 (0.846-1.000) in the validation set, with 71.4% sensitivity and 100% specificity. In comparison, The AUCs for three independent risk factors—LDH ≥538 IU/L, FIB <0.95 g/L, and D-D ≥ 6865 ng/mL—were 0.775, 0.690, and 0.755, respectively (see Table 5). A cut-off score of 5, based on the maximum Jorden index of new warning scoring system, was set as the optimal threshold, dividing patients into low-risk (0-5 scores) and high-risk (5-10 scores) groups.

ROC Curves of Three Independent Risk Factors and Warning Scoring System for Predicting Moderate/Severe Bleeding in Development and Validation Sets.
Results of the ROC Curve Analysis for Three Independent Risk Factors and the new Warning Scoring System in Both Development and Validation Sets.
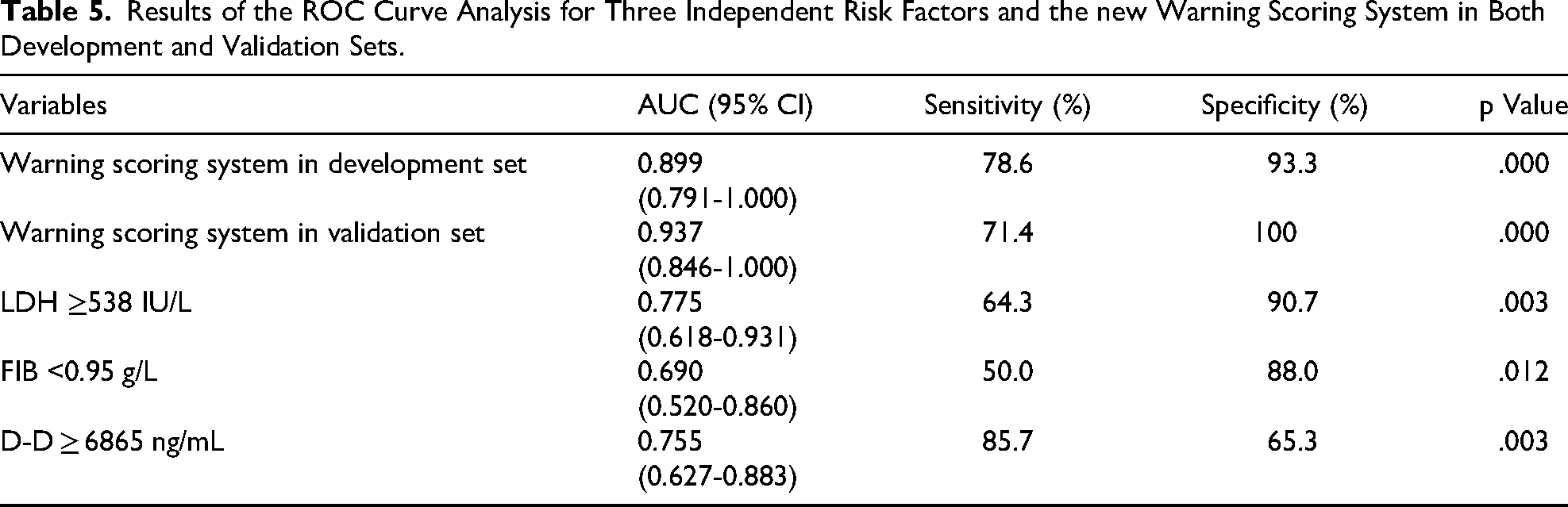
Table 6 shows that moderate/severe bleeding was significantly more common in high-risk patients than low-risk ones in both development and validation sets. To further illustrate the variation in the newly developed warning score system relative to the severity of bleeding events, the Mann–Whitney test was conducted. The results indicated that APL patients experiencing moderate/severe bleeding events had significantly higher warning scores compared to those with no/mild bleeding (P < .001). Additional details are presented in Figure 4.

Newly Developed Warning Scores Significantly Differ Between Patients with no/mild and Moderate/severe Bleeding (p < .001).
Occurrence of Moderate/Severe Bleeding in APL Patients Under Different Risk Stratification in the Development and Validation Sets.

The Correlation Between the ISTH DIC Score and Bleeding Severity, as Well as the Established Bleeding Warning Score System
We employed the ISTH DIC scoring system to assess DIC in all eligible patients at the time of diagnosis, defining a score of ≥5 as overt DIC. 18 Among 89 patients diagnosed with APL, 36 individuals (40.4%) exhibited overt DIC, characterized by ISTH DIC scores of ≥5. Furthermore, the numerical characteristics of warning score in each group of APL patients with different ISTH DIC score were further compared with the cut-off value as the critical value. the ISTH DIC score demonstrated a significant correlation with the severity of bleeding (p = .015) and the previously established warning score (p = .005), as illustrated in Figure 5A and 5B.

A: ISTH DIC Scores for Patients with no/Mild and Moderate/Severe Bleeding; B: ISTH DIC Scores for Patients with Warning Scores <5 and ≥5. C: ROC Curves of the Warning Scoring System, ISTH DIC score, and their Combination for Predicting Moderate/Severe Bleeding in the Development set. ISTH DIC Scores Significantly Correlated with Bleeding Severity and Warning Scores (p = .015 and p = .005, chi-Square Test).
In the development set, we conducted further calculations of the AUCs for the new warning scoring system, the ISTH DIC score, and their combination in diagnosing moderate/severe bleeding. The results are presented in Figure 5C. The AUC for the combined diagnostic approach was 0.916, which is significantly higher than the AUC of 0.759 for the ISTH DIC score (p = .013). However, no significant difference in diagnostic performance was observed when compared to the new warning scoring system alone (p > .05). The diagnostic sensitivities for moderate/severe bleeding were 78.6% for the new warning scoring system, 71.4% for the ISTH DIC score, and 85.7% for the combined approach. The specificities were 93.3%, 78.7%, and 92.0%, respectively, as detailed in Table 7.
Results of the ROC Curve Analysis for new Warning Scoring System, ISTH DIC Score and the Combined Approach.

Discussion
Severe bleeding remains a significant issue during APL induction therapy, with early mortality rates due to bleeding ranging from 5% to 41%,3,21 and our study showed 57.14%. Although our small sample size may introduce bias, the hemorrhage risk in APL patients is undeniable. However, identifying high-risk patients for early bleeding and providing preventive measures remains challenging. Numerous studies have focused on laboratory identification for early severe bleeding. Nevertheless, a single indicator may not fully assess bleeding risk. For instance, multiple studies have demonstrated the link between high WBC counts and severe bleeding in APL patients. 15 In contrast, Thakur et al present a differing perspective. 12 According to the findings of Song et al and Chang et al,13,22 APL patients with low platelet levels and prolonged APTT are more likely to experience bleeding. However, in our study, these two laboratory markers were not strongly associated with bleeding, potentially due to bias arising from insufficient data. Moreover, the patient data showed a median platelet count of 19 × 109/L (range: 3-182 × 109/L). Given that no significant differences between low platelet counts and bleeding can be attributed to the overall inhibition of platelets due to the prolonged interval from onset to admission (median: 10 days, range: 1-210 days). Therefore, it is crucial to create a risk assessment model to effectively and fairly identify patients at high risk for fatal bleeding. This study seeks to develop a warning scoring system for moderate/severe bleeding by incorporating all independent risk factors to improve prediction accuracy.
In our development set with 89 newly diagnosed APL patients, several factors were linked to bleeding events, including WBC ≥ 3.45 × 109/L, lymphocyte count ≥ 1.08 × 109/L, PT ≥ 15 s, FIB < 0.95 g/L, FDP ≥ 63 μg/mL, D-D ≥ 6585 ng/mL, LDH ≥ 538 IU/L, and early granulocyte ratio in bone marrow ≥ 87.5%. However, only LDH ≥ 538 IU/L, FIB < 0.95 g/L, and D-D ≥ 6865 ng/mL (all P < .05) were determined to be independent predictors of moderate/severe bleeding, aligning with previous studies.8,14,15 Scores were subsequently assigned based on the OR values of these three indicators. The new warning scoring system for diagnosing moderate/severe bleeding showed an AUC of 0.899 in the development group, with sensitivity of 78.6% and specificity of 93.3%, outperforming three independent indicators. In the validation set, the AUC was 0.937, with 71.4% sensitivity and 100% specificity, confirming the system's effectiveness. The warning scoring system is simple, convenient, and fairly accurate for assessing early moderate/severe bleeding risk in APL patients.
In early induction therapy for APL patients, bleeding is mainly due to the release of coagulant substances and fibrinolysis.7,23 Our early warning scoring system for bleeding severity includes two key biomarkers for coagulation and fibrinolysis, which are crucial for monitoring bleeding in APL patients and improving system accuracy. In addition, LDH's role in leukemia prognosis, tumor growth, and invasion is well-documented, and its predictive value for bleeding risk in APL patients has also been assessed. 24 Our study found that patients with moderate/severe bleeding often had LDH levels ≥538 IU/L, aligning with Kim's research. 25 These three independent risk factors are more effective in predicting bleeding risk when combined into an early warning scoring system than individually.
This study used the ISTH DIC criteria, valued for their simplicity and effectiveness in predicting poor outcomes, to assess DIC in APL patients.26,27 DIC is linked to worse prognosis in APL, affecting hospital stay, increasing sepsis risk, and major bleeding events.28,29 Rajpurkar et al identified an ISTH DIC score ≥ 6 as an indicator of early death and coagulopathy in pediatric APL. 10 However, Chang's study did not find a link between DIC and severe bleeding.13,30 Our study found a significant correlation between the ISTH DIC score, bleeding severity, and newly established warning scoring system (p < .05), which appeared to be consistent with clinical experience. The new warning scoring system, when combined with the ISTH DIC score, shows high sensitivity and a higher AUC for diagnosing early moderate/severe bleeding in APL patients. Furthermore, the AUC of the new warning scoring system in diagnosing moderate/severe bleeding in APL patients was higher than that of ISTH DIC score(p = .005). However, the AUC of the new system alone is similar to its combination with the ISTH DIC score for diagnosing moderate/severe bleeding. This finding underscores the diagnostic efficacy of our newly established early warning scoring system in identifying moderate/severe bleeding in APL patients
In addition, with only 14 moderate/severe bleeding cases (15.73%) compared to 26 (22.4%) in Chang's study, 13 our data may not be fully representative. Therefore, comprehensive studies and expert reviews are essential to clarify this issue, and the three risk factors in the warning system should be continuously monitored during induction treatment to assess their predictive value.
Conclusions
This study creats and validates a new warning scoring system for assessing bleeding severity in newly diagnosed APL patients through a multi-center retrospective analysis. The system effectively predicts moderate/severe bleeding complications, aiding early identification and timely treatment of high-risk patients. Further studies are necessary for clinical validation.
Footnotes
Ethical Considerations
Ethical statement is not applicable for this article.
Author Contributions
Xueqin Li analyzed results, created figures, and drafted the manuscript. Hongying Tang collected data from Tianjin Medical University General Hospital. Yu Lian guided the study and revised the manuscript. Xinlei Yang , Xinyao Liu and Wei Liu analyzed data, Yukai Jing designed the study and revised the manuscript. Each co-author contributed to the study or protocol development, and all authors approved the final version for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Yang Xinlei, Lianyu, Wang Limin, (grant number No. 202103021223400, No. 82100145, No.2022RC06, No. C2023402063, No. QN2022002).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed in this study are available on reasonable request to the corresponding author.
Financial Support and Sponsorship
This research was funded by grants from the Fundamental Research Program of Shanxi Province (No. 202103021223400), the National Natural Science Foundation of China (No. 82100145), Shanxi Bethune Talent Foundation Project (No.2022RC06), Biological Agricultural Joint Fund of Natural Science Foundation of Hebei Province (No. C2023402063) and Scientific and technological research projects in colleges and universities Foundation of Hebei Province (No. QN2022002).