
Abstract
Pulmonary embolism (PE) patients have an increased prevalence and incidence of atrial fibrillation (AF). Because comorbid AF increases risk of morbidity and mortality, we sought to investigate the role of thrombo-inflammatory biomarkers in risk stratifying patients who experience an acute PE episode. Study participants were enrolled from a Pulmonary Embolism Response Team (PERT) registry between March 2016 and March 2019 at Loyola University Medical Center and Gottlieb Memorial Hospital. This cohort was divided into 3 groups: PE patients with a prior diagnosis of AF (n = 8), PE patients with a subsequent diagnosis of AF (n = 11), and PE patients who do not develop AF (n = 71). D-Dimer, CRP, PAI-1, TAFIa, FXIIIa, A2A, MP, and TFPI were profiled using the ELISA method. All biomarkers were significantly different between controls and PE patients (P < 0.05). Furthermore, TFPI was significantly elevated in PE patients who subsequently developed AF compared to PE patients who did not develop AF (157.7 ± 19.0 ng/mL vs. 129.0 ± 9.3 ng/mL, P = 0.0386). This study suggests that thrombo-inflammatory biomarkers may be helpful in indicating an acute PE episode. Also, elevated TFPI levels may be associated with an increased risk of developing AF after a PE.
Introduction
Pulmonary embolism (PE) and atrial fibrillation (AF) are both separately associated with significant morbidity and mortality. 1,2 There has been much debate in the literature regarding how these diseases are related to oneanother with some studies suggesting that PE can be a complication of AF via thrombus formation in the right atrium. 3,4 However, new research has recently demonstrated that patients with an acute PE episode not only have an increased age-adjusted prevalence of AF, but also have an increased age-adjusted incidence of AF, suggesting perhaps that increased cardiac stress associated with an acute PE episode can increase risk of new-onset AF. 5 Despite this bidirectional relationship, little is known about how to differentiate PE patients with pre-existing AF from patients at risk of developing AF after an acute PE. Because PE patients with comorbid AF, regardless of whether it is preexisting or new-onset, are at an increased risk of morbidity and mortality, developing a prediction model to understand this relationship is important. 5 We sought to investigate the role of biomarkers of thrombo-inflammation in risk stratifying patients who present with an acute PE.
D-Dimer
D-Dimers are circulating protein fragments released from disintegrating blood clots that are clinically measured to rule out PE in patients with a low pre-test probability. 6 While an important practical screening tool for decision making in the hospital, the D-dimer test has been further studied for its role in predicting outcomes after PE. A study done by Blamoun et al suggests a strong correlation with increasing levels of D-dimer and in-hospital mortality and PE recurrence. 7 Multiple studies have also noted this biomarker’s utility in AF as an indicator of left atrial enlargement, thrombus formation, and cardiac stress. 8 –10 Overall, while not clinically relevant in AF, the D-dimer test seems to be an indicator of the prothrombotic atmosphere created by AF. Therefore, we included this biomarker in our study to investigate its role in PE patients with comorbid AF. We hypothesized that D-dimer levels would be elevated in PE patients with pre-existing or new-onset AF versus PE patients without AF.
C-Reactive Protein (CRP)
CRP is a liver-made protein used clinically to detect inflammation in various disease processes, including AF. The literature notes that not only do CRP levels in AF patients predict recurrence of AF post-ablation therapy, but they also predict thromboembolic complications and mortality in AF. 11 –14 Furthermore, a large epidemiological study done by Lee et al revealed that persistently elevated CRP is associated with increased risk of AF development. 15 Like in AF patients, CRP has also been described as a helpful tool in predicting outcomes in PE patients. 16,17 Despite its utility in AF and PE separately, CRP has not been investigated when both diseases co-exist. Therefore, we decided to research how this biomarker behaves in PE patients with pre-existing or new-onset AF. We hypothesized that this biomarker, like D-dimer, would also be elevated in PE patients with comorbid AF when compared to PE patients without AF.
Plasminogen Activator Inhibitor-1 (PAI-1)
PAI-1 is a primary inhibitor of activators of the fibrinolytic pathway; therefore, elevated levels of this biomarker may serve as an indicator of impaired fibrinolysis. While this biomarker has not been studied in PE patients, PAI-1 levels have been found to predict the presence of left atrial appendage thrombus in AF patients, thus representing the prothrombotic and inflammatory state of this disease process. 18 –20 We included this biomarker to not only study its role in PE patients, but also to investigate whether or not there are differences in PAI-1 levels in PE patients with pre-existing or new-onset AF. Like our previously mentioned biomarkers, we hypothesized that PAI-1 levels would also be elevated in PE patients with AF when compared to PE patients without AF.
Thrombin Activatable Fibrinolysis Inhibitor Antigen (TAFIa)
TAFIa is an essential part of the coagulation and fibrinolysis process; thrombin activates TAFIa after forming a fibrin clot to protect it against lysis. 21 While it has not been extensively studied in either disease state, a small study done by Negreva et al reveals that TAFIa levels are reduced in the first day after new onset AF which may explain the thromboembolic potential of this disease immediately after its onset. 10 On the other hand, another study done by Schroeder et al exploring TAFIa’s role in PE found that TAFI levels are increased with increasing pulmonary occlusion rate, perhaps suggesting inefficient fibrinolysis. 22 In order to study this biomarker’s role in both diseases, we measured the levels of TAFIa in PE patients in hopes of further studying its role in risk stratifying patients with pre-existing AF or new-onset AF. We hypothesized that this biomarker would also be elevated in patients with both diseases when compared to PE patients without AF.
Factor XIIIa (FXIIIa)
FXIIIa, like TAFIa, is involved in fibrin clot stabilization, increasing clot resistance to lysis. A study looking at polymorphisms of genes encoding FXIIIa and TAFIa found that certain alleles of these genes can be protective against PE. 23 Overall, not much more is known about FXIIIa’s role in PE or AF. Therefore, we choose to include this biomarker in our study to learn more about how its role in PE patients with and without AF. Like with TAFIa, we hypothesized that this biomarker would also be elevated in patients with both diseases.
Alpha-2-Antiplasmin (A2A)
A2A is an enzyme that inactivates plasmin, thus inhibiting the fibrinolytic process. Several studies on mice models of PE have found that inhibiting this biomarker while administrating thrombolytic therapy was helpful in treatment of PE. 24,25 Meanwhile, the role of A2A in AF has been contraindicatory. While some studies have shown a lower level of this biomarker in new onset AF, other studies have noted elevated levels of this biomarker in AF patients at higher risk of thromboembolic complications. 10,26 Therefore, we decided to include this biomarker in our investigation to further clarify A2A’s role in PE patients with and without AF. We hypothesized that this biomarker would be significantly elevated in patients with both diseases.
Microparticle (MP)
MPs are membrane vesicles excreted from cells in response to activation and apoptosis. This biomarker has been well studied in AF as a marker of hypercoagulability. 27,28 Likewise, MPs have been associated with hyperactivation of platelets in PE. 29 Because this biomarker has been shown to be elevated in both diseases separately, we hypothesized that its levels would be even more elevated in patients with both PE and AF when compared to PE patients without AF.
Tissue Factor Pathway Inhibitor (TFPI)
TFPI is an important factor involved in inhibiting initiation of coagulation process. 30 The literature describes conflicting roles of this biomarker in AF. A study done by An et al found that TFPI is not significantly different between AF patients and controls so long as there is no presence of LA thrombus. 31 However, a study by Yamashita et al revealed that AF paced rats had lower levels of this biomarker, perhaps indicating a hypercoagulable state. 32 Meanwhile, little research exists about TFPI in PE. It has been postulated in the literature that low levels of TFPI are associated with increased risk of venous thromboembolism, but a study done by Zakai et al does not support this claim. 33 To further investigate this biomarker’s role in PE and AF, we included it in our study.
Materials and Methods
Patient Selection
This study is a retrospective observational study. Study patients were enrolled from a Pulmonary Embolism Response Team (PERT) registry. This registry consists of patients presenting with an acute PE at a 2-hospital tertiary health care center (Loyola University Medical Center and Gottlieb Memorial Hospital) between March 2016 and March 2019. Acute PE was confirmed using either CT angiography or ventilation/perfusion imaging. Because this was an observational study, sample size calculation was not performed priori. At the time of PE diagnosis, discarded blood samples from these patients were assigned a unique code to de-identify and access to protected health information was limited to the primary investigators of the study. These samples were then analyzed for this study. Due to the study design and due to minimal risk to the participant, a consent waiver was obtained. The study was approved by the Institutional Review Board at Loyola University Medical Center.
Eligibility Criteria
Inclusion criteria comprised of patients who were older than 18 years and were discharged with a principal discharge diagnosis of PE (ICD-9 codes: 415.1, 415.11, 415.12, 415.19). Exclusion Criteria were patients who did not meet the eligibility criteria were excluded.
Plasma Biomarker Analysis
All patients had blood samples collected at the time of PE diagnosis. Blood was centrifuged to separate the plasma, which was then aliquoted and frozen for future analysis. Blood samples were analyzed. PAI-1, D-dimer, TAFIa, FXIIIa, MP, CRP, and TFPI were profiled using Enzyme Linked-Immuno-Sorbent Assay (ELISA). TAFIa, A2A, and FXIIIa levels were measured using a functional assay and were reported as a percentage of normal controls. Normal controls were obtained from a commercial source (n = 10; George King Bio-Medical, Inc., Overland Park, KS). These controls consisted of pooled normal human plasma samples from volunteers. After data was obtained, it was stored on RedCap, a secure network within the Loyola University Medical Center’s secure research server.
Once biomarker data was collected and stored, this cohort was divided into 3 groups: PE patients with a prior diagnosis of AF, PE patients with a subsequent diagnosis of AF, and PE patients who did not develop AF. Levels of the above mentioned biomarkers were then compared between these 3 groups.
Statistical Analysis
GraphPad Prism software was used to perform the statistical analysis. Plasma levels of biomarkers were recorded as means ± standard errors. Kruskal Wallis ANOVA tests were performed to compare levels of each biomarker in control patients, PE patients with pre-existing AF, PE patients without AF, and PE patients with new-onset AF. Box plots were constructed to visualize differences of biomarker levels across different patient groups. Two-tailed Mann-Whitney U-tests were performed to compare biomarker levels between PE patients who did not develop AF and those who did. Patient demographics and clinical characteristics were presented using descriptive statistics, mean, and standard error. Demographics between these 4 groups were analyzed using Chi-square analysis.
Results
The study cohort was divided into 3 groups: PE patients with a prior diagnosis of AF (n = 8), PE patients with a subsequent diagnosis of AF (n=11), and PE patients who did not develop AF (n = 71). Patients with pre-existing AF were the eldest, averaging 75.9 years, while patients with new-onset AF and no AF averaged 68.1 years and 56.1 years, respectively (P = 0.0006). The distribution of sex, race, BMI, and PE severity in the 3 study cohorts, as noted in Table 1, was insignificant (P > 0.05). The distribution of types of AF between the PE group with pre-existing AF and the PE group with new-onset AF was also insignificant (P > 0.05).
Demographics of PE Patients With Pre-Existing AF (“Pre”), PE Patients Without AF (“PE”), and PE Patients With a Subsequent Diagnosis of AF (“Post”).

Overall, circulating levels of PAI-1, D-dimer, TAFIa, MP, CRP, and TFPI were higher than the study group compared to the control group. As noted in Table 2, PAI-1 levels were significantly elevated in PE patients with preexisting AF (69.9 ± 17.2 ng/mL), in PE patients without AF (66.5 ± 5.3 ng/mL), and PE patients with new-onset AF (71.4 ± 13.0 ng/mL) compared to controls (11.5 ± 5.1 ng/mL, P = 0.0001). Likewise, D-dimer levels were significantly elevated in PE patients with preexisting AF (5119.9±1188.3 ng/mL), in PE patients without AF (8234.1 ± 768.1 ng/mL), and PE patients with new-onset AF (5236.5 ± 1525.2 ng/mL) compared to controls (89.6 ± 22.3 ng/mL, P < 0.0001). TAFIa levels were also significantly elevated in PE patients with preexisting AF (114.4 ± 13.0%), in PE patients without AF (107.8 ± 3.0%), and PE patients with new-onset AF (114.2 ± 8.7%) compared to controls (76.4 ± 8.5%, P = 0.0072). MP levels were significantly elevated in PE patients with preexisting AF (33.5 ± 2.8 nM), in PE patients without AF (83.1 ± 8.0 nM), and PE patients with new-onset AF (97.9 ± 22.1 nM) compared to controls (7.9 ± 1.9 nM, P < 0.0001). CRP levels were significantly elevated in PE patients with preexisting AF (13.8 ± 2.7 ng/mL), in PE patients without AF (55.0 ± 7.4 ug/mL), and PE patients with new-onset AF (22.5 ± 6.3 ug/mL) compared to controls (17.7± 9.2 ug/mL, P = 0.0052). Lastly, TFPI levels were significantly elevated in PE patients with preexisting AF (120.0 ± 22.8 ng/mL), in PE patients without AF (129.0 ± 9.3 ng/mL), and PE patients with new-onset AF (157.7 ± 19.0 ng/mL) compared to controls (60.2 ± 6.7 ng/mL, P = 0.0002). See Figure 1A for a pictorial depiction of this data.
Circulating Levels of Biomarkers in the Control Group Compared to the 3 Study Groups.a
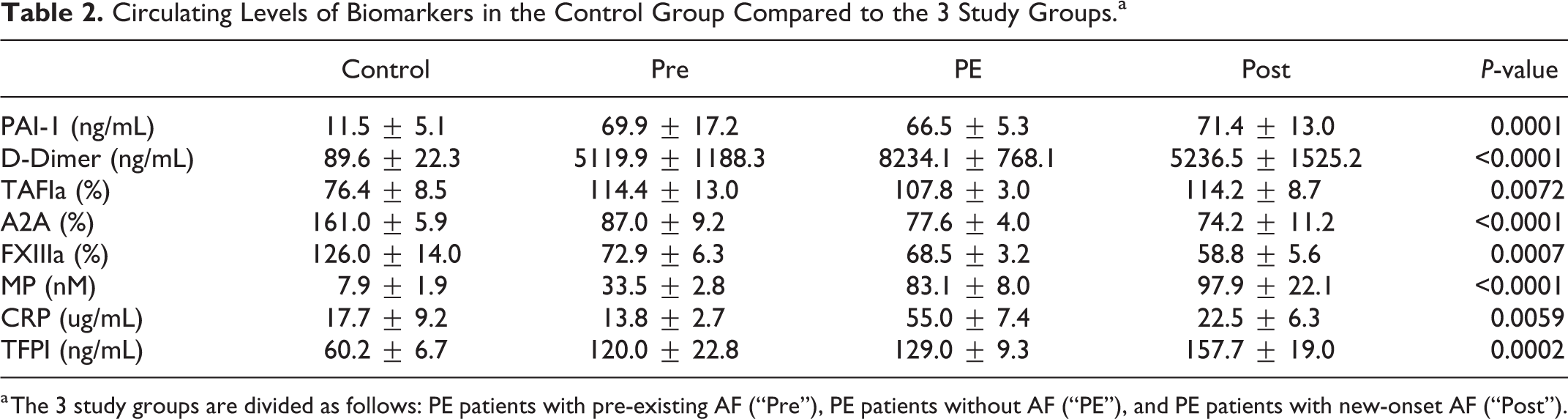
a The 3 study groups are divided as follows: PE patients with pre-existing AF (“Pre”), PE patients without AF (“PE”), and PE patients with new-onset AF (“Post”).

A, Box plots with standard error bars showing significantly elevated levels of the following biomarkers in the 3 study groups compared to controls. B, Box plots with standard error bars showing significantly decreased levels of the following biomarkers in the 3 study groups compared to controls.
Contrastingly, circulating levels of A2A and FXIIIa were lower in the study group compared to the control group. As noted in Table 2, A2A levels were significantly decreased in PE patients with preexisting AF (87.0 ± 9.2%), in PE patients without AF (77.6 ± 4.0%), and PE patients with new-onset AF (77.6 ± 4.0%) compared to controls (161.0 ± 5.9%, P < 0.0001). Also, FXIIIa levels were significantly decreased in PE patients with preexisting AF (72.9 ± 6.3%), in PE patients without AF (68.5 ± 3.2%), and PE patients with new-onset AF (58.8 ± 5.6%) compared to controls (126.0 ± 14.0%, P = 0.0007). See Figure 1B for a pictorial depiction of this data.
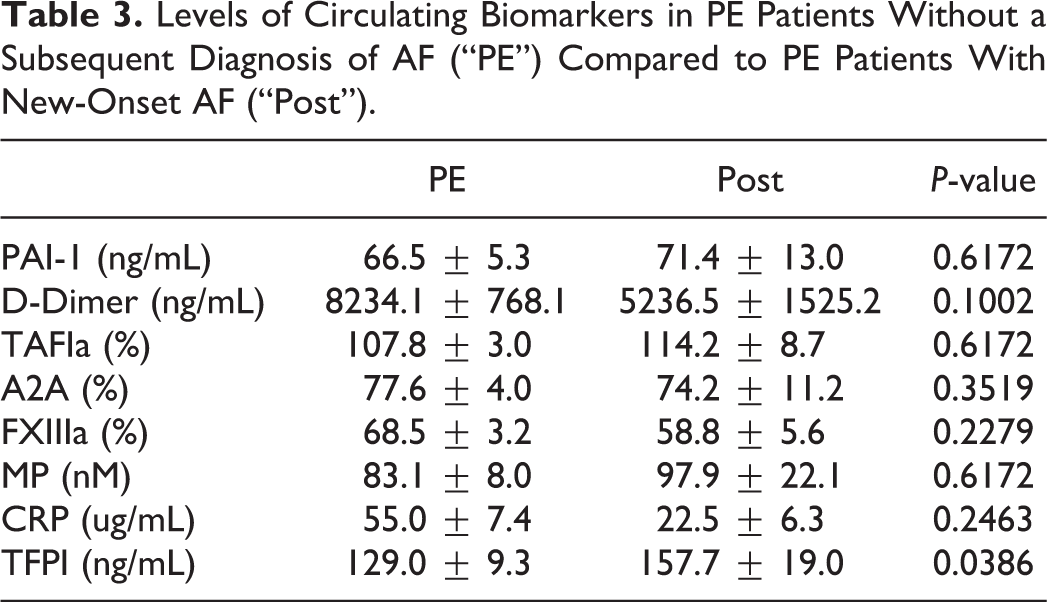
When circulating levels of all of the abovementioned biomarkers were compared between PE patients without AF and PE patients with new-onset AF, TFPI was significantly elevated in PE patients with a subsequent diagnosis of AF compared to PE patients who did not develop AF (157.7 ± 19.0 ng/mL vs. 129.0 ± 9.3 ng/mL, P = 0.0386). All other biomarkers were insignificantly different between the 2 groups as noted in Table 3. See Figure 2 for a pictorial depiction of this data.
Levels of Circulating Biomarkers in PE Patients Without a Subsequent Diagnosis of AF (“PE”) Compared to PE Patients With New-Onset AF (“Post”).

Box plot with standard error bars comparing significant increase in TFPI in PE patients who subsequently developed AF versus those who did not.
Discussion
In this study, we utilized various thrombo-inflammatory biomarkers to investigate the relationship between PE and AF. Our findings are as follows: (1) PAI-1, D-dimer, TAFIa, MP, CRP, and TFPI were significantly increased in all 3 study groups compared to controls; (2) A2A and FXIIIa were significantly decreased in all 3 study groups compared to controls; and (3) TFPI was significantly elevated in PE patients with a subsequent diagnosis of AF compared to PE patients who did not develop AF.
A2A and FXIIIa Levels During Acute PE
It is well established that clot formation in the body increases not only the thrombotic process but also the fibrinolytic process in order to self-correct the underlying pathophysiology. In our study, A2A and FXIIIa were 2 biomarkers that strayed from our expected hypothesis. Levels of this biomarker were both significantly lower in the study group than the control group. A study investigating a mice model of PE found that low levels of A2A decreased mortality in mice after their acute PE episode. 24,34 This may suggest that low levels of A2A could play protective role in PE patients. Therefore, we speculate that low levels of this biomarker in our study group may be representative of the fact that a majority of our patients had either a low risk or submassive PE rather than a massive PE. Further investigation with larger study groups would be necessary to discern how A2A can be utilized to determine the risk of mortality after an acute PE.
Though we also anticipated levels of FXIIIa to be elevated in our study group compared to our control group, our results showed otherwise. This was less surprising than decreased levels of A2A, because a study done by Sane et al in International Journal of Laboratory Hematology found that consumption of coagulative factors during an acute PE episode result in low levels of these biomarkers right after. 35 Again, however, more research with larger and more balanced study groups are necessary to understand how a PE affects levels of FXIIIa.
TFPI’s Role in Risk Stratifying PE
Of all the biomarkers studied, this research shows that elevated TFPI levels in patients presenting with an acute PE episode are associated with an increased risk of developing AF after a PE. While TFPI has been shown to be elevated in patients with PE or other venous thromboembolic disease compared to healthy volunteers, no studies have looked at this biomarkers utility in predicting AF in patients presenting with an acute PE episode. 36,37 Considering the increased risk of mortality in patients with both diseases, this may provide a useful tool in risk stratifying patients. 5 However, larger studies would be necessary to study TFPI’s role in differentiating PE patients at an increased risk of developing AF and those who are not.
Age as a Risk Factor of New-Onset AF After PE
One last demographic difference between the 3 study groups was the distribution of age. Those with preexisting AF were the eldest, which is expected considering that age is one of the most significant risk factors for AF alone. Those who developed AF after a PE were also significantly older than those who did not, suggesting that age may also be a risk factor for post-PE development of AF. This finding, though logical, has not been supported by the one Turkish study that explores this question; rather, in that study, Sahan et al find that age is not associated with an increased risk of developing AF after a PE. 38 More research and is necessary to further investigate this relationship.
Limitations
The study limitations include unbalanced study groups and relatively small sample sizes. Because PE patients were stratified based on their AF status after enrollment in the PERT group, it was difficult to ensure balanced study groups. We did not have access to patient comorbidities such as coronary artery disease, hypertension, diabetes mellitus, chronic kidney disease, heart failure, cancer, or chronic obstructive pulmonary disease. We also did not have access to medications, like anticoagulants, antiplatelets, beta blockers, or calcium channel blockers, used by these patients at baseline. This information would have given us a better understanding of confounding variables that could have impacted the results of this study.
Using propensity score matching to compare the experimental group to the control group would have better accounted for covariables; however, our study was limited by our use of pooled human plasma as controls since the medical histories of volunteers contributing to these samples were unknown. Thus, in future studies, we would want to ensure that experimental and control groups were matched in terms of comorbidities, medications, etc. to avoid confounding variables.
This study also found a significant difference in age between the groups. PE patients with pre-existing AF were generally older than patients without AF at baseline. While this is reasonable based on the fact that age is one of the most common risk factors of AF, a more balanced distribution of patient groups in terms of demographics would further validate these observations. Additionally, more clinical information from the time of PE diagnosis such as heart rate, blood pressure, pulse oximetry, echocardiography data, BNP levels, and renal function would also have been interesting to further characterize patients. Because we sought to profile biomarkers in PE patients, we did not collect this information for our study; however, we obtain this information for future studies. Despite these limitations, this study underscores the importance of further investigating biomarkers that may help stratify PE patients at risk of developing AF.
Conclusion
Various thrombo-inflammatory biomarkers like PAI-1, D-dimer, TAFIa, MP, CRP, TFPI, A2A and FXIIIa are significantly elevated at the time of acute PE. Elevated levels of TFPI may be associated with PE patients who are more likely to develop new-onset AF. The clinical utility of TFPI as a risk stratifying biomarker needs to be further investigated with study models appropriately designed to determine this information.
Footnotes
Authors’ Note
Informed consent for patient information to be published in this article was not obtained because of the study design and the minimal risk to the participant. A consent waiver was obtained. Ethical approval for this study was obtained from the Institutional Review Board at Loyola University Medical Center (LU#2094572).
Acknowledgments
The authors are thankful to the Pulmonary Embolism Response Team (PERT) for the facilitation of the collection of blood samples at various locations. We are also thankful to the staff of the hemostasis and thrombosis laboratories of the Department of Pathology, Laboratory Medicine, and clinical laboratories of Loyola University Medical Center for their assistance in completing this study. We are thankful to Dr. Seth Robia and Dr. Alain Heroux, Co-Directors of the Cardiovascular Institute, for providing partial funding for this project. The skillful assistance of Ms. Erin Healy-Erickson in preparing this manuscript is gratefully acknowledged. A special thanks to Mr. Jonas Kingo of Aniara Diagnostics for providing some of the kits and reagents used in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Received partial funding from Dr. Seth Robia and Dr. Alain Heroux, Co-Directors of the Cardiovascular Institute.