
Abstract
The pathogenesis of venous thromboembolism in multiple myeloma is still poorly understood because multiple factors are involved. In particular, the increase in whole blood viscosity has a key role and, therefore, we performed an evaluation of some hemorheological determinants in multiple myeloma patients, putting them in relation to the thrombotic risk, with the aim to evaluate if an alteration of the hemorheological pattern was associated with a higher thrombotic risk. We performed an observational retrospective cohort study with data collected from January 2017 to September 2022. In a group of 190 patients with newly diagnosed multiple myeloma, we have examined the trend of calculated blood viscosity according to the Merrill formula, and we stratified the patients for the thrombotic risk in accordance with the IMWG/NCCN guidelines and with IMPEDE VTE score. Using the thrombotic risk stratification proposed by IMWG/NCCN any variation in calculated blood viscosity is evident, while, with the IMPEDE VTE score, we observed an increase in calculated blood viscosity in patients with “intermediate + high” risk. The calculated blood viscosity is higher in subjects presenting an “intermediate + high” thrombotic risk according to the IMPEDE VTE score. This association could therefore lay the groundwork for further research with the aim to confirm the role of hemorheological pattern in MM-related thrombotic risk.
Keywords
Introduction
Multiple myeloma (MM) is a biologically heterogeneous disease, direct consequence of malignant transformation of post-germinal center plasma cells in a multi-step process,1,2 with an uncontrolled growth of pathological cells in the bone marrow (BM) and an overproduction of non-functional intact immunoglobulins or immunoglobulin chains. The accumulation of these immunoglobulins and the interaction of the aberrant monoclonal plasma cells with other BM cells lead to a specific clinical picture including anemia, fatigue, bone lesions and pain, infections, hypercalcemia, and renal failure.3,4 MM is the second most common hematologic malignancy with a median age at diagnosis of 65 years. The risk of developing MM is higher in older age groups, whereas it is a much more uncommon diagnosis for patients under the age of 45. 5 Despite the treatment advances, MM remains an incurable disease and the affected patients may have poor quality of life due to disease-related symptoms and adverse events from prior therapies or cumulative toxicity. Among these symptoms, venous thromboembolism (VTE) has emerged as one of the leading complications, because of an impairment of both anticoagulant and fibrinolytic pathways, with at least 10% of patients developing VTE during the disease.6‐12 The considerable impact of VTE on survival and quality of life in MM patients has made increasingly necessary the availability of a thrombotic risk stratification, to apply valid prophylaxis strategies. To date, the IMWG/NCCN guidelines provided a thromboembolic risk score, which, based on data relating to the patient's characteristics and the pathology itself, allow stratifying the patients into two groups, “standard risk” and “high risk,” with consequent different pharmacological indications in terms of antithrombotic prophylaxis.13‐15 In recent years, another thrombotic risk stratification model has been proposed in MM patients, the IMPEDE VTE score. This latter seems to outperform the current IMWG/NCCN guidelines, thus being able to be considered as the new standard risk stratification for VTE in MM.16‐18 The pathogenesis of VTE in MM patients is still poorly understood because multiple factors are involved, both patient-related (advanced age, immobility, concomitant infections, hormonal therapy, and a history of thrombosis), and disease-related (increased blood viscosity, infections, high levels of immunoglobulin, autoantibody directed against natural anticoagulants, the procoagulant activity of inflammatory mediators, and therapy-related etiologies, such as immunomodulatory agents –IMiDs– and steroids).19‐22 In particular, the increase in whole blood viscosity (WBV) may interfere with fibrin polymerization with an impairment of normal fibrinolysis. 23 Since the 1980s several authors have hypothesized24‐26 the role of WBV in thrombogenesis, considering indeed that the increase in WBV reduces the rate of flow in the venous district, and that cellular and plasma elements involved in the thrombogenic process (erythrocytes, platelets, fibrinogen) are the main responsible for blood viscosity in vivo. 27 The role of hemorheological pattern in MM is very important also in terms of deformability and aggregation of red blood cells.28‐30 Generally, the measurement of WBV is carried out ex vivo using different types of viscometers such as rotational, capillary, and oscillatory ones. However, WBV can also be estimated or calculated using specific formulas, from some simple laboratory parameters (such as hematocrit, total plasma proteins, and plasma levels of fibrinogen), overcoming the limits represented by the technical difficulties, as well as by the costs of use and maintenance of the instrumentation.31‐34 With Merrill's formula, the calculated whole blood viscosity (c-WBV), expressed as yield shear stress (YSS), is estimated using the hematocrit values and the plasma levels of fibrinogen. Instead, in the de Simone's study, the hematocrit and total plasma proteins are the used laboratory parameters, because they seem to predict more than 80% of the variability of the blood viscosity. All the used formulas for the indirect calculation of WBV do not consider neither the deformability nor the aggregation of red blood cells; however, the latter parameter could be indirectly calculated using the albumin/fibrinogen ratio as a surrogate.35,36 In addition, the reliability of the c-WBV is higher for specific reference ranges of the laboratory parameters considered, hardly respected in MM patients, especially due to the low hematocrit values at diagnosis and the high total protein. However, the possibility of using them also in the context of plasma cell dyscrasias was provided by the results of our recent clinical study in which, by comparing the subjects with both monoclonal gammopathy of undetermined significant (MGUS) and MM the measured and calculated blood viscosity data, it emerged that the c-WBV (both with de Simone's and Merrill's formulas) and the surrogate marker of erythrocyte aggregation, show a parallel trend with the corresponding hemorheological determinants obtained using their direct measurement. 37 Therefore, considering the importance of VTE in MM and the possible pathogenetic role of blood viscosity, we performed an analysis of some hemorheological determinants in a cohort of patients with a new diagnosis of MM, with the aim to evaluate their possible association with the thrombotic risk at diagnosis. The hemorheological pattern was evaluated in a calculated way using the Merrill formula for the c-WBV and the albumin/fibrinogen ratio for the erythrocyte aggregation.
Materials and Methods
Population
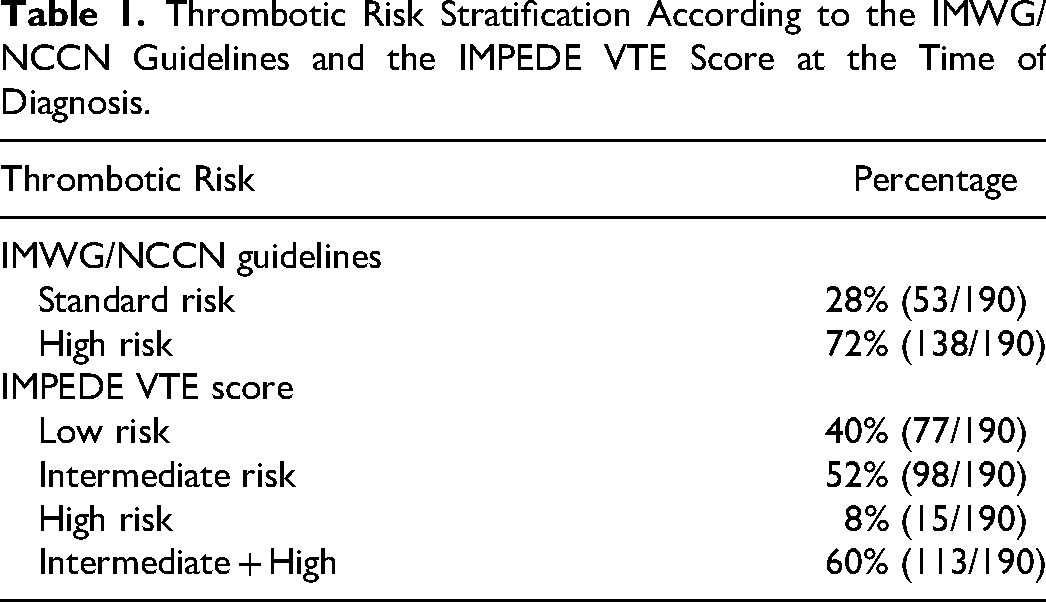
The population study is represented by 190 patients with a new diagnosis of MM, evaluated at the Hematology Division of the “Paolo Giaccone” University Hospital in Palermo from January 1, 2017, to September 30, 2022. At the time of diagnosis, regarding the thrombotic stratification of patients, we employed both the NCCN/IMWG guidelines and the IMPEDE VTE score (Table 1). The data were collected by consulting the medical records and the laboratory history of the company computer system. The Institutional Ethics Committee of the University approved this study Hospital of Palermo (report N° 01/2022). The research was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association's Declaration of Helsinki. Written informed consent was obtained from each participant/patient for study participation and data publication.
Thrombotic Risk Stratification According to the IMWG/NCCN Guidelines and the IMPEDE VTE Score at the Time of Diagnosis.
Methods
In this retrospective study, we evaluated the following parameters: hematocrit (Ht) obtained using an automated hematology analyzer, fibrinogen expressed in g/L and evaluated with the Clauss method, YSS calculated according to Merrill's formula [13.5 × 10−6 × Fib2 × (Ht-6)3], albumin (g/L), evaluated with the colorimetric method, and albumin (g/L)/fibrinogen (g/L) ratio. At the time of diagnosis, we also performed a thrombotic risk assessment according to the international guidelines of the IMWG/NCCN and to the IMPEDE VTE score.
Statistical Analysis
All statistical analysis was performed using GraphPAd Prism version 9.5. Data were expressed as medians and interquartile ranges. Regarding thrombotic risk stratification, carried out both according to the IMWG/NCCN guidelines and based on the IMPEDE VTE score, in the entire group of MM patients, as well as in the three subgroups identified in relation to the isotype, the comparison between the medians was carried out with the Mann-Whitney test. The null hypothesis was of P ≥ 0.1. About this P-value level, we know that the statistical significance is valid for values of P ≤ 0.05 but performing our analysis on a numerically inhomogeneous sample (27 patients with LCMM, 56 with IgA, and 107 with IgG MM), and considering different parameters, we have made this doctrinal forcing with the aim to consider also the tendential statistical significance of the analyzed parameters, especially in the evaluation of MM isotypes (LCMM, IgA, and IgG).
Results
Firstly, we evaluated the medians, interquartile ranges, and the range of all considered parameters in the entire cohort of MM patients (Table 2). Then, we performed an initial thrombotic risk stratification in accordance with the international IMWG/NCCN guidelines, comparing in the identified subgroups (standard and high risk) the behavior of all the considered hemorheological parameters (Table 3). Specifically, from this first evaluation, no statistically significant differences are observed in the calculated blood viscosity (expressed as YSS), total plasma protein, fibrinogen, and albumin. We also tried to examine whether this same trend was maintained in the different MM isotypes (LCMM, IgA, and IgG). In this regard, we observed that in LCMM patients (Table 4A) there is no difference between the considered parameters; nevertheless, in this isotype, it cannot be excluded that the limited number and distribution of cases influence the results (27 patients out of 190 of whom only 7 patients at standard thrombotic risk). In patients with IgA MM (Table 4B), the division into standard and high thrombotic risk does not seem to show any statistical difference, although in the high-risk subgroup, the value of the YSS shows a decrease. This datum is related to the fact that the tendential reduction of the hematocrit is not accompanied by an increase in plasma fibrinogen. In patients with IgG MM (Table 4C), representing 56% of the entire cohort examined, in the “high risk” subgroup we observed a significant reduction of the hematocrit, associated with a slight decrease in the YSS; no difference is appreciable for the remaining considered parameters. After the above analysis, a similar approach was carried out evaluating the thrombotic risk according to the IMPEDE VTE score. Considering the whole cohort of MM patients (Table 5), we observed that in the “intermediate + high risk“ subgroup the c-WBV and plasma fibrinogen are significant increased compared to the “low risk“ subgroup (respectively P = 0.02 and P = 0.07); no significant variation seems to concern the remain considered parameters. Instead, evaluating the trend of the c-WBV in the three different MM isotypes the following emerges in the LCMM (Table 6A) the division in the two subgroups does not show any variation and this could, once again, be related to the size of this group (only 5 of the 27 patients with LCMM fall into the “low risk” subgroup). Conversely, in the same MM isotype, a significant increase in albumin level is evident, not only in comparison of the whole cohort but also respect to the remain isotypes (data not shown). In the IgA MM (Table 6B) we observed a significant increase in YSS in the “intermediate + high risk” subgroup, in which is also present a tendential increase in hematocrit and plasma fibrinogen, and a reduction of the albumin/fibrinogen ratio, indirect marker of increased red blood cell aggregation. In the IgG MM (Table 6C) the stratification of thrombotic risk by IMPEDE VTE score shows in the subgroup “intermediate + high risk” an increase in YSS, which, however, does not reach statistical significance, unlike what happens instead in the whole cohort of MM patients and in IgA MM patients; none of the other parameters appears to diversify the two subgroups of this MM isotype. The same evaluations, when carried out using the de Simone formula for the calculation of blood viscosity, did not reveal any statistically significant information (data not shown).
Medians, IQRs, and Ranges of Hemorheological Determinants in MM Patients.
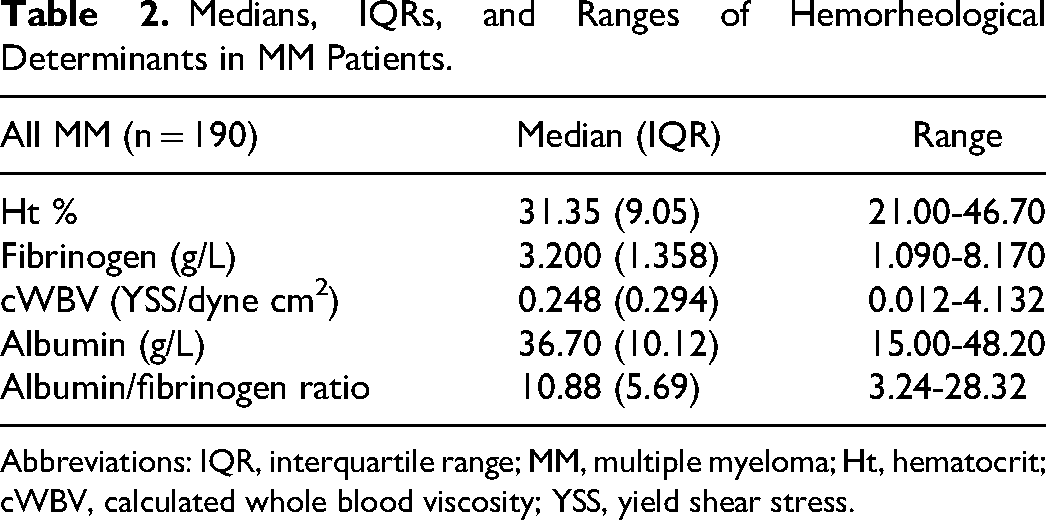
Abbreviations: IQR, interquartile range; MM, multiple myeloma; Ht, hematocrit; cWBV, calculated whole blood viscosity; YSS, yield shear stress.
Medians (IQR) of Hemorheological Determinants in MM Patients, Subdivided According to the Thrombotic Risk (IMWG).
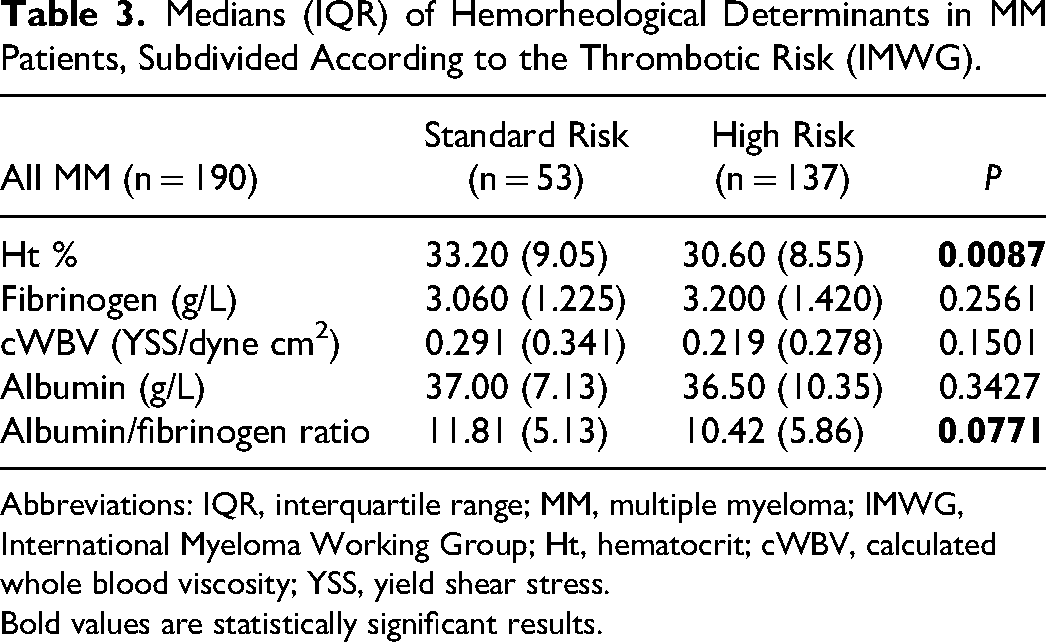
Abbreviations: IQR, interquartile range; MM, multiple myeloma; IMWG, International Myeloma Working Group; Ht, hematocrit; cWBV, calculated whole blood viscosity; YSS, yield shear stress.
Bold values are statistically significant results.
Medians (IQR) of Hemorheological Determinants in MM Patients, Subdivided According to the Thrombotic Risk (IMWG).
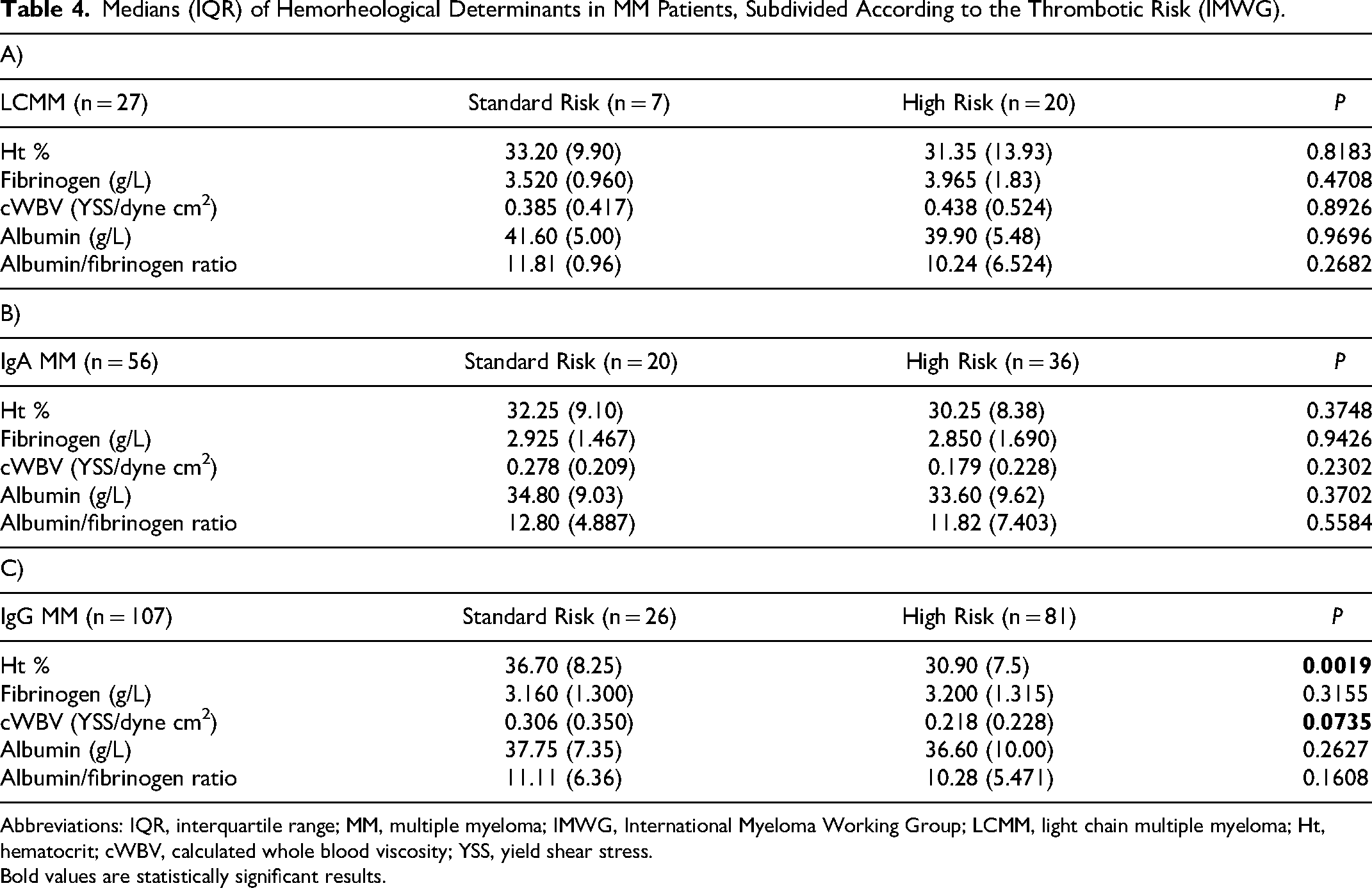
Abbreviations: IQR, interquartile range; MM, multiple myeloma; IMWG, International Myeloma Working Group; LCMM, light chain multiple myeloma; Ht, hematocrit; cWBV, calculated whole blood viscosity; YSS, yield shear stress.
Bold values are statistically significant results.
Medians (IQR) of Hemorheological Determinants in MM Patients, Subdivided According to the IMPEDE VTE Score.
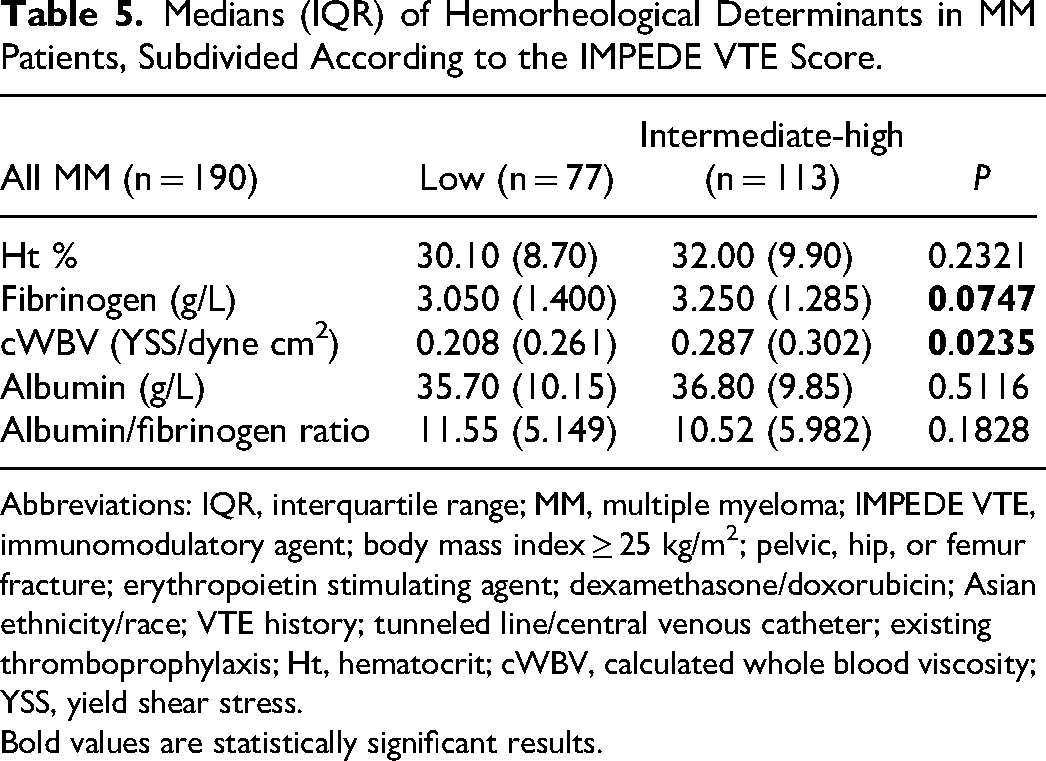
Abbreviations: IQR, interquartile range; MM, multiple myeloma; IMPEDE VTE, immunomodulatory agent; body mass index ≥ 25 kg/m2; pelvic, hip, or femur fracture; erythropoietin stimulating agent; dexamethasone/doxorubicin; Asian ethnicity/race; VTE history; tunneled line/central venous catheter; existing thromboprophylaxis; Ht, hematocrit; cWBV, calculated whole blood viscosity; YSS, yield shear stress.
Bold values are statistically significant results.
Medians (IQR) of Hemorheological Determinants in MM Patients, Subdivided According to the IMPEDE VTE Score.
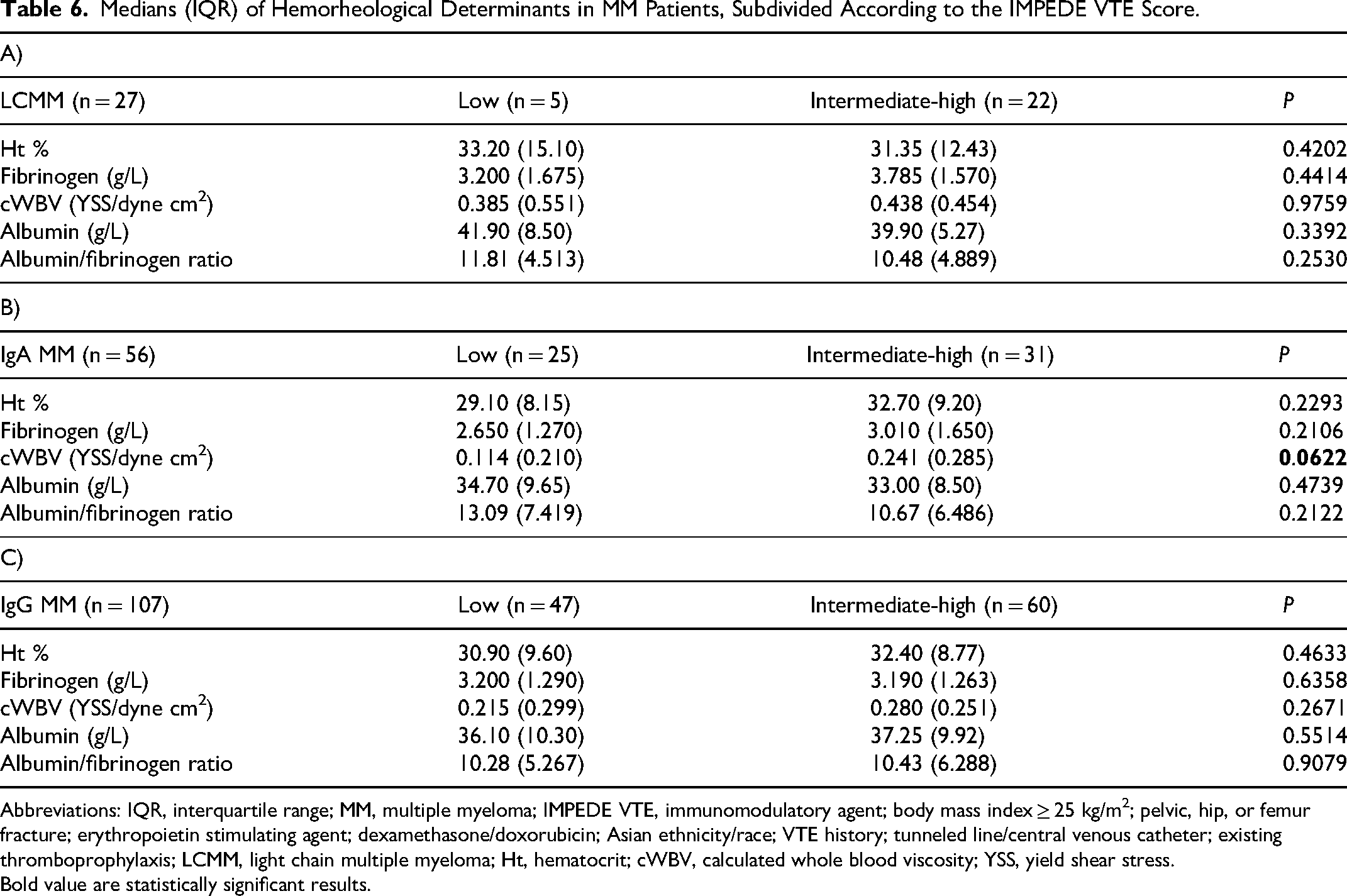
Abbreviations: IQR, interquartile range; MM, multiple myeloma; IMPEDE VTE, immunomodulatory agent; body mass index ≥ 25 kg/m2; pelvic, hip, or femur fracture; erythropoietin stimulating agent; dexamethasone/doxorubicin; Asian ethnicity/race; VTE history; tunneled line/central venous catheter; existing thromboprophylaxis; LCMM, light chain multiple myeloma; Ht, hematocrit; cWBV, calculated whole blood viscosity; YSS, yield shear stress.
Bold value are statistically significant results.
Discussion
In the context of neoplastic diseases, VTE certainly has a significant impact on the clinical management and quality of life of patients. Deep vein thrombosis and its potential complications, such as pulmonary embolism, represent the clinical manifestations of VTE and, among the hematologic malignancies, MM is the one with the highest risk of thromboembolic events. The importance of these complications has made necessary not only to search for stratification tools able to predict the thrombotic risk, but also to have an in-depth knowledge of the causes and pathogenic moments with a greater impact on the development of thromboembolic phenomena. Among the factors implicated in the development of VTE in MM, blood viscosity plays a key role, and hence our aim of evaluating whether some hemorheological determinants, obtained in a calculated way, could be related to the different thrombotic risk. We therefore stratified the study population using two different approaches, the one provided by the international guidelines of the IMWG/NCCN and the second one represented by IMPEDE VTE score, noting that these two risk stratification tools do not appear to be superimposable. In fact, in the whole cohort of MM patients, only 53/190 fell into the “standard risk” group according to the IMWG/NCCN score; while using the IMEPDE VTE score 77/190 patients fell into the “low-risk” group. In relation to VTE, we also evaluated the number of patients who developed thromboembolic events during the treatment (18/190) and then we calculated, in this very small subgroup, the median value and the interquartile range of the YSS, observing that, these latter are higher, although non statically significant, in patients with thromboembolic events (0.319 [0.314] versus 0.240 [0.394]). This is because, in the subgroup of patients who develop VTE, the values of hematocrit and fibrinogen are higher than compared to those observed in the whole cohort.
We must remember that, in MM patients, the decrease in hematocrit values, as well as the high levels of total plasma proteins and the reduction in albumin values significantly influence the calculated hemorheological profile.38‐42 The albumin not only represents an important nutritional indicator and a marker of inflammation but, in MM setting, it is related to the hemoglobin and disease stage, with a significant prognostic role. In fact, albumin levels are significantly reduced in patients with early mortality (12 months). 43 Similarly, to the behavior of plasma proteins, particular attention in MM patients should be paid to plasma levels of fibrinogen. In fact, some studies show a significant increase in fibrinogen values 44 and the albumin/fibrinogen ratio, used in this research as a surrogate for erythrocyte aggregation, has an important impact on the prognosis of patients with MM, representing an important mortality predictor. 45
It must be therefore considered that the variations of all these protein parameters and the associated anemic condition, inevitably influence the state of blood viscosity obtained in a calculated way, but in large patient cohorts, even an indirect evaluation can be useful in clinical monitoring. Moreover, the viscosity calculated according to specific formulas, does not consider two particularly significant rheological aspects, such as erythrocyte deformability, which operates above all in the microcirculation, where high shear rates are in force, and erythrocyte aggregation, which dominates instead in vascular districts where low shear rates prevail. In relation to this latter, we tried to overcome the impossibility of directly exploring and measuring the erythrocyte aggregation, using the albumin/fibrinogen ratio. Finally, from this research emerges that, the blood viscosity, expressed as YSS, although only calculated, is associated with a higher risk of thromboembolic events, but only when the thrombotic risk stratification is performed using the IMPEDE VTE score.
Conclusion
The pathogenesis of VTE in MM patients is not yet fully clarified as it includes multiple factors, linked to patient characteristics and to the disease itself. The need to better control this clinical condition has led over the years to the development of accurate risk stratification tools, aimed at implementing valid prophylaxis strategies and, at the same time, at a thorough analysis of possible pathogenic moments. Among the factors responsible for a higher incidence of thromboembolic events blood viscosity may play an important role. For this reason, we performed this retrospective clinical study with the aim to report the calculated hemorheological pattern in a cohort of patients with a new diagnosis of MM, but above all to evaluate the possibility of intercepting any associations between the c-WBV and the thrombotic risk. The obtained and above-discussed data allow us to conclude that the cWBV, expressed in terms of YSS is higher in subjects presenting an “intermediate + high” thrombotic risk according to the IMPEDE VTE score, but this is not observed when the stratification of the thrombotic risk is carried out according to the indications of the IMWG/NCCN. It is in fact known that WBV plays a key role in determining thrombotic events46‐48 and in our analysis, this hemorheological parameter is associated with a higher VTE risk, when the thrombotic risk stratification is performed using the IMEPDE VTE score. Despite the small sample size and the retrospective nature of the study, our data represent an important preliminary analysis, which serves as a starting point for further evaluations, possibly on a wider and more uniformly distributed sample, to confirm the importance of the hemorheological pattern in the VTE risk stratification of MM patients.
Footnotes
Authors’ Contributions
MC and GC conceptualized the study, analyzed, interpreted data, and wrote the original draft. MC acquired the data and performed writing–review and editing. RLP performed statistical analysis; visualization SM and SS. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.