
Abstract
Objective
Investigations on coagulation parameters including fibrinogen (Fbg), fibrinogen degradation products (FDP), and D-dimer in ischemic stroke patients treated with intravenous thrombolysis are insufficient. We aimed to investigate the association between in-hospital clinical outcomes and the coagulation parameters at different time points in ischemic stroke patients treated with intravenous tissues plasminogen activator (IV tPA).
Methods
We retrospectively enrolled patients who received IV tPA therapy within 4.5 h from symptoms onset. Demographics, clinical characteristics, imaging measures, and the discharge mRS score were collected. Multivariable logistic regression analyses were performed to test whether coagulation parameters were independent predictors for the in-hospital clinical outcomes. We also employed machine learning models to investigate whether coagulation parameters were able to improve the prediction of favorable functional outcomes.
Results
One hundred and fifty-two patients treated with IV tPA were included. Among the coagulation parameters, low D-dimers at 48 h proved to be an independent predictor of favorable functional outcome (adjusted odd ratio 0.24, 95% confidential intervals 0.06-0.92, P = 0.04). The AUC of D-dimer at 48 h to predict favorable functional outcome was 0.73 (0.60-0.87) and the optimal cut-off value was 0.92 (sensitivity 0.69, specificity 0.78). Machine learning models with D-dimer at 48 h had superior performance in predicting favorable functional outcomes and among the input variables in the machine learning models, D-dimer at 48 h showed the highest weight in predicting mRS 0-1 at discharge (38.44%).
Conclusion
Increased levels of D-dimer at 48 h was associated with lower proportion of favorable functional outcomes in acute ischemic stroke patients with intravenous thrombolysis.
Introduction
Stroke is a major cause of disability and death in the world and ranked third among the top 10 causes of disability-adjusted life-years in 2019. 1 Intravenous thrombolysis with recombinant tissue plasminogen activator (IV tPA) has been proposed as a standard of care efficacy to achieve recanalization and improve functional outcomes for ischemic stroke patients.2,3 However, in the real-world, about 40% of the ischemic stroke patients that received IV tPA therapy within 4.5 h failed to achieve favorable functional outcomes at 90-day.4,5
Coagulation cascades play a vital role in the process of onset and recovery of ischemic stroke.6–8 Some parameters related to the coagulation cascades have been identified as predictors of the prognosis for patients with ischemic stroke including fibrinogen 9 and D-dimer. 10 In patients treated with IV tPA, coagulation parameters including fibrinogen11,12 and D-dimer 13 were also reported to be related to the prognosis for ischemic stroke. However, as most studies8,11–13 only investigated the clinical significance of one coagulation parameter at one or two time points, still much is unknown on variation trends of the coagulation parameters before and after IV tPA, and their association with prognosis of patients treated with IV tPA.
In this study, we aimed to delineate the variation trends of coagulation parameters at different time points and investigate the predictors for clinical outcome in patients treated with IV tPA. Moreover, we established 5 machine learning models and calculated the diagnostic values among the 5 machine learning models after adding coagulation parameters to test their predictive capability in patients treated with IV tPA.
Methods
Study Design
We conducted a retrospective cohort study based on a database of the patients treated with IV tPA at Beijing Tiantan Hospital. Ethical approval has been obtained from the ethics committee of Beijing Tiantan Hospital (No.: KY2019-019- 05). The Local institutional review board permitted the waiver of informed consent of our study considering its retrospective study design and de-indentification of the patient data.
Participants
Patients treated with IV tPA at our emergency department (ED) from October first, 2018 to November fifth, 2020 were screened for eligibility and enrolled if they met the following inclusion criteria: 1) diagnosed with ischemic stroke at the ED (focal neurological signs or symptoms due to vascular etiology and confirmed by brain CT); 2) treated with 0.9 mg/kg alteplase within 4.5 h from stroke onset. We excluded patients 1) with incomplete data on coagulation tests; 2) without mRS score at discharge; 3) receiving anticoagulation agents within 24 h before IV tPA and 4) post-tPA MRI scan and other in-hospital imaging or laboratory tests implying stroke mimics or non-vascular disease.
Data Collection
A neurological physician (L.G.) collected the clinical, imaging, and laboratory data blinded to the discharge mRS score. The clinical data included demographic information (age, sex), medical history (hypertension, diabetes, hyperlipidemia, atrial fibrillation, prior stroke, etc), alcohol intake / smoking status, medication history (prior antiplatelet therapy of oral aspirin / clopidogrel), and time delay before IV tPA (onset-to-needle time and door-to-needle time). Neurological impairment severity was assessed by the National Institute of Health Stroke Scale (NIHSS) score. 14 Etiology of ischemic stroke was classified according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification. 15 Symptomatic intracerebral hemorrhage was categorized according to the NINDS criteria. 16 White matter hyperintensities severity was evaluated using the Fazekas scale. 17 We recorded periventricular and deep white matter hyperintensities separately, then the highest score for white matter hyperintensities were recorded as the score of Fazekas scale. Large vessel occlusion was identified through magnetic resonance angiography after tPA. Considering that some thrombosis events after ischemic stroke onset could be related to the coagulation parameters and clinical outcomes, we also recorded the number (proportion) of in-hospital thrombosis events including deep vein thrombosis, muscular calf vein thrombosis and pulmonary embolism.
Peripheral blood samples were collected at 4 time points (0 h, defined as the time point before the initiation of IV tPA; 24 h, defined as 24 ± 3 h after IV tPA; 48 h, defined as 48 ± 3 h after IV tPA; and at discharge) for analyzing coagulation parameters including fibrinogen (Fbg), fibrinogen degradation products (FDP) and D-dimer. Blood samples were collected in 5 mL evacuated tubes using one-tenth of 0.129 mol/L saline sodium citrate as an anticoagulant and analyzed photo-optically using an ALC-Top coagulometer.
Outcome Evaluation
The study outcome was favorable functional outcome, defined the modified Rankin Scale (mRS) score 0-1 at discharge. The mRS score is widely used to assess the independent status ranging from 0 to 6 and a higher mRS score indicated poorer independent status.
Statistical Analysis
For continuous variables, normally distributed data were displayed as mean ± SD and compared using the student t test while non-normally distributed data were displayed as median (interquartile range) and compared using Mann–Whitney U test. Shapiro test was used to test data distribution. Categorical variables were displayed as number (percentage) and compared using the χ2 test or Fisher's exact test, as appropriate. Boxplots were used to delineate the variation trends of the coagulation parameters with Wilcoxon tests tested the statistical significance of the change values between different time points. Multivariable logistics regression analyses were conducted to find out the independent predictors of favorable functional outcome among the coagulation parameters at different time points. Considering the potential collinearity among the different coagulation parameters at different time points, we conducted multivariable logistics regression analyses using the backward stepwise method. Subsequent receiver operating characteristic (ROC) curves were used to assess the predictive capability and determine the optimal cut-off value of the predictive coagulation parameters. All statistical analyses were performed with the SPSS 25.0. P <0.05 was considered statistically significant.
We established 5 machine learning models to predict favorable functional outcome and calculated the change value of the diagnostic ability before and after adding the coagulation parameters. The 5 machine learning models included the traditional linear model, k-Nearest Neighbor (kNN) model, multilayer perceptron (mlp) model, random forest (rfc) model, and extreme gradient boosting (XGBoost) model. The mlp model, also known as a deep neural network model, was an automated feedforward architecture model with 3 hidden layers, 50 epochs, and mini-batch training. One consecutive step with no further decrease in the error term was the stopping criterion. The rfc model consisted of a multitude of 100 decision trees comprising multiple true or false conditions using input variables. The sum of the decisions made by the decision trees was used for the final classification. The rfc model was also employed to compute the importance of the input variables. Input variables were 7 acknowledged factors related to functional outcomes of ischemic stroke including bridging mechanical thrombectomy (MT), admission NIHSS score, history of hypertension, smoking, alcohol intake, large vessel occlusion and sICH. Continuous variables were standardized to distribution from 0 to 1 before training the 5 models. We trained all of the 5 machine learning models with all of the 7 variables as inputs to classify patients likely to have favorable outcomes (mRS 0-1 at discharge). Before training the machine learning models, we divided the included patients into a training cohort (70%, to establish and train the models) and a test cohort (30%, to test the predictive capability). ROC curves with area under curve (AUC) were used to show and compare the predictive capability of the machine models. P value < 0.05 indicated that the coagulation parameter added to the model could enhance the predictive capability significantly. All of the machine models and related ROC curves were performed using Python 3.6 (Python Software Foundation, Beaverton, OR,USA; https://www.python.org/).
Results
From October first, 2018 to November fifth, 2020, a total of 595 patients treated with IV tPA at Beijing Tiantan Hospital were screened for eligibility, and 158 of them had complete data on coagulation tests at 4 time points including at 0 h of IV tPA, 24 h after IV tPA, 48 h after IV tPA, and at discharge. Among the patients that had complete data of coagulation tests, 5 patients were excluded for missing data on mRS score at discharge, and 1 patient was excluded for having anticoagulation agents within 24 h before IV tPA. Baseline comparisons between included and excluded patients were summarized in the Supplemental materials. The included patients tended to have a worse clinical status (more comorbidity and higher admission NIHSS score), a higher proportion of MT and be less likely to achieve favorable functional outcome at discharge. In the final study, 152 patients were included with an average age of 63.75 ± 12.60 and 72.37% (110/152) of them were male. The median time interval from onset to needle was 170 (133.75-228.25) minutes. 21.71% (33/152) of patients received bridging MT after IV tPA. The median admission NIHSS score was 8 (4-11.25).
Dynamic Changes at Different Time Points
The dynamic changes of FDP, D-dimer, and Fbg at different time points were displayed in

Boxplots to show dynamic change trends of FDP (a), D-dimer (b) and Fbg(c).
Relationship Between Coagulation Parameters and Functional Outcome
Comparison of baseline information between mRS 0-1 and mRS 2-6 at discharge was summarized in
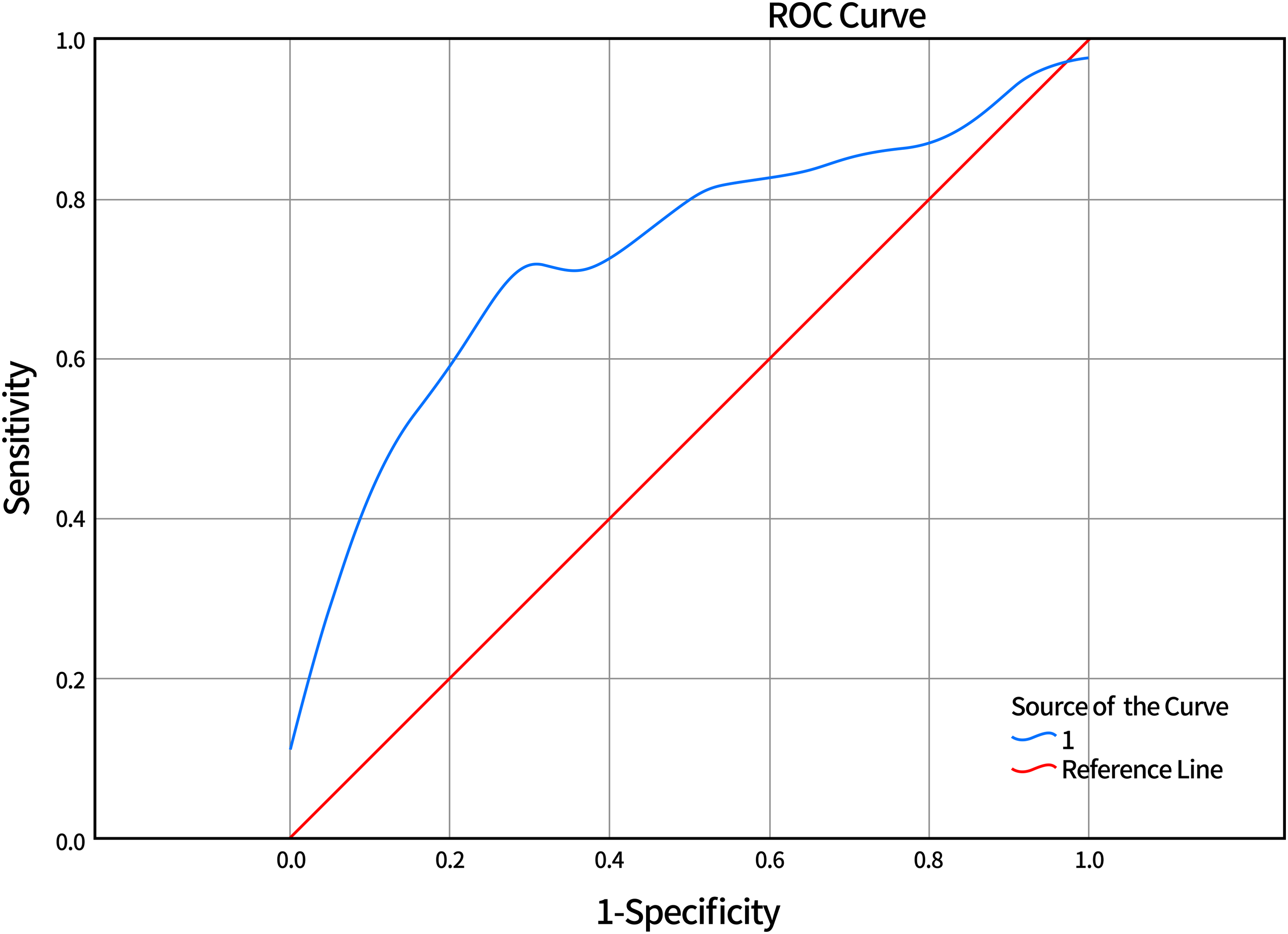
Receiver operating characteristic curves D-dimer at 48 h.
Baseline Characteristics Between mRS 2-6 and mRS 0-1 Group in Patients Treated with IV tPA

DNT, door-to-needle; IV, intravenous thrombolysis; tPA, tissue plasminogen activator; mRS, modified Rankin Scale; NIHSS, national institutes of health stroke scale; TOAST, Trial of Org 10172 in Acute Stroke Treatment; LAA, large atherosclerosis artery; CE, cardiac embolism; SAA, small artery occlusion; SBP, systolic blood pressure; DBP, diastolic blood pressure; FDP, fibrinogen degradation products; Fbg, fibrinogen; MCA, middle cerebral artery; sICH, symptomatic intracerebral hemorrhage;
Machine Learning Models with D-Dimer at 48 h
Based on 8 traditional factors related to functional outcomes of ischemic stroke as input variables (MT, admission NIHSS score, history of hypertension, smoking, alcohol intake, large vessel occlusion and sICH), we employed 5 machine learning models (traditional linear model, kNN model, mlp model, rfc model and XGBoost model). As shown in
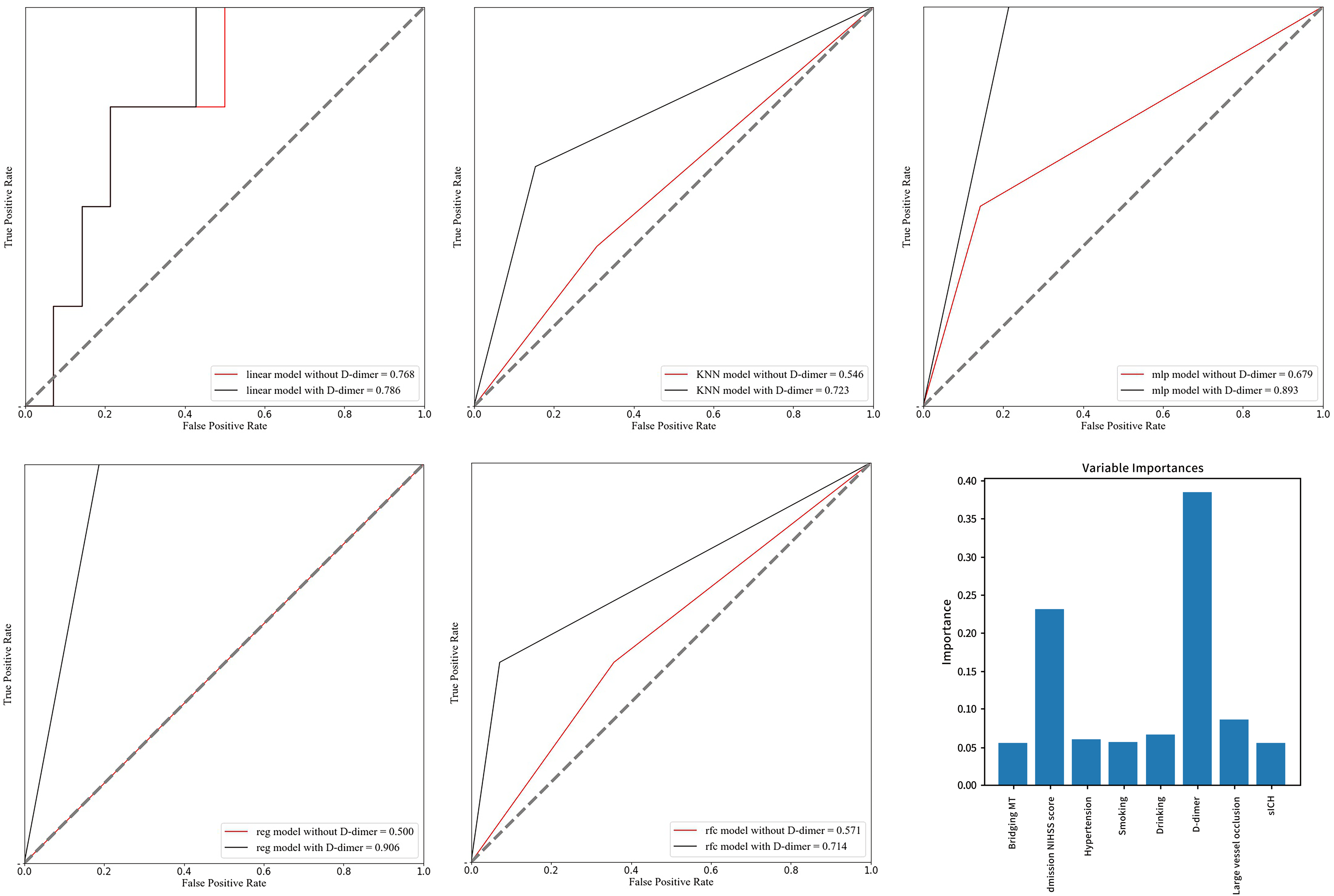
Receiver operating characteristic curves of different machine learning models: (a) traditional linear model; (b) K-Nearest Neighbor (kNN) model; (c) multilayer perceptron (mlp) model; (d) extreme gradient boosting (XGBoost) model; (e) random forest (rfc) model
Discussion
In our study, D-dimer at 48 h was suggested to be an independent predictor for favorable functional outcome at discharge in patients treated with IV tPA among the 3 coagulation parameters (Fbg, FDP and D-dimer). The optimal cut-off value was 0.92 μg/ml and the addition of D-dimer at 48 h to machine learning models was benefit to enhance the predictive ability of favorable functional outcome at discharge. Our study investigated 3 different coagulation parameters in one study cohort and delineated the variation trends at 4 time points. Moreover, we utilized 5 machine learning models with ROC curves to demonstrate that D-dimer at 48 h significantly enhanced the predictive capability.
Our study found different dynamic change trends among the coagulation parameters. FDP and D-dimer level increased from baseline (0 h) to 24 h and Fbg level decreased from baseline to 24 h. In the coagulation cascades, the activated protease thrombin converts Fbg to fibrin and forms the cross-linked fibrin skeleton of a thrombus. Once the thrombus formation occurs, the fibrinolytic system is activated and tPA converts plasminogen to plasmin. Activated plasmin breaks down fibrin on the thrombus into FDP and forms D-dimer. Hence, thrombosis and subsequent fibrinolytic events deplete Fbg and produce a large amount of FDP as well as D-dimer, indicating decreased Fbg level but elevated FDP and D-dimer level after ischemic stroke onset. Considering that IV tPA (alteplase) therapy complements endogenous tPA and accelerates the fibrinolytic process, these inverse trends should also be observed in patients treated with IV tPA, as shown in our study. Shi J. et al also reported a decrease of 0.1 g/L Fbg from baseline to 24 h in a cohort of 364 patients treated with IV tPA. 11 A meta-analysis enrolling 2901 patients confirmed that patients with ischemic stroke had elevated level of D-dimer compared with patients with stroke mimics/controls. 18 This high level of D-dimer could persist as long as 3 months after stroke onset.19,20
Our study found that D-dimer level at 48 h was associated with functional outcomes and patients with lower D-dimer level at 48 h tended to have favorable functional outcome. The restricted cubic spline showed the odd ratio of D-dimer to predict favorable functional outcome was not higher than 1 among the different D-dimer levels, indicating that D-dimer was always a disruptive marker of functional outcome in ischemic stroke (

The restricted cubic spline showed the odd ratio of D-dimer to predict favorable functional outcome was not higher than 1 among the different D-dimer level.
All 5 machine learning models showed that the addition of D-dimer was beneficial for enhancing the predictive ability, and the rfc model also demonstrated its importance. After the addition of D-dimer, the AUC of the mlp and XGBoost models in the test group was close to 90%. Artificial intelligence tools including machine learning models have become more and more widely used in the field of clinical studies. Several studies employed different machine learning models and demonstrated their superiority in predicting clinical outcomes of ischemic stroke compared with traditional prediction scales and other statistical methods.30–32 Lehmann ALCF et al employed neural network models to separate non-survivors from survivors using coagulation parameters and other biomarkers and conducted an optimal model with an AUC of 0.975, demonstrating the predictive value of coagulation parameters and outstanding performance of machine learning models. 33 Neurol network models contain multiple layers of complex network and may be suitable for processing complex data with variables predicting clinical outcomes of ischemic stroke. 30 However, due to the limited sample size in our study, the AUC of the mlp model failed to show a statistically significant increase (P < 0.05) after adding D-dimer, even a great increase in AUC was observed. In a Korean stroke database enrolling over 6000 patients, an increase of 0.01 in AUC showed significant differences among different machine learning models. 34
Several limitations have to be acknowledged in our study. First, the included patients were derived from a single stroke center rather than a multi-center registry, indicating potential selection or observational bias that could weaken the external validation. However, different investigators collected the data on mRS score at discharge and other study data independently to minimize the bias. Considering different laboratory machines, reagents, and blood routine test kits, additional biases may arise in multicenter cohort studies. Secondly, the sample size of our study may not be that large because our study focused on the relationship between coagulation parameters and clinical outcome only in patients treated with IV tPA and only included patients with complete data on coagulation tests. In the future, a large-scale, prospective study is required to further investigate the relationship between coagulation parameters and clinical outcomes as well as the validation of the machine learning models. Third, 90-day mRS score was not obtained in our study. In the clinical practice, the COVID-19 pandemic and population mobility in Beijing, the capital of China, made face-to-face follow-up difficult to achieve. Besides, discharge mRS was also reported to be similar and a predictor of 90-d mRS.35–37 Fourth, large vessel occlusion was assessed by MRA within 24 h after IV tPA. In the real-world, only non-contrast CT scan was required before the injection of tPA to reduce the time delay. It is difficult to assess whether the patients were accompanied with vessel occlusion before tPA injection. Hence, in this study, we could only assess the proportion of large vessel occlusion using MRA after tPA injection. A minority of patients might manifest without vessel occlusion due to the recanalization of tPA and this study might report a lower proportion considering some patients. However, considering that the recanalization rate of tPA was low in patients with large vessel occlusion, 38 this bias may be limited.
Conclusion
D-dimer at 48 h can be serve as an important biomarker for functional outcome at discharge in acute ischemic stroke patients after IV tPA.
Supplemental Material
sj-docx-1-cat-10.1177_10760296221121287 - Supplemental material for Clinical Significance and Dynamic Change of Coagulation Parameters in Ischemic Stroke Patients Treated with Intravenous Thrombolysis
Supplemental material, sj-docx-1-cat-10.1177_10760296221121287 for Clinical Significance and Dynamic Change of Coagulation Parameters in Ischemic Stroke Patients Treated with Intravenous Thrombolysis by Guangshuo Li, Chuanying Wang, Shang Wang, Yahui Hao, Yunyun Xiong and Xingquan Zhao in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Author Contributions
G.L., Y.X. and X.Z. contributed to the conception and design of the study; G.L., C.W., S.W. and Y.H. contributed to the acquisition and analysis of data; G.L. and Y.X. contributed to drafting the text and preparing the figures.
Acknowledgements
None.
Ethics Approval and Consent to Participate
The study was approved by the ethics committee of Beijing Tiantan Hospital (No.: KY2019-019- 06). The fully dei-dentified data on the patients enrolled in the current study and its retrospective study design enables this study conducted under a waiver of informed consent by the local institutional review board of Beijing Tiantan Hospital. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for Publication
Not applicable. No information or images that could lead to identification of a study participant was mentioned in our study.
Availability of Data and Materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by grants from Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2019-I2M-5-029), the National Natural Science Foundation (82171272), Beijing Municipal Science & Technology Commission (Z211100003521019), Beijing Hospitals Authority (PX2022019), Ministry of Finance of the People's Republic of China [issued by Finance and Social Security [2015] Document No. 82; [2016] Document No. 50; [2017] Document No. 72; [2018] Document No. 48; [2019] Document No. 77; [2020] Document No. 75; [2021] Document No. 84, Ministry of Finance], Beijing Hospitals Authority Innovation Studio of Young Staff Funding Support, code: 202112,.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.