
Abstract
The biomarkers for predicting venous thromboembolic events (VTEs) after oncologic surgery are still lacking. The current study aimed to analyze the relationships of CD62P and GP IIb/IIIa with hypercoagulation after oncologic surgery. A total of 76 patients with primary abdominopelvic tumors in our hospital were enrolled. The patients were divided into groups A (malignancy with no VTE group), B (malignancy with VTE group), and C (benign with no VTE group). Twenty healthy volunteers were selected as control. The plasma CD62P (4.69 ± 2.55 vs. 1.76 ± 0.48) and the GP IIb/IIIa (9.28 ± 3.79 vs. 1.76 ± 0.48) levels in group A were significantly higher than those in the control group preoperatively. The CD62P (31.46 ± 17.13 vs. 13.51 ± 7.43, P < 0.05), GP IIb/IIIa (42.33 ± 21.82 vs. 13.51 ± 7.43, P < 0.05), and D-dimer (7.33 ± 2.34 vs. 2.03 ± 0.55, P < 0.05) levels in group B were markedly higher 7 days after operation compared with those in group A. The CD62P and the GP IIb/IIIa exhibited a positive correlation with the hypercoagulable state after oncologic surgery.
Introduction
Venous thromboembolic events (VTEs), which consist of deep venous thrombosis (DVT) and pulmonary embolism (PE), are common complications in patients with cancer undergoing surgery and associated with increased mortality at the early stage of cancer surgery. 1 The overall incidence of VTE is estimated to be 2.3%, and the risk of VTE in patients who underwent surgery can last for 90 days. 2 The risk of VTE after oncologic surgery varies in accordance with the cancer type, study region, surgical location, and thromboprophylactic strategy. 2 However, the biomarkers for predicting VTEs after oncologic surgery are still lacking.
The glycoprotein IIb/IIIa (GPIIb/IIIa or αIIbβ3), a major membrane protein complex on the surface of platelets, is involved in platelet aggregation. 3 The platelet GPIIb/IIIa also participates in angiogenesis, tumor growth, and metastasis. 4 The P-selectin (CD62P) is located on activated endothelial cells and platelets and functions as a cell adhesion molecule. 5 The P-selectin is recognized as the major marker of platelet activation and may mediate cancer cell adhesion, inflammation, growth, and thrombosis. 6
VTE is associated with increased mortality at the early stage of cancer surgery. 2 At the same time, the use of anticoagulants for VTE may cause hemorrhage. Thus, challenges in the thromboprophylaxis remain in cancer patients undergoing surgery. Consequently, the platelet particle P-selectin and the platelet activation biomarker GPIIb/IIIa levels in patients with cancer undergoing surgery are tested in this study to analyze their relationships with hypercoagulation after oncologic surgery. The levels of different biomarkers are compared between patients with cancer undergoing surgery with and without VTE. The identification of biomarkers for predicting VTEs after oncologic surgery might provide critical evidence for clinicians on which to base the choice for thromboprophylaxis.
Materials and Methods
Patients
A total of 76 patients with primary abdominopelvic tumors in West China Hospital of Sichuan University between June 2018 and June 2019 were enrolled. Adults aged 18 years or older undergoing open or minimally invasive tumor resection were considered for enrollment. Patients were excluded if they had thromboembolism or hemorrhagic disease history, hormone use within the last 3 months, thrombocytopenia or antiplatelet drug use within 2 weeks, operation history within 3 months, and contrast agent allergy. This study was preapproved by the Ethical Committee of West China Hospital of Sichuan University. All subjects signed the informed consent before recruitment in this study.
The patients were divided into groups A (malignancy with no VTE group), B (malignancy with VTE group), and C (benign with no VTE group). A postoperative venous thromboembolism was defined as the occurrence of clinically detected DVT or PE. Patients were screened for DVT or PE if clinically suspected within 7 days after surgery. Diagnosis was confirmed using Doppler ultrasonography of the leg for DVT and a computed tomography pulmonary angiography for PE. Another 20 healthy volunteers were selected as the control group. Tumors were graded according to the AJCC 8th staging system. 7
Experimental Procedure
In group A and C, venous blood samples were collected preoperation, 7 days after operation, and 30 days after operation. In group B, venous blood samples were collected 7 days after operation, and 30 days after operation. The peripheral blood was extracted, and the supernatant was centrifuged and stored. Immunoenzymatic assays were used to measure the D-dimer. The activation of the platelet GPIIb/IIIa receptors and the expression of the platelet activation marker CD62P in the blood samples were quantified using flow cytometry as previous described. 8 After centrifugation at 800 r/min for 30 min and 3000 r/min for 5 min, platelet-rich plasma (450 μl) was incubated with 20 μmol platelet activator for 5 min at room temperature. The sample (5 μl) was incubated with antibody (BioLegend, San Diego, CA, USA) at room temperature without light for 15–20 min. Next, the sample was mixed with 1% paraformaldehyde (1 ml) at 2°C–8°C without light for 30 min. The sample was further resuspended in 1 ml phosphate-buffered saline and 1 µl standard microspheres (1:400, 0.82 μm). Lastly, the CD62P and the GP IIb/IIIa rates were determined using flow cytometry (Beckman XL; Beckman Coulter, Inc., Brea, CA, USA).
Statistical Analysis
The measurement data were presented as mean ± standard deviation. The comparison between 2 groups was tested using the independent sample t-test. The analysis of variance with Fisher’s exact test of measures was used for the percentages of CD62P and GPIIb/IIIa comparison at different time points. The countable data were expressed by the number of cases (%). Comparisons among groups were performed using the χ2 method. The data were analyzed using the SPSS 17.0 software (SPSS Inc., Chicago, IL, USA). P < 0.05 indicated that the difference was statistically significant.
Results
The baseline demographic and clinical characteristics of the study population are listed in Table 1. A total of 96 participants were enrolled in this study. Group A contained 25 males and 18 females with average age of 53.3 ± 11.7 years. Group B consisted of 12 males and 8 females with mean age of 54.5 ± 12.8 years. The thrombotic events in Group B included 9 isolated distal DVT, 11 proximal DVT, and no PE event. Median time point of VTE occurrence in malignancy with VTE group in this study was 4 days after surgery. Patients who were clinically detected DVT or PE received 4000 u enoxaparin or 6150 u nadroparin injected subcutaneously every 12 h. Group C consisted of 5 males and 8 females with mean age of 55.7 ± 12.8 years. Twenty healthy volunteers, including 11 males and 9 females with mean age of 53.8 ± 10.5 years, were enrolled as control. On the basis of the distribution of patient characteristics, no significant difference was found among the 3 groups. Pancreatic malignancy was recorded in 26 cases (41%), whereas hepatic malignancy was recorded in 20 cases (32%). Most patients (76%) belonged to stage I or II. Differences in operative time and blood loss between the groups were not observed. Significant differences in surgical characteristics were not observed between Groups A, B, and C.
Baseline Demographics and Clinical Characteristics of the 3 Groups.

BMI, Body mass index; n.a., data not available.
The plasma CD62P (4.69 ± 2.55 vs. 1.76 ± 0.48, P < 0.001) and the GP IIb/IIIa (9.28 ± 3.79 vs. 1.76 ± 0.48, P < 0.001) levels in group A were significantly higher than those in the control group preoperatively (Table 2). There is no significant difference of plasma CD62P (Pancreatic 4.88 ± 3.12; Hepatic 4.01 ± 1.77; Biliary 4.75 ± 1.44; Digestive tract 4.83 ± 2.73) and the GP IIb/IIIa (Pancreatic 10.34 ± 3.33; Hepatic 8.21 ± 1.79; Biliary 9.04 ± 3.21; Digestive tract 9.51 ± 3.16) levels between different types of cancer. The CD62P (13.51 ± 7.43 vs. 4.69 ± 2.55; P < 0.001) and the GPIIb/IIIa (19.77 ± 5.75 vs. 9.28 ± 3.79, P < 0.001) levels in group A were markedly higher 7 days after operation compared with preoperation (Table 3). The CD62P level remained higher 30 days after operation than 7 days after operation (22.36 ± 13.63 vs. 13.51 ± 7.43, P = 0.008). The CD62P (31.46 ± 17.13 vs. 13.51 ± 7.43, P < 0.001), GP IIb/IIIa (42.33 ± 21.82 vs. 13.51 ± 7.43, P < 0.001), and D-dimer (7.33 ± 2.34 vs. 2.03 ± 0.55, P < 0.001) levels in group B were markedly higher 7 days after operation compared with those in group A.
Comparison of the Laboratory Features of the Examined Groups Before Operation.

#P < 0.05, compared with control; $ P < 0.05, compared with group C.
Comparison of the Laboratory Features of the Examined Groups After Operation.
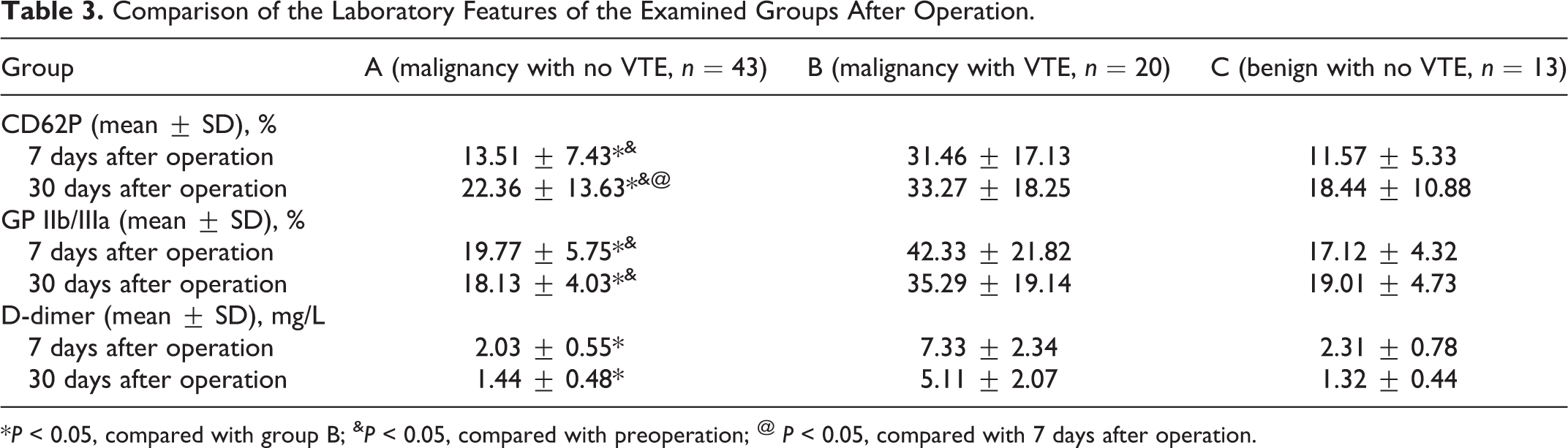
*P < 0.05, compared with group B; & P < 0.05, compared with preoperation; @ P < 0.05, compared with 7 days after operation.
After operation, 43 and 13 patients were confirmed malignant and benign, respectively. The histology of the benign tumors was the cystadenoma of pancreas, gastrointestinal stromal tumors, and solitary fibrous tumors. The CD62P (5.33 ± 2.67 vs. 2.89 ± 1.12, P = 0.03) and the GPIIb/IIIa (10.63 ± 3.84 vs. 6.21 ± 2.11, P = 0.01) levels in malignant patients were markedly higher compared with those in benign patients preoperatively. However, the D-dimer levels were similar between malignant and benign patients preoperatively (0.33 ± 0.09 vs. 0.29 ± 0.16, P = 0.32).
Discussion
VTE remains a major source of postoperative morbidity and mortality following oncologic surgery and is clinically important in the abdominopelvic surgery population. 9 The identification of the risk factors for VTEs is critical for thromboprophylaxis to be prescribed for patients with high risk. Guidelines have used the Caprini score to stratify the risk of VTE in patients with nonorthopedic surgery, which involves many clinical predictive factors. 10 Besides, age, radiation, transfusion, and operative time are identified as possible risk factors for VTEs after oncologic surgery. 2 However, the biomarkers for predicting VTEs after oncologic surgery are still lacking. In this study, we have found that the plasma CD62P and the GP IIb/IIIa levels in patients receiving oncologic surgery are significantly higher than those in healthy volunteers preoperatively. The CD62P, GP IIb/IIIa levels in malignancy with VTE group were also markedly higher 7 days after operation compared with those in malignancy with no VTE group. Besides, the CD62P and the GPIIb/IIIa levels in malignant patients are markedly higher compared with those in benign patients preoperatively. These findings suggest that CD62P and GP IIb/IIIa may have clinical potential for predicting the risk of VTE after cancer surgery and cancer risk assessment and diagnosis.
The integrin GP IIb/IIIa signaling pathway is an important direction in the research of new anticoagulant drugs. 11 GP IIb/IIIa antagonists abciximab, tirofiban, lamifeban, and eptifibatide, have been developed but are used for percutaneous coronary intervention. 12 The GP IIb/IIIa is expressed in some cancer cells, such as MCF-7 breast cancer cells, squamous cell carcinoma, and malignant melanoma. The use of GP IIb/IIIa antagonist eptifibatide can significantly inhibit the activity of MCF-7 breast cancer cells. 13 In addition, the interaction of the integrin GPIIb/IIIa expressed on platelets and melanoma cells contributes to the molecular interface between these 2 cell types, which may be relevant for melanoma cell metastasis. 14 In patients with colon cancer, the occurrence of the mutation of the β3 structural gene is identified as an independent risk factor for VTE. 15 A nested matched case–control study has assessed the association between the evolving markers of platelet activation, such as soluble P-selectin (sP-selectin), soluble CD40 ligand (sCD40 L), thrombospondin-1 (TSP-1), and platelet factor-4 (PF-4), and the development of cancer-associated VTE. 16 Results show that sP-selectin but not sCD40 L, TSP-1, or PF-4 is associated with the risk of VTE in patients with cancer. These results may explain the significantly higher CD62P and the GP IIb/IIIa levels in patients receiving oncologic surgery than those in healthy volunteers preoperatively.
Whether the routine scanning for DVT is necessary in patients with cancer after surgery remains controversial because asymptomatic VTE may also cause a mortality event. 17 In this study, all the DVT events detected are symptomatic, and the plasma CD62P, GP IIb/IIIa, and D-dimer levels in patients with VTE are markedly higher 7 days after operation compared with those without VTE. The D-dimer is a marker of hypercoagulation and reflects increased thrombin generation and fibrinolytic activity. Although the D-dimer is highly sensitive, its specificity remains low because the D-dimer can be elevated in a multitude of medical conditions. Thus, a high D-dimer level alone is not sufficient to diagnose DVT. Further studies need be performed to investigate the diagnostic sensitivity and specificity of preoperative and postoperative CD62P and GP IIb/IIIa.
Different from other types of surgery, the relative risk after surgery for cancer remains high at the period of postoperative weeks 5–12. 18 The relative risks for VTE in cancer surgery significantly decrease after 3 months postoperatively. Thus, in this study, we have tested the D-dimer, CD62P, and GP IIb/IIIa levels 30 days after operation. We have found that the CD62P level 30 days after operation remains higher than those at 7 days after operation and preoperation, revealing platelet aggregation and activation after cancer surgery. These results may support the use of extended antithrombotic prophylaxis for cancer surgery.
Many abdominopelvic cancers are mostly asymptomatic until they progress to advanced stages. Thus, the early detection can have a pivotal role in reducing disease-related mortalities. Carbohydrate antigens are traditional biomarkers for abdominopelvic cancers. 19 Current studies have indicated that the circulating cell-free DNA, metastasis-related genes, circulating tumor cells, long noncoding RNAs, exosomes, and circular RNAs can be potentially used for the early diagnosis and the accurate prediction of therapeutic approaches. 20,21 In this study, the CD62P and the GPIIb/IIIa levels in malignant patients are markedly higher compared with those in benign patients preoperatively, suggesting the potential clinical application of CD62P and GPIIb/IIIa as helpful biomarkers or therapeutic targets in abdominopelvic cancers.
The character of the research was its greatest limitation. We could not perform sensitivity and specificity analysis and establishment of the cut-offs of the biomarkers in relation to ruling out a VTE event, so that we could not conclude that an elevated CD62P and the GP IIb/IIIa levels were associated with an increased risk of VTE in patients after cancer surgery. Since incidence of symptomatic DVT was relatively low in patients with cancer undergoing surgery, much more participants without VTE were needed for biomarkers’ tests. Their role of CD62P and the GP IIb/IIIa for predicting VTE events in patients after cancer surgery needs to be validated in further cohort studies.
Conclusions
In summary, this study demonstrates that the CD62P and the GP IIb/IIIa levels are elevated in patients before oncologic surgery. Improved therapeutic or prophylaxis schedule for VTEs after oncologic surgery targeting on GP IIb/IIIa signaling pathway or CD62P may improve the prognosis. The precise detection of the CD62P and the GP IIb/IIIa levels may provide a new choice for the early detection of malignancy. CD62P and GP IIb/IIIa monitoring should be widely promoted in clinics.
Footnotes
Authors’ Note
Qiang Guo conceived the idea for the study. Xin Zhong and Qiang Guo contributed to the design of the research. All authors were involved in data collection. Zhongze Cao, Jiayi Song, and Yuanmeng Liu analyzed the data. Qiang Guo coordinated funding for the project. All authors edited and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Science and Technology Project of the Health Planning Committee of Sichuan Province No.19PJ234.