
Abstract
Purpose
To evaluate the efficacy and safety of ultrasound-guided femoral nerve block (FNB) in treating great saphenous vein (GSV) insufficiency by endovenous radiofrequency ablation (EVRA) combined with punctate stripping (PS).
Methods
This was a single-center, retrospective cohort study. A total of 135 patients were divided into Group A (59 patients) and Group B (76 patients). All patients received tumescent anesthesia during the operation, and group A received an additional ultrasound-guided FNB before the procedure. Intraoperative and postoperative pain score, the volume of tumescent anesthesia solution (TAS), and other indicators were compared in two groups.
Results
Group A had a significantly lower intraoperative pain visual analog scale than group B (2.7 ± 1.2 vs 5.2 ± 1.5, P < 0.001). The volume of TAS in group A was significantly lower than that in group B (198 ± 26.6 ml vs 338 ± 34.7 ml, P < 0.001). Postoperative muscle strength of group A was significantly decreased compared with group B (54.2% vs 3.90%, P < 0.001); no patient had severe limitation of active movements in both groups, and all motor blocks recovered within 24 h. The incidence of skin ecchymosis in group A was lower than that in group B (18.6% vs 46.1%, P = 0.001). The operation duration of the two groups had no statistically significant difference.
Conclusions
Ultrasound-guided FNB in treating GSV insufficiency by EVRA combined with PS significantly relieved intraoperative pain and reduced the dosage of TAS and the incidence of skin ecchymosis without increasing the complications of anesthesia or any other surgical complications.
Keywords
Introduction
Lower extremity varicosis is a common clinical disease, usually caused by blood regurgitation due to valve insufficiency of the great saphenous vein (GSV), small saphenous vein, or communicating vein, of which the varicose GSV is the most common. 1 The lower extremity varicose vein is a manifestation of chronic venous insufficiency, with a high incidence and increasing with age, 2 with females (25%) higher than males (15%). In the early stage, there are no obvious clinical symptoms. However, with the progression of the disease, many symptoms affecting the quality of life may appear, among which leg heaviness (70.4%), pain (54.0%), and swelling (52.7%) are the main manifestations. 3
At present, the radical treatment of varicose GSV is a surgical intervention. The principles of surgical treatment include the removal of visible varicose veins and the correction of venous regurgitation. The traditional surgical method is high ligation of the main GSV and punctate stripping (PS) of varicose veins, which has the advantages of actual efficacy and low recurrence rate and the disadvantages of extensive trauma and multiple complications. With the development of technology, more and more patients prefer minimally invasive surgery, including endovenous radiofrequency ablation (EVRA), laser ablation, microwave ablation, and other minimally invasive methods. They have the characteristics of less trauma, quick recovery, and simple and safe anesthesia. 4
EVRA directly damages the vein wall by generating heat from the head of the radiofrequency catheter, denaturation, and contracting the collagen fibers, resulting in the contraction or occlusion of the vein. 5 Studies have shown that the success rate of EVRA is 93%, 6 and the reproducibility rate is 5.5%. 7 Our center has routinely performed EVRA combined with PS to treat GSV insufficiency. This method can not only correct blood regurgitation but also remove varicose veins and has achieved an excellent effect. It is relatively simple and safe to use a tumescent anesthetic solution (TAS) for local anesthesia during the operation. However, we found that multiple puncture injections into the skin would cause pain and discomfort to the patients, especially in the process of PS; the number of remedial injections and the amount of TAS were significant, significantly increasing pain, reducing comfort, and even affecting the surgical effect. It has been reported in the literature8,9 that the application of ultrasound-guided femoral nerve block (FNB) combined with tumescent anesthesia (TA) in lower extremity varicose surgery has a better anesthetic effect than TA alone. However, applying ultrasound-guided FNB with TA in EVRA combined with PS is rarely reported. The objective of this study was to compare the effects of ultrasound-guided FNB with TA and TA alone applied in treating GSV insufficiency by EVRA combined with PS.
Materials and Methods
Research Object
A total of 135 patients hospitalized in the interventional vascular department of Nanjing First Hospital from January 2020 to May 2023 who received EVRA combined with PS for unilateral lower extremity GSV insufficiency were selected and randomly divided into group A (59 cases) and group B (76 cases). All patients received TA during surgery, while group A received additional ultrasound-guided FNB before surgery. The ethics committee of the Nanjing First Hospital approved the present study and waived the requirement for written informed consent because of the retrospective study design.
Inclusion Criteria
(1) According to the Chinese Expert Consensus on the Diagnosis and Treatment of Chronic Venous Diseases of Lower Limbs, 10 primary varicose GSV was diagnosed through symptoms, physical examination, ultrasound and angiography. (2) According to the Clinical-Etiology-Anatomy-Pathophysiology (CEAP) classification of chronic venous diseases of lower extremities published in 2004, 11 the grade was C2-C5. (3) Complete clinical data. (4) Voluntarily signed the informed consent form.
Exclusion Criteria
(1) Deep vein abnormalities, including valvular insufficiency, stenosis and thrombosis. (2) Excessive distortion of the main GSV. (3) Combined with cardiopulmonary insufficiency, abnormal coagulation function, and other primary diseases that cannot tolerate surgery. (4) The surgeon assessed that the surgery was not suitable.
Preoperative Preparation
Preoperative blood routine, coagulation routine, biochemistry, electrocardiogram, cardiac ultrasound, and lower extremity venography were performed in all patients. Patients were informed of anesthesia techniques and surgical risks and voluntarily signed an informed consent form. Skin preparation was performed, and the alignment of the varicose veins was marked on the skin using a marker before surgery.
Modified TAS and Nerve blocker 8
The modified TAS: 500 ml of normal saline, 20 ml of 2% ropivacaine, 200 mg of lidocaine injection, 0.25 mg of epinephrine, and 10 ml of 5% sodium bicarbonate. Nerve blocker: 20 ml of normal saline, 20 ml of 2% ropivacaine and 200 mg of lidocaine injection.
Surgical Procedures
Group B (with no FNB)
The patient was placed supine with routinely disinfected and draped, and the medial side of the knee joint was selected for local anesthesia. After an ultrasound-guided puncture of the GSV trunk using a 16G trocar, the 5F vascular sheath was inserted by the Seldinger technique. A radiofrequency electrode needle (CELON ProCurve, Olympus Surgical Technologies Europe, Japan) (diameter: 1.8 mm, heat length: 15 mm, total length: 1.2 m, marked points: every 10 cm) was inserted through a vascular sheath, and the tip was placed approximately 1 cm below the saphenous femoral junction. Then, under ultrasound guidance, the TAS was injected along and around the trunk of the GSV, and the affected limb was elevated during the injection to promote blood flow emptying. After anesthesia, the radiofrequency host (CELON Lab PRECISION, Olympus Surgical Technologies Europe, Japan) was started, and the power parameters were set to 10 to 15W. The Radiofrequency needle was initiated by stepping on the pedal. It was slowly withdrawn at a speed of 0.2 cm /s to ensure that the electrode needle was working under the typical prompt sound of the host computer. If the host computer shows an abnormal prompt sound, stop working, clean the head of the electrode needle, and insert it again for work. At the same time, the assistant kept his hand above the electrode needle to compress the GSV and promote the complete closure of the vein. The varicose veins in the lower leg were stripped, and the TAS was used for local anesthesia before stripping. The patients were asked about their subjective feelings during stripping, and additional anesthesia was performed if it was insufficient. Small incisions were closed by tissue glue.
Group A (with FNB)
The ultrasound-guided FNB was first completed after disinfected and draped. The patient was placed supine with the leg slightly abducted and externally rotated. The high-frequency linear array ultrasound probe was placed in the area above the transverse lines of the groin and perpendicular to the long axis of the common femoral artery. On this plane, the femoral vein, femoral artery, femoral nerve, and iliacus muscle could be observed from inside to outside. After local skin anesthesia, the needle was inserted at a roughly 45-degree angle using the In-plane technique from the lateral side. After ensuring no blood was withdrawn, about 20ml of anesthetic was circularly injected around the femoral nerve so that the anesthetic could wrap around the nerve and avoid direct puncture. After the onset of anesthesia, the remaining surgical procedures were the same as in group B.
Postoperative Management
After the operation, the affected limb was bandaged with an elastic bandage, the elastic socks were replaced 3 days later, and the incision was observed. Patients were instructed to perform ankle pump exercises and get out of bed appropriately when lying in bed. All patients received anticoagulant therapy for at least 1 month after the operation. An ultrasound examination was performed before discharge to determine whether hematoma and thrombosis occurred.
Observation Target
General data of patients were collected: age, gender, BMI, smoking history, history of cardiac insufficiency, family history, history of antithrombotic drugs, the surgical side of affected extremities, and CEAP grade at admission. A visual analog scale (VAS) was used to score the most severe pain experienced by the patients during the operation and within 24 h after the operation. The patients were asked to do leg lift and knee extension to evaluate the muscle strength level (0–5) at the end of the operation and 24 h after the operation, and the degree of femoral nerve motor block was defined as severe (0–1), moderate (2–3), mild (4), and no block (5). The duration of surgery was defined as from the beginning of disinfection to the end of dressing. The dosage of intraoperative TAS was the initial volume minus the remaining volume. Postoperative complications were recorded, including but not limited to incision bleeding, incision infection, subcutaneous hematoma, skin ecchymosis, and deep vein thrombosis. VAS score, motor block degree, operation duration, TAS dosage, and postoperative complications were compared between the two groups.
Statistical Analysis
SPSS 26.0 software was used for statistical analysis. Measurement data of normal distribution were expressed by mean ± standard deviation (x ± s), and an independent Sample t-test was used to compare groups. Categorical data were expressed by n (%), and comparison between groups was performed by χ2 test. The rank sum test was used to compare rank data. A two-sided test was used, and P < 0.05 was considered statistically significant.
Result
The two groups had no significant differences concerning age, gender, BMI, smoking history, history of cardiac insufficiency, family history, history of antithrombotic drugs, the surgical side of affected extremities, and CEAP grade (Table 1).
Baseline Data of Patients in Two Groups.
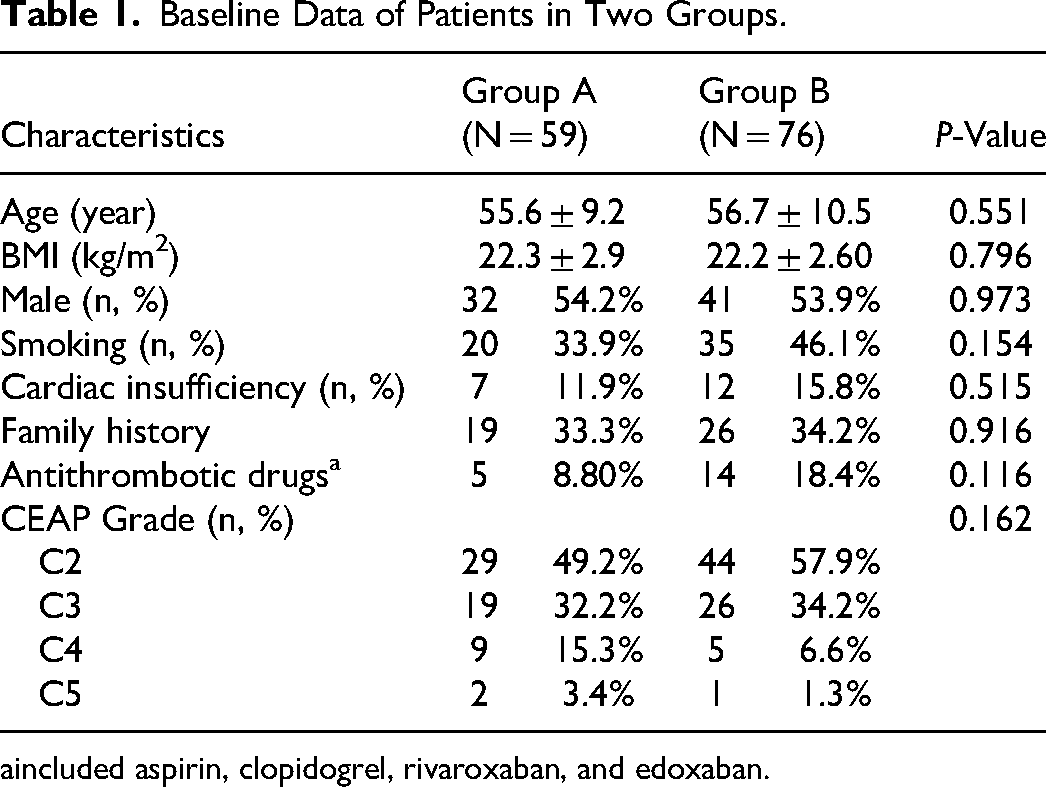
included aspirin, clopidogrel, rivaroxaban, and edoxaban.
The degree of intraoperative pain in group A was significantly less than that in group B (P < 0.001). At the same time, the two groups had no significant difference in pain within 24 h after surgery (Table 2). The two groups had no significant difference in operation duration between the two groups (Table 2). The volume of TAS used during surgery in group A was statistically significantly less than that in group B (P < 0.001) (Table 2).
Comparison of two Groups in Pain Score (VAS), Operation Duration, Volume of TAS, Motor Block and Postoperative Complications.

TAS, tumescent anesthesia solution; VAS, visual analog scale.
Motor block was measured at the end of the surgery immediately and 24 h after surgery and assessed by muscle strength grade; it showed that there was a statistically significant difference between the two groups; only 3.9% of group B had mild limitation of active movements while 5.1% and 49.2% of group A had mild and moderate limitation of active movements, respectively (P < 0.01). No patient had severe limitation of active movements in both groups, and none had any motor block at 24 h after surgery (Table 2).
Regarding postoperative complications, the incidence of skin ecchymosis in group A was lower than that in group B (P = 0.001). The two groups had no statistically significant difference in the incidence of incision bleeding and subcutaneous hematoma, while no severe complications occurred (Table 2).
Discussion
There are many methods for treating GSV insufficiency, each with advantages and disadvantages. 12 EVRA can close the main GSV and block venous regurgitation, and PS can eradicate local varicose veins with a small incision. EVRA combined with PS has a definite curative effect, minimally invasive esthetics, quick recovery, fewer complications, and less pain. In order to protect the surrounding tissues from radiofrequency energy and reduce the pain caused by thermal injury and stripping, it is necessary to puncture and inject TAS at multiple points around the GSV and varicose venules. 13 As a method of local anesthesia, TA was first proposed by Klein 14 in 1987. In recent years, it has been widely used in surgical treatment, that is, by injecting a solution composed of epinephrine, lidocaine, and sodium bicarbonate into the subcutaneous tissue to make the subcutaneous tissue edema, separate the space between tissues and cells, compress the tiny blood vessels, to relieve pain, reduce bleeding, and protect tissues. Although local TA avoids the injury and risk associated with epidural anesthesia, the most significant pain experienced by patients during surgery is the pain and discomfort caused by multiple injections, which will reduce patient satisfaction and affect the surgical effect and increase the occurrence of postoperative complications. Frequent supplementary TAS injections can also affect the surgeon's concentration and increase the operation time.
Applying an ultrasound-guided FNB can further reduce the pain caused by puncture and injection. The femoral nerve is the largest branch of the lumbar plexus; it crosses the inguinal ligament and then divides into anterior and posterior branches. The anterior branch innervates the motor nerves of the sartorius and pubic muscles and the sensory nerves of the anteromedial skin of the thigh. The posterior branch innervates the quadriceps’ motor nerve and the medial leg's sensory nerve through the saphenous nerve. By blocking the femoral nerve, adequate analgesia can be provided in the anterior and medial sides of the thigh and lower leg, which are also the typical position of GSV insufficiency and resulting varicose veins. 15 Ultrasound can clearly show the location of the femoral nerve, which makes its blocking technique easy with few complications.
The procedure duration of ultrasound-guided FNB was about 8 to 10 min, whereas, in this study, the two groups had no significant difference in the procedure time. In group B without FNB, the operation duration was not shortened; it was considered that multiple supplementary TAS injections added additional operation time due to insufficient analgesia during the operation.
The intraoperative pain score of group A was significantly lower than group B's, indicating that FNB has a very excellent anesthetic effect on the pain caused by puncture, thermal injury, and PS during operation. The dose of TAS used during the operation in group A was also significantly lower than that in group B, indicating that the effect of basic anesthesia in group A was better than that in group B, and the additional TAS dose to reduce pain was also lower than that in group B.
It should be emphasized that the role of TAS was irreplaceable during the EVRA of the GSV, and it was necessary to inject an adequate volume of TAS in order to protect the tissues surrounding the vein. Applying FNB could reduce the pain caused by puncture injection, but it did not reduce the amount of TAS during EVRA. The reduction in TAS consumption was mainly during PS. Varicose clusters in the lower extremities were often extensive and required multiple PS. The pain caused by PS was severe and could not be tolerated by the patients without local anesthesia. The consumption of TAS used during PS was significant. If the local anesthesia was inadequate, the patients could still experience tingling and pulling pain. The pain caused by multiple puncture injections and inadequate local anesthesia could bring both great fears to the patients and psychological pressure and operational fatigue to the surgeons. After using FNB, however, only a tiny amount of TAS was required for pain relief, and the number of puncture injections was reduced. Especially in areas with adequate nerve block, PS could be performed directly without local anesthesia, and the patients felt no pain. Therefore, applying FNB could improve the anesthetic effect in PS, reduce the repeated local anesthesia operation, reduce the consumption of TAS, and ensure smooth operation.
The two groups had no significant difference in the highest pain scores experienced in the first 24 h after surgery. The duration of the FNB is approximately 1–12 h, which varies with the formulation of TAS and the patient's constitution. The highest pain score in the first 24 h after surgery means the pain score after anesthesia wore off. The pain after anesthesia wore off was within the acceptable range of the patient, and there was no significant difference between the two groups.
The peripheral nerve block is a relatively safe clinical technique; the overall incidence of complications is about 0.05%, mainly including nerve injury (0.03%), peripheral tissue injury, local anesthetic overflow, local anesthetic toxicity, and infection. Most nerve damage manifested as paresthesia or muscle weakness in the block area, which could be recovered quickly. The incidence of long-term or permanent nerve damage was very low. With the application and proficiency of ultrasound visualization technology, the incidence of femoral nerve injury will be lower and lower. 16 The muscle strength of patients in group A was significantly lower than that in group B immediately after the operation, but there was no severe motor block in both groups. The muscle strength of patients in both groups returned to normal within 24 h after surgery, and there were no symptoms of neurological injury. In group B, three patients had a mild nerve block, which was considered to be related to local nerve paralysis or neurotoxicity caused by an excessive dosage of TAS.
The incidence of postoperative skin ecchymosis in group A was lower than that in group B. Since patients in group B had a higher intraoperative pain score, the increase in blood pressure caused by pain would increase the amount of local blood loss during PS. During additional TAS injections, the operation and bleeding time were also increased, resulting in an increased incidence of skin ecchymosis in group B. However, the skin ecchymosis is acceptable and will gradually disappear within a week. Due to the small incision, although 14.3% of the patients used antithrombotic drugs, the incidence of incision bleeding and subcutaneous hematoma was low in both groups, and there was no significant difference between the two groups. Low molecular weight heparin anticoagulant therapy was used routinely after surgery, and the patients were encouraged to do more ankle pump exercises while resting in bed. During hospitalization, no severe complications, such as deep venous thrombosis and superficial thrombotic phlebitis, occurred in the two groups.
There are some limitations in this study. First, this study is retrospective, with a small sample and a single center. Second, the follow-up time of this study is short, and the types of complications involved were relatively limited. Therefore, in the later period, it is necessary to expand the sample size for multi-center research, extend the follow-up time to verify the accuracy of the conclusion, and effectively apply it in the clinic.
In conclusion, ultrasound-guided FNB in treating GSV insufficiency by EVRA combined with PS can significantly relieve intraoperative pain and reduce the dosage of TAS and the occurrence of skin ecchymosis complications without increasing the complications of anesthesia or delaying postoperative rehabilitation exercise, which is worthy of clinical promotion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jiangsu Medical Association Interventional Medicine Special Funding Project [grant number SYH-3201140-0026(2021021)].
Ethics Approval and Informed Consent
The ethics committee of the Nanjing First Hospital approved the present study and waived the requirement for written informed consent because of the retrospective study design.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.