
Abstract
Aims
We investigated the incidence and clinical features of venous thromboembolism (VTE) in inpatients with mental illnesses.
Methods
We retrospectively analyzed records of inpatients with mental illnesses and confirmed VTE at The First Hospital of Hebei Medical University between August 2018 and July 2022. We recorded demographic characteristics, psychosis-related conditions, and thrombus distribution.
Results
Among 12939 patients diagnosed with mental illness, 156 (1.21%) presented with VTE at the first visit or during the disease course. Crude VTE incidence varied significantly across mental illnesses, being highest in patients with organic mental disorders (5.20%), followed by emotional disorders (1.10%), and others (P < 0.001). Distal and proximal deep venous thromboses (DVT) occurred in 79.17% and 20.84% of patients, respectively. The Hamilton Depression Scale (HAMD) score was higher in patients with proximal DVT than in those with distal DVT (P < 0.001). On multivariate analysis, the HAMD score (odds ratio [OR] 1.173, confidence interval [CI] 1.100−1.251, P<0.001) was a risk factor and the Hamilton Anxiety Scale (HAMA) (OR 0.862, CI 0.796−0.934, P<0.001), a protective factor against DVT progression.
Conclusion
VTE is not rare in patients with mental illnesses and is most commonly associated with organic mental disorders. Psychosis-related DVT typically shows a significantly high incidence of distal DVT. Prevention and early treatment in patients with severe depression and distal DVT can prevent DVT aggravation.
Introduction
Venous thromboembolism (VTE) is a common and potentially life-threatening condition. 1 Epidemiological studies have identified many risk factors associated with VTE, such as surgery and cancer, among others. 1 Several studies have reported a high prevalence of VTE (2.3%–25.3%) in hospitalized patients with mental illnesses.2–4 Some risk factors associated with VTE are secondary to the mental illness itself, and a few may be attributable to specific treatments, including antipsychotic and physical therapy. 5
Although previous studies have investigated VTE in patients with psychiatric conditions, limited research has focused on the anatomical distribution of VTE and on the association between thrombus distribution and psychiatric factors. The risk of pulmonary embolism (PE) and post-thrombosis syndrome and the overall prognosis vary depending on the affected venous territory. Knowledge of the distribution of deep venous thrombosis (DVT) is important for diagnosis, treatment, and prognosis. Further studies are warranted to clarify the current status of VTE in patients with psychiatric disorders.
In this retrospective study, we analyzed the clinical data of patients diagnosed with psychiatric illnesses and VTE to determine the incidence and clinical characteristics of this condition. This knowledge is important to create awareness among clinicians to closely monitor patients with psychiatric illnesses for the risk of VTE to facilitate prompt individualized prevention and treatment.
Patients and Methods
Patients
In this retrospective observational study, we investigated VTE incidence in 12939 inpatients diagnosed with mental illnesses at the Mental Health Center of the First Hospital of Hebei Medical University between August 2018 and July 2022. VTE was defined as DVT and/or PE and was diagnosed based on ultrasonography, computed tomography pulmonary angiography, and conventional venography. This study was approved by the Ethics Committee of the First Hospital of Hebei Medical University. Written informed consent was provided by all patients or their family members.
Methods
Patient data regarding psychosis and VTE were extracted from the hospital medical record system. Psychosis-related information included disease type, the Hamilton Anxiety Scale (HAMA) and Hamilton Depression Scale (HAMD), and treatments administered including restraint, artificial hibernation, antipsychotic, antidepressant, and electroconvulsive therapy (ECT). VTE-based information included thrombus distribution. We obtained demographic data regarding admission and investigated the approximate incidence of each mental illness and the clinical features of VTE, including VTE distribution in the left and right extremities and venous involvement. Based on the site of thrombosis, patients with VTE were categorized into proximal and distal DVT groups, and we performed intergroup comparison of characteristics and risk factors for mental illnesses. Patients with VTE were further categorized into PE and non-PE groups based on detection of PE. We also performed intergroup comparison of types of mental illnesses and mental disorder scores.
Definitions
Depending on the venous drainage territory, DVT can be classified as proximal or distal DVT. Thrombosis of the iliac, femoral, and/or popliteal veins was classified as proximal DVT, regardless of involvement of a deep vein of the calf. Thrombosis confined to the deep veins of the calf was classified as distal DVT. DVT classification was based on the European Society for Vascular Surgery 2021 Clinical Practice Guidelines on the Management of Venous Thrombosis. 6 Mental illnesses were classified based on the International Classification of Diseases, 10th Edition.
Statistical Analysis
The crude incidence rate of psychosis-related VTE was calculated by dividing the number of patients with VTE by the total number of patients with mental illnesses. Categorical variables are presented as numbers and percentages and continuous variables as the mean and standard deviation or medians and interquartile ranges, based on their distributions. The chi-square or Fisher's exact test was used to determine differences between various combinations. Univariate logistic regression analysis was used to confirm the potential risk factors for VTE progression. Factors specific to patients with psychiatric disorders7–10 were subjected to multivariate logistic regression analysis. Statistical analysis was performed using the SPSS software, version 26.0 (SPSS Inc., Chicago, IL, USA). P value <0.05 was considered statistically significant.
Results
Patient Characteristics
Of the 12939 patients with mental illnesses who visited our hospital between August 2018 and July 2022, 156 (1.21%) were diagnosed with VTE (Figure 1). Among the 12939 patients, the female-to-male ratio was 1.4:1.0. Compared with the non-VTE group, the VTE group included a greater number of women (67.30% vs. 58.32%, P = 0.0015) (Figure 2) and patients who were older at the time of diagnosis (median age 65 years vs. 36 years, P < 0.001) (Figure 3). The median body mass index (BMI) of patients was 23.60 (21.20–27.25) kg/m2. The most common comorbidities included hypertension (26.92%), stroke (14.10%), and diabetes (12.82%). In terms of hospitalization, there was no statistical difference in length of stay between the VTE and non-VTE groups (21 [13–30] day vs. 19 [13–27] day, P = 0.340). The VTE events occurred in 4 (2–7)day of hospitalization. Of the 156 patients with VTE, 93 were treated with anticoagulation and 52 were monitored for coagulation alone. Nine patients were treated with inferior vena cava filter placement combined with anticoagulation and one with inferior vena cava filter placement combined with embolectomy. All patients were discharged with no VTE-related deaths after treatment.

Flow chart of the study population.
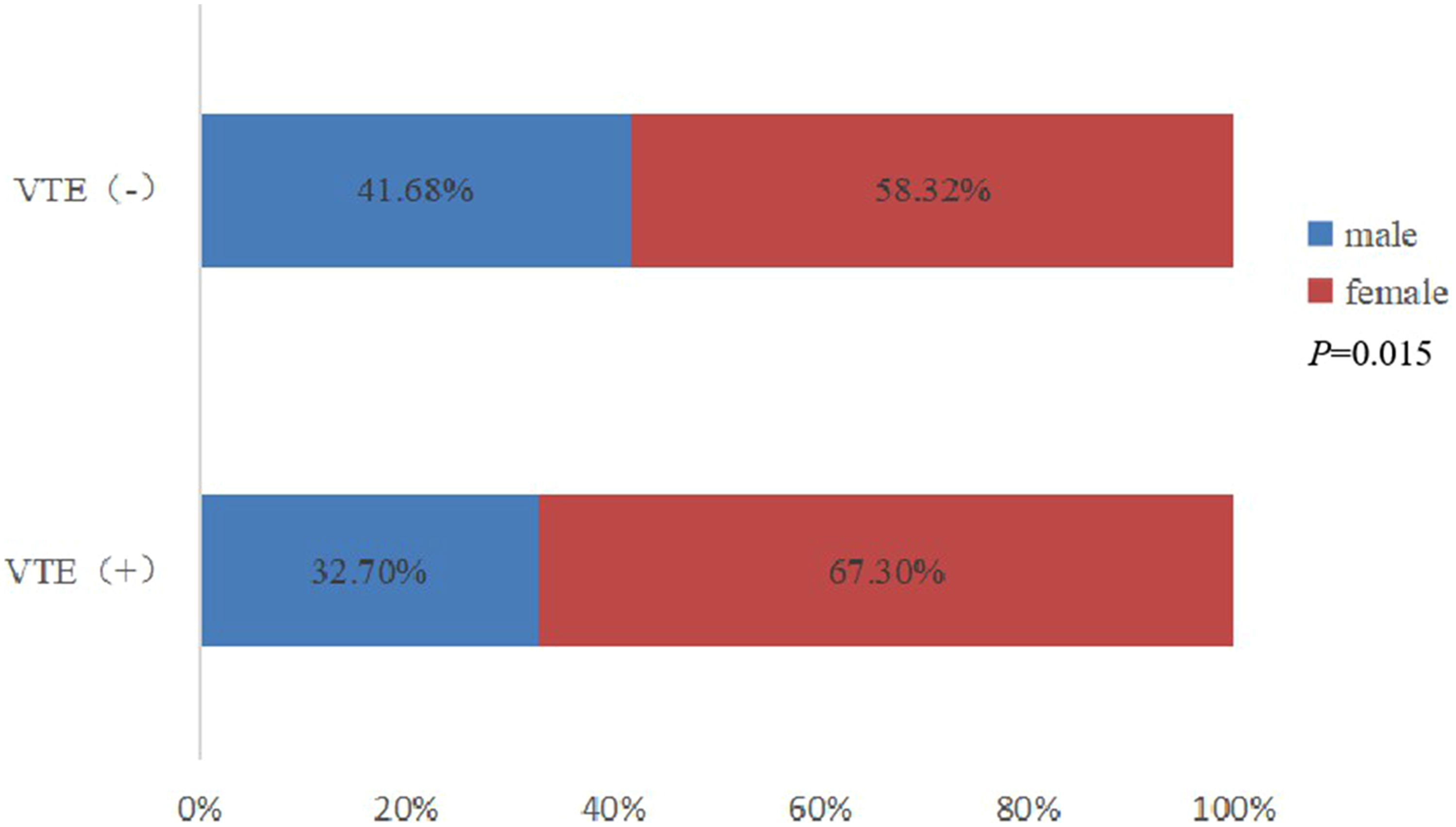
The gender of the study population.
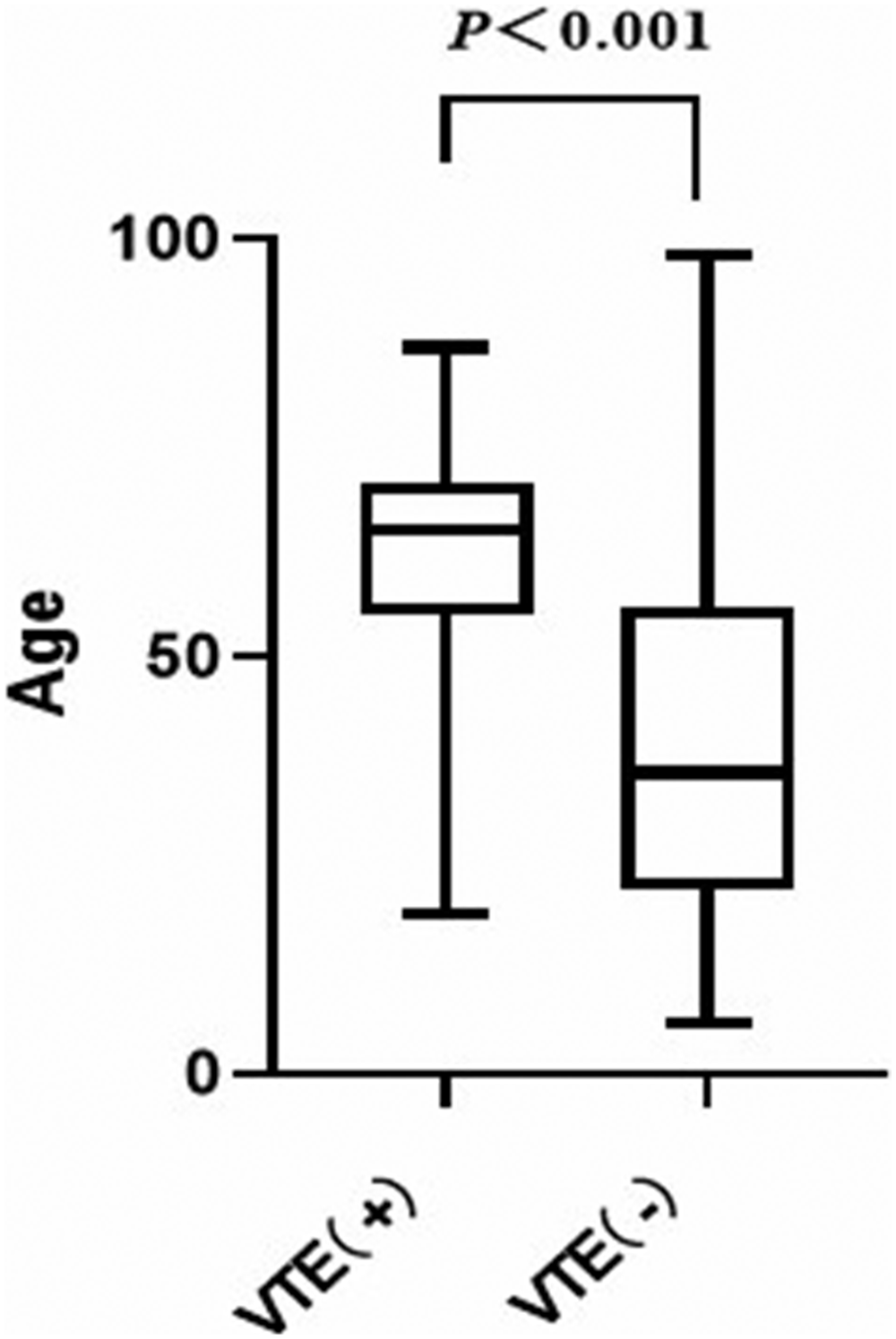
The age of the study population.
Clinical Features of Venous Thromboembolism
In this study, a total of 156 patients with mental illness were diagnosed with VTE after admission. We observed 123 DVT (78.85%) and 12 PE (7.69%) events, and 21 patients (13.46%) with simultaneous DVT and PE at the time of diagnosis (Figure 1). Of these DVT events, 41 (28.47%) were left-sided, 54 (37.50%) were right-sided, and 49 (34.03%) were bilateral in distribution (Figure 1). The ratio of involvement of the left and right lower extremities did not significantly differ between men and women (P = 0.295), between age groups (P = 0.479), BMI scores (P = 0.244), or between different types of mental illnesses (P = 0.286). Of the 144 DVT events, 79.17% were classified as distal DVT and 20.84% as proximal DVT. We identified 144 DVT events in the lower extremities of 198 patients and 151 lower extremities (76.26%) with a single vein segment of DVT; the muscle calf vein (MCV) was involved in 87.42%, followed by the posterior tibial vein (PTV) in 6.62%. At least two vein segments were involved in 47 lower extremities (23.74%), among which the superficial femoral vein(SFV) and popliteal vein(PV), the MCV and PTV were most commonly involved (Table 1).
Involvement of Lower Extremity Deep Veins in Patients with Mental Illness.
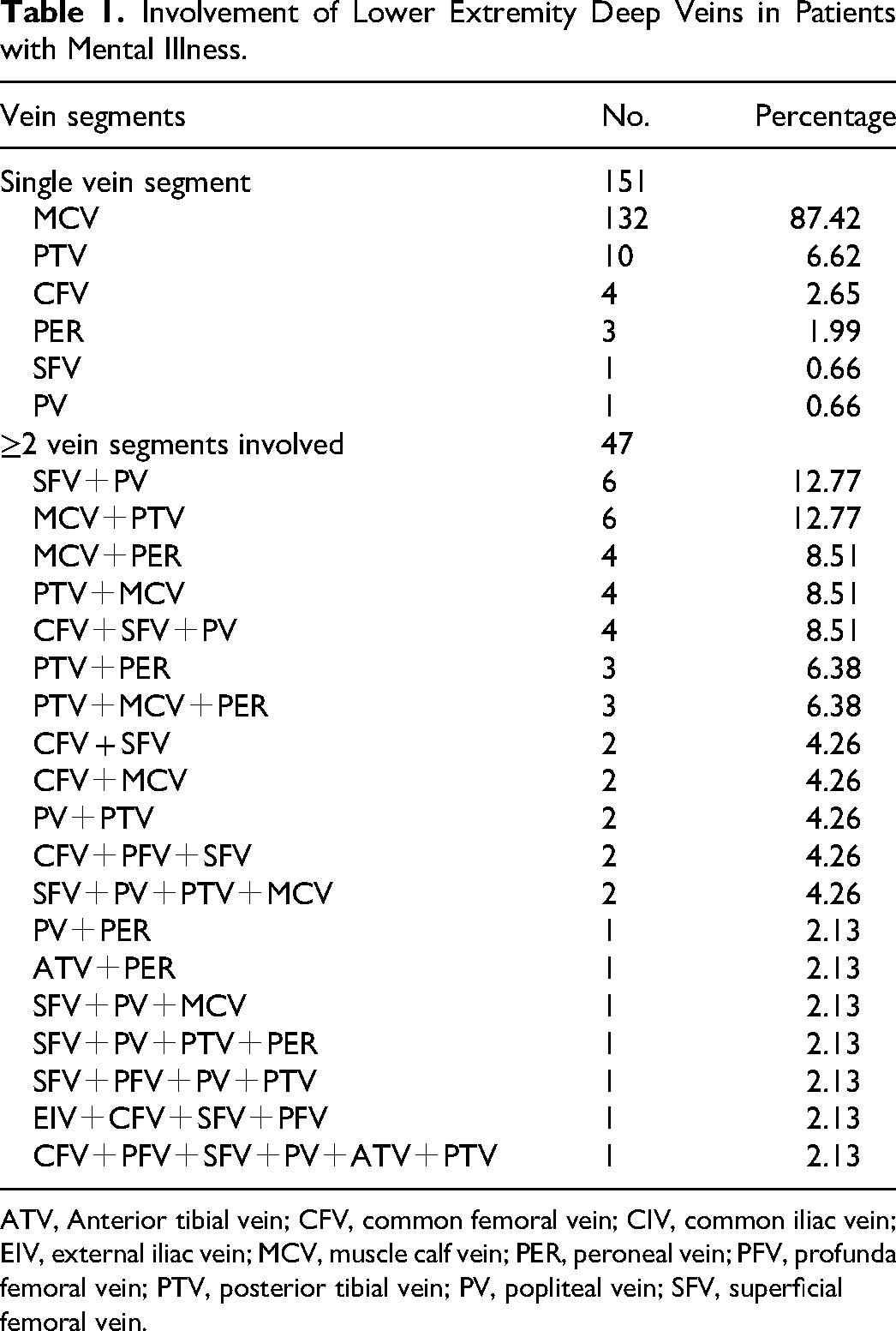
ATV, Anterior tibial vein; CFV, common femoral vein; CIV, common iliac vein; EIV, external iliac vein; MCV, muscle calf vein; PER, peroneal vein; PFV, profunda femoral vein; PTV, posterior tibial vein; PV, popliteal vein; SFV, superficial femoral vein.
Characteristics and Risk Factors of Mental Illnesses Associated with Venous Thromboembolism
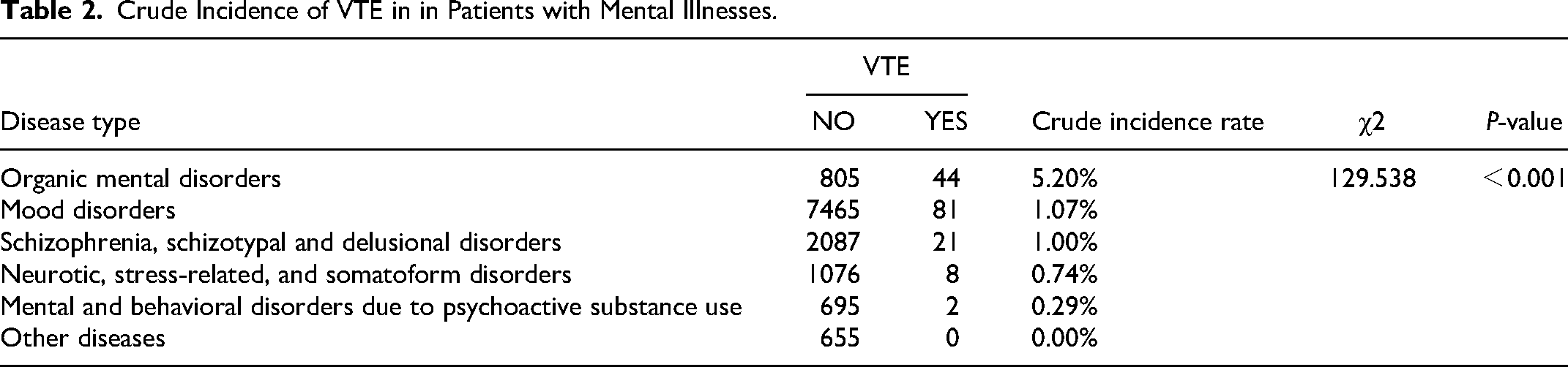
VTE occurred in 1.20% (156/12939) of all patients; however, the crude incidence rate differed across mental illnesses as follows: organic mental disorders (44/849, 5.20%), mood disorders (81/7546, 1.07%), schizophrenia, schizotypal and delusional disorders (21/2108, 1.00%), neurotic, stress-induced, and somatoform disorders (8/1084, 0.74%), and mental and behavioral health disorders secondary to psychoactive substance use (2/697, 0.29%) (P < 0.001) (Table 2).
Crude Incidence of VTE in in Patients with Mental Illnesses.
Based on HAMA score, 19.23% of patients with VTE had moderate-severe and 30.77% had severe anxiety. With regard to HAMD score, 36.54% of patients had moderate and 45.51% had severe depression (Figure 4).

A, The proportion of HAMA. B, The proportion of HAMD.
The HAMD score was significantly higher in patients with proximal than in those with distal DVT (40 [33–52] points vs. 28 [20–40] points, P<0.001) (Figure 5). The HAMA score did not significantly differ between patients with proximal and distal DVT (P = 0.888). The HAMD score was identified as a risk factor for progression of distal to proximal DVT on univariate (odds ratio [OR] 1.069, confidence interval [CI] 1.035−1.105, P<0.001) (Figure 6) and multivariate analyses (OR 1.173, CI 1.100−1.251 P<0.001) (Table 3). Multivariate analysis showed that HAMA (OR 0.862, CI 0.796−0.934, P<0.001) served as a protective factor against DVT progression (Table 3). Compared with the non-PE group, we observed no significant differences in the HAMA and HAMD and various mental illnesses in the PE group.

HAMD of proximal and distal DVT patients.

Risk factors for progression of distal to proximal DVT by univariate analysis.
Risk Factors for Progression of Distal to Proximal DVT by Multivariate Logistic Regression Analysis.

Discussion
This study investigated the characteristics of VTE in patients with mental illnesses. The incidence of psychosis-related VTE in the present study was slightly lower than that reported by previous studies (1.2% vs. 2.3%–25.3%). Results may have been inaccurate owing to the small sample sizes of previous studies or may be attributable to the fact that some patients with psychiatric disorders were asymptomatic. Some symptoms of VTE may have been misdiagnosed or missed because patients with mental disorders may not accurately describe the presentation of VTE. Similarly, physicians may also attribute physical complaints to anxiety disorders or mental illnesses. Therefore, the potential incidence was higher than the actual incidence of VTE.
Patients with psychosis and concomitant VTE were older than those without psychosis. Advanced age is a well-known risk factor for VTE. 11 Compared with men, women showed a significant increase in the incidence of VTE. Previous studies have reported conflicting results regarding the risk of the first VTE event in men and women. Hwang et al. 12 observed a 1.29-fold higher incidence of VTE in Korean women than men. Elderly women show greater predisposition to thrombosis than men. Women have typical risk factors for VTE, including oral contraceptive use, hormone replacement therapy, and pregnancy, all of which increase their risk of VTE.13–15 In contrast, some studies have reported no sex-based differences in VTE incidence.16–18 However, a cohort study also observed an increased risk of the first VTE event in men compared with women. 19 The results of these studies are difficult to interpret owing to differences in methods used and insufficient sample sizes to allow separate investigation of men and women, which may be associated with the inclusion of male and female populations. Among all patients with mental disorders included in this paper, the proportion of women is higher. Based on this data, it can be explained that the incidence of VTE is also higher in women. In addition, we speculate that the risk of VTE in women may also be related to the following factors: (a) Early and late menopause may be newly discovered risk factors for VTE in postmenopausal women, followed by the use of hormone replacement therapy in menopausal women with more severe symptoms, which therefore increases the risk of VTE.20,21 (b) Prenatal and perinatal factors are also associated with the onset of psychosis. 22 Physiological factors and emotional stress may act synergistically to precipitate VTE. Further studies are required to investigate the association between hormonal changes in psychosis and VTE.
The MCV was the most commonly affected vessel. Qiu et al. 23 investigated 1431 patients with hospital-acquired lower-extremity DVT and observed that the MCV was the most common site of thrombosis, which is consistent with the results of previous studies and indicates that this site is the most likely source of DVT. Currently, the clinical significance and optimal treatment of isolated calf deep vein thrombosis (C-DVT) remain controversial. Research on the natural history of isolated C-DVT has shown that 25%–33% of symptomatic C-DVT spreads to the proximal vein. 24 Isolated C-DVT is also associated with a high prevalence of PE in hospitalized patients. Therefore, the MCV requires close monitoring. 25
Patients with severe mental illnesses often require ECT; therefore, proximal DVT requires attention in these patients. Some experts are of the view that strong muscle contractions during ECT increase the risk of PE. 8 The consensus is withdrawal of ECT and continuation of anticoagulation in patients with proximal DVT with reintroduction of ECT only after DVT resolution. 26 Patients with PE require close attention. PE is pathologically characterized by a severe imbalance in the lung ventilation/perfusion ratio and hypoxia or hypoxemia, which leads to cerebral hypoxia. Previous clinical and animal studies have shown an increased risk of mood disorders, anxiety disorders, and dementia in hypoxia-induced conditions, such as obstructive sleep apnea syndrome and chronic obstructive pulmonary disease.27–29 Cerebral hypoxia triggers a series of reactions in the inflammatory factor cascade, which eventually lead to neurodegenerative diseases. 30 Patients with psychiatric disorders are invariably predisposed to PE, which may consequently aggravate pre-existing mental illnesses; therefore, early detection and prompt treatment of PE is important.
The overall crude incidence rate (high to low) differed across diseases as follows: organic mental disorders, mood disorders, schizophrenia, schizotypal and delusional disorders, mental and behavioral health disorders secondary to psychoactive substance use, and neurotic, stress-related, and somatoform disorders. Some studies have reported that patients with schizophrenia, bipolar disorder, catatonia, depressive disorder, post-traumatic stress disorder, or neuroleptic malignant syndrome are predisposed to VTE.31–33 Mood changes may increase blood levels of circulating procoagulant markers and result in a hypercoagulable state. Obesity, antipsychotic drug use, restraint therapy, and sedation among other interventions increase the risk of VTE. Notably, organic mental disorders showed the highest incidence rate in this study. Organic mental disorders refer to mental illnesses that occur secondary to brain or physical diseases and primarily including delirium and Alzheimer's disease, among others. Among 849 patients diagnosed with organic mental disorders, 44 (5.20%) showed complications of VTE, including delirium (n = 3), dementia (n = 5), epilepsy (n = 3), Alzheimer's disease (n = 6), demyelination (n = 1), dementia with Lewy bodies (n = 1), and vascular cognitive impairment (n = 25). In contrast to other mental illnesses, organic mental disorders involve not only functional changes but also organic injury. With regard to the association between organic mental disorders and VTE, the authors of a prospective study observed that VTE prevalence was particularly high (approximately 10.0%) in older patients diagnosed with dementia. 34 However, studies have not investigated other mental disorders in this context. In this study, we observed vascular cognitive impairment, represented by evidence of previous cerebral infarction. Further studies are necessary to investigate the association between organic brain injury and VTE in addition to the aforementioned risk factors associated with VTE.
HAMD and HAMA, developed by Hamilton in the 1960s are simple with clear evaluation criteria and user friendly; therefore, these scales are widely used in clinical practice to evaluate the severity of mental disorders. In the present study, the HAMD scores were higher in the proximal than in the distal DVT group, which indicates higher levels of depression in the proximal DVT group. With regard to the association between psychiatric rating scales and VTE, Von Känel et al 35 investigated 271 patients with VTE and observed that an increase of three points in the Hospital Anxiety and Depression Scale increased the risk of VTE recurrence by 44.0%. In our study, a high HAMD score was identified as a risk factor for VTE progression; this phenomenon may be attributable to the following underlying mechanisms: (A) Depressed mood is invariably clinically accompanied by “catatonia,” which typically manifests with immobility. Long-term immobility favors blood stasis, which further aggravates thrombosis and spread. 2 (B) Severe depression is accompanied by hemodynamic changes that lead to hyperviscosity of blood, reflected by increased hematocrit, plasma viscosity, and whole blood high shear viscosity, and whole blood low shear viscosity among other such features.36,37 Furthermore, activation of the coagulation cascade accompanied by increased thromboxane A2 and fibrinogen levels and enhanced platelet aggregation lead to a hypercoagulable state. 38 In contrast, HAMA was negatively correlated with DVT progression, which may be attributable to the fact that patients with severe anxiety are more likely to be nervous, hyperactive, and in a state of panic; therefore, compared with depressed patients, these patients show more physical movements and not prolonged immobility (and are therefore not predisposed to blood stasis and aggravation of thrombosis).
Previous studies have reported that physical restraint causes blood flow stasis, which in turn may contribute to the formation of VTE. Naoki Hirose found that 13.2% of psychiatric patients with VTE experienced at least 1 day of physical restraint. 39 Funayama et al. 40 divided 1308 psychiatric inpatients into two groups: a physical restraint group and a non-physical restraint group. The study found that physical restraint significantly increased the risk of DVT through controlled experimental studies in groups. No significant association between restraint and thrombosis has also been reported in the literature, but in this study, a prophylactic dose of low molecular heparin was administered daily to patients subjected to physical restraint for thromboprophylaxis. 41 Hans Hilger, on the other hand, concluded that in psychiatric patients who are restrained for less than 24 h, measures to prevent VTE in physically restrained psychiatric patients do not seem necessary. 42 In the present study, restraint was not a risk for progression of distal DVT. First, none of the psychiatric patients who were restrained had been restrained for more than 24 h and were loosened for 10 min at half-hour intervals. Even patients who were severely agitated were taken to an isolation room for unrestraint. Secondly, most of the patients who were restrained were manic patients who were at risk of aggression and violence and would have made small movements even when restrained and would not have become an absolutely stationary state. Third, we are a cross-sectional study and the evidence is not strong and better studies are needed to explore it in the future.
Following are the limitations of this study: (i) The retrospective design of this population-based study is a drawback. (ii) The study included patients with all types of mental illnesses, without any exclusion criteria; therefore, we could not accurately determine the causal association between mental illnesses and VTE. (iii) Risk factors for VTE development in the overall population of patients with psychiatric disorders were not investigated in this study. (iv) All patients do not routinely undergo lower extremity venous ultrasonographic screening. Therefore, the incidence of VTE may have been underestimated. VTE is asymptomatic or not fatal even in patients in whom this diagnosis is missed. Although this study lacks absolute rigor, our results can serve as guidelines to create greater awareness among clinicians regarding the importance of VTE monitoring in patients with psychiatric disorders.
Conclusion
This study highlights that VTE was not uncommon in patients with mental illnesses. We observed the highest percentage of VTE events in patients with organic mental disorders and a significantly high rate of distal DVT in patients with mental illnesses and that HAMD is a risk factor for DVT progression. Patients with severe depression and distal DVT merit special attention for careful evaluation and close monitoring of VTE to enable initiation of optimal preventive measures after considering the risk-benefit ratio of the intervention. However, further prospective studies are warranted to confirm the association between thrombosis and psychosis to develop clinical guidelines for optimal management of these patients.
Footnotes
Acknowledgements
We thank all the doctors, nurses, and students who participated in this study during these years.
Ethics Approval
Ethical approval for this study was obtained from the Medical Ethics Committee of the First Hospital of Hebei Medical University (20220666).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants No. 20160680 from the Key Project of Medical Science Research of Hebei Province and No. 20230169 from the Scientific Research Funding of Hebei Provincial Health Commission.