
Abstract
Postpartum hemorrhage (PPH) is responsible for 30% to 50% of maternal deaths. There is conflicting evidence if prepartum anemia facilitates PPH. A comprehensive analysis of studies describing their relation is missing. An extensive database search was conducted applying the terms “anemia” OR “hemoglobin” AND “postpartum hemorrhage.” We used a random-effects meta-analysis model to estimate an overall odds ratio (OR) for PPH and prepartum anemia, separating studies that were conformant and non-conformant with the World Health Organization (WHO) definitions for anemia. The search yielded 2519 studies, and 46 were appropriate for analysis. The meta-analyses of WHO-conformant (n = 22) and non-conformant (n = 24) studies showed that the risk of PPH was increased when anemia was present. The ORs were 1.45 (CL: 1.23-1.71) for WHO-conformant studies, 2.88 (CL: 1.38-6.02) for studies applying lower thresholds for anemia, and 3.28 (CL: 2.08-5.19) for undefined anemia thresholds. PPH risk appeared to increase with lower anemia thresholds. Prepartum anemia is associated with an increased risk of PPH, an observation that is important regarding improved anemia correction strategies such as iron supplementation.
Introduction
Postpartum hemorrhage (PPH) is a life-threatening complication following vaginal birth or caesarian delivery. The incidence of PPH has increased even in high-income countries,1–5 where it ranges between 2.5% and 10.4%. 6 PPH remains the leading cause of maternal mortality worldwide, accounting for up to 30% of all maternal deaths. 7 Between 2000 and 2017, the worldwide maternal mortality rate declined by 38% (from 342 to 211 per 100 000 live births), but geographical differences persist. For instance, mortality has improved in South East Asia during this period, but maternal deaths in sub-Saharan Africa remain high. 8 As such, the Sustainable Development Goal of 70 deaths per 100 000 live births by 2030 remains a global challenge. 8
There is some evidence that low hemoglobin levels during pregnancy put women at risk for PPH, suggesting prepartum anemia facilitates PPH.9–18 In turn, PPH augments the risk of maternal death. 7 The underlying pathophysiology regarding the influence of anemia on PPH remains poorly understood, but evidence gathered in recent years suggests that red blood cells may play an essential role in hemostasis.19–21 This is important since it is estimated that nearly 529 million women of reproductive age, including 38% of all pregnant women, are affected by prepartum anemia worldwide. 22 The most common reason for prepartum anemia is a preventable condition, iron deficiency (≈50%), with hemoglobinopathies and infectious diseases (eg, malaria) making up the remainder of causes.23,24 This is especially meaningful for low- and middle-income countries as they are affected most by prepartum anemia. 25
One major impediment towards illuminating the association of prepartum anemia and PPH is the lack of uniform definitions for both conditions. The World Health Organization (WHO) definition of PPH is blood loss of ≥500 ml within 24 hours after vaginal birth, and ≥1000 ml within 24 hours after caesarean delivery, whereas the American College of Obstetrics and Gynecology defines PPH as blood loss of ≥1000 ml regardless of delivery mode. However, there is a lack of standardized methods to measure blood loss, often leaving it to attending physicians, midwives, or community health workers to provide an estimate, sometimes incorporating hemodynamic change as a clinical sign of blood loss.9,10,15,16
Similarly, a lack of uniform definitions also applies to prepartum anemia. Hemoglobin levels change during pregnancy with a natural drop during the second trimester due to plasma volume expansion. Therefore, the WHO and the Center for Disease Control and Prevention recommend trimester-specific cut-offs, 23 which complicates the diagnosis of prepartum anemia especially in resource-limited countries where hemoglobin measurements are often performed only once per pregnancy or only in women in distress. 9 In many studies anemia is defined as hemoglobin level of <11 g/dl during all stages of pregnancy, without distinction of severity based on hemoglobin levels, and without knowledge of hemoglobin levels just prior to delivery.
We intended to investigate the association of prepartum anemia as a risk factor for PPH with a conventional meta-analysis, namely studies that all approached the research question (how is prepartum anemia associated with PPH?) in the same way. Accordingly, only studies conformant with the WHO Threshold for prepartum anemia (hemoglobin level of <11 g/dl) were to be included in the meta-analysis. However, many studies had alternative definitions. Since information from such studies may still be valuable and contribute knowledge, we added separate analyses to also assess the association of prepartum anemia and PPH in studies with alternative criteria for prepartum anemia. This approach generated a comprehensive perspective of prepartum anemia and its effect on PPH, and identified gaps, which could be addressed during next generation study design.
Methods
Study Search, Selection, and Extraction
We followed the MOOSE guidelines for meta-analysis and systematic reviews of observational studies. 26 Studies published up to December 2021 that addressed the topic of prepartum anemia and risk of PPH were included. A MEDLINE, EMBASE, CENTRAL, Ovid, and Google Scholar database search was conducted applying the terms “anemia” OR “hemoglobin” AND “postpartum hemorrhage.” MeSH (Medical Subject Headings) and Emtree terms as a thesaurus-controlled vocabulary were also part of the search, which included alternative spellings. Study titles and abstracts were screened, and reference lists were hand screened for additional studies. Full-text examination was performed by HG, LL, and MMG. Studies were included if they were: observational, peer-reviewed, and written in English (or English translation available). We excluded studies that did not provide a result for at least 1 of our outcomes of interest. We extracted information from the selected full-text articles using a comprehensive data extraction sheet. Authors individually extracted data; however, questionable results and ambiguous data were discussed by at least 2 of the authors until a consensus was reached. Data extracted included: author, year of publication, country of study, study type, study size, anemia definition and prevalence, and PPH definition and incidence.
Studies that recognized their anemia exposure group as having a hemoglobin threshold of 11 g/dl (WHO-conformant) were named the “WHO Threshold” group. Other groups of studies with alternative thresholds for anemia (either more severe or undefined) were analyzed separately; we named these groups the “Lower Threshold” group and the “Unspecified Threshold” group, respectively.
Statistical Analysis
The primary outcome was the risk of PPH (expressed as the odds ratio [OR]) in women experiencing prepartum anemia. Secondary outcomes were prevalence of prepartum anemia and incidence of PPH. We used the information (when sufficient) provided in each study to calculate an OR, as well as the incidence of PPH and the prevalence of prepartum anemia calculated as p^ = x/N, where x was the number of cases and N was the number of patients at risk. If the reported prevalence and/or incidence was not representative of the population at risk (as would be the issue in a case-control study due to an intentionally constructed case:control proportion), it was dropped unless a statistic representing the broader population was also provided.
Pooled results—overall OR, overall incidence of PPH, and overall prevalence of prepartum anemia—were estimated by fitting random-effects models that accounted for weight and heterogeneity between studies. 27 The distribution of ORs was log-normal. Proportion (percentage) data are often normalized via arcsine square root transformation. 28 However, for likelihood of both anemia and PPH, a logit transformation improved normality more effectively (agreement among assessments: histogram, Q-Q plot, and Kolgoromov-Smirnov Dmax statistic).
We prepared a funnel plot in order to detect selection bias (failure to perform proper randomization of individuals) or publication bias (more frequent publication of data in case of significant results) by plotting precision, shown as the inverse of the standard error of log(OR), against log(OR). 29 All statistical analysis was done using SAS 9.4.
Results
Literature Search
The search yielded 2519 publications (Figure 1). We excluded 2428 publications due to being non-relevant or duplicates (n = 2412), non-English (n = 7), not peer-reviewed (n = 6), or unable to obtain (n = 3). The remaining 91 publications were assessed for eligibility; 45 were excluded for lack of data to calculate at least 1 of the outcomes of interest—anemia prevalence, PPH incidence, or an OR associating the 2 parameters. The remaining 46 studies originated mostly from Asia (n = 18) and Africa (n = 14), and fewer from Europe (n = 7), North America (n = 3), Oceania (n = 3), or South America (n = 1). They were mostly cohort studies (n = 30 [15 retrospective and 15 prospective]), with some case-control (n = 11) or cross-sectional (n = 5) design. All hemoglobin measurements were obtained prepartum, which ensured hemoglobin measurements were not a consequence of peri- and/or postpartum bleeding. Twenty-two of these studies defined anemia using the WHO-conformant threshold of <11 g/dl (Table 1),9,10,12,14,16,30–46 the other 24 studies fell into the Lower or Unspecified Threshold groups and were analyzed separately (Table 2).11,13,15,47–67

Flow chart of publication search.
WHO-Conformant Study Characteristics (n = 22).

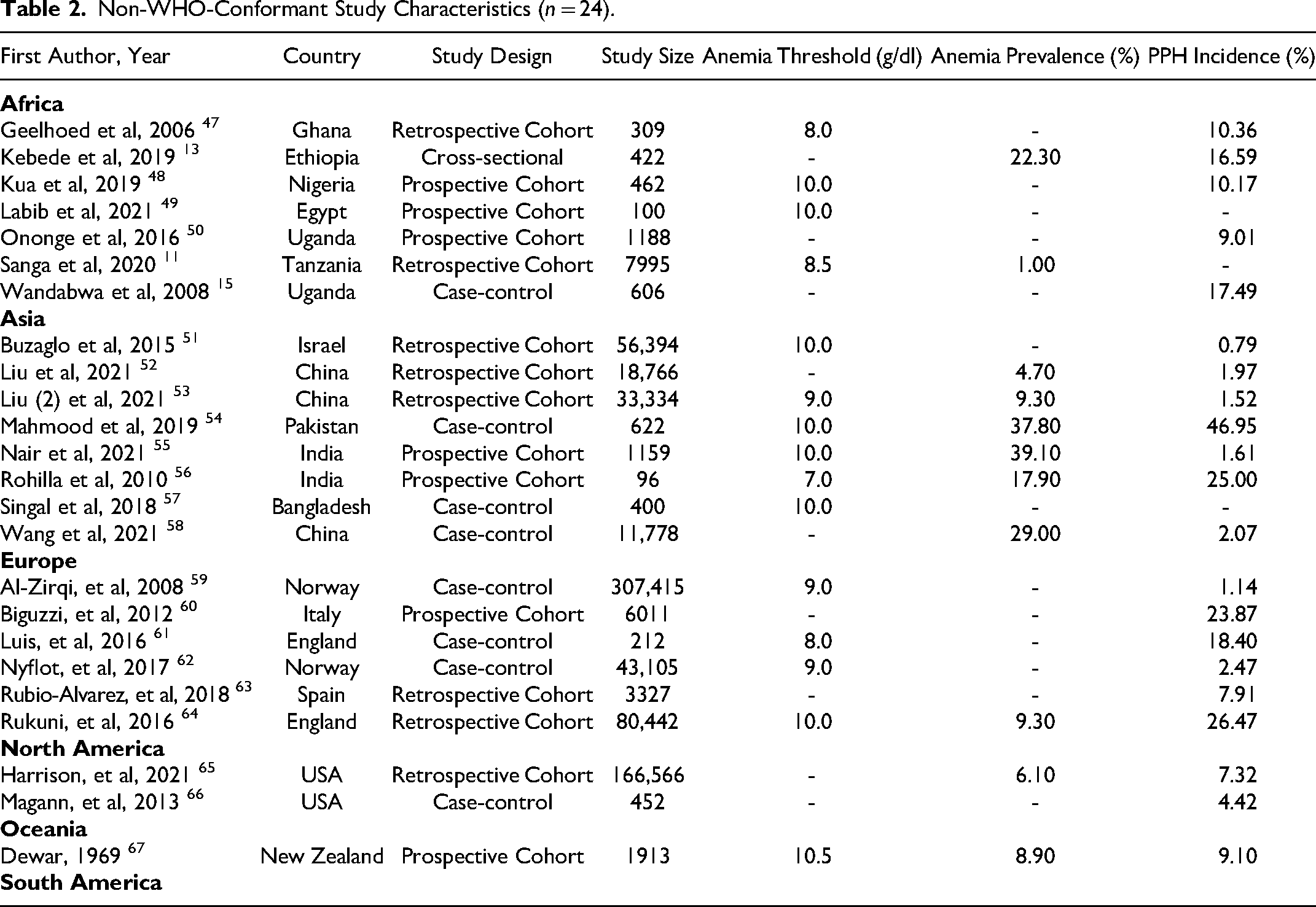
Non-WHO-Conformant Study Characteristics (n = 24).
Meta-Analysis of the Studies Conformant With the WHO Anemia Threshold
We performed a meta-analysis on studies that were WHO-conformant in their definition for anemia (threshold of <11 g/dl). These studies originated from Asia (n = 10), Africa (n = 7), Oceania (n = 2), Europe (n = 1), North America (n = 1), and South America (n = 1) (Table 1). There was a greater risk of PPH in women with prepartum anemia, with pooled OR = 1.45 (CL: 1.23-1.71, studies = 16, n = 533,330). Study ORs ranged from 0.91 (the only study in this group with OR <1) to 5.65 (Figure 2). Nineteen of the 22 studies provided data to calculate anemia prevalence, resulting in a pooled estimate of 42.94% (95% confidence limits [CL]: 25.54%-62.28%) (Table 3). The range of prevalence was wide, 6.30% to 87.70%. Eighteen of the 22 studies provided data to calculate PPH incidence, resulting in a pooled estimate of 5.08% (CL: 3.26%-7.85%). The range of incidence was also wide, 0.80% to 20.30%.

Forest plot of ddds ratios relating anemia as a risk factor for PPH among “WHO-conformant” studies. A logarithmic scale (base 2) was used to capture the range of confidence intervals.
Anemia Prevalence and PPH Incidence Among Different Groups of Studies.

Abbreviations: CI, confidence interval; N, number of studies; SE, standard error.
In order to evaluate publication or selection bias, we performed a funnel plot analysis (Figure 3). The 4 studies with greater precision (>10, observationally) had very similar ORs, and the studies with less precision had much a wider scatter of ORs. Also, there was a lack of symmetry, suggesting that some bias may be present, although it is difficult to draw firm conclusions based on small sample size.

Funnel plot among the WHO-conformant studies.
Characteristics of the Studies Not Conformant With the WHO Anemia Definition
We conducted 2 seperate meta-analyses on the 24 studies that used alternative definitions for anemia than the WHO (hemoglobin <11 g/dl) (Table 2). These studies originated from Asia (n = 8), Africa (n = 7), Europe (n = 6), North America (n = 2), and Oceania (n = 1). Fifteen of these studies were included in the Lower Threshold Group since they defined anemia using various thresholds below 11 g/dl (range of thresholds: 7-10.5). The other 9 studies did not explicitly define their threshold for anemia and were therefore included in the Unspecified Threshold Group.
Meta-Analysis of the Lower Threshold Group
The most common alternative definition of anemia was a hemoglobin threshold of 10 g/dl (7 of 15 studies). Thresholds of 9 g/dl and 8 g/dl were utilized by 3 and 2 studies, respectively. Thresholds of 10.5, 8.5, and 7 were employed by 1 study each. The pooled OR estimate associating prepartum anemia with PPH was 2.88 (CL: 1.38-6.02) (Figure 4). The number of studies with available OR and pooled sample size was similar to the WHO Threshold group (studies = 12 vs 16 and n = 533 330 vs 524 850, respectively). Despite those similarities, the Lower Threshold group exhibited much larger variability in its pooled OR estimate than the WHO Threshold group (logSE = 0.376 compared to logSE = 0.084 in the WHO-conformant group). Seven of the 15 studies supplied a valid parameter for anemia prevalence, resulting in a pooled estimate of 12.00% (CL: 6.74%-20.42%) (Table 3). Twelve of the 15 studies provided a valid parameter for PPH incidence, resulting in a pooled estimate of 6.68% (CL: 2.80%-15.11%).

Forest plot of odds ratios relating anemia as a risk factor for PPH among “Lower Threshold” studies. A logarithmic scale (base 10) was used to capture the range of confidence intervals.
Meta-Analysis of the Undefined Threshold Group
Among the 9 studies that did not specify a threshold for anemia, 6 provided enough information to calculate an OR, with a pooled estimate of 3.28 (CL: 2.08%-5.19%) (Figure 5). Only 4 studies provided a valid anemia prevalence, resulting in a pooled estimate of 12.21% (CL: 5.63%-24.49%) (Table 3). All 9 Undefined Threshold studies provided PPH incidence, with a pooled estimate of 7.61% (CL: 4.30%-13.13%).

Forest plot of odds ratios relating anemia as a risk factor for PPH among “Undefined Threshold” studies. A logarithmic scale (base 2) was used to capture the range of confidence intervals.
Additional Observations Related to Anemia, PPH, and Blood Loss Assessment
This review also revealed additional insights regarding the heterogeneity in timing of blood draws during pregnancy, the practice of blood loss assessments and PPH definition. The timing of hemoglobin measurements throughout pregnancy was variable between studies: 18 studies measured hemoglobin prior to delivery, 13 studies at any antenatal visit, 8 studies used any measurement during late pregnancy, whereas 3 used early pregnancy hemoglobin values as their variable of interest. Four studies did not specify when hemoglobin was measured. Objective blood loss assessment during delivery was performed rarely. Only 11 studies used any type of measurement such as “under buttocks drapes,” pads, or a collector bag to objectify blood loss, and another 11 studies used visual estimates that were not further specified. Half of the studies (n = 23) did not specify how blood loss was assessed, and only 1 study used pre- and post-delivery hemoglobin as a parameter of blood loss. The definition of PPH varied widely. Irrespective of vaginal delivery or delivery by C-section, PPH was defined as blood loss of >500 ml (n = 20) in some studies, whereas some studies used more than 500 ml as a threshold (n = 7), or simply used clinical signs and symptoms as surrogate parameters for massive blood loss (eg, shock) (n = 4), or did not specify their definition at all (n = 14).
Discussion
The findings from this study indicate that prepartum anemia increases the risk of PPH regardless of anemia definition. ORs were 1.45 (CL 1.23-1.71) for studies using the WHO-conformant anemia definition, and increased to 2.88 (CL 3.38-6.02), and 3.28 (CL 2.08-5.19), for studies using lower anemia thresholds and unspecified anemia definitions, respectively. Therefore, it appears that the magnitude of the OR estimate is influenced by anemia definition and/or anemia threshold, with more severe anemia portending a more pronounced PPH risk.
We interpret the finding of a higher OR in the meta-analysis of the studies applying lower hemoglobin thresholds as an indicator that anemia severity may increase the likelihood of PPH. This hypothesis is supported by a previous review by Omotayo et al (including 13 studies), which found that mild and moderate anemia were not associated with PPH, but severe anemia was. 17 Additional support is provided by results from a systematic review and meta-analysis by Young et al, which also demonstrated a higher risk of PPH in anemic women (OR = 1.84), 18 aligning well with our results, especially in respect to the meta-analysis of the WHO Threshold group (OR 1.45). While Young's inclusion criteria allowed only for the analysis of 6 studies, the segregation of ORs by hemoglobin levels revealed that the risk to suffer from PPH increased with the degree of anemia. ORs increased from 1.84 to 2.40, to 4.02, and to 6.15 for hemoglobin thresholds of 11, 10, 9, and 8 g/dl, respectively, demonstrating that more severe anemia was associated with higher ORs for PPH. These results are further supported by just recently published results from the only 2 prospective studies to date. One study investigated the effects of tranexamic acid on PPH risk in 10 561 anemic women from low- and middle-income countries (Women-2 trial). The Women-2 trial investigators demonstrated an increasing risk of PPH as hemoglobin levels decreased, 68 irrespective of the several PPH definitions investigators were allowed to used in the trial. The second study analyzed 8799 consecutive delivery records in Maputo Central Hospital, the largest University Hospital in Mozambique, located in sub-Saharan Africa. While laboratory data were drawn only for women who were in distress on admission due to resource restrictions (n = 1137), analyses revealed a strong relationship between prepartum hemoglobin levels below a threshold of 10 g/dl and the risk of PPH. 69
The prevalence of prepartum anemia for the WHO Threshold group was 42.94%, which aligns well with WHO data (41.8%). 70 At least 50% to 75% of anemic pregnant women are assumed to have iron deficiency anemia, and preventive iron supplementation reduces maternal anemia at term by 70%.12,71 Anemia thresholds in the studies comprising the Lower Threshold group ranged from from 7 to 10.5, and tended to exclude women with mild anemia (hemoglobin levels 10-10.9 g/dl), and sometimes moderate anemia (7-9.9 g/dl). These exclusions likely explain the notably lower anemia prevalence compared to the WHO Threshold group (12.00% vs 42.94%).
PPH incidence estimates were similar (ranging 5.08%-7.61%) for WHO-conformant and non-conformant anemia definition groups, and fell within the worldwide reported incidence rates of 1% to 10%. 72 In addition to anemia, incidence rates are influenced by many factors such as PPH definition, delivery pratices, blood loss assessment methodology, and other locoregional risk factors.
The recognition that prepartum anemia, particulary moderate and severe anemia, increases the propensity of PPH should be helpful to devise strategies to optimize prepartum hemoglobin levels. Intensification of iron repletion strategies in iron deficiency anemia appears to be relatively low hanging fruit, while it may be more complicated to target other reasons for anemia during pregnancy such as hereditary hemoglobinopathies or anemia of inflammation.
Limitations
This study has several limitations. First, the lack of objective blood loss data in many studies may have caused over- or under-reporting of blood loss. Also, the studies encompassed all regions of the world with wide variations in socioeconomic conditions that may influence the study results but could not be accounted for in the available data. Information on regional socioeconomic conditions (eg, Human Development Index) and health care systems and adherence to institutional or (inter)national guidelines was missing from most studies. Such information could be helpful if included in future studies to better determine the influence of health systems, knowledge, and standard of living on the interplay of anemia, PPH, and maternal mortality.
Conclusions
Our findings suggest that prepartum anemia is associated with a higher rate of PPH, particularly when anemia is more severe. The recognition of a link between prepartum anemia and PPH is important since iron deficiency, which is responsible for most of the anemia worldwide,12,71 is preventable if recognized and treated. Future prospective studies investigating anemia or anemia mitigation in relation to PPH may benefit from WHO standardization of anemia and PPH definitions, including a standardized way to assess blood loss.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics and Patient Consent
Our institution does not require ethical approval for reporting of Meta-analysis.
Informed consent for patient information to be published in this article was not obtained because only secondary data of published studies was extracted and no individual can be traced back in any way.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Notes
This manuscript is not under consideration by any other journal. Preliminary results were presented at the Annual Meeting of the International Society of Haemostasis and Thrombosis (ISTH) in July, 2021 (virtual due to COVID-19).