
Abstract
Background
The etiology and mechanism of HELLP syndrome have not been fully elucidated. Previous studies show that HELLP syndrome is a severe phenotype of preeclampsia. Therefore, HELLP syndrome may be associated with the placental development and dysfunction. In addition, HELLP syndrome has significant characteristics of liver inflammation, complement system, and hemostatic system disorder. 7 Among them, hemostatic system disorder often causes postpartum hemorrhage in HELLP syndrome. Disseminated intravascular coagulation (DIC)is one of the main causes of postpartum hemorrhage in HELLP syndrome. 8 There may be the following mechanisms for the occurrence of DIC: (1) platelet activation, (2) endothelial dysfunction, (3) trophoblast activation of the coagulation cascade, and (4) liver function damage. 9 So, early monitoring of changes in coagulation system and timely treatment may reduce the complications of postpartum hemorrhage and improve the prognosis of pregnant women with HELLP syndrome.
Prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen (FIB), and
Patients and Methods
Patients
In a retrospective cohort study, 106 patients who were diagnosed as pregnant women with HELLP syndrome in Peking University Third Hospital from August 2010 to January 2017 were collected. Tennessee classification system was used as the diagnostic criterion of HELLP syndrome: platelet count <100 × 109/L, aspartate transaminase ≥70 UI/L or alanine transaminase ≥40 U/L, and intravascular hemolysis (observed in the peripheral blood analysis of the microscopic film abnormal, serum bilirubin ≥20.5 μmol/L or 1.2 mg/dL, lactate dehydrogenase > 600 U/L). 10 The demographic characteristics of maternal and fetus, postpartum complications, days of hospital stay, maternal age, weeks to terminate pregnancy, and maternal basic diseases are also included. Exclusion criteria included are as follows: (1) The pregnant women did not terminate their pregnancy in our hospital, and (2) the data of coagulation markers were not available within 3 days before delivery. In addition, 100 healthy parturient pregnant women were collected as a control group. Exclusion criteria included are as follows: (1) The pregnant women did not terminate their pregnancy in our hospital, and (2) cases had liver diseases, kidney diseases, hematological diseases, malignant tumor, familial thrombophilia, autoimmune diseases, and severe systemic bacterial or viral infections.
This study was approved by the hospital research and ethical committee. Every participant provided informed consent before any procedures were undertaken.
Measurement of Coagulation Markers
The laboratory coagulation markers within 7 days before delivery were measured. Blood samples were collected by venipuncture of an antecubital vein into vacuum tubes (Becton Dickinson Medical Devices Co Ltd, Franklin Lakes, New Jersey) containing 1:9 (vol/vol) of 0.109 mmol/L sodium citrate. All blood samples were centrifuged at 1500g for 15 minutes to obtain plasma within 1 hour. Each blood sample was tested within 4 hours. All assays were performed on an automated coagulation analyzer (ACL TOP, Instrumentation Laboratory, Spain). These tests were detected according to standard operating procedures of the instrument. The methods are listed below.
Reagents

Follow-Up and End Points
Patients were followed up at regular intervals. In the early pregnancy, patients were followed up at 3-month intervals. In the second trimester of pregnancy, patients were followed up at 1-month intervals. In the third trimester of pregnancy, patients were followed up at 1- to 2-week intervals. Afterward, patients were followed up for 1 month after delivery. The major events were postpartum hemorrhage and death.
Diagnostic criteria for postpartum hemorrhage include blood loss after vaginal delivery ≥500 mL or blood loss after cesarean delivery ≥1000 mL. 11
Statistical Analysis
Data were checked for normality. Normally distributed continuous are expressed as mean (
Results
Demographic and Clinical Characteristics of Pregnant Women With HELLP Syndrome
A total of 106 pregnant women with HELLP syndrome were included in the study. The demographic and clinical characteristics of 106 cases are listed in Table 1. Postpartum hemorrhage occurred in 11 cases of pregnant women with HELLP syndrome. The level of FIB in postpartum hemorrhage group was lower than that in nonpostpartum hemorrhage group (P < .001). Weeks of terminate pregnancy in postpartum hemorrhage group were shorter than that in nonpostpartum hemorrhage group (P = .026). The length of hospital stay in postpartum hemorrhage group was longer than that in nonpostpartum hemorrhage group (P = .038). The incidence of preeclampsia in pregnant women with postpartum hemorrhage was higher than that in pregnant women without hemorrhage (P = .011). No significant difference was found in age, blood pressure, multiple birth, dead fetus, APTT, PT, and D-D between postpartum hemorrhage group and nonpostpartum hemorrhage group (P < .05, respectively).
Demographics and Clinical Characteristics of Pregnant Women With HELLP Syndrome.

Abbreviations: APTT, activated partial thromboplastin time; D-D,
Comparison of the Level of FIB Between Healthy Pregnant Women Group and Pregnant Women With HELLP Syndrome Group
The level of FIB in postpartum hemorrhage pregnant women with HELLP syndrome was lower than that in nonpostpartum hemorrhage pregnant women with HELLP syndrome and healthy pregnant women (2.3 [1.68-2.81] vs 3.64 ± 0.95, P = .000; 2.3 [1.68-2.81] vs 4.48 ± 0.62, P = .000; Figure 1).

The level of prenatal FIB in postpartum hemorrhage group, nonpostpartum hemorrhage group, and healthy pregnant women. The level of FIB in postpartum hemorrhage group of pregnant women with HELLP syndrome was lower than that in nonpostpartum hemorrhage group of pregnant women with HELLP syndrome and healthy pregnant women (2.3 [1.68-2.81] vs 3.64 ± 0.95, P = .000; 2.3 [1.68-2.81] vs 4.48 ± 0.62, P = .000). FIB indicates fibrinogen; HELLP,
Prognostic Value of Coagulation Markers in Postpartum Hemorrhage of Pregnant Women With HELLP Syndrome
Multivariate analysis showed that decreased levels of FIB independently predicted postpartum hemorrhage of pregnant women with HELLP syndrome (odds ratio [OR] = 7.374, 95% confidence interval [CI], 1.551-35.05, P = .012; Table 2). The receiver operating characteristic curve showed that the area under the curve (AUC) of FIB when predicting postpartum hemorrhage was 0.841 (95% CI, 0.708-0.976; Figure2). When the cutoff value of FIB was 3.04 g/L, the sensitivity was 90.90% and the specificity was75.80%. The cutoff values were identified by Youden index (sensitivity + specificity − 1). When the level of FIB was 1.42 g/L, the specificity was 100% and the positive predictive value was 100%; when the level of FIB was 4.28 g/L, the sensitivity was 100% and the negative predictive value was 100%.The AUC of APTT and PT was 0.571 (95% CI, 0.397-0.745) and 0.613 (95% CI, 0.415-0.811), respectively.
Prognostic Factors for Pregnant Women With HELLP Syndrome With Postpartum Hemorrhage.
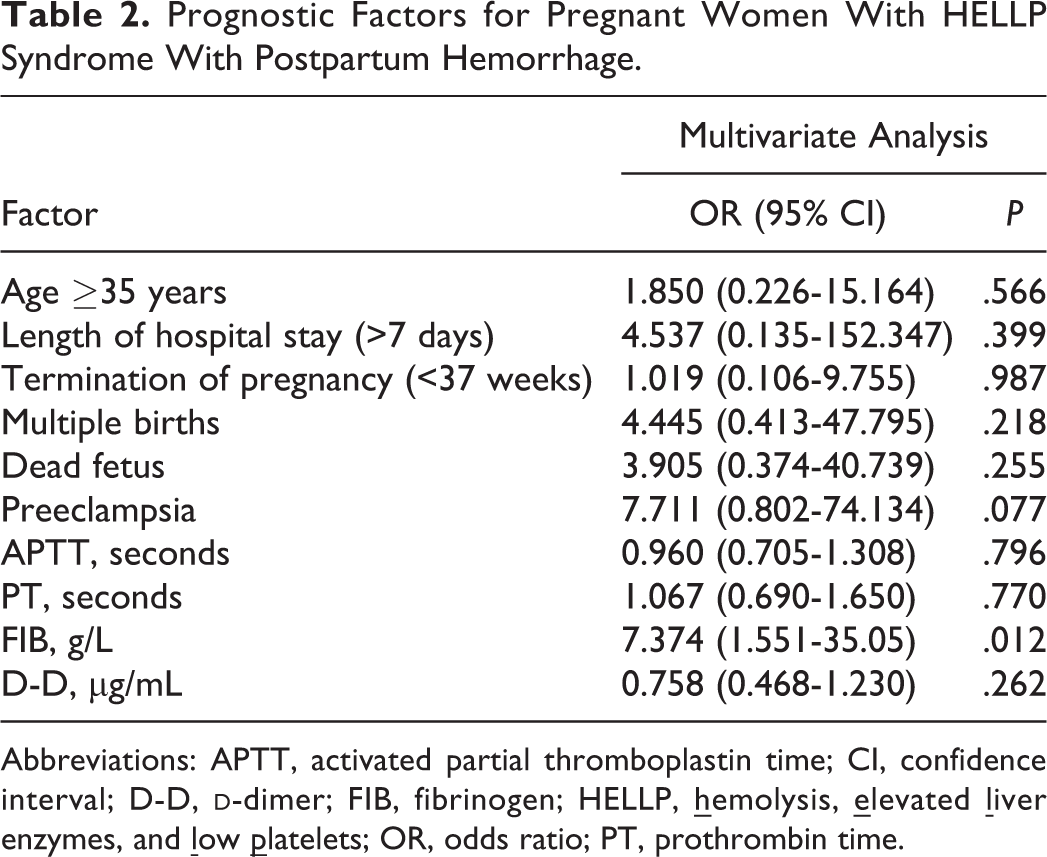
Abbreviations: APTT, activated partial thromboplastin time; CI, confidence interval; D-D,

The levels of prenatal FIB predict postpartum hemorrhage of pregnant women with HELLP syndrome. ROC showed that AUC of FIB when predicting postpartum hemorrhage was 0.841 (95% CI, 0.708-0.976). But, the AUC of APTT and PT was 0.571 (95% CI, 0.397-0.745) and 0.613 (95% CI, 0.415-0.811), respectively. When the cutoff value of FIB was 3.04 g/L, the sensitivity was 90.90% and the specificity was75.80%. The cutoff values were identified by Youden index (sensitivity + specificity − 1). When the level of FIB was 1.42 g/L, the specificity was 100% and the positive predictive value was 100%; when the level of FIB was 4.28 g/L, the sensitivity was 100% and the negative predictive value was 100%. APTT indicates activated partial thromboplastin time; AUC, area under the curve; CI, confidence interval; FIB, fibrinogen; HELLP,
Discussion
With the development of medicine, most of the pregnant women with HELLP syndrome had good outcomes. In this study, only 1 patient died. This result was consistent with the study of Rimaitis et al. 4 The main complication of pregnant women with HELLP syndrome was postpartum hemorrhage (11/106, 10.38%). The cause of postpartum hemorrhage is uterine contraction and hemostatic dysfunction. 16 In the normal physiological state, procoagulant system and anticoagulant fibrinolysis system maintain the balance of hemodynamics. However, patients with HELLP syndrome have extensive damage of endothelial cell, persistent activation of platelets, and clotting factors, followed by secondary activation of anticoagulant proteins and fibrinolysis systems, ultimately leading to persistent consumptive changes in the hemostatic system. Therefore, the disorders of coagulation system may predict postpartum hemorrhage of HELLP syndrome.
In our study, the level of FIB in healthy pregnant women was higher than that in pregnant women with HELLP syndrome (P < .001). This result was in agreement with the study of Haram et al. 8 Fibrinogen is a key component in the thrombosis and hemostasis. During normal pregnancy, in order to prepare for the delivery, the level of FIB in pregnant women will increase about twice as much as that in nonpregnant women. 8,17 When the level of FIB is below 3 g/L, coagulation abnormalities are usually present. 18 In this present study, the level of FIB in postpartum hemorrhage group was lower than that in nonpostpartum hemorrhage group (P < .001). Multivariate analysis showed that decreased FIB levels independently predicted postpartum hemorrhage of pregnant women with HELLP syndrome (OR = 7.374, 95% CI, 1.551-35.05, P = .012). The receiver operating characteristic curve showed that the AUC of FIB when predicting postpartum hemorrhage of pregnant women with HELLP syndrome is 0.841 (95% CI, 0.708-0.976). When the cutoff value of FIB was 3.04 g/L, the sensitivity was 90.90% and the specificity was75.80%. But, The AUC of APTT and PT was only 0.571 (95% CI: 0.397-0.745) and 0.613 (95% CI:0.415-0.811). This result was similar to the study of Collins et al 19 and Lockhart. 20 Their studies speculated that the level of FIB was more sensitive than PT, APTT, or platelet count in the prediction for hemorrhage. In their studies, when the level of FIB <2g/L, the positive predictive value for progression to severe postpartum hemorrhage was 100%; when the level of FIB >4g/L, the negative predictive value was 79%. This may be related to the fact that FIB was not only the substrate of coagulation cascade activation reaction but also the substrate of fibrinolytic system lysis reaction. 21 However, both PT and APTT can only reflect the activation of coagulation systems, but can’t reflect the state of anticoagulant and fibrinolytic systems. And, D-D can only reflect the degradation of fibrin formation, but can’t reflect the activation of coagulation systems. Therefore, as a common substrate of thrombin and plasmin, the level of FIB may be more sensitive to reflect the extent of hemostatic system consumption. These results suggest that maintaining a certain level of FIB in pregnant women with HELLP syndrome during the perinatal period may help reduce the complication of postpartum hemorrhage.
Conclusions
The low prenatal FIB level is a reliable biomarker to predict postpartum hemorrhage of pregnant women with HELLP syndrome, which make it useful for pregnant women with HELLP syndrome in guiding the surveillance therapy and prognosis assessment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Natural Science Foundation of China (81601824), CAMS Innovation Fund for Medical Sciences (CIFMS; Grant No. 2017-I2M-3-005), and the Peking University Third Hospital Clinical Key Project (BYSY2017008).