
Abstract
Background:
Cesarean section is an independent risk factor for Venous thromboembolism (VTE). Low molecular weight heparin (LMWH) is extensively used for VTE prophylaxis after cesarean section. In this study, the effects of LMWH on coagulation and fibrinolysis after cesarean section and its clinical value were explored by studying the changes in laboratory indicators.
Methods:
Antepartum and postpartum peripheral blood of 44 pregnant women who underwent vaginal delivery and 44 pregnant women who underwent cesarean section treated per routine with LMWH thromboprophylaxis on the first day post-operatively were collected for the following tests: D-dimer; thrombotic markers such as thrombomodulin (TM), thrombin-antithrombin complex (TAT), α2-plasmin inhibitor-plasmin complex (PIC), and tissue plasminogen activator inhibitor complex (t-PAIC); thromboelastography.
Results:
Compared to the antepartum levels, PIC increased, TM, TAT, and t-PAIC decreased significantly in the parturients after a spontaneous vaginal delivery. Compared to the antepartum levels, parturients routinely treated with LMWH after cesarean section had higher PIC levels and lower D-dimer, TAT, and t-PAIC levels. Compared with parturients after vaginal delivery, parturients treated with LMWH after cesarean section had higher levels of TM, R, and MA, while there was no significant differences in the levels of D-dimer, TAT, PIC, t-PAIC, K, angle, LY30, and CI.
Conclusion:
The coagulation and fibrinolytic systems in gravidas and parturients are in a high level of dynamic equilibrium. The levels of coagulation and fibrinolytic system activation were similar in parturients who were routinely treated with LMWH after cesarean section compared with parturients after a spontaneous vaginal delivery.
Keywords
Introduction
Venous thromboembolism (VTE) is a leading cause of maternal mortality. The risk for VTE in gravidas and parturients is due to special physiologic changes, such as hypercoagulability, venous stasis, and vascular endothelial injury. Such changes make pregnant women at high risk for VTE. The incidence of VTE is 5 times higher among pregnant women than non-pregnant women of the same age. In addition, the risk of VTE is 5 times higher in the puerperium than during pregnancy. 1 After a cesarean section, 3 in 1000 women will develop a postpartum VTE and the incidence is increased four-fold compared to women who have a spontaneous vaginal delivery. 2 To reduce the occurrence of VTE after cesarean section, clinicians often utilize mechanical preventive measures or pharmacologic prophylaxis, and encourage maternal ambulation as soon as possible.
Low molecular weight heparin (LMWH) is the agent of choice for postnatal thromboprophylaxis. In April 2015, the Royal College of Obstetricians and Gynecologists (ROCG) issued Green-top Guideline No. 37a (Reducing the Risk of Venous Thromboembolism during Pregnancy and the Puerperium), which recommends that all women who undergo caesarean section should be considered for thromboprophylaxis with LMWH for 10 days after delivery in addition to women who undergo an elective cesarean section and should be considered for thromboprophylaxis with LMWH for 10 days after delivery if they have any additional risk factors. 3 However, the routine use of LMWH in pregnant women post-cesarean section is still controversial in China, and clinicians use different measures to prevent thrombosis. Some clinicians favor LMWH prevention for women at moderate or higher risk VTE after cesarean section. The confidential Enquiries for Maternal and Child Health (CEMACH) report showed that > 20% of women who died secondary to a VTE had no identifiable risk factors. 4 In this study LMWH (nadroparin calcium, 4100 IU) was routinely administered on the first day after cesarean section to prevent thrombosis.
D-dimer is the final fragment of the fibrinolytic enzyme applied to cross-linked fibrin and is the most commonly used laboratory marker for coagulation and fibrinolytic activation. 5 As a marker of endothelial cell injury, TM is of great significance in the diagnosis and treatment of VTEs. 6 TAT is a sensitive indicator of coagulation pathway activation. 7 The presence of PIC reflects the degree of plasmin activation. 8 When fibrin is formed, fibrin activates tissue plasminogen activator (t-PA), and the activated t-PA and plasminogen activator inhibitor (PAI) are combined at a 1:1 ratio to form a complex (t-PAIC), which is a marker that comprehensively reflects the degree of fibrinolytic system activation and vascular endothelial cell injury. Thromboelastography can demonstrate the patient’s coagulation status. The parameters of a TEG tracing include the reaction time (R; This reflects the adequacy of coagulation factors.), clot formation time (K; This reflects clot kinetics.), alpha angle (Angle; This reflects fibrinogen level.), maximum amplitude (MA; This reflects platelet function.), percentage lysis at 30 min (LY30; This reflects clot lysis.), Coagulation Index (CI; This describes the overall coagulation). 9
The aim of this study was to compare the changes and differences in indicators related to the blood coagulation and fibrinolysis systems in pregnant women who routinely used LMWH after cesarean section with those who had a spontaneous vaginal delivery. We also explored the role of routinely used LMWH after cesarean section and its clinical significance.
Materials and Methods
Patients and Study Design
Eighty-eight healthy women, 18-45 years of age with singleton gestations, signed informed written consent and were recruited for this study at Nanfang Hospital of Southern Medical University from January 2019 to July 2019. Forty-four patients who had spontaneous vaginal deliveries with no complications were designated the VD group and 44 women who underwent caesarean section were designated the CS group. LMWH (nadroparin calcium, 4100 IU) was routinely administered by subcutaneous injection to all parturients on the first day after undergoing a cesarean section. The exclusion criteria consisted of the following: anticoagulant therapy or antiplatelet agents during pregnancy; BMI > 30 kg/m 2 ; assisted reproduction; history of recurrent abortion (≧ 3); pre-eclampsia and placental abruption; history of venous thrombosis or pathologic bleeding; hereditary or acquired thrombophilia; autoimmune disorders; tumors; diabetes; cardiopathy; acute or chronic infections; chronic nephropathy; abnormal blood loss; blood transfusion; amniotic fluid embolism; and disseminated intravascular coagulation (DIC). Ethical approval was obtained from the Medical Ethics Committee of Nanfang Hospital.
Blood Sampling and Assays
We performed blood sampling for D-dimer, TM, TAT, PIC, and t-PAIC at the following 2 time points: before delivery; and 2 days after vaginal delivery or cesarean section (before the next dose of LMWH). Peripheral blood samples were collected by venipuncture of an antecubital vein into vacuum tubes. Sample tubes containing 1.8 ml of blood and 0.2 ml of 3.2% sodium citrate were centrifuged at 2000 g for 10 min at room temperature. The detection of D-dimer was completed within 4 h after plasma separation. The separated plasma was collected and stored at −80°C for subsequent determination of the TM, TAT, PIC, and t-PAIC levels.
Thromboelastography assays were performed 2 days after vaginal delivery or cesarean section. Whole blood (2 mL) was collected in an anticoagulant tube containing 3.2% sodium citrate. The samples were thoroughly mixed before the test, and the test was completed within 2 h. For each assay, we pipetted 1 mL of citrated whole blood sample into a kaolin tube and gently mixed it by inversion 5 times. 340 µL kaolin-activated blood was pipetted into a disposable microreaction cup in which 20 µL 0.2 mol/L CaCl2 was pre-pipetted, followed by lifting the cup holder and starting analysis.
Laboratory Methods
D-dimer assays were measured with latex-based immunoturbidimetry on a CA 1500 or CS 5100 automatic coagulation analyzer (Sysmex, Kobe, Japan). TM, TAT, PIC, and t-PAIC levels were determined by chemiluminescent immunoassay using an HISCL 800 chemiluminescence apparatus (Sysmex). Thromboelastography assays were performed using a TEG 5000 Thrombelastograph Hemostasis Analyzer system (Haemonetics, Braintree, MA, USA).
Statistical Analysis
Statistical analyses were performed using SPSS (version 20.0). Paired sample t-tests were used for intra-group comparisons. The measurement data were represented by the median (quartile spacing). Statistical comparisons were tested with the Mann–Whitney U test. A P-value < 0.05 was considered statistically significant.
Results
Patient Demographics
Eighty-eight women were recruited (44 patients in the VD group and 44 patients in the CS group). There were no significant differences with respect to age, parity, pre-pregnancy BMI, and gestational at the time of delivery between these 2 groups (Table 1). All women were non-smokers and had no personal or family history of a VTE or thrombophilia. None of the patients in this study had bleeding complications following LMWH prophylaxis.
Patient Demographics.

Data are presented as the mean ± standard deviation. Data were statistically analyzed using an independent sample t-test.
Correlation Analysis
There was a positive correlation between prenatal TM and patients’ age (rs = 0.323; P < 0.01; Table 2). There were positive correlation between postpartum TM, K and patients’ age (rs = 0.331, 0.284; P < 0.01, 0.05). There was a negative correlation between postpartum MA and patients’ Pre-pregnancy BMI (rs = −0.227; P < 0.05). There was a negative correlation between postpartum TAT and patients’ Gestation at delivery (rs = −0.223; P < 0.05; Table 3).
Correlation Between Prenatal Coagulation Parameters and Patients’ Characteristics.
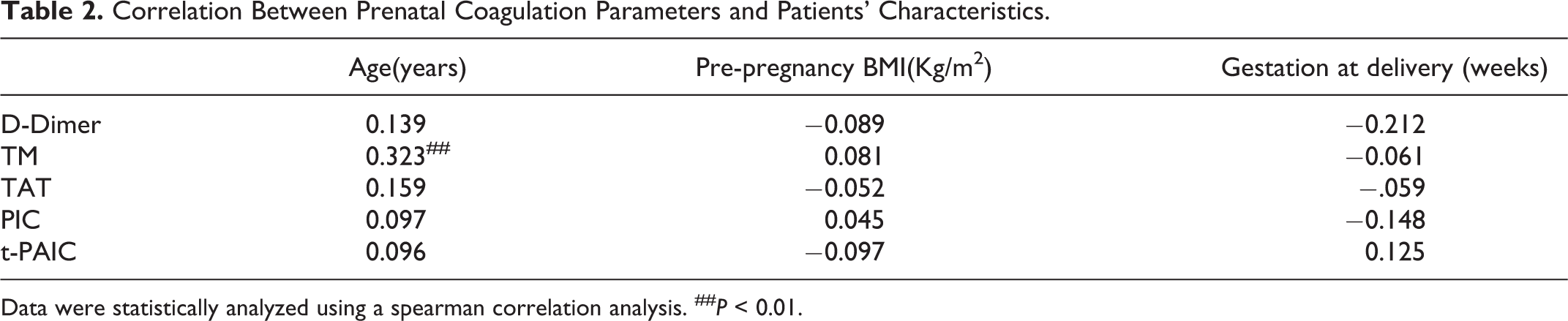
Data were statistically analyzed using a spearman correlation analysis. ## P < 0.01.
Correlation Between Postpartum Coagulation Parameters and Patients’ Characteristics.

Data were statistically analyzed using a spearman correlation analysis. ## P < 0.01; # P < 0.05.
Comparison of Prenatal and Postpartum Indicators in the VD Group
The prenatal PIC level increased (P = 0.035) and the TM, TAT, and t-PAIC levels decreased (P = 0.000, 0.006, and 0.000, respectively) in the VD group after delivery; however, there was no significant difference in the D-dimer level (P > 0.05; Table 4) .
Comparison of Prenatal and Postpartum Indicators in the VD group (n = 44).

Data are presented as the mean ± standard deviation. Data were statistically analyzed using a paired sample t-test. # P < 0.05.
Comparison of Prenatal and Postpartum Indicators in the CS Group
The PIC level in the CS group after delivery increased (P = 0.004) and the levels of TM and t-PAIC decreased (P = 0.000, 0.000) compared to the prenatal levels, while the D-dimer and TAT levels showed no statistically significant differences (P > 0.05; Table 5).
Comparison of Prenatal and Postpartum Indicators in the CS group (n = 44).

Data are presented as the mean ± standard deviation. Data were statistically analyzed using a paired sample t-test. # P < 0.05.
Comparison of Postpartum Indicators Between the VD and CS Groups
Compared with the VD group after delivery, the postpartum TM, R, and MA levels in the CS group increased (P = 0.011, 0.008, and 0.003, respectively), while the D-dimer, TAT, PIC, t-PAIC, K, angle, LY30, and CI levels showed no statistically significant differences (P > 0.05; Table 6).
Comparison of Various Indicators Between the VD and CS Groups After Delivery.

Data are presented as the median (25th-75th percentiles). The comparison between the 2 groups was statistically analyzed using the non-parametric Mann–Whitney U test. # P < 0.05.
Discussion
Epidemiologic and laboratory findings have shown that hypercoagulability occurs early in human pregnancies. Indeed, thrombin generation begins to increase in women at approximately 5 weeks gestation. 10 Both the coagulation and fibrinolysis systems are activated. As the pregnancy advances, coagulation and fibrinolysis functions are enhanced. TAT is a molecular marker of thrombin generation and a sensitive indicator of activation of the coagulation pathway. The TAT levels after vaginal and cesarean section deliveries were significantly lower than before delivery, indicating that the degree of coagulation system activation before delivery was more apparent than after delivery. PIC is an activation marker of the fibrinolytic system and reflects the degree of fibrinolytic enzyme activation. Independent of the mode of delivery, the PIC level was shown to be increased after delivery, indicating that the degree of fibrinolytic system activation was more apparent than before delivery. The basis for the low fibrinolytic capacity in pregnancy is mainly due to the significant increase in endothelial cell PAI-1 levels and placenta PAI-2 levels. 11 During delivery, platelets, coagulation factors, and fibrinogen are consumed in large quantities. After the placenta is delivered, the fibrinolytic capacity rapidly improves and is enhanced, and the PAI-1 and PAI-2 levels decrease rapidly. T-PAIC is formed by the combination of activated t-PA and PAI-1 at a 1:1 ratio. Therefore, the t-PAIC level decreased in the early postpartum period and the difference was statistically significant compared with before delivery. Blood coagulation, anticoagulation, fibrinolytic, and anti-fibrinolytic systems in gravidas and parturients are maintained at a high level in a dynamic equilibrium. 12
It has been shown that the TM level is significantly increased throughout pregnancy 13 and the increase is associated with increased t-PA and PAI-1 levels. The TM level remains elevated 1 h after delivery, but is significantly decreased by the third day after delivery. 14 In the current study, TM detection was performed on the second day after delivery. Compared with the VD group before delivery, the TM level was significantly lower after vaginal delivery. Because of more severe vascular endothelial injury, the TM level of women undergoing cesarean section was not significantly different from before delivery, but higher than after vaginal delivery.
LMWH is the agent of choice for puerperal thromboprophylaxis because it is safe, effective, and has no adverse effects on lactation. Due to the smaller molecular weight of LMWH than heparin, the combination with AT-III after forming complexes with factor X has high selectivity. The combination of LMWH with IIa and other coagulation factors is weak. Therefore, the effect of LMWH inhibition on thrombin is less than factor X. Cesarean section exacerbates the pathologic basis of venous thrombotic diseases and aggravates the hypercoagulability of blood, venous blood stasis, and vascular endothelial injury, which are independent risk factors for VTE. To reduce the occurrence of VTE after cesarean section, LMWH is commonly used to prevent thrombosis. In the current study, LMWH was routinely used after cesarean section for healthy gravidas at term to determine the clinical application value of LMWH.
The postpartum TM level in the CS group was significantly higher than the VD group, likely because cesarean section results in more severe vascular endothelial injury. At the same time, the postpartum R and MA values in the CS group were also higher than the VD group. The R time reflects the activity of coagulation factors. The shorter the R time is, the stronger the activity of coagulation factors. The MA value reflects the activity of platelets. The greater the MA value is, the stronger the activity of platelets. The postpartum R time was longer in the CS group than the VD group, suggesting that the activity of coagulation factors was low in the CS group. This change suggests that the use of LMWH inhibits factor X activity after a cesarean section, thus inhibiting activation of the coagulation pathway but not inhibiting platelet activity. Compared with the postpartum VD group, however, there was no significant difference in the postpartum D-dimer, TAT, PIC, and t-PAIC levels in the CS group, suggesting that there was no significant difference in the degree of coagulation and fibrinolysis system activation between parturients who routinely used LMWH after cesarean section and those who underwent vaginal delivery.
To determine the effect of LMWH therapy in the first 24 h post-cesarean section, Ismail et al. 15 showed that LMWH thromboprophylaxis in a healthy cohort of patients had a sustained effect in reducing excess thrombin production post-elective caesarean section. This finding is consistent with the lack of difference in postpartum TAT levels between the VD and CS groups in the current study, which further suggests that routine use of LMWH may benefit parturients after cesarean section.
At present, the reason why LMWH is not routinely used after cesarean section is that LMWH may increase the risk of postpartum bleeding; however, previous studies have shown that anticoagulation following cesarean delivery is associated with an increased risk of post-cesarean wound complications, but not postpartum bleeding complications. 16 In the current study, all parturients after cesarean section were treated with LMWH on the first day post-operatively and no postpartum hemorrhage was observed. In conclusion, we regard the routine use of LMWH thromboprophylaxis after cesarean section inhibits coagulation factor activation and might be helpful in inhibiting the coagulation pathway by combining the results of laboratory tests in this study. The benefits of routine use of LMWH may outweigh the risks.
Conclusion
Based on an analysis of laboratory indicators, antepartum hypercoagulability was shown to be more apparent than postpartum hypercoagulability, and the postpartum activation of fibrinolysis system was more apparent than antepartum. The levels of coagulation and fibrinolysis system activation were similar in women who routinely used LMWH anticoagulation after cesarean section and vaginal deliveries. Thus, the routine use of LMWH after cesarean section may be beneficial.
Footnotes
Acknowledgments
The authors are grateful for skillful technical assistance and the supply of testing reagents from Improve Medical, Ltd. (Guangzhou, Guangdong Province) and Vastec Medical, Ltd. (Guangzhou, Guangdong Province).
Author Contribution
Ziwei Liu and Chixiang Liu contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from the Medical Ethics Committee of Nanfang Hospital (NFEC-2018-143).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant No. 201604016093 from the Major Projects of Collaborative Innovation of Industry, University and Research of Guangzhou Municipal Science and Technology Bureau (Guangdong Province, China).
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.