
Abstract
To limit complications and optimize anticoagulant therapy, some units treating venous thrombo embolism offer a formalized educational program to patients. In our clinic we developed a patient questionnaire to target aspects of patient knowledge about their venous thromboembolism (VTE) disease and their treatment that require reinforcement. The VTE questionnaire, composed of 7 questions, has been proposed to adult patients with a diagnosis of deep venous thrombosis or pulmonary embolism requiring anticoagulant therapy for at least 3 months. Patients who completed the VTE questionnaire between March 2022 and February 2023 were included in the present retrospective study. A poor score was defined as < 5 correct answers. We investigated the factors associated with a poor score on the questionnaire, using univariable and multivariable analysis, in order to better target patients education in our unit. A total of 132 patients were included. The majority were men (56.8%) and the mean (±SD) age was 55.4 (±18.3) years. The total score was < 5 in 43.2% of patients. Those with a poor score most frequently lacked knowledge regarding the treatment; only 22.8% of patients knew of the risk of bleeding, 5.3% the contraindication of non steroidal anti inflammatory drugs NSAIDs, and 19.3% knew of the precautions related to physical activity. In multivariate analysis the only factor associated with poor VTE questionnaire score was age ≥ 55 years (OR 2.61, 95%CI 1.14–5.94). Poor knowledge of venous thrombo embolism concerned older patients and particularly treatment-related aspects.
Introduction
Venous thromboembolism (VTE), comprising deep venous thrombosis (DVT) and pulmonary embolism (PE), is a common disease with significant morbi-mortality.1–3 Current guidelines from the European Society of Cardiology recommend anticoagulant treatment for ≥3 months, or indefinitely for unprovoked proximal DVT or PE. 4 However, anticoagulation is associated with potential side effects, including the risk of major bleeding 5 but also the risk of recurrent VTE that is mostly due to poor adherence.6,7 Despite these risks, it has been reported that > 75% of VTE patients indicated that they did not receive information on the risks related to anticoagulants, long-term complications of VTE, or the prevention of VTE recurrence, 8 but also that patients identify poorly potential anticoagulant-related emergencies. 9 It has also been reported that knowledge on VTE and anticoagulation was suboptimal 10 ; the authors used the Jessa AF Knowledge Questionnaire modified for VTE patients. Other studies have also used questionnaires to evaluate knowledge of VTE, but, to our knowledge, was aimed at patients under thromboprophylaxis without personal VTE history.11,12
To limit complications and optimize anticoagulant therapy, some VTE units offer a formalized educational program to patients receiving anticoagulation.6,7,13 Educational programs may be hard to set up due to lack of time of caregivers and cost, but also in a context of reduced length of hospital stay for VTE that, for certain patients, is managed in an ambulatory setting. Moreover, contradictory results have been reported regarding the effectiveness of current educational programs on adherence, and patient outcomes in terms of mortality, thromboembolic events and bleeding. 14
In our hospital there is no formal educational program after VTE, and initial oral information provided to patients may differ, in particular as the initial management of VTE is delivered at several different sites. We therefore developed a patient questionnaire that serves to direct a discussion with the vascular physician to ascertain the level of patient knowledge regarding VTE and its treatment during follow-up visits in our VTE clinic in order to then target aspects that require reinforcement. Herein, we report the baseline patient knowledge and the factors associated with poor knowledge in order to identify areas that could be improved at the time of diagnosis or initial management.
Materials and Methods
Study Area
The VTE questionnaire in our VTE clinic (part of the vascular medicine department of the Edouard Herriot university hospital, Lyon, France) has been proposed since March 2022 to adult patients with a diagnosis of DVT or PE requiring anticoagulant therapy for at least 3 months.
Definitions
The diagnosis of PE is based on computed tomography (CT) scan. Lower limb DVT is diagnosed using ultrasonography (US) and categorized as proximal or isolated distal DVT. We also distributed the questionnaire to patients with an unusual site of deep vein thrombosis (upper limbs, ovarian vein, and splanchnic vein) diagnosed using CT scan or US; the questionnaire is not distributed to patients with cognitive disorders or to those unable to complete it. The questionnaire is distributed at patient admission to the department before consultation.
Study Period
Patients who completed the VTE questionnaire between March 2022 and February 2023 were included in the present retrospective study. For those who completed >1 questionnaire, only the first was considered.
VTE Questionnaire
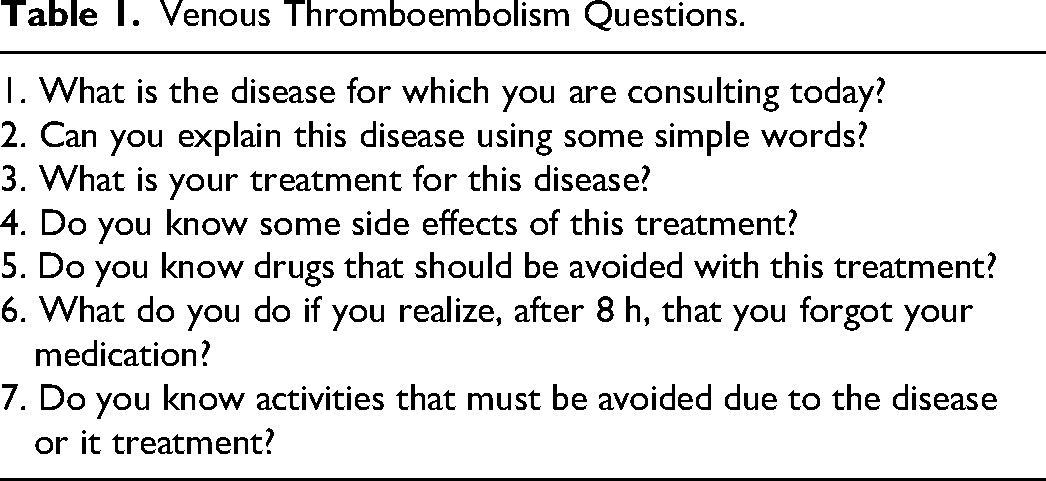
The VTE questionnaire comprises 7 questions focused on patient knowledge of VTE and anticoagulation (Table 1). During consultation, physicians evaluated answers to each question as correct or incorrect, using written replies (on the questionnaire) but also through discussion with the patient. Expected answers were adapted to each patient medical history (PE or DVT for example) and anticoagulant treatment. For the first question, physicians expected PE and/or DVT. For the second question, physicians expected that patients mentioned clot in the vessels. For the third question, anticoagulant treatment or the name of the medication were considered as sufficient. The side effect of the treatment expected in the fourth question was bleeding. Other drugs avoided with this treatment expected in the fifth question was Non-Steroidal Anti Inflammatory Drugs (NSAIDs). For the sixth question, patients were asked to describe their behavior if they realized after 8 h that they had forgotten to take their medication, and the expected answer was, according to the anticoagulant, either to take immediately their medication (for example this was the case for rivaroxaban and VKA) or to wait for the next planned intake (for example in the case of apixaban). For the seventh question relating to activities to avoid, the expected answer was combat sport or other activities with high bleeding risk. We selected the closest cut off to the median score; a good score was defined as 5/7 correct answers, and a poor score was defined as < 5 correct answers. The last question related to functional status and was based on the post-VTE Functional Status scale [12].
Venous Thromboembolism Questions.
Study Variables
Patient baseline characteristics (age, sex, weight and height, tobacco use, active cancer, and other treatments; polymedication was defined as at least 3 other medications in addition to an anticoagulant) as well as data regarding VTE were collected from medical files. The index VTE was the VTE event leading to the first consultation in our VTE clinic, even if the patient had previous VTE event. Data regarding VTE history (recurrence, number of previous VTE episodes) and index VTE were collected. Data collected regarding the index VTE were: PE severity, DVT localization, and for both PE and DVT the association with transient major risk factor according to guideline definition [4], as well as hospital admission and duration of hospital stay, and VTE symptoms. Clinical VTE symptoms were dyspnea, chest pain, hemoptysis, syncope, pain at the site of DVT, edema at the site of VTE, as was the absence of symptoms (asymptomatic). In addition, the current anticoagulant therapy and bleeding history since the initiation of anticoagulation therapy for index VTE were collected. Bleeding was classified as major or non-major according to the International Society on Thrombosis and Hemostasis (ISTH) definition; major bleeding was defined as any fatal bleeding or bleeding that causes a decrease of hemoglobin level in blood dropped to 2 g/dL or which required a transfusion of packed blood cells of at least two units, or any hemorrhage into any major anatomical sites whether intracranial, peritoneal, pericardial etc. Those that did not satisfy criteria for major bleeding were considered as non-major bleeding [13].
Ethical Considerations
The study was approved by the institutional review board of the Hospices Civils de Lyon (number 23_5081); patient consent was not mandatory due to retrospective nature of the study.
Statistics
The primary endpoint was having a poor VTE questionnaire score. Descriptive variables are reported as means ± standard deviation (SD). Differences in mean values between groups were assessed using the Student t test analysis of variance (or Mann Whitney test for non-normal distribution). Categorical variables were compared using the Chi-squared test. Univariate analyses were performed to screen for factors associated with a poor VTE questionnaire score. The predefined potential confounding factors tested were: characteristics of patients (age ≥ 55 years, sex, body mass index [BMI] ≥ 30 kg/m2), polymedication, tobacco use, active cancer, type of index VTE (PE [irrespective of DVT status], isolated DVT, recurrent VTE, association with a major risk factor for VTE, hospitalization), current anticoagulation by direct oral anticoagulants (DOACs), bleeding history since anticoagulant treatment, and post-VTE Functional Status scale score. Variables with a p value <0.15 were entered into the final multivariate regression analysis which provided odds ratios (OR) and corresponding 95% confidence intervals 95% CI). In multivariate analysis, variables were selected on the following basis: (1) p-value <0.15 in univariate analysis, (2) prevalence >3%, (3) clinical relevance, and (4) <2% of missing data. Factors with a p value <0.05 in the multivariate analysis were considered as independent confounding factors. All reported p-values are 2-sided, and a p-value < 0.05 was considered to be significant. Statistical analyses were performed using IMB® SPSS® Statistics version 21 (SPSS Inc., Chicago, IL, United States).
Results
A total of 132 patients were included in the present study. The majority were men (56.8%), the mean (±SD) age was 55.4 (±18.3) years, and the mean BMI was 28.4 (±7.3) kg/m2. Nearly a third of patients were polymedicated (31.1%), 10.6% were active smokers, and 13.7% had concomitant active cancer (Table 2).
Patient Characteristics.
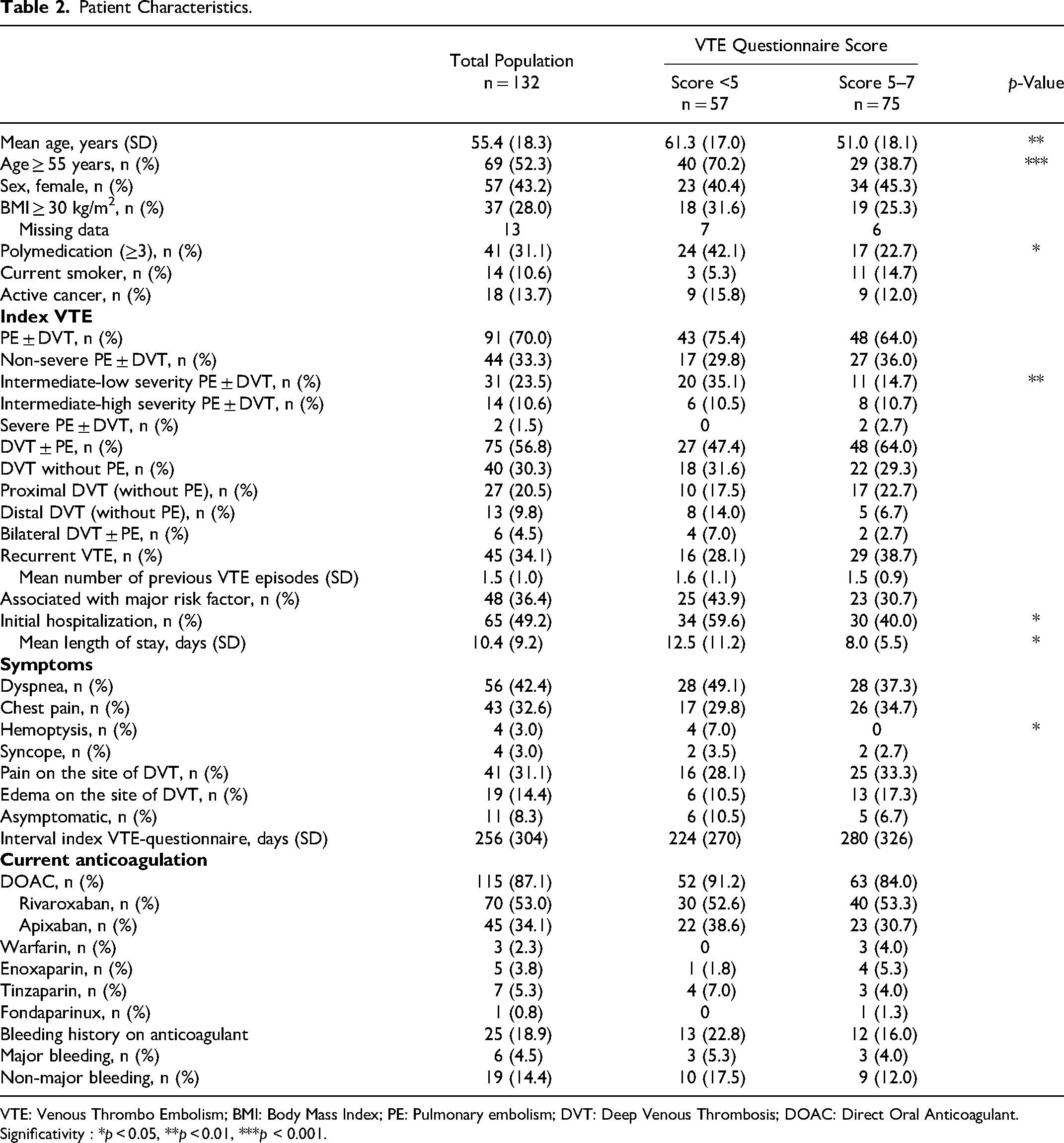
VTE: Venous Thrombo Embolism; BMI: Body Mass Index; PE: Pulmonary embolism; DVT: Deep Venous Thrombosis; DOAC: Direct Oral Anticoagulant. Significativity : *p < 0.05, **p < 0.01, ***p < 0.001.
For nearly three-quarters of patients the index VTE was PE (irrespective of DVT status; 70%). A third of patients had recurrent VTE (34.1%), and for a third of patients the VTE was associated with a major risk factor (36.4%). Half of the patients were hospitalized (49.2%). Symptoms were dyspnea for 42.4%, chest pain for 32.6%, hemoptysis for 3.0%, syncope for 3.0%, pain on the site of DVT for 31.1%, edema on the site of DVT for 14.4%; 8.3% where asymptomatic. At the time of the visit at the VTE clinic, 87.1% patients were on anticoagulant therapy with DOACs. Bleeding history during anticoagulation was reported in 18.9% patients (4.5% major bleeding and 14.4% non-major bleeding; Table 2).
Most of the patients knew that they had a VTE (95.5%), could explain their disease (80.3%) and knew that they had an anticoagulant treatment for their disease (96.2%). Just over half of the patients were aware of bleeding risk associated with their treatment (56.8%), what to do if they forgot to take their medication (54.5%), and the activities to avoid (51.5%); under a third knew that NSAIDs are contraindicated in association with their treatment (29.5%). The total score was between 5 and 7 for 56.8% of patients, and <5 (poor score) for 43.2% (Table 3). A total of 123 patients answered the question relating to post-VTE functional status; functional limitations reported were absent for 44.7% (n = 55), negligible for 26.8% (n = 33), slight for 14.6% (n = 18), moderate for 9.8% (n = 12) and severe for 4.1% (n = 5).
Patient Answers.
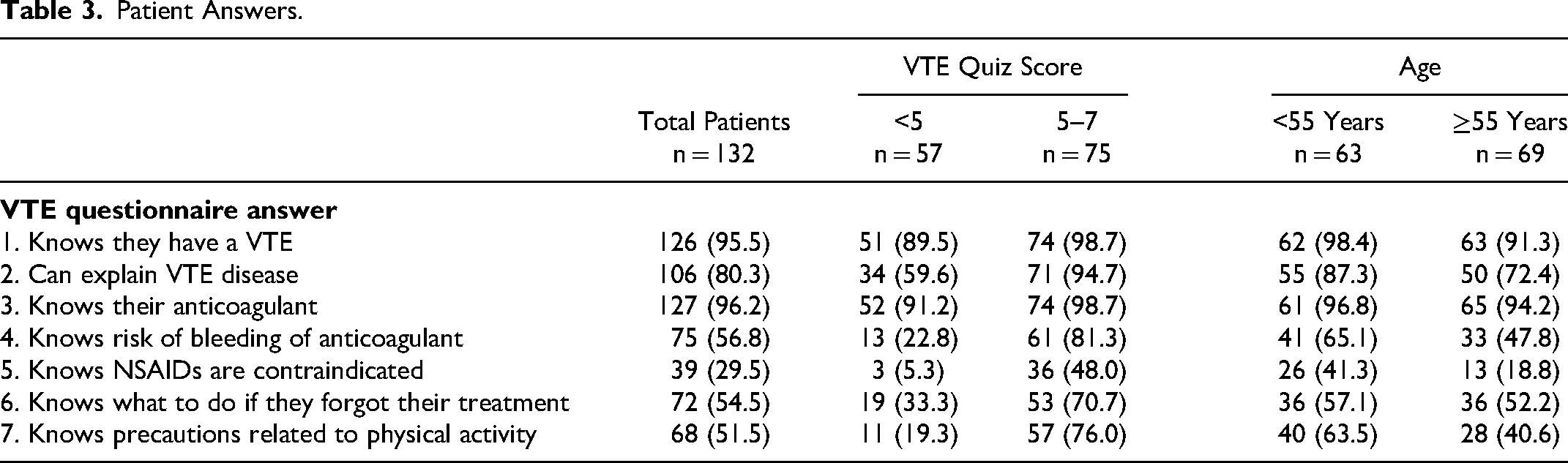
Patients with a poor score most frequently lacked knowledge regarding the treatment; only 22.8% of patients knew of the risk of bleeding, 5.3% the contraindication for NSAID, 33.3% knew what to do if they forgot their treatment, and 19.3% knew of the precautions related to physical activity. Conversely, 89.5% of them knew that they had a VTE, 59.6% could explain their VTE, and 91.2% knew that they took an anticoagulant for VTE (Table 3).
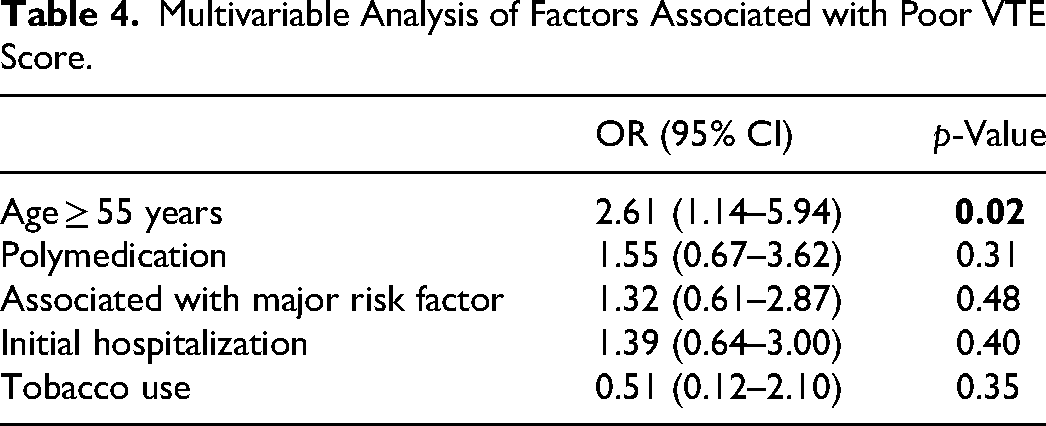
Patients with poor VTE questionnaire score were significantly older (mean ± SD, 61.3 ± 17.0 years) than patients with good score (51.0 ± 18.1 years, p = 0.001). In addition, patients with poor score had significantly more frequently polymedication (42.1%) compared to those with good score (22.7%, p = 0.02) and were more frequently hospitalized (59.6%) compared to those with good score (40.0%, p = 0.03). There was a trend towards less frequent current smokers in those with a poor score (5.3%) than those with a good score (p = 0.09), and more frequent association between the index VTE and a major risk factor (43.9% vs 30.7%, respectively; p = 0.14). In multivariate analysis, the only factor significantly associated with poor VTE questionnaire score was age ≥ 55 years (OR 2.61, 95%CI 1.14–5.94; Table 4).
Multivariable Analysis of Factors Associated with Poor VTE Score.
Patients aged ≥ 55 years most infrequently correctly answered the question regarding contraindication of NSAIDs (18.8%); other questions with a frequent incorrect answer were precautions related to physical activity (40.6%), risk of bleeding (47.8%), and what to do if they forgo their treatment (52.2%).
Discussion
The present study found that age ≥ 55 years was an independent risk factor for poor knowledge of VTE. It is also of note that the severity of index VTE, initial symptoms, ambulatory setting, recurrent VTE, choice of anticoagulant, and bleeding history during anticoagulant treatment were not associated with poor medical knowledge.
The question to which most patients answered incorrectly was the contraindication for NSAID, and this seems to be an important aspect to address. For example, questioning patients on their habits, it has been reported that almost a quarter of patients treated by VKA were exposed to NSAIDs 15 and that 9% of patients receiving apixaban did so. 16 It would therefore be of interest to reinforce the information regarding this contraindication at the moment of prescription and also delivery.
Herein the only factor independently associated with poor knowledge was age ≥ 55 years. Previously, Obamiro et al developed a questionnaire to evaluate patient knowledge (the Oral Anticoagulation Knowledge Tool) and did not find any influence of patient age on disease knowledge and awareness; however, the mean (± SD) age of those included was 74 ± 12 years which may explain this. 17 In addition, Fang et al compared patients taking warfarin according to health literacy level (ie the degree to which individuals can obtain, process, and understand the information and services necessary to make appropriate decisions involving their health); those with limited health literacy where significantly older [mean age: 63.3 years, 95%CI (61.0–65.6)] compared to those with adequate health literacy [53.8 years (50.4–57.1), p < 0.001]. 18 Taken together this underlines that patients with poorer knowledge are relatively young compared to life expectancy in developed countries, 19 but this has been reported in other contexts notably diabetes mellitus where older age (> 60 years old) was found to be associated with inadequate level of knowledge.20,21 In the present study patients aged ≥ 55 years were more frequently initially hospitalized, and we therefore propose to target this period to deliver information to these patients; which is all the more important as older patients are exposed to a greater risk of complications including bleeding due to their age. 22
We found no influence of index VTE severity, index VTE clinical symptoms, bleeding history during anticoagulant treatment or VTE functional status on patient knowledge. This was surprising as it would seem likely that these aspects would increase the perception of patients to VTE-related risk and that this could influence their knowledge of VTE and its treatment, as found in diabetes prevention where patients who had been informed of their risk had significantly higher perceived risk scores and significantly higher knowledge scores. 23 It is also of note that ambulatory setting is the new gold standard for the management of non-severe PE and DVT 4 and we did not find this to be associated with patient knowledge level although we feared that this would be negatively affected owing to the limited time for the delivery of information. Moreover, as did Tran et al, 24 we found no influence of anticoagulant choice of patient knowledge.
The present study has several limitations, notably owing to its retrospective design. For example, the education level of included patients was not available although this has been reported to influence medical knowledge,
25
but among the variables collected there was missing data only for BMI and this concerned relatively few patients and equally those with a poor and good score. In addition, the level of knowledge was ascertained by both the questionnaire and during the subsequent interview but the latter was conducted at the discretion of the vascular physician which could have introduced heterogeneity and subjectivity in the scoring system, and thus influence the final results. Only 7 questions were chosen to determine the knowledge about VTE, however this questionnaire had to be quick and easy to be filled out in the waiting room and to not prolong the time of consultation
Conclusions
Poor knowledge of VTE concerned older patients and particularly treatment-related aspects. At follow up consultation, practitioners should re-inform all patients whatever the history of their VTE with more emphasis for those over 55 years old. In our clinic, we continue to inform patients using this questionnaire at each consultation and expect an improvement of patient knowledge.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this case was obtained from by the institutional review board of the Hospices Civils de Lyon (number 23_5081); patient consent was not mandatory due to retrospective nature of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.