
Abstract
Background
this study aimed to investigate the efficacy of recombinant human thrombopoietin (rhTPO) in the treatment of sepsis-associated thrombocytopenia, and to evaluate its impact on coagulation function, inflammatory markers, platelet (Plt) count, and patient prognosis.
Methods
a total of 144 patients with sepsis-associated thrombocytopenia, admitted to our hospital between 2022 and 2023, were selected for the study. The patients were randomly divided into two groups using a random number table: the control group (Group C, n = 72) and the research group (Group R, n = 72). The Group C received standard treatment, while the Group R received rhTPO in addition to standard care. We compared the general demographic data, Acute Physiology and Chronic Health Evaluation II (APACHE II) scores, coagulation parameters, serum levels of Toll-like receptor 4 (TLR4), interleukin-6 (IL-6), serum creatinine (SCr), tumor necrosis factor-alpha (TNF-α), Plt count, transfusion volume, treatment duration, incidence of complications, and mortality rates between the two groups.
Results
there were no significant differences in the general demographic characteristics between the two groups (P > 0.05). After treatment, the APACHE II scores in both groups significantly decreased, with a more pronounced reduction observed in the Group R. Coagulation function indicators, including activated partial thromboplastin time (APTT), fibrinogen (FIB), plasminogen activator inhibitor-1 (PAI-1), antithrombin III (AT-III), protein C, thrombomodulin (TM), and Plt factor 4 (PF4), showed greater improvement in the Group R compared to the Group C (P < 0.05). The serum levels of TLR4, IL-6, and TNF-α in the Group R were significantly lower than those in the Group C (P < 0.05), whereas no significant difference in SCr levels was observed between the groups (P > 0.05). The Plt count in the Group R began to significantly increase on day 3 of treatment, and was consistently higher than that in the Group C on days 3, 5, and 7 (P < 0.05). The Group R required significantly fewer red blood cell transfusions compared to the Group C and did not require Plt suspension (P < 0.05). No significant differences were found between the groups in terms of mechanical ventilation time, intensive care unit (ICU) length of stay, and total hospital stay (P > 0.05). However, the ICU and overall hospital mortality rates were significantly lower in the Group R than in the Group C (P < 0.05). Multivariate logistic regression analysis indicated that rhTPO treatment was an independent protective factor for reducing mortality (OR = 0.475, P = 0.042).
Conclusion
rhTPO treatment effectively improves coagulation function and inflammatory status in patients with sepsis-associated thrombocytopenia, increases Plt count, reduces transfusion requirements, and lowers mortality. These findings suggest that rhTPO has significant clinical application value in the management of this condition.
Keywords
Background
Sepsis is typically caused by bacterial infections and is a severe complication in patient post-surgery, particularly in those with burns or infections. When bacteria enter the bloodstream and trigger a systemic inflammatory response, it leads to organ dysfunction and, in some cases, may result in fatalities. 1 Sepsis progresses rapidly and poses a significant risk. In China, millions of postoperative patients develop sepsis annually, with a mortality rate as high as 30%.2,3 The mortality rate of sepsis-induced thrombocytopenia is 15.6%. 4 Sepsis impairs the body's resistance and disrupts the immune system. Common symptoms of sepsis include hypotension, rapid breathing, fever, and leukocytosis. Thrombocytopenia further exacerbates coagulation abnormalities, increasing the risk of bleeding. Research has proposed that thrombocytopenia is an independent predictor of adverse outcomes in sepsis patients and may elevate mortality rates. 5 Hence, effective treatment of thrombocytopenia is crucial for improving the prognosis of sepsis patients.
In patients with sepsis, immune system dysregulation primarily manifests as sustained activation of the body's inflammatory response. The release of inflammatory mediators in the patients’ serum triggers inflammatory reactions, including vasodilation, increased vascular permeability, and leukocyte aggregation, which are partly the body's protective mechanisms against infection. 6 However, due to sustained inflammatory stimulation, platelet (Plt) aggregation and destruction increase. Additionally, certain inflammatory cytokines such as interleukin-1 and tumor necrosis factor-alpha inhibit the development of megakaryocytes and the generation and release of Plts in the bone marrow. This leads to a decrease in Plt count, thereby affecting normal coagulation function. 7 Thrombocytopenia leads to coagulation dysfunction. In the context of infection, the pathogen releases pathogen-associated molecular patterns (PAMPs) when it disrupts the host's circulation, and host cells release damage-associated molecular patterns (DAMPs) upon being attacked by pathogen.8,9 PAMPs and DAMPs are recognized and bound by specific pattern recognition receptors (PRRs) on the surface of monocytes and macrophages, leading to activation of PRRs. Activated monocytes and macrophages release cytokines and chemokines, which further activate neutrophils, Plts, and endothelial cells. Additionally, activated monocytes release vesicles carrying procoagulant tissue factors and phosphatidylserine, which upon entering the circulatory system activate the extrinsic coagulation pathway. 10 When neutrophils are activated, they release extracellular fibers composed of decondensed chromatin and granule proteins, known as neutrophil extracellular traps (NETs), which play a role in limiting infections. However, excessive release of NETs can lead to a procoagulant state in the host. 11
Recombinant human thrombopoietin (rhTPO) is a biopharmaceutical that stimulates Plt production. It was introduced to the market in 2005 and has found widespread clinical application in the treatment of thrombocytopenia. 12 Utilizing gene recombination technology, rhTPO is expressed in animal systems, purified, and modified to closely resemble the structure of endogenous Plt growth factors in the human body. RhTPO acts on the Plt receptor c-MPL, activating downstream pathways to stimulate hematopoietic cell proliferation, induce megakaryocyte formation, promote megakaryocyte nuclear division, and accelerate Plt production. Research has shown that rhTPO can increase the number of megakaryocytes in the bone marrow and enhance the speed at which stem cells enter the division phase. 13 RhTPO can stimulate immune cell proliferation, regulate the patient's immune system, improve T lymphocyte function, and reduce Plt consumption. Currently, the application of rhTPO in the treatment of immune thrombocytopenia is extensive. Yu et al 14 treated pregnant women with immune thrombocytopenia using rhTPO and found that it effectively alleviated thrombocytopenia symptoms in pregnant women, with no adverse events observed in newborns. 14 Investigations have delved into the application of rhTPO for managing aplastic anemia. The research revealed that rhTPO facilitates Plt regeneration by activating the STAT3/STAT5 signaling pathway and modulating apoptosis-related mediators. Additionally, it induces the proliferation of 32D cells treated with serum from individuals with aplastic anemia, concurrently mitigating cell apoptosis. 15 Furthermore, rhTPO possesses the potential to inhibit the production of inflammatory factors and alleviate inflammatory responses, which could potentially enhance the outlook for individuals suffering from sepsis.
This study sought to assess the effectiveness and safety of rhTPO in addressing thrombocytopenia associated with sepsis. Furthermore, the investigation aimed to explore the impact of rhTPO on enhancing coagulation function and modulating the levels of inflammatory factors. The ultimate goal was to provide more effective treatment options for clinical practice, thereby improving the prognosis of patients with sepsis.
Materials and Methods
Research Object
A total of 144 patients with sepsis-associated thrombocytopenia, admitted to our hospital between 2022 and 2023, were selected for the study. The patients were randomly assigned to either the control group (Group C) or the research group (Group R), with 72 patients in each group. In the Group C, there were 39 male and 33 female patients, with a mean age of (56.65 ± 15.26) years. The underlying conditions included 25 cases of severe pneumonia, 26 cases of intra-abdominal infection, 15 cases of severe pancreatitis, 3 cases of infection due to severe burns, and 3 cases of severe intracranial infection. Additionally, 17 patients developed shock, and 11 patients experienced disseminated intravascular coagulation (DIC). In the Group R, there were 37 male and 35 female patients, with a mean age of (57.17 ± 16.34) years. The underlying conditions included 28 cases of severe pneumonia, 25 cases of intra-abdominal infection, 13 cases of severe pancreatitis, 3 cases of infection due to severe burns, and 3 cases of severe intracranial infection. Moreover, 14 patients in the Group R developed shock, and 10 patients had DIC. The general characteristics of all patients differed slightly (P > 0.05). This study had been approved by the hospital's ethics committee, and all patients and their guardians had provided informed consent.
Patients enrolled had to satisfy all the following conditions: patients were included based on the diagnostic criteria for sepsis as per the Third International Consensus: New Definitions for Sepsis and Septic Shock. 16 This included patients with a severe infectious condition and sequential organ failure assessment (SOFA) score ≥2, along with a Plt count less than 100 × 109/L. All patients received standard care in accordance with the International Sepsis Survivors Campaign Guidelines.
Patients with any of following conditions had to be excluded: those with a history of allergies to the drugs used in this study, those with hypercoagulable blood, individuals with immune system disorders, pregnant patients, individuals with a history of organ transplantation, and those who had recently used anticoagulant medications were excluded from the study. Patients who had recently used anticoagulant or anti-Plt medications (such as low-dose heparin or aspirin); patients who had recently received high-dose intravenous immunoglobulin therapy.
Research Process
The research process is detailed in Figure 1.

Research flow chart.
Therapeutic Methodologies
All patients who were enrolled received standard treatments, including fluid resuscitation, anti-infection measures, nutritional support, and other routine therapies. In the Group C, patients received the aforementioned standard treatments following the onset of sepsis. In Group R, rhTPO treatment was initiated with a subcutaneous injection of 15,000 U of rhTPO (specification 15,000 U/1 mL, approved by China Food and Drug Administration, license number S20050048, manufactured by Shenyang Sansheng Pharmaceutical Co., Ltd), once daily. During treatment, medication was discontinued if the patient's Plt count increased by 50 × 109/L compared to baseline or reached ≥100 × 109/L. Plt suspension therapy (obtained through single-donor Plt collection and suspended in plasma) was administered if the Plt count dropped below 20 × 109/L. Fresh frozen plasma (FFP) was transfused if the patient exhibited significant bleeding signs and prolongation of prothrombin time (PT) by more than 3 s or activated partial thromboplastin time (APTT) by more than 10 s. Normal reference values for PT are 11.0–13.0 s (time) and 75.0%-115.0% (activity). Normal APTT reference values are 25.0–37.0 s. However, while laboratory indicators are important, they may not fully reflect the patient's clinical condition. Therefore, clinicians also consider the actual bleeding situation when deciding on transfusion or other treatments. Packed red blood cells (PRBCs) were transfused when the patient's hemoglobin level dropped below 70 g/L.
Outcome Measures
The severity of patients’ conditions before and one week after treatment was recorded and evaluated using the Acute Physiology and Chronic Health Evaluation (APACHE) II score, with higher scores indicating poorer recovery. Additionally, observations were made and recorded for parameters including mechanical ventilation duration, ICU stay duration, and total treatment duration during the patient's treatment course. The amounts of fresh plasma, Plt suspensions, and concentrated red blood cells transfused to patients were also monitored and documented. Following completion of treatment, patients did not receive any further unconventional interventions, and they were followed up for six months. The incidence of complications and mortality rates were observed and recorded, with a specific focus on complications such as myocardial infarction (MI), deep vein thrombosis (DVT), ischemic stroke (IS), and pulmonary embolism (PE).
Inspection Indicators
Blood samples were collected from fasting venous blood of patients, 6 mL each, before and one week after treatment. The samples were centrifuged for ten minutes for a collection of serum, which was subsequently stored for analysis. The ADVIA® 2120i hematology analyzer (manufacturer: Siemens Medical Systems Limited) was employed to measure the Plt count of patients before they were treated and at 1, 3, 5, and 7 days after relevant intervention. The patients’ coagulation parameters, including PT, APTT, and fibrinogen (FIB) concentration, were analyzed using the CX-9000 fully automated coagulation analyzer (Mindray Medical). Serum levels of toll-like receptor 4 (TLR4), interleukin-6 (IL-6), serum creatinine (SCr), and tumor necrosis factor-alpha (TNF-α) were determined using enzyme-linked immunosorbent assay (ELISA).
Statistical Analysis
Data were analyzed using SPSS version 26.0. Continuous data were presented as mean ± standard deviation (x−± s) and were compared between groups using the t-test. Categorical data were expressed as percentages (%) or the number of cases (n) and were compared between groups using the χ2 test. P < 0.05 indicated statistical significance.
Results
Comparison of General Demographic Data Between the Two Groups
In Table 1, there were no significant differences between the two groups in terms of general demographic characteristics, underlying diseases, disease severity, infection types, laboratory indicators, and treatment measures, indicating that the baseline characteristics of the patients in the two groups were comparable following random assignment.
Comparison of General Demographic Data Between the Two Groups.

Changes in APACHE II Scores of Patients
Comparing the APACHE II scores of the two patient groups before treatment revealed negligible differences (P > 0.05), indicating no statistical significance. Nevertheless, after one week of treatment, both patient groups exhibited a drastic reduction in their APACHE II scores when compared to their pre-treatment scores (P < 0.05), signifying statistical significance. Nonetheless, no notable differences were observed between the two patient groups when their APACHE II scores were compared (P > 0.05). Notably, the patients of Group R had lower APACHE II scores after treatment than the patients of Group C post-treatment (Figure 2).

Comparison of APACHE II scores of patients in different groups. Note: *P < 0.05 before treatment.
Comparison of Coagulation Parameters Before and After Treatment Between the Two Groups
In Table 2, after one week of treatment, the PT in both groups was significantly shortened (P < 0.05), but no significant difference was observed between the groups (P = 0.802). The APTT was also significantly shortened in both groups (P < 0.05), with Group R showing a significantly lower APTT than Group C (P = 0.028), indicating a more pronounced improvement in coagulation function in Group R. The FIB levels decreased in both groups (P < 0.05), with a greater reduction in Group R (P = 0.003), suggesting a reduction in FIB consumption in Group R. Plasminogen activator inhibitor-1 (PAI-1)levels decreased in both groups (P < 0.05), with a more significant decrease in Group R (P = 0.000), indicating an earlier recovery of fibrinolytic activity in Group R. antithrombin III (AT-III) and protein C levels increased in both groups (P < 0.05), and the levels in Group R were significantly higher than those in Group C (P = 0.002, P = 0.009), reflecting a more pronounced improvement in anticoagulant function in Group R. Thrombomodulin (TM) and Plt factor 4 (PF4) levels decreased in both groups (P < 0.05), with a more significant reduction in Group R (P = 0.002, P = 0.001), suggesting a more notable repair of endothelial injury and reduced Plt activation in Group R.
Comparison of Coagulation Parameters Before and After Treatment Between the Two Groups.

Note: *P < 0.05, **P < 0.01.
Comparison of Serum TLR4, IL-6, SCR, and TNF-α Levels
Statistical results indicate that there were negligible differences in serum levels of TLR4, IL-6, SCr, and TNF-α between patients in Groups C and R before they were treated (P > 0.05). Nevertheless, following one week of treatment, both groups of patients exhibited a great reduction in TLR4, IL-6, SCr, and TNF-α levels relative to the pre-treatment levels (P < 0.05), indicating statistical significance. In Group R, TLR4, IL-6, and TNF-α levels were markedly lower after treatment versus Group C (P < 0.05), demonstrating statistical significance. The post-treatment levels of SCr demonstrated slight differences in both patient groups (P > 0.05), indicating no statistical significance (Figure 3).

Comparison of serum TLR4, IL-6, SCR, and TNF-α levels. Note: *P < 0.05 before treatment; #P < 0.05 versus Group C.
Comparison of Plt
Statistical results are shown in Figure 4. The pre-treatment serum Plt counts differed inconsiderably between the patient in various groups (P > 0.05). Nevertheless, one week after the patients were treated, both groups of patients demonstrated a drastic increase in serum Plt counts versus baseline (P < 0.05), showing statistical significance. In Group C, patients’ serum Plt counts started to greatly increase from the fifth day of treatment. In Group R, patients experienced a notable rise in serum Plt counts starting from the third day. Additionally, on the third, fifth, and seventh days, Group R patients exhibited a notable rise in serum Plt counts compared to Group C (P < 0.05), indicating statistical significance.
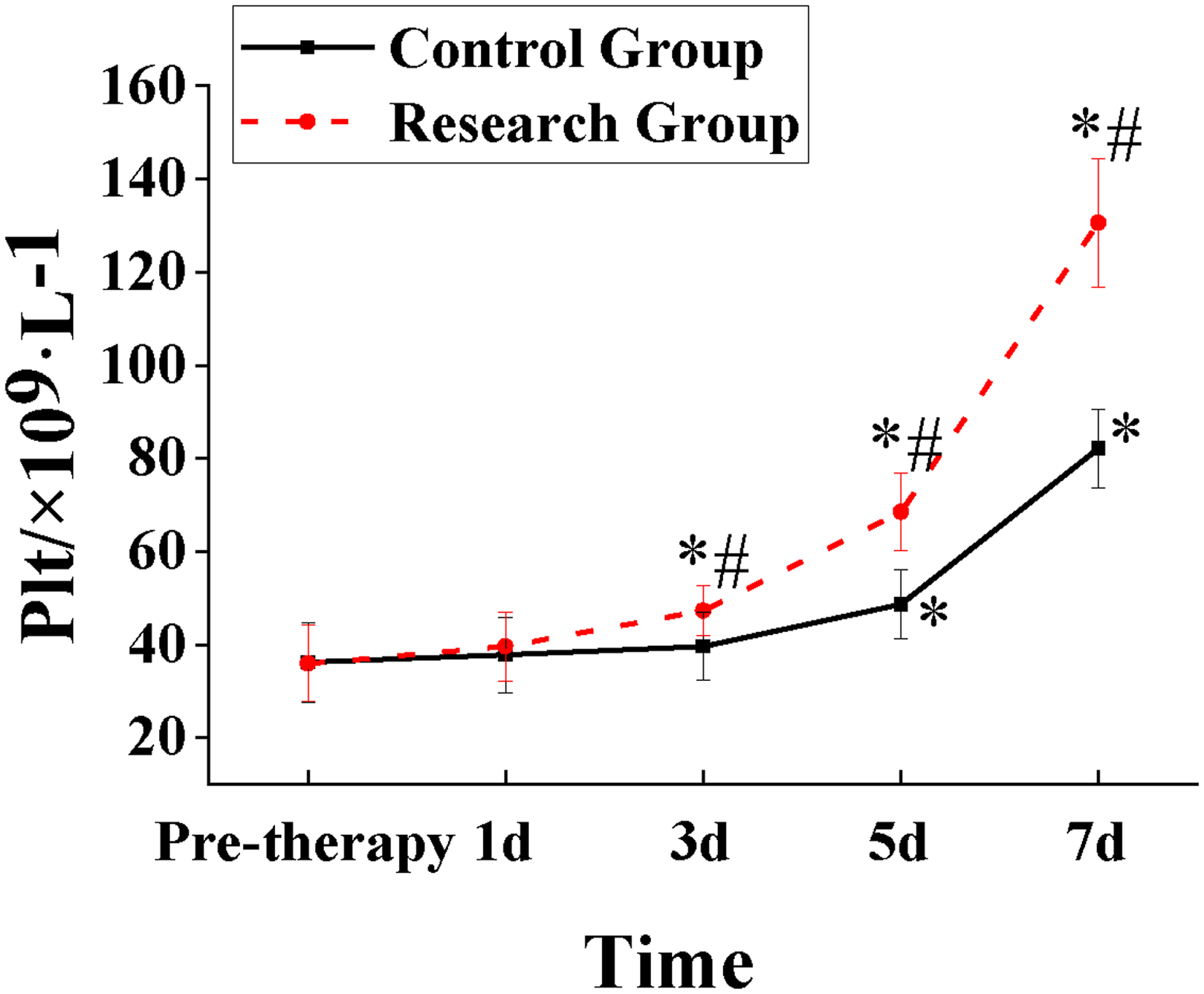
Comparison of Plt between patients in Groups C and R. Note: *P < 0.05 before treatment; #P < 0.05 versus Group C.
Comparison of Blood Composition Input During Treatment Between Two Groups of Patients
The statistical results are shown in Figure 5, indicating that the amount of PRBCs used in the Group R was significantly lower than that in the Group C (P < 0.05), demonstrating statistical significance. Additionally, patients in the treatment group did not receive Plt suspensions.

Changes in blood composition input of patients during different treatments. Note: *P < 0.05 before treatment.
Comparison of Treatment Time for Patients in Different Groups
Statistical results are depicted in Figure 6. During the treatment period, Group R exhibited slightly shorter mechanical ventilation time, ICU residence time, and total treatment time compared to Group C (P > 0.05). Nevertheless, no marked differences were observed between Groups R and Cin terms of mechanical ventilation time, ICU residence time, and total treatment time (P > 0.05), indicating no statistically significant significance.

Comparison of treatment time between patients in various groups.
Comparison of Complications and Mortality Rates Between the Two Groups
During the treatment period, neither of the two patient groups experienced complications such as MI, DVT, IS, or PE. Table 3 presents a comparison of the ICU and overall hospital mortality rates between the two groups. Group R, which received rhTPO treatment, had significantly lower ICU and overall hospital mortality rates compared to Group C (ICU mortality: P = 0.042, P < 0.05; overall hospital mortality: P = 0.047, P < 0.05).
Comparison of ICU and Overall Hospital Mortality Rates Between the Two Groups.

Univariate Analysis
The results of the univariate analysis (Table 4) indicated that age, SOFA score, APACHE II score, shock, DIC, Plt count, lactate level, mechanical ventilation before ICU admission, hemodialysis before ICU admission, and whether the patient received rhTPO treatment were significantly associated with mortality (P < 0.05). In contrast, no statistically significant differences were found for sex, BMI, underlying diseases (hypertension, diabetes, coronary artery disease, chronic kidney disease), hemoglobin, and C-reactive protein with respect to mortality (P > 0.05).
Univariate Analysis of Variables Associated with Mortality.

Multivariate Analysis
The results of the multivariate logistic regression analysis (Table 5) indicated the following. For each 1-year increase in age, the risk of death increases by 3.0% (OR = 1.030, P = 0.024). For each 1-point increase in SOFA score, the risk of death increases by 33.0% (OR = 1.330, P = 0.007). For each 1-point increase in APACHE II score, the risk of death increases by 17.1% (OR = 1.171, P = 0.028). The mortality risk in patients who developed shock was 2.401 times higher than in those who did not develop shock (OR = 2.401, P = 0.027). The mortality risk in patients with DIC was 2.123 times higher than in those without DIC, with a P value approaching significance (P = 0.051). For each 1 × 109/L decrease in Plt count, the risk of death increases by 1.8% (OR = 0.982, P = 0.046). For each 1 mmol/L increase in lactate level, the risk of death increases by 51.0% (OR = 1.510, P = 0.028). Patients who received rhTPO treatment had a 52.5% lower risk of death (OR = 0.475, P = 0.042), suggesting that rhTPO treatment independently reduces mortality risk.
Results of Multivariate Logistic Regression Analysis.

Discussion
Sepsis has emerged as a leading cause of patient mortality in the ICU, and the number of patients admitted with sepsis as well as those succumbing to the disease has been increasing yearly.17,18 Thrombocytopenia is one of the primary complications observed in septic patients, affecting 3% to 15% of ICU patients in hospitals. Interestingly, studies have shown that the occurrence of thrombocytopenia is not linked to the disease severity or the number of organ failures. 19 Nevertheless, patients with sepsis of traumatic or surgical origin exhibit a notably higher probability of developing thrombocytopenia, ranging from 35% to 41%. 20 The research findings indicated an inverse relationship between Plt count in critically ill patients and their mortality rate. Particularly, patients whose Plt counts remain below normal for more than four days after admission or those who experience a decrease in Plt counts for over 50% of their ICU stay have an increased risk of mortality. 21 Research of Abebe Gebreselassie et al 22 substantiates the significant association between sepsis and the development of thrombocytopenia. 22
The progressive development of sepsis-associated thrombocytopenia may lead to organ failure, which is one of the crucial factors contributing to patient mortality. 23 The primary treatment modalities for thrombocytopenia include transfusion of blood components such as plasma, PRBCs, and Plt suspensions. Typically, these treatments are considered when the Plt count drops below 20 × 109/L or when patients exhibit significant bleeding symptoms. Given the structural similarity of rhTPO to endogenous Plt growth factors, it can stimulate Plt production in the bone marrow. Hence, in the treatment of thrombocytopenia, administering rhTPO to patients is a viable therapeutic option. This study investigated the clinical efficacy and safety of rhTPO treatment for sepsis-associated thrombocytopenia. Parameters such as patients’ APACHE II scores, coagulation indicators, levels of TLR4, IL-6, SCr, TNF-α, and Plt counts in serum showed negligible differences between the groups. Hence, the research data were deemed worthy of exploration.
A study that included 681 patients investigated the effectiveness and safety of rhTPO in patients with sepsis-associated thrombocytopenia. The results revealed that rhTPO could greatly increase Plt counts and extend patients’ prognosis while reducing the need for blood product transfusions and ICU stay. 24 In this study, it was observed that one week after treatment, both Group R and Group C showed a drastic increase in Plt counts. Nevertheless, Group R exhibited notably higher Plt counts on the third, fifth, and seventh days versus Group C, indicating that the treatment in Group R may have had a more favorable impact on Plt recovery for the patients. These findings align with the results of the aforementioned study. The primary approach for treating patients with thrombocytopenia revolves around increasing Plt count. Transfusing patients with fresh plasma, concentrated red blood cells, and Plt suspensions can rapidly boost Plt numbers in the patient's bloodstream, reducing the risk of organ bleeding. However, transfusion of blood products carries risks such as infection and immune system attacks on the patient. Additionally, transfusions may lead to other adverse effects, including fluid overload (fluid retention), allergic reactions, transfusion-related acute lung injury (TRALI), and post-transfusion purpura. Therefore, before deciding on transfusion therapy, careful consideration of its potential risks and benefits is essential. Additionally, hospital blood supplies may be limited, or there may be a lack of blood products matching the patient's blood type, which presents challenges when opting for direct blood-based treatments. In contrast, rhTPO is primarily produced through recombinant gene expression and modification in animal cells, allowing for large-scale production. RhTPO can promote Plt production and modulate the patient's immune system, thereby reducing the patient's consumption of Plt suspensions. RhTPO, a biological agent, acts on megakaryocytes in the bone marrow by mimicking natural TPO. It enhances their differentiation and maturation, thereby increasing Plt production and release. RhTPO binds to TPO receptors on megakaryocytes, activates signaling pathways, and promotes Plt generation. This is particularly crucial for septic patients, as sepsis often leads to significant thrombocytopenia, increasing the risk of bleeding. In this study, it was observed that patients in Group R experienced a rapid increase in Plt count following the administration of rhTPO. Moreover, when compared to Group C, the transfusion requirements for fresh plasma, concentrated red blood cells, and Plt suspensions were considerably reduced, implying the enhanced effectiveness of the treatment strategy in Group R. These findings align with the results by Zhang et al, 25 demonstrating that rhTPO therapy leads to a reduction in Plt transfusion requirements. 25 Furthermore, in addition to its role in promoting Plt growth, research has revealed that rhTPO is associated with modulating the inflammatory response in sepsis patients. RhTPO stimulates Plt production, and Plts recruit leukocytes in a calcium-dependent manner through P-selectin. The expression of Plt P-selectin can stimulate Plt-leukocyte binding in whole blood. 26 Additionally, rhTPO can facilitate the release of reactive oxygen species, inducing monocytes and neutrophils to express IL-6. 27 In the study, although changes in coagulation parameters between Group R and Group C were not significant, the use of rhTPO may contribute to maintaining or slightly improving patients’ coagulation function, thereby reducing the risk of bleeding associated with thrombocytopenia. Additionally, there is an important consideration regarding patients with severe sepsis complicated by acute respiratory distress syndrome (ARDS). In these patients, Plt aggregation and sequestration in the pulmonary circulation may lead to microcirculatory dysfunction in the lungs, impairing gas exchange and reducing the ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2), while increasing the ratio of dead space to tidal volume (VD/VT). Although rhTPO treatment can increase Plt counts and improve coagulation function, it may exacerbate Plt aggregation in the lungs of septic patients with pulmonary infections, increasing the risk of microthrombus formation and further impairing gas exchange, potentially leading to higher mortality. This mechanism may be attributed to rhTPO's promotion of Plt production, which increases Plt aggregation at sites of inflammation, thereby worsening pulmonary microcirculatory dysfunction. In contrast, in septic patients with non-pulmonary infections, the impact of rhTPO on the pulmonary circulation may be minimal, with a correspondingly limited effect on gas exchange function, potentially leading to a lower risk of increased mortality. Therefore, when using rhTPO treatment, careful evaluation of the patient's infection etiology and pulmonary condition is necessary to balance its potential benefits and risks, so as to avoid an increase in mortality due to treatment-related complications.
This study observed that the serum levels of TLR4, IL-6, SCr, and TNF-α substantially decreased in both treatment groups. Furthermore, the post-treatment serum levels of the inflammatory factors TLR4, IL-6, and TNF-α were markedly lower in Group R versus Group C. These findings indicate that the treatment in Group R was effective in alleviating the inflammatory cascade reaction caused by sepsis, suggesting its relatively superior therapeutic effect. The occurrence of sepsis can potentially lead to organ bleeding or coagulation abnormalities. The reduction in inflammatory markers may be attributed to the immunomodulatory effects of rhTPO, which potentially aid in mitigating inflammatory responses and thereby improving overall patient condition. Inflammation can suppress Plt production and function, whereas the use of rhTPO may partially reverse this suppression, assisting in restoring normal Plt generation. 28 In this study, it was found that both treatment groups exhibited a significant decrease in coagulation indicators, including PT, APTT, FIB levels, and APACHE II scores after treatment. However, the observed differences between the two groups were negligible, suggesting that septic patients are capable of internally regulating coagulation parameters. This implies that despite sepsis, patients retain a certain degree of self-regulation ability, maintaining a balance in coagulation function to some extent. This self-regulation capability may be associated with overall patient health status, immune system response, and the effectiveness of treatment measures. 29
The results showed that patients receiving rhTPO treatment had significantly lower ICU and overall hospital mortality rates compared to those in Group C who did not receive rhTPO, indicating that rhTPO plays a crucial role in reducing mortality in patients with sepsis-associated thrombocytopenia. During the treatment period, neither group experienced complications such as MI, DVT, IS, or PE, suggesting that the use of rhTPO is safe and reliable. Univariate analysis revealed that age, SOFA score, APACHE II score, shock, DIC, Plt count, lactate levels, mechanical ventilation before ICU admission, blood dialysis before ICU admission, and receipt of rhTPO treatment were closely associated with patient mortality. Among these factors, age and disease severity scores reflect the patient's baseline condition and the severity of the disease, which have a significant impact on prognosis. The occurrence of shock and DIC further exacerbated the condition and increased the risk of death. The decrease in Plt count was closely associated with higher mortality, which may be related to coagulopathy and microcirculatory dysfunction in septic patients. Elevated lactate levels reflect insufficient tissue perfusion and metabolic disturbances, and serve as indicators of poor prognosis. Multivariate logistic regression analysis further confirmed that rhTPO treatment is an independent protective factor for reducing mortality. rhTPO may improve patient prognosis through multiple mechanisms: on the one hand, by promoting Plt production, increasing Plt count, improving coagulation function, and reducing the risk of bleeding; on the other hand, it may have a role in modulating immune and inflammatory responses, thus reducing the incidence of systemic inflammatory response syndrome (SIRS). Additionally, the use of rhTPO may improve organ function and reduce the occurrence of complications. The results of this study suggest that early application of rhTPO in the treatment of sepsis-associated thrombocytopenia has significant clinical implications. By increasing Plt levels, improving coagulation function, and modulating the inflammatory response, rhTPO helps to reduce patient mortality. However, this study also has some limitations, such as a relatively small sample size, lack of stratified analysis for different degrees of sepsis, and the need for further research to determine the optimal dose and treatment duration of rhTPO.
Conclusion
This study demonstrated that rhTPO treatment can significantly improve coagulation function and inflammatory status, increase Plt count, reduce blood transfusion requirements, and lower mortality in patients with sepsis-associated thrombocytopenia, showing promising clinical applicability. However, due to the relatively small sample size, lack of long-term follow-up data, and the absence of in-depth analysis of patients with varying degrees of severity, this study has certain limitations. Future research should involve multi-center, large-scale studies with extended follow-up periods to further explore the mechanisms of action of rhTPO and determine the optimal treatment regimen, thereby validating its efficacy and providing more effective treatment strategies for sepsis patients.
Footnotes
Author Contribution
HW, DC and MH contributed to the design of the study and data collection, performed the data analysis and wrote the manuscript. All authors read and approve the manuscript version final.
Consent for Publication
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The study was approved by the local ethics committee of the First People's Hospital of Linping. All experiments were performed in accordance with relevant guidelines and regulations such as the Declaration of Helsinki and the patients signed the informed consent form and agreed to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.