
Abstract
Anticoagulation management using warfarin is challenging in clinical practice. This study aimed to evaluate the knowledge, adherence, and satisfaction with warfarin therapy and associated factors among outpatients at the Tikur Anbessa Specialized Hospital (TASH) in Addis Ababa, Ethiopia. An interview-based cross-sectional study was conducted among 350 patients receiving warfarin therapy at cardiac and hematology clinics of TASH. Anticoagulation knowledge assessment (AKA) questionnaires assessed the patients’ warfarin knowledge. Adherence to warfarin was evaluated using the Morisky Green Levine Scale (MGLS), and patient satisfaction with warfarin therapy was assessed using the 17-item anticlot treatment scale (ACTS). Binary logistic regression was used to determine factors associated with the outcome variables, and p < .05 was used as the cut-off point to declare a significant association. The mean AKA score was 59.35 ± 13.04% (10.68 ± 2.34 correct answers), and 82 (23.4%) of participants achieved a passing score. Based on the MGLS, 192 (54.9%) study participants adhered well to warfarin. The mean level of satisfaction was 53.67 ± 8.56, with mean scores of 41.93 ± 7.80 and 11.74 ± 2.43 in the ACTS burden and benefit subscales, respectively. One hundred eighty-four (52.6%) patients were satisfied with warfarin therapy. The absence of hyperthyroidism was significantly associated with poor knowledge of warfarin therapy (adjusted odds ratio [AOR] = 4.28, 95% confidence interval [CI]: 1.01–18.22). Those living with family had a 56% lower chance of poor warfarin adherence (AOR: 0.44; 95% CI: 0.21–0.93) than those living alone. This study shows room for improvement in patient knowledge, adherence, and satisfaction with warfarin therapy.
Introduction
Warfarin is the most commonly prescribed anticoagulant for preventing and treating thrombosis. 1 However, anticoagulation management is notoriously challenging in clinical practice because of the vast number of factors that influence international normalized ratio (INR) control, including its narrow therapeutic window,2,3 many drug and food interactions, 4 miscommunication about dosing between the patient and physician, poor patient knowledge,5,6 adherence, 7 and satisfaction 8 regarding anticoagulation treatment. Knowledge of warfarin, its potential side effects, interacting medicines and foods, and the need for warfarin adherence play a role in attaining the desired therapeutic outcome while preventing adverse reactions. 9 However, minimal patient knowledge about warfarin therapy was seen elsewhere, including only 13.9% of patients receiving a passing score in Ethiopia, 10 a mean score of 59.39% in Hungarian patients, 11 only 14.9% of Saudi Arabian patients with adequate knowledge 12 and 50% of the patients with a poor knowledge score on oral anticoagulation therapy in Indian study. 12
Medication adherence is integral to patient care to achieve optimized anticoagulation control and outcomes. Poor adherence to warfarin therapy has a significant effect on anticoagulation control and is one of the most common barriers to obtaining favorable anticoagulation outcomes. 13 Previous studies have shown that patients’ adherence to warfarin therapy is suboptimal, that is, in the range of 27.5%–54.9%.5,12,14 Several factors, including poor health literacy, lack of patient education, complex dosing regimens, clinical characteristics, knowledge of warfarin, low income, marital status, living arrangements, and drug regimens, play significant roles in warfarin nonadherence.15,16
The burden of anticoagulation treatment affects patient satisfaction. 8 Patient satisfaction is critical for treatment adherence, clinical outcomes, and healthcare utilization. 17 The characteristics of warfarin, including regular blood testing, lifestyle limitations, and fear of bleeding, may result in reduced patient satisfaction. 12 Few studies have documented a moderate level of patient satisfaction with oral anticoagulation therapy and its impact on anticoagulation control in patients taking warfarin.17–19 Improving patient satisfaction with opioid agonist therapy can result in better clinical outcomes and reduce the risk of adverse events such as bleeding and thrombosis. 20 Despite the importance of warfarin therapy and the known factors influencing patients’ knowledge, adherence, and satisfaction, studies in the Ethiopian context are lacking. This study addressed this gap by evaluating patients’ knowledge, adherence, and satisfaction with warfarin therapy, and identifying the determinants of these outcomes in Ethiopia.
Methods
Study Setting
This study was conducted at the Tikur Anbessa Specialized Hospital (TASH) and included patients receiving warfarin therapy at cardiac and hematology clinics (CHCs). The clinics are staffed with cardiologists, hematologists, cardiac and hematology fellows, resident physicians, nurses, and support members, and each clinic functions 4.5 days per week.
Study Design and Period
An interview-based cross-sectional study was conducted between March 1 and June 30, 2023, among patients on warfarin to evaluate their knowledge of, adherence to, and satisfaction with anticoagulation treatment. We also collected the clinical data of the study participants from the electronic medical records (iCare system).
Source and Study Population
The source population was outpatients with follow-up at the CHCs of the TASH, whereas the study population included all patients who received anticoagulation management services (AMS) in the same hospital, had been receiving warfarin therapy, and fulfilled the inclusion criteria.
Eligibility Criteria
We enrolled patients aged ≥18 years who had been taking warfarin for at least 6 months. However, we excluded patients who were unwilling to participate, unable to complete the questionnaire in Amharic, critically ill, or had mental health issues, and those with missing or incomplete medical and medication data.
Sample Size Determination and Sampling Technique
This study included all eligible patients who visited and received AMS during the data-collection period. Accordingly, we interviewed 397 study participants, and 350 were included in the final analysis after excluding responses with incomplete or missing information. For better representativeness, we attempted to enroll a proportional number of participants per week, based on the expected study population in that week, until the end of the data-collection period.
Data Collection Instrument, Procedures, and Outcomes Measurement
The data collection instrument was structured into 4 sections. Section I gathered the study participants’ sociodemographic and socioeconomic characteristics, while Section II consisted of anticoagulation knowledge assessment (AKA) questionnaires. The AKA questionnaire was developed based on validated questionnaires from previous studies to assess patients’ knowledge of warfarin.11,12,21,22 Eighteen multiple-choice questions were administered, and the patients were asked to choose 1 answer from the available choices for all questions. Scoring was conducted using a dichotomous scale, with correct responses as 1 and “incorrect” and “do not know” responses as 0. The cumulative scores were presented as a percentage of correct answers, and adequate knowledge regarding AKA ranged from 70% to 75%.22–24 In our study, at least 13 questions answered correctly (72.22%) were considered passing scores. Section III evaluates patient adherence to warfarin using the Morisky Green Levine Scale (MGLS). 25 It included 4 questions with yes/no response options, with total scores ranging from 0 to 4—3 levels of medication adherence. The MGLS resulted in 3 levels of medication adherence based on these scores: high, medium, and low adherence, with 0, 1–2, and 3–4 points, respectively. The measurement was scored bivariate (0 = no, 1 = yes) to assess adherence to anticoagulation treatment. A dichotomous definition of adherence based on the MGLS is also commonly used, with 0 point indicating perfect adherence and 1+ points indicating some level of nonadherence. Potential reasons for nonadherence were also assessed in a cohort of participants who reported <100% adherence in the past 4 weeks. As the MGLS has been validated for the broadest range of diseases, including patients with low literacy, it is the most widely used scale in research. The last section addressed patient satisfaction with warfarin therapy using an anticlot treatment scale (ACTS). It is a robustly validated, patient-reported instrument for measuring treatment satisfaction with anticoagulants. It comprises 17 items across 2 subscales (burdens and benefits). Thirteen items assessed the burden of anticoagulant treatment (12-item burden scale and 1 global question on treatment burden), and 4 items assessed the benefits of anticoagulant treatment (3-item benefits scale and 1 global question on treatment benefits). Study participants were asked to rate their experiences of anticoagulant treatment during the past 4 weeks on a 5-point scale of intensity (1=not at all, 2 = a little, 3 = moderately, 4 = quite a bit, and 5 = extremely). Reverse coding was used to calculate the burden scale, with higher scores indicating higher satisfaction. The ACTS burdens total score ranges from 12 to 60, and the ACTS benefits total score ranges from 3 to 15, with a total score ranging from 15 to 75 scores. 26 Patients were considered satisfied with the anticlot treatment if they scored above the mean score for all patients and dissatisfied if their score was below this cut-off point. 27 Data related to the patients’ clinical and medication records were collected from the patients’ electronic records (iCare system).
Data Collectors and Quality Assurance
Two pharmacists and 2 nurses collected the data. They were selected based on their educational level, clinical and research experience, and possible familiarity with serving patients who have received warfarin therapy in one way or another. The questionnaires for the exit interviews were prepared in English, translated into Amharic, and translated again into English to maintain consistency and facilitate better understanding. The Amharic version was used to interview patients. The instruments were reviewed and approved by a team of senior clinical pharmacists, cardiologists, and hematologists for their content, flow, completeness, and clarity to be used by data collectors and their suitability for extracting the required information before using them for data collection. The AKA, MGLS, and ACTS have been validated and widely used to evaluate the knowledge, adherence, and satisfaction of patients on oral anticoagulants. We pretested the data collection tool before data collection to ensure its quality, clarity, and feasibility of use, after which amendments were made to its structure. A 1-day training session was given to the data collectors on how to use data collection instruments, explaining the study purpose to participants, approaching and obtaining verbal consent, implementing sampling techniques, and conducting interviews to collect and maintain data confidentiality. The quality of collected data was ensured by reviewing and checking for completeness.
Data Analysis
Data were analyzed using the Statistical Package for Social Science version 27. Percentages and frequencies, mean (±standard deviation), and median (interquartile range) were used to summarize the descriptive data. Logistic regression was used to identify the determinants of knowledge, adherence, and satisfaction among the patients taking warfarin. Variables with p < .25 from the bivariable analysis were candidates for multivariable analysis to adjust for confounding effects. Odds ratios () (ORs) at 95% confidence intervals (CIs) were used to determine the association between the independent and dependent variables. In multivariable analysis, p < .05 was used to declare the significance of the association.
Ethical Considerations
Ethical clearance was granted by the School of Pharmacy Ethical Review Committee (ERB/SOP/454/15/2022), and subsequently by the Institutional Review Board of the College of Health Sciences, Addis Ababa University (096/22/SoP). Written informed consent was obtained from all participants after they were provided with information about the purpose of the study, why and how they were selected to be involved in the study, and what was expected from them. To maintain confidentiality, the research team avoided using personal identifiers and analyzed the data in the aggregate. The research team handled the data obtained from the study participants with the utmost confidentiality.
Results
Sociodemographic Characteristics of Study Participants
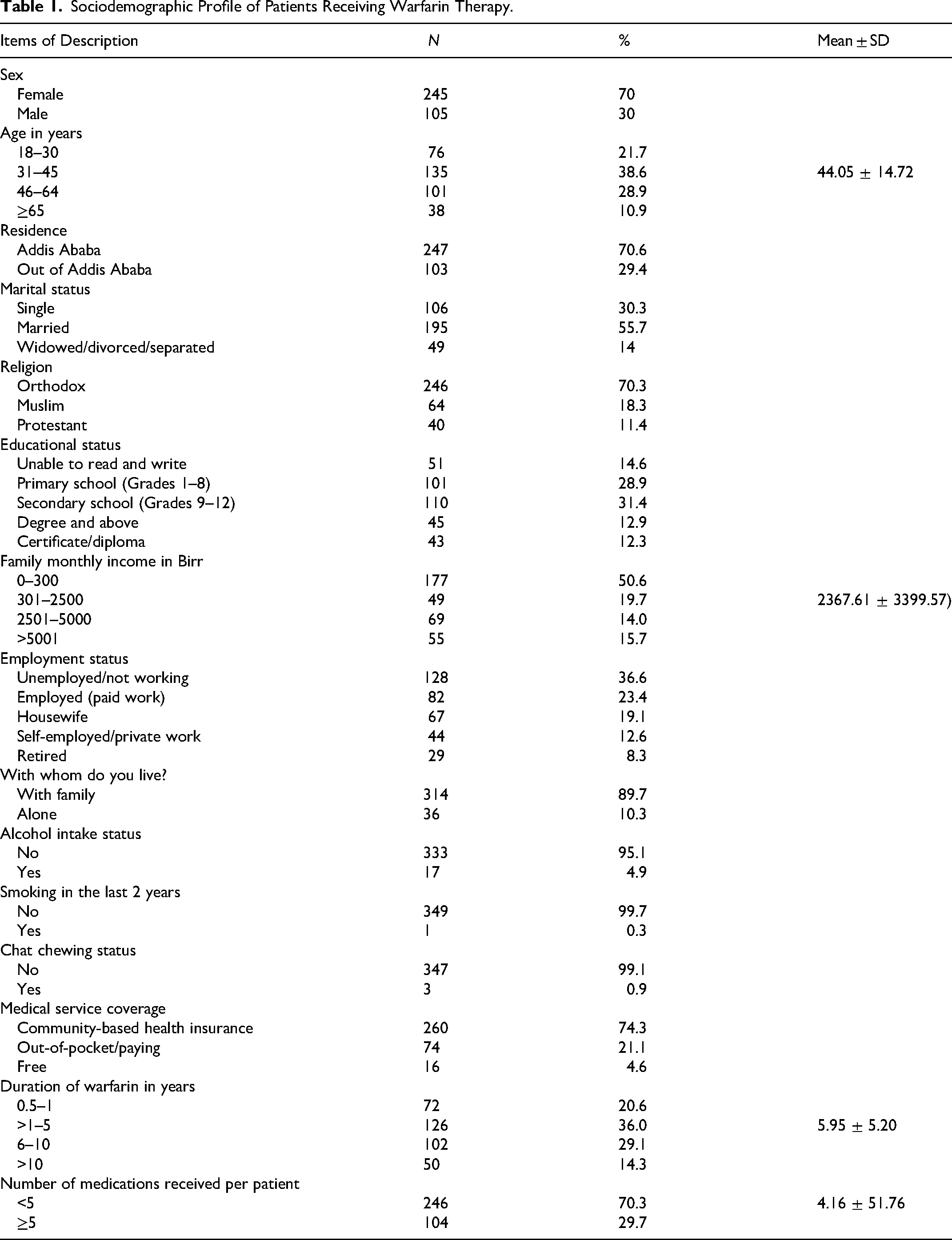
Three hundred fifty patients receiving warfarin participated in the present study, among whom 245 (70%) were female, and the mean age was 44.05 (±14.72, range = 18–82) years. Most participants (55.7%) were married, and 70% resided in Addis Ababa. Most participants (70.0%) were Orthodox Christians, half (50.6%) had low monthly incomes (0–300 birr), and one-third (33.7%) of participants were unemployed. Most participants (89.7%) lived with their families, and 75% used community-based health insurance. The mean duration of warfarin therapy was 5.95 years (±5.20 years) (range = 0.5–29.5 years), and participants received an average of 4.16 drugs (±1.76) (range = 1–13). Moreover, 29.7% of participants reported polypharmacy (Table 1).
Sociodemographic Profile of Patients Receiving Warfarin Therapy.
Clinical Characteristics of Patients Receiving Warfarin
Most of the participants (76.4%) had at least 1 comorbidity that did not require warfarin, most of whom had heart failure (45.4%), valvular heart disease (41.4%), and hypertension (24%). History of stroke and vascular diseases were recorded in 18.9% and 11.1% of patients, respectively. The most common indication for warfarin was atrial fibrillation (60%), followed by valvular heart disease with left atrial/venous thrombus (13.1%), post mechanical heart valves (mitral and/or aortic valves) (12.6%), and recurrent and/or unprovoked deep vein thrombosis (10.6%). During the follow-up, 89 bleeding episodes and 64 all-cause emergency visits were recorded. The details are presented in Supplemental File 1.
Knowledge of Warfarin Therapy
The mean AKA questionnaire score was 59.35 ± 13.04% (10.68 ± 2.34 correct answers). None of the patients scored 0 or 100%, and 16.7% scored below 50%. The minimum and maximum scores were 11.1% and 83.3%, respectively. All patients correctly answered questions regarding risky activities while taking warfarin. Seven of the questions were answered correctly by at least 70% of the patients (71.7%–100%) (Table 2). Questions “on the effect of high intake alcohol in a single evening” and “how to eat green leafy vegetables while on warfarin” were answered correctly only by 6.9% and 9.4% of respondents, respectively. Similarly, frequently incorrect questions covered knowledge of the INR target range, decisions on advice regarding the consumption of herbal supplements, conditions/actions that may have a significant effect on warfarin work, INR value above the target range, and warfarin drug interaction, as 42.3%–76.3% of patients did not select correct responses.
Study Participants’ Knowledge of Warfarin Therapy Based on AKA Questionnaire.
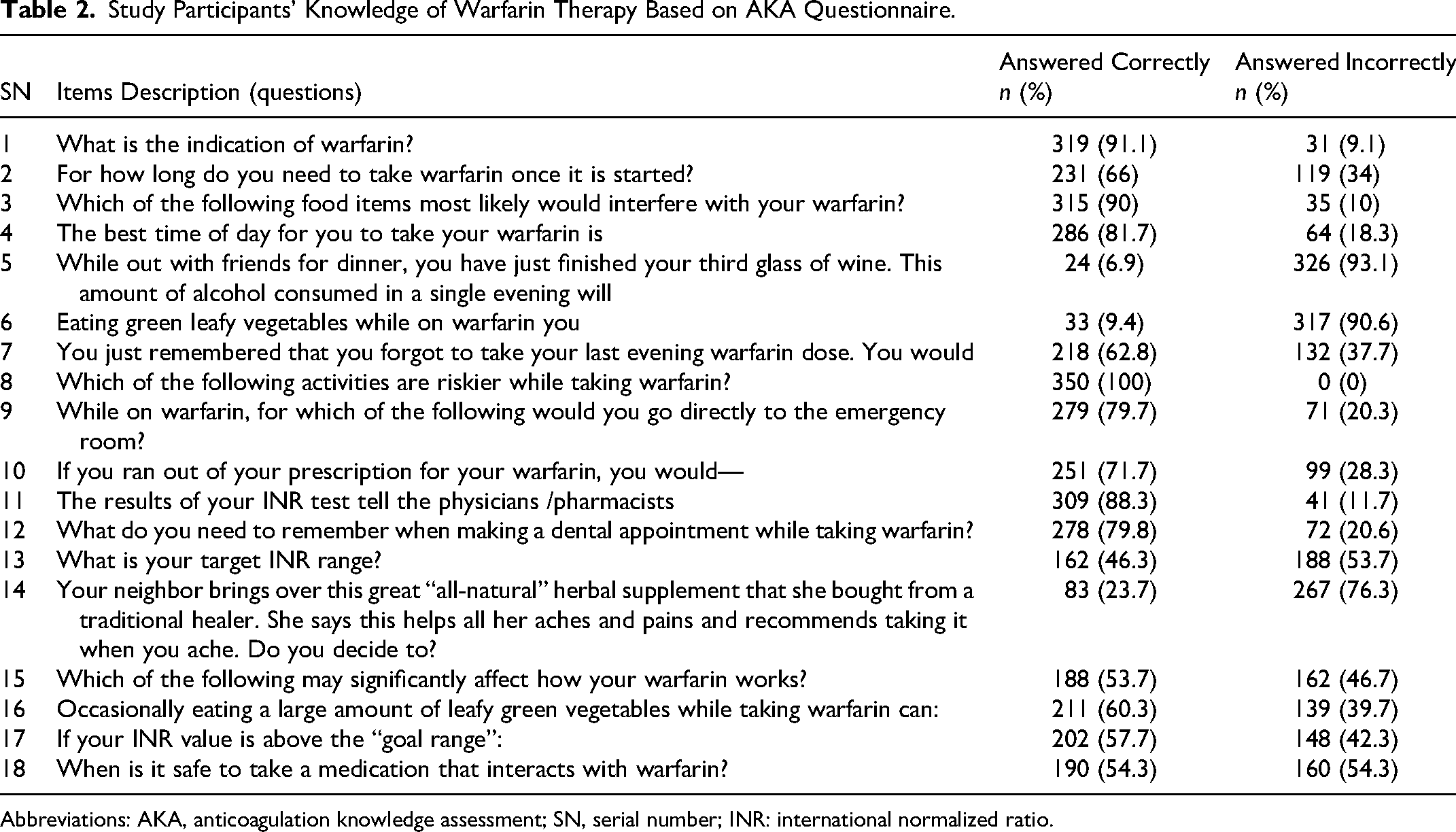
Abbreviations: AKA, anticoagulation knowledge assessment; SN, serial number; INR: international normalized ratio.
Of the 350 patients who participated in the study, 82 (23.4%) achieved a passing score and they answered at least 13 questions correctly (Figure 1).
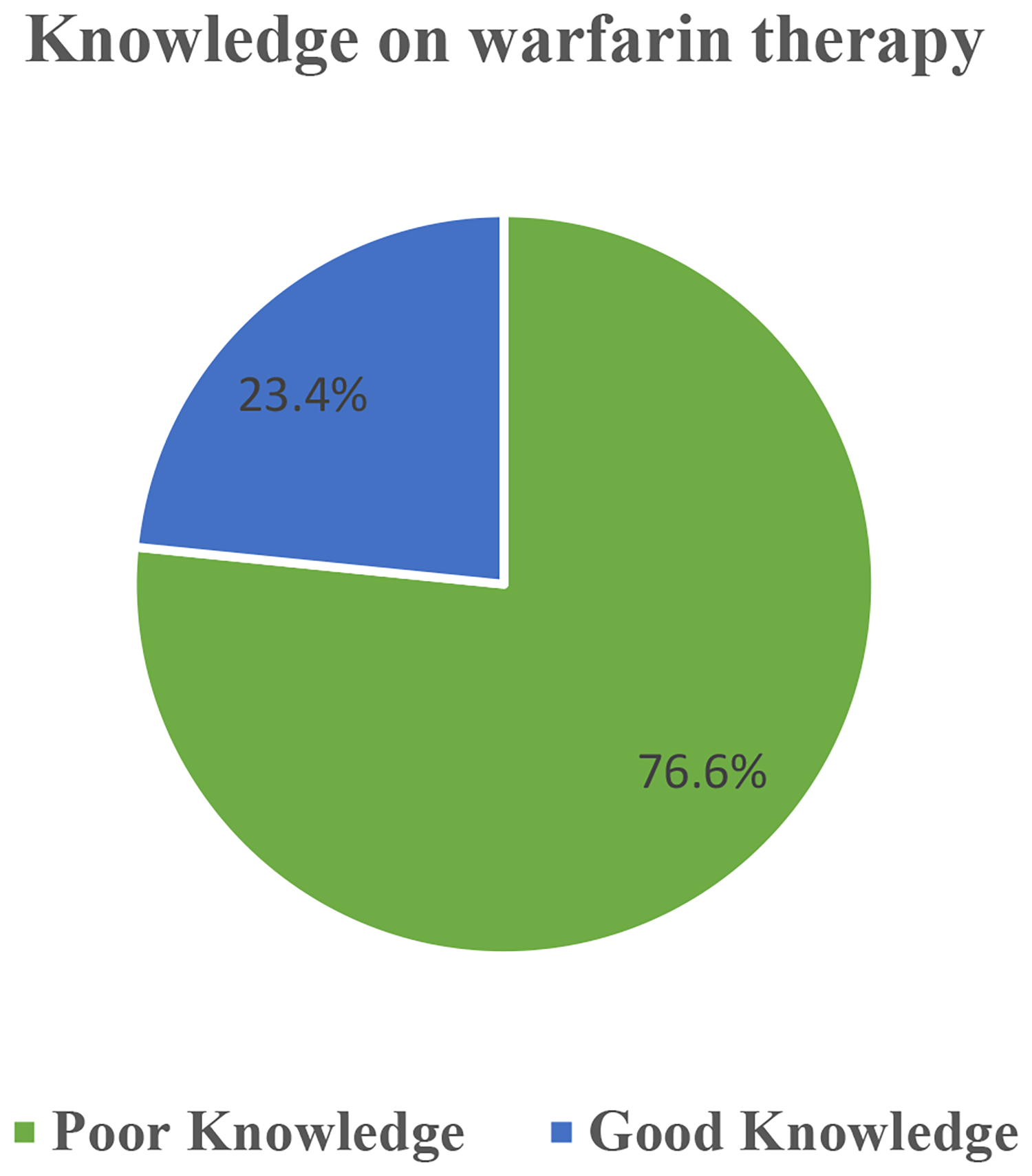
Study participants’ knowledge of warfarin based on the anticoagulation knowledge assessment (AKA) questionnaire.
Adherence to Warfarin
Based on the MGLS, approximately one-third (34.3%) of the participants indicated that they had forgotten to take warfarin during the past 4 weeks (Table 3).
Adherence to Warfarin among Patients Attending CHCs of TASH (N = 350).
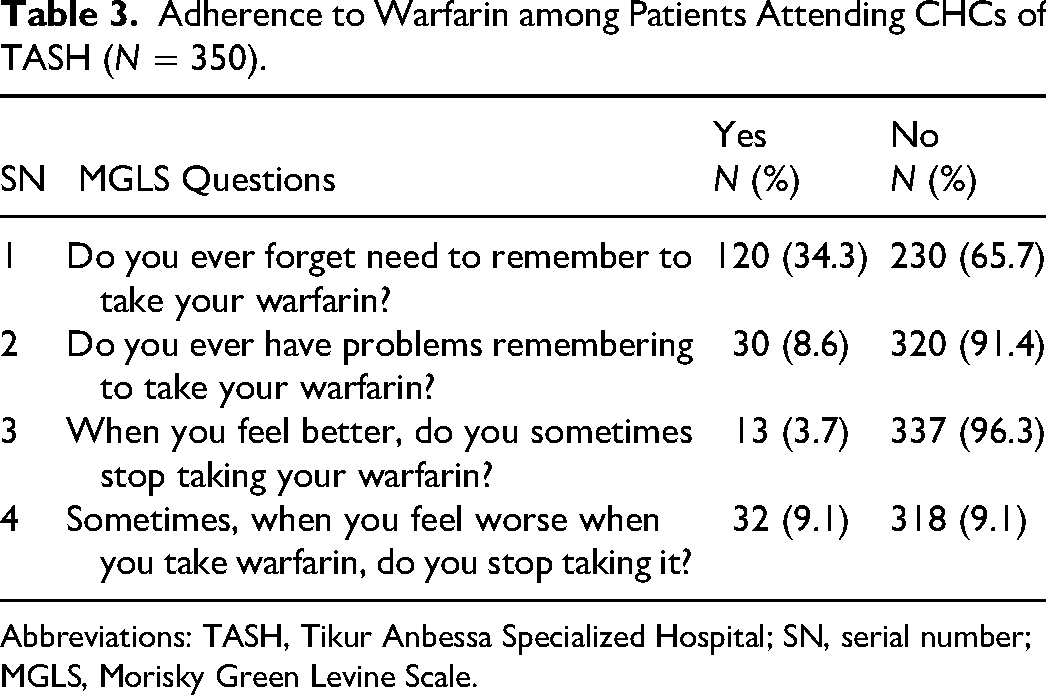
Abbreviations: TASH, Tikur Anbessa Specialized Hospital; SN, serial number; MGLS, Morisky Green Levine Scale.
In this study, 54.9% of the participants adhered well to their warfarin (Figure 2).
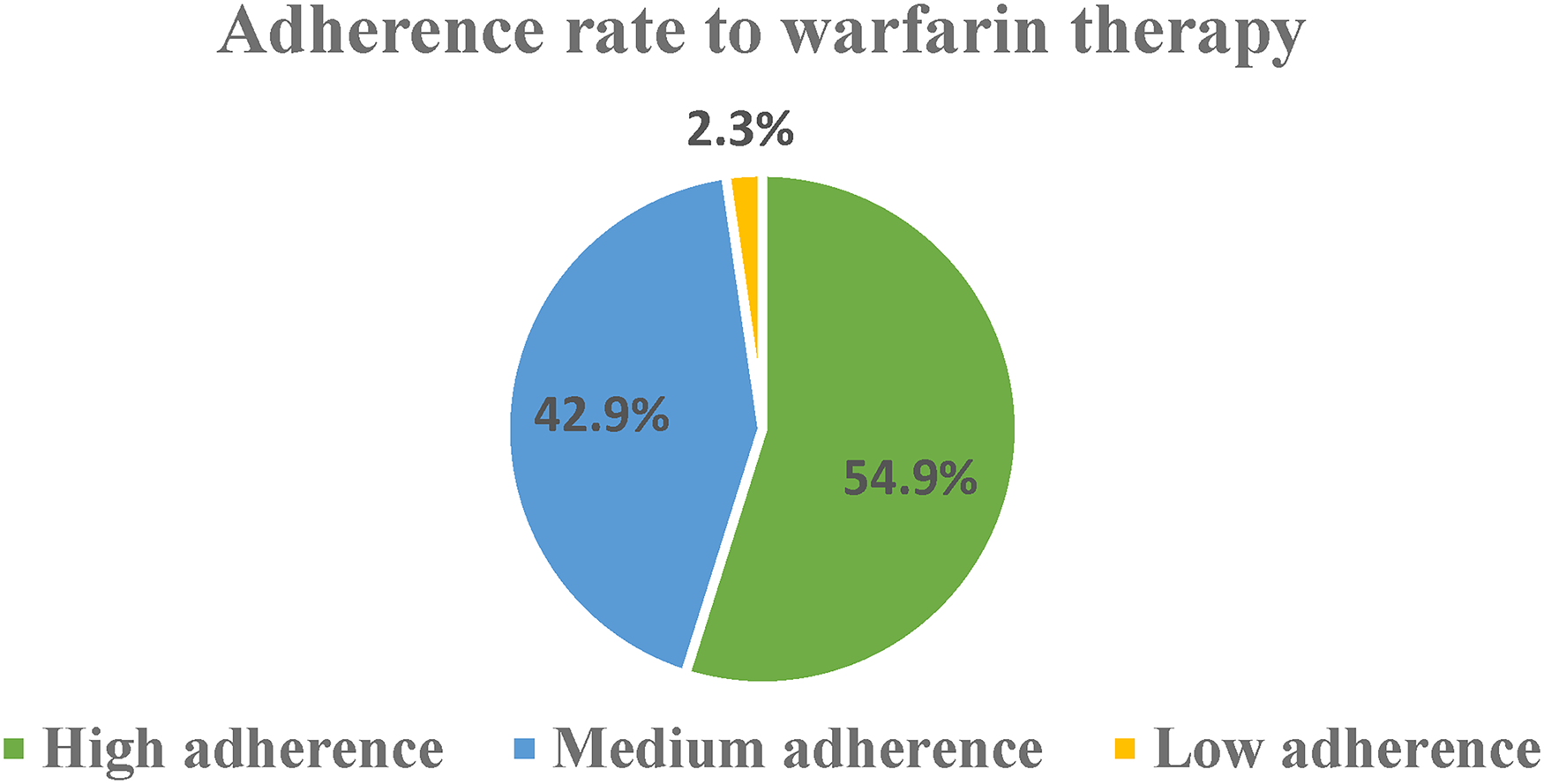
Adherence to warfarin using the Morisky Green Levine Scale (MGLS) among patients receiving warfarin.
Reasons for Nonadherence to Warfarin
Among the cohort participants who reported <100% adherence in the past 4 weeks, self-reported reasons for medication nonadherence were asked, and 11 potential reasons for nonadherence were identified. Forgetfulness (67.7%) was the most self-reported reason, followed by fear of warfarin side effects and workload/being busy, as both were reported by 15.2% of nonadherent study participants (Figure 3).
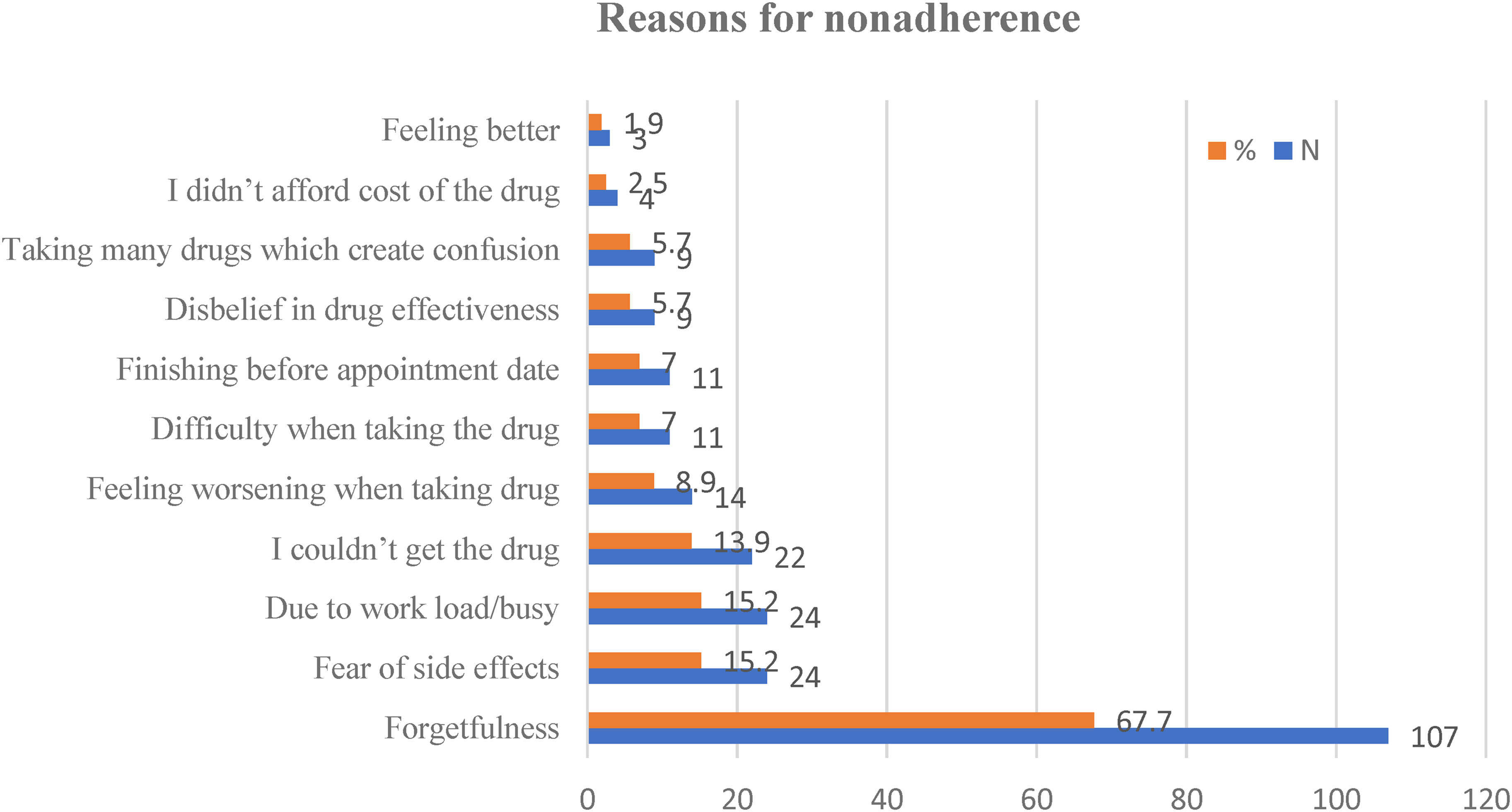
Reasons for nonadherence to warfarin.
Satisfaction With Warfarin Treatment
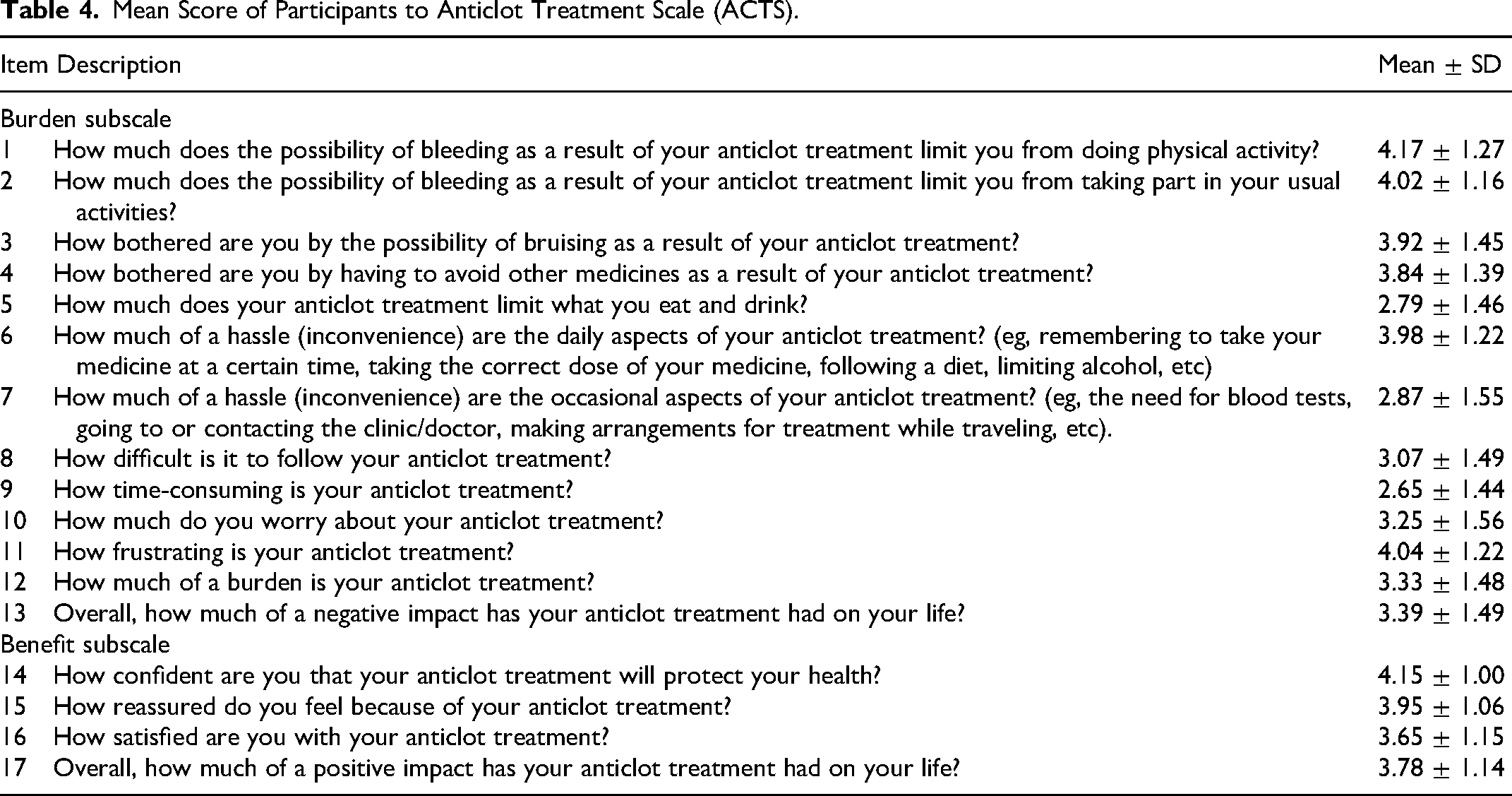
The mean level of satisfaction was 53.67 ± 8.56, with mean scores of 41.93 ± 7.80 and 11.74 ± 2.43 in the ACTS burden and benefit subscales, respectively. In this study, 184 (52.6) patients were satisfied with warfarin therapy and the remaining 47.4% were unsatisfied. The highest mean satisfaction scores 4.17 ± 1.27 and 4.15 ± 1.00 were reported on the “effect of possible anticlot treatment-related bleeding on doing physical activity” and “confidence level with anticlot treatment in its benefit” in burden and benefit subscales, respectively. In another way, the “impact of warfarin therapy on food and drinking limitations” and “satisfaction with anticlot treatment” were subscales with the lowest mean satisfaction scores (Table 4).
Mean Score of Participants to Anticlot Treatment Scale (ACTS).
Factors Associated With Warfarin Therapy Knowledge
Twelve variables (Table 5) were evaluated to identify their association with study participants’ knowledge of warfarin therapy. In the univariate binary logistic regression analysis, HIV/AIDS and hyperthyroidism were significantly associated with poor knowledge of warfarin therapy. However, patients without hyperthyroidism were 4.28 times (adjusted OR [AOR] = 4.28, 95% CI: 1.01–18.22, p = .049) more likely to have poor knowledge of warfarin than those with hyperthyroidism (Table 5).
Factors Associated With Knowledge of Warfarin Therapy.
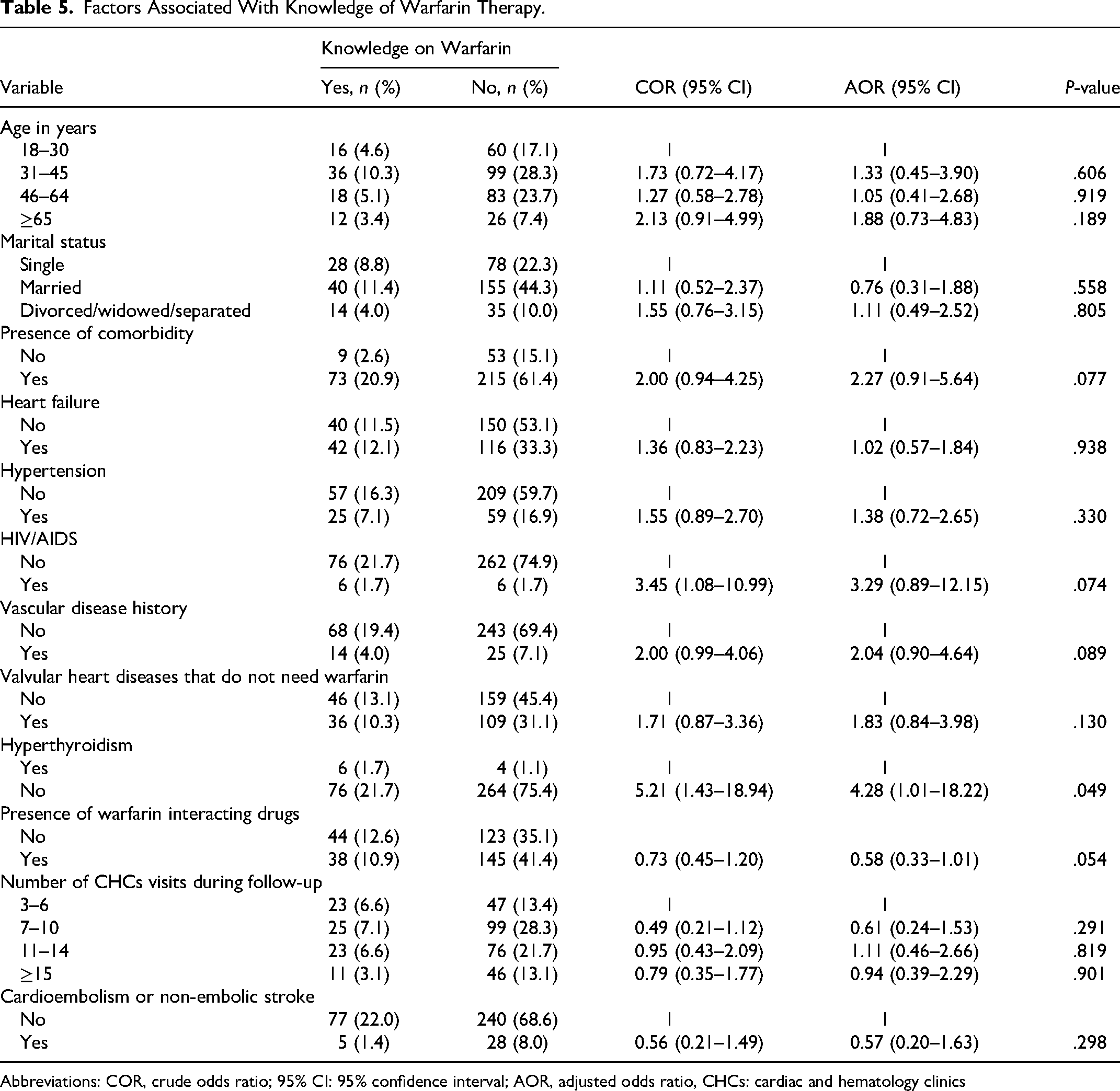
Abbreviations: COR, crude odds ratio; 95% CI: 95% confidence interval; AOR, adjusted odds ratio, CHCs: cardiac and hematology clinics
Associated Factors With Adherence to Warfarin
In the multivariate logistic regression analysis, living alone and visiting CHCs 15 or more times demonstrated a statistically significant association with adherence to warfarin therapy. The odds of poor adherence to warfarin were reduced by 56% among patients living with family (AOR: 0.44; 95% CI: 0.21–0.93; p = .032) compared to those living alone (Table 6).
Factors Associated With Adherence to Warfarin Therapy.
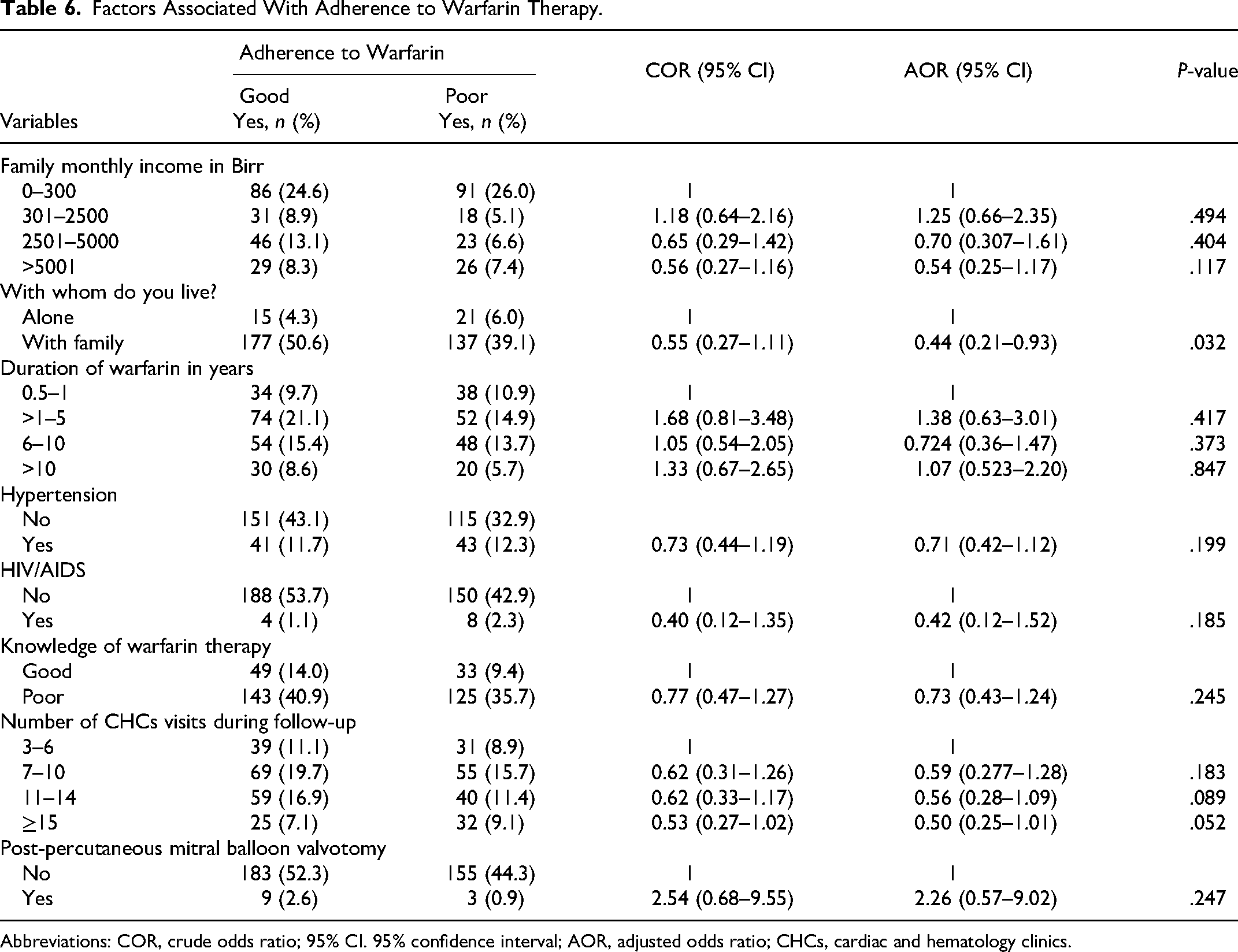
Abbreviations: COR, crude odds ratio; 95% CI. 95% confidence interval; AOR, adjusted odds ratio; CHCs, cardiac and hematology clinics.
Factors Associated With Satisfaction With Anticoagulation Treatment
Eleven variables were assessed to identify their association with patient satisfaction with anticoagulation treatment, using univariate binary logistic regression analysis. Multivariate logistic regression revealed that living alone, older age, better educational status, living outside Addis Ababa, portal vein thrombosis, warfarin indication, and bleeding history were all associated with being more likely to be dissatisfied with warfarin therapy. However, none of these factors was significantly associated with the current study's satisfaction with anticoagulant treatment (Table 7).
Factors Associated With Satisfaction With Anticoagulation Treatment in Patients Receiving Warfarin.
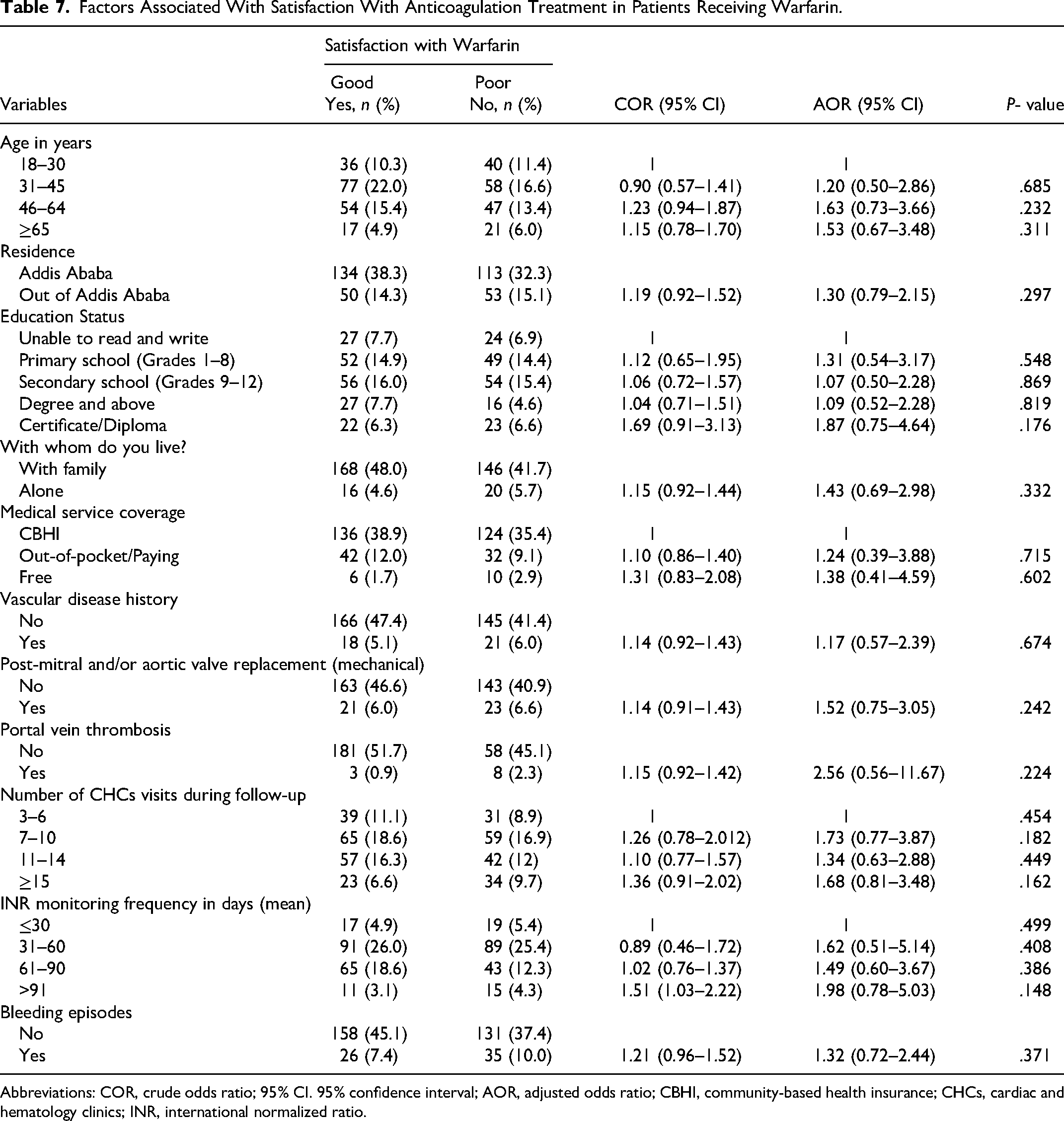
Abbreviations: COR, crude odds ratio; 95% CI. 95% confidence interval; AOR, adjusted odds ratio; CBHI, community-based health insurance; CHCs, cardiac and hematology clinics; INR, international normalized ratio.
Discussion
This is the first study in Ethiopia to evaluate patients’ knowledge, adherence, and satisfaction regarding warfarin therapy. The participants in this study comprised a diverse group of patients with various comorbidities and different warfarin indications for long-term care to prevent thrombosis. The patient population was relatively younger, with a mean age of 44.05 ± 7.9 years, which may have resulted from a higher prevalence of rheumatic heart disease in our study and Ethiopia. 28
The mean knowledge of warfarin therapy (59.35 ± 13.04%) obtained in the present study was comparable with the Hungarian study 59.39 (±17.62) 11 and a systematic review and meta-analysis report of 60.4% average level of knowledge on warfarin therapy 29 and slightly lower than that found by Hua et al 30 in China (62.3 ± 8.8%). However, the mean score in our study was much higher than that reported by Nader and co-workers, 31 with an overall mean score of 29.3%. In the present study, 23.4% of patients achieved an AKA passing score (good knowledge of warfarin therapy), higher than previous studies that reported passing scores between 5.8% and 15.8%.6,9,32 Nevertheless, 75.2% of patients had good knowledge of warfarin (scoring ≥ 75%) in a study carried out at the King Khalid University Hospital outpatient anticoagulant clinic in Riyadh, Saudi Arabia. 33 The lower knowledge level among our study participants might be due to a lack of proper understanding among the patients or inadequate counseling provided by the treating physicians.
In this study, 7 frequently incorrect answers (Table 2) were potential areas for improvement in patient education on warfarin therapy, and more broadly show that long-term warfarin users require continuing education and sustained beneficial communication between healthcare providers for successful anticoagulation management. To address this, healthcare providers, including pharmacists, should strengthen their role in providing patient education and counseling by designing educational programs to improve the clinical outcomes of those on warfarin therapy. We did not find a significant association between any sociodemographic characteristic and knowledge of warfarin therapy. However, in studies conducted elsewhere, age, educational status, living alone or with family, and duration of warfarin therapy were significantly associated with knowledge of warfarin therapy.24,31,34,35
Adherence to warfarin therapy is beneficial in clinical practice, as it can help identify patients who require closer monitoring and educational interventions to improve treatment outcomes. 36 In the present study, ∼55% of patients reported adherence to warfarin, which was higher than in prior studies, with 5.4% and 37.6% adherence rates in Sudan and Vietnam, respectively.27,32 However, our findings contradict a Turkish study that found a higher adherence rate (79.8%). 37 This suggests that there is room for improvement in patient adherence to warfarin to shape positive attitudes among pharmacists. A significant association was only observed between living with family (AOR = 0.44, 95% CI: 0.21–0.93, p = .03) and poor warfarin adherence (negative association) in the multivariate regression analysis, which contradicts with other previous studies, 38 while other sociodemographic and clinical characteristics did not show a significant association.
Similarly, our study did not find a significant association between knowledge of warfarin (AOR = 0.73, 95% CI: 0.43–123, p = .245) and adherence, contrary to previous reports.32,38 In the current study, forgetting, fear of side effects, workload, and not receiving warfarin on time were the most common self-reported reasons among nonadherent cohorts. Improving warfarin adherence is crucial for effective anticoagulation therapy and for reducing the risk of thromboembolic events. 7 Hence, strategies that include memory refreshment to avoid forgetfulness, tailored education and provision of written format recommendations and reminders, pharmacist consultation between clinic visits focused on explaining misconceptions and encouraging adherence, telephone counseling, and open discussions with the patient to minimize doubts or fears have the potential to significantly improve warfarin adherence7,39 . Structured education focused on warfarin can have a favorable impact on patients’ attitudes toward medication, leading to an improvement in their quality of life. Patients are more inclined to adhere to the warfarin regimen by acknowledging the negative experiences associated with the drug as manageable. 38
The overall mean level of satisfaction with warfarin therapy (53.67 ± 8.56) in the present study was lower than that reported in a previous study. 12 Our study found that 52.6% of patients were satisfied with the anticlot treatment, which is similar to the satisfaction level reported in Sudanese patients (50.5%), 27 but lower than the Saudi Arabian study's report (63.7%). 12 Regarding ACTS subscale scores, the mean ACTS burden score was lower than that reported in studies conducted in Canada, Japan, and Saudi Arabia17,40,41 among patients receiving warfarin therapy. Conversely, a higher ACTS benefit score was reported in our study when compared with the same studies, but was consistent with the Saudi study (11.74 ± 2.43 vs 11.92 ± 2.4). The differences in the degree, mean level of satisfaction, and ACTS subscale scores in the present study may be explained by the differences in the patients’ demographic characteristics (sex, age, and education level), quality of anticoagulation management service, sample size, and indications for warfarin. Multiple regression analysis revealed no significant association between independent variables and ACTS scores. Participants who lived outside Addis Ababa, lived alone, had postmitral and/or aortic valve replacement (mechanical) and portal vein thrombosis warfarin indication and bleeding history, and had an extended INR monitoring frequency were more likely to be unsatisfied with anticlot treatment when compared with their counterparts, without significant difference in satisfaction level (Table 7). However, significant associations with anticlot treatment satisfaction have been identified in previous studies.8,12,27,40
Strengths and Limitations of the Study
The present study had a relatively large sample size. This is also the first study in Ethiopia to assess the 3 essential aspects of oral anticoagulation. Hence, this study provides unique insights into patient knowledge, adherence, and satisfaction with anticlot treatment in our study population, which have not been previously reported, and our findings can inform the development of targeted interventions to improve warfarin therapy. Despite these strengths, this study has several limitations. The first is its cross-sectional design, which made it difficult to establish a relationship between cause and effect. Second, this single-center study recruited participants from outpatient CHCs; therefore, the results cannot be generalized to a large patient population receiving warfarin. Third, this study relied on self-reported data collected from patients, who may be prone to response and recall bias. Participants may have provided socially desirable answers or inaccurately represented their behavior in the medication adherence and satisfaction questionnaires.
Conclusions
This study highlights the importance of understanding the knowledge, adherence, and satisfaction with anticoagulation treatment of patients receiving warfarin at TASH, Ethiopia. About a quarter of the patients passed the AKA questionnaire. More than half of the study participants adhered well to warfarin, and forgetting, fear of side effects, and workload/being busy were the most frequent reasons for nonadherence. Approximately half of the patients were satisfied with the warfarin therapy. This study shows room for improvement in the knowledge, adherence, and satisfaction of patients taking warfarin. Future research should explore the impact of patient education and counseling on improving knowledge, adherence, and satisfaction with anticoagulation treatment among patients receiving warfarin.
Supplemental Material
sj-docx-1-cat-10.1177_10760296241260736 - Supplemental material for Knowledge, Adherence, and Satisfaction With Warfarin Therapy and Associated Factors Among Outpatients at University Teaching Hospital in Ethiopia
Supplemental material, sj-docx-1-cat-10.1177_10760296241260736 for Knowledge, Adherence, and Satisfaction With Warfarin Therapy and Associated Factors Among Outpatients at University Teaching Hospital in Ethiopia by Tamrat Assefa Tadesse, Dejuma Yadeta, Legese Chelkeba, Amha Gebremedhin and Teferi Gedif Fenta in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgments
The authors would like to thank all the study participants for their time and willingness to participate in this study. The first author would like to express his sincere gratitude to Dr. Suthesh Sivapalaratnam at the Precision Healthcare University Research Institute, Queen Mary University of London, for his mentorship in preparing this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported financially by Addis Ababa University Graduate Programs, CDT-Africa College of Health Science Addis Ababa University and the International Society of Thrombosis and Haemostasis Scientific and Standardization Committee (ISTH-SSC) Small Grant.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.