
Abstract
The incidence and mortality of sepsis in the intensive care unit (ICU) are extremely high. Thrombocytopenia, one of the most common laboratory abnormalities, is correlated with prognosis in sepsis. The pathophysiology of sepsis-associated thrombocytopenia (SAT) remains unclear and may be associated with several factors such as platelet activation due to vascular injury and pathogen, suppression of bone marrow, platelet-targeted antibodies and desialylation. This review summarized all these possible mechanisms in the 3 subtypes of SAT: increased platelet consumption, reduced platelet production and increased platelet destruction. Based on the clinically available platelet parameters, the evidence for identifying SAT subtypes and the recent progress in treatments according to these subtypes are proposed to provide new prospects for the management of SAT.
Background
Sepsis-3 diagnostic criteria defined sepsis as organ dysfunction caused by an imbalanced host response to infection, while septic shock is defined as sepsis complicated by circulatory, cellular and metabolic disorders. 1 Although there is a large body of research on sepsis and the mortality of sepsis has declined in the last few years, 2 it is still one of the leading causes of death worldwide, mainly because of the unclear underlying mechanisms and lack of indicators for guiding clinical treatment. 3 Different studies have shown that platelets play pivotal roles in sepsis, 4,5 and thrombocytopenia is a risk factor for mortality in septic patients. 6 Thrombocytopenia commonly occurs in patients in the intensive care unit (ICU), with a prevalence of 8%-68% and an incidence of 13%-44% respectively. 7,8 A prospective observational study on medical ICU patients revealed that 67% of thrombocytopenia cases were caused by sepsis, indicating that sepsis is the leading cause of thrombocytopenia in critically ill patients. 9 More importantly, the rate of mortality in patients with sepsis-associated thrombocytopenia (SAT) increased. In a 6-year single-center study involving more than 1,100 patients, Azkárate I et al. found that thrombocytopenia was associated with a 1.7-fold increased risk of mortality in patients with sepsis. 10 The specific pathophysiology of SAT remains uncertain, and several mechanisms were indicated: platelet activation due to vascular injury and pathogen, marrow suppression, platelet-targeted antibodies and desialylation. 4,11 –13 Based on the clinical observation of the heterogeneous, even paradoxical changes in platelet-related laboratory parameters, we suppose firstly that the predominant mechanism of SAT may be diverse, and dividing SAT into several subtypes may be beneficial in establishing a more precise diagnosis and selecting the appropriate treatment. Considering the clinical convenience and effectiveness, we aimed to summarize the underlying mechanisms in the 3 subtypes: increased platelet consumption subtype, reduced platelet production subtype and increased platelet destruction subtype.
Subtypes of SAT
Increased Platelet Consumption Subtype
Pathogens can release multiple components and induce pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs) to initiate sepsis. With the direct or indirect effects of PAMPs and DAMPs, platelets activate and participate in pathological processes including complex interactions with innate immune cells, adhesion to the exposed vascular extracellular matrix, resulting in increased platelet consumption and eventually thrombocytopenia. 14 Moreover, Larkin CM et al. agreed that thrombocytopenia in patients with sepsis is partly related to platelet consumption. 15 Furthermore, increased platelet consumption was considered as the primary mechanism of SAT. 16
Some receptors, such as CD63 in lysosomes and CD62P in α-granule, can translocate from cytoplasmic organelles to the surface during platelet activation, providing the potential detectable biomarkers for platelet activation. Previous research revealed that the expression of CD63, CD62P and CD31 on the surface of platelets in SAT patients was significantly upregulated. 17 The up-regulation of CD62P, CD40 and other receptors enhances the interaction between platelets and vascular endothelial cells, or platelets and leukocytes, resulting in an increase in platelet aggregation and consumption. 4 Raque VX et al. reported high expression of toll-like receptor-4 (TLR-4) and protease-activated receptor-1 (PAR-1) on the surface of platelets in patients with sepsis. 18 Interestingly, thrombin-mediated platelet activation is among the most common mechanisms of platelet consumption, 11 of which the effect of PAR-1 is dominant. 19 Therefore, the up-regulation of platelet-activating receptors and consequently the increased platelet aggregation cause a large amount of platelet consumption, which ultimately leads to SAT development.
In addition, microparticles (MPs) released from activated platelets are involved in intercellular communication, thrombin formation and even activation of platelet at rest during the course of septic shock and heparin-induced thrombocytopenia. 20 Recently, Boscolo A and colleagues reported the overt association between the high level of platelet-derived MP (PMP) /platelet ratio detected in septic shock patients and disease severity. 21
Extensive cell injury, including vascular endothelial cell injury, can induce a systemic inflammatory response in patients with sepsis. When the integrity of vascular wall is damaged, the subendothelial structures expose and bind to glycoprotein (GP) Ⅰb-Ⅸ-Ⅴ complex in the platelet surface through the von Willebrand factor (vWF), which facilitates the adhesion between platelet and subendothelial matrix under a high blood flow shear. Ultra-large vWF multimers contain multiple sites that mediate the interaction among vascular endothelial cells, subendothelial matrix and platelets, and hence play an important role in platelet consumption. A high level of vWF antigen and propeptide can be detected in patients with sepsis, and the concentrations of circulatory ultra-large vWF multimers are related to the severity of the disease. 22 The size of the vWF multimers is regulated by the vWF-cleaving protease, also known as a disintegrin and metalloproteinase with a thrombospondin type 1 motif member 13 (ADAMTS13). Unfortunately, a previous research suggested that the release of a huge amount of ultra-large vWF multimers led to the consumption of ADAMTS13 in sepsis animal models. 23 The deficiency in the amount and activity of ADAMTS13 in patients with sepsis has a predictive value for the severity of disease (by Acute Physiologic Assessment and Chronic Health Evaluation [APACHE] II or other score systems) and mortality. 24 In those patients suffering from thrombotic thrombocytopenic purpura (TTP), the accumulation of ultra-large vWF multimers occurs due to the decrease in the level of ADAMTS-13 and thus results in persistent platelet consumption. Similar mechanisms also exist in the context of sepsis. 25
In addition to the platelet count (PC), the platelet-related parameters in blood routine examination include mean platelet volume (MPV), platelet distribution width (PDW), platelet larger cell ratio (P-LCR) and immature platelet fraction (IPF). MPV measures the average platelet volume, while PDW describes the variation in platelet size. P-LCR is representative of the percentage of platelet with a volume larger than 12 × 10−12 L. IPF is a measure of the percentage of immature platelets in peripheral blood, while the absolute immature platelet counts (AIPC) is calculated by multiplying the IPF by the PC (AIPC = PC×IPF).
Compared with the mature platelet, the immature one contains more dense granules, produces more TXA2, aggregates faster, has a larger size and a higher expression of membrane receptors such as CD62P and GPⅢa. The level of MPV, PDW and P-LCR elevates because of the increased proportion of immature platelets in the blood. If thrombocytopenia is not a result of myeloproliferative disorders, bone marrow hyperplasia leads to the release of immature platelets, which is manifested as an increase in IPF and AIPC. 26 Supernormal MPV and PDW were both associated with poor outcomes in adult patients with sepsis. 27 The high variation of MPV (ΔMPV) was related to the prolonged length of ICU stay. 28 According to a previous study, the difference in ΔMPV between 72 hours after admission and upon admission of septic non-survivors was significantly higher than that of survivors, and was positively correlated with the APACHE II score. 29 Oh GH et al. suggested that neither MPV nor PC was sufficient to accurately predict the 28-day mortality in patients with severe sepsis; however, the ratio of MPV to PC on admission and 24-hour after admission could both accurately predict the 28-day mortality in patients with severe sepsis. 30 Another study showed that the optimal cutoff value for predicting prognosis is 10.5 × 10−12 L (area under the curve, AUC = 0.812). 31
In general, the consumption subtype of SAT is presented as a high expression of platelet activation biomarkers including CD63, CD62P, CD31 and PAR-1, an increased level of PMP and vWF antigen, a decreased activity and level of ADAMTS13 and partly increased IPF, AIPC, MPV, PDW and P-LCR due to marrow hyperplasia.
Reduced Platelet Production Subtype
The process of platelet development undergoes multiple stages. Under the effects of stimulating factors, such as thrombopoietin (TPO), IL-6 and TNF-α, megakaryocytes are converted into proplatelets after proliferation and maturation in the bone marrow. The proplatelets are transformed into preplatelets (also called immature platelets), which are then released into the peripheral blood and develop into mature platelets after 24 hours. 32 Decreased platelet production may imply the direct suppression of bone marrow due to underlying diseases, pathogenic toxins, drugs, inflammatory mediators, 16 the attenuated bone marrow reactivity to TPO, impaired function of megakaryocytes or destruction of newly synthesized platelets in the bone marrow. 14
In a multicenter trial including 301 ICU patients (227 with sepsis and septic shock), bone marrow smears were obtained from 238 patients with laboratory-confirmed thrombocytopenia; results showed a reduction in platelet production in 17 patients (7%), suggesting that some SAT may result from marrow suppression. 33 The study did not dynamically record the platelet production in the bone marrow. Hence, a subgroup analysis was performed based on the severity of thrombocytopenia, which may partly explain for the low proportion of patients with decreased platelet production. Koyama K et al. found that there is a correlation between platelet production and the length of ICU stay in SAT patients, in a clinical trial enrolling 205 patients in the ICU. These patients were categorized into 4 groups according to the lowest PC within the first 7 days following ICU admission: severe (minimum PC≤40 × 10 9 /L), moderate (41–80 × 10 9 /L), mild thrombocytopenia (81–120 × 109/L) and normal-thrombocytosis group (> 120 × 109/L). Although the AIPF in the severe thrombocytopenia group was not significantly different from that of the other 3 groups on the first day, it quickly declined until the third day and did not recover to the levels of the other 3 groups on the seventh day, 14 indicating that reduced platelet formation may be more commonly observed in patients with severe thrombocytopenia with a dynamic change. Although Thiolliere F et al. recommended that sepsis was not a contraindication for bone marrow aspiration, 33 a marrow examination was not routinely performed in this patients group. To a certain extent, the lack of active surveillance for bone marrow aspirates may account for the insufficient evidence of this SAT subtype.
Reduced IPF was a useful marker of platelet production inhibition, 34,35 whereas AIPC was considered as a more beneficial indicator in recent literature. 36 Gondo K et al. suggested that if the platelet production depressed, MPV, PDW and P-LCR decreased because of the reduction in the proportional of immature platelets. 37 However, there was another research showing opposite result that the volume of young platelets increased, leading to the magnified MPV and PDW. 38
Nonetheless, we prompt a more acceptable criterion for the preliminary identification of reduced platelet production subtype of SAT: severe thrombocytopenia with decreased AIPF, IPF, MPV, PDW and P-LCR.
Increased Platelet Destruction Subtype
SAT is also implicated in increased platelet destruction, which is closely related to platelet apoptosis, autoimmunity-mediated destruction and increased platelet clearance by desialylation. Escherichia coli and Staphylococcus aureus isolated from the blood of sepsis patients can trigger endogenous platelet apoptosis by producing α-hemolysin and α-toxin to degrade pro-survival protein bcl-x and result in thrombocytopenia, delineating the potential mechanism of SAT caused by specific pathogens. 39,40 In addition, elevated platelet-associated immunoglobulin (PAIg) level was associated with sepsis and cardiopulmonary bypass, supporting that the immune system is involved in thrombocytopenia. 41 Furthermore, Semple JW et al. found that platelet phagocytosis was also enhanced in the presence of PAIg and led to increased platelet destruction, which may be one of the factors causing thrombocytopenia. 42
As a ubiquitous sugar acid compound, sialic acid exists at the ends of the GP chain on the platelet membrane, preventing platelet from destruction. Both endogenous and exogenous neuraminidase can be a catalyst of the desialylation of sialic acid-glycoprotein compounds. After desialylation, the exposure of β-galactose residues to the platelet surface can be recognized by the Ashwell-Morell receptor (AMR) of hepatocytes, soliciting platelet clearance. 43 A previous research found that platelet desialylation in sepsis patients with suboptimal PC is enhanced compared to that in patients with normal PC. 4 Another study showed that the release of neuraminidase increased in sepsis caused by Streptococcus pneumoniae, inducing exposure of β-galactose residues recognized by AMR and eventually evoking thrombocytopenia. 44
Therefore, the increased platelet destruction subtype of SAT is characterized by increased platelet apoptosis, amplified PAIg level and platelet desialylation, which may be clinically measured by relevant indexes.
Progress in Treatment of SAT
Undoubtedly, low PC in patients with sepsis is related to poor sequelae. However, whether the recovery of PC improves the prognosis remains controversial and there is a lack of persuasive evidence. Sepsis is defined as an organ dysfunction syndrome caused by the host abnormal response triggered by infection; hence, appropriate and adequate infection control is important in the treatment of SAT regardless of subtype. Platelet transfusion is also debatable and is recommended only in patients with severe thrombocytopenia or those with potential risk of severe bleeding. In addition, different studies have proposed kinds of strategies directed at managing the main mechanisms of SAT, such as ADAMTS13 supplement, recombinant human thrombopoietin (rhTPO) and neuraminidase inhibitor oseltamivi. 45 –47 Besides, it was postulated that treatments for immune thrombocytopenia (ITP) can also be applied to patients with SAT, such as immunoglobulin, glucocorticoid, immunosuppressant and plasma exchange. 48 The primary reason for various but consensus-less treatments may be that most of the studies were only focused on the overall SAT population without determining the pathogenesis based on the subtype; as a result, it was difficult to develop more precise treatments. Subtype-targeted treatment may prove the effectiveness of SAT reversal and sepsis prognosis.
Infection Control as the Basic Treatment
Anti-infection is the cornerstone of sepsis treatment. 49 The earlier the antimicrobial treatment is initiated, the lower the decline of platelets. 50 However, it is noteworthy that even after starting the antibiotic treatment, the microbial virulence factors may continue to exist in the microcirculation instead of instantly eradicating and damaging the platelet and vascular endothelial cells. 51 In addition, some antibiotics can cause thrombocytopenia per se, 52 such as linezolid 53 and vancomycin. 54 Therefore, other than the premise of adequate and appropriate anti-infection therapy, a pathophysiology-guided treatment is essential as well.
Platelet Transfusion
The threshold of prophylactic platelet transfusion (PPT) in current guidelines and expert opinions of SAT is <10 × 10 9 /L for those without significant bleeding, <20 × 109/L for those with a notable risk of bleeding and <50 × 109/L before surgery or invasive procedures. 55 Though therapeutic transfusion for patients with SAT and bleeding is definitely beneficial, 56 there is a lack of high-level evidence to confirm the effectiveness of PPT in SAT patients. Consequently, PPT must be more conservative. 57 It was remarkable that platelet transfusion poorly improved PC with the persistence of sepsis, 58 and inappropriate PPT was even associated with increased mortality and risk of thrombosis. 59 The effect of PPT in SAT remains controversial, so clinicians should fully assess the bleeding risk of SAT patients to avoid unnecessary PPT.
Strategies Based on SAT Subtypes
A feasible way to deal with the increased platelet consumption subtype of SAT is to replenish ADAMTS13 and limit the formation of ultra-large vWF multimers, thereby decreasing vWF-mediated binding between platelets and the subendothelial matrix. Although ADAMTS13 level can be recovered by plasma exchange, several problems may still occur, such as allergic reactions and infection risks. 45 In addition, a phase I clinical trial concerning recombinant human ADAMTS13 (rhADAMTS13) was conducted in patients with congenital TTP, revealing an upward trend in PC within 6 days in all 15 patients included. 60 To the best of our knowledge, only a few studies have been conducted to examine the rhADAMTS13 in SAT patients or animal model, further research is needed.
For patients with reduced platelet production subtype, the use of rhTPO and TPO-receptor agonist (TPO-RA) showed promising results. Wu Q and coauthors reported that subcutaneous injection of rhTPO (15000 u/d) for 5 days significantly improved the PC and reduced the need for platelet transfusion in patients with SAT, with an efficacy rate of 76.32%. 46 The latest study revealed that as a TPO-RA, high-dose eltrombopag (100 mg/d) can also ameliorate the PC decrease in 64.71% of SAT patients without adverse events observed. 61 In contrast to the findings of clinical trials, blocking TPO with a mouse TPO receptor-maltose-binding protein (mTPOR-MBP) dramatically prevented organ damage in animal experiments. 62 The underlying mechanism may be the diminution of immature platelets, from generation to release, as studies have shown that increasing immature platelets correlate with the higher mortality and disease severity. 63 Unfortunately, the small sample size resulted in less convincing findings; hence, the conduct of larger clinical trials and prognosis tracking are still needed. A recent systematic review involving 10 randomized controlled trials (RCTs) also agreed that although rhTPO appeared to benefit those patients with SAT, conclusions need to be verified exhaustively by performing additional multicenter RCTs. 64 Heretofore, 2 large-scale RCTs of SAT patients are ongoing, which will provide higher-quality evidence to confirm the efficacy and safety of rhTPO. 65,66
The presence of immune mechanisms in increased platelet destruction subtype provides the potential for immunoglobulins, glucocorticoids, immunosuppressants and plasma exchange. In addition, inhibiting the desialylation of platelets may become a novel and hopeful intervention for this subtype. As a neuraminidase inhibitor, oseltamivir combined with antibiotics can shorten the time of PC recovery in SAT patients and reduce platelet transfusion with an effective rate of 83.3% (45/54), which is higher than that in the control group [(antibiotics only), 65.4% (34/52), P = 0.045]. 47 Overall, 3 SAT Subtypes with major laboratory parameters and general and peculiar treatments are presented in Table 1.
1. Subtypes of SAT With Major Laboratory Parameters, General and Peculiar Treatments.
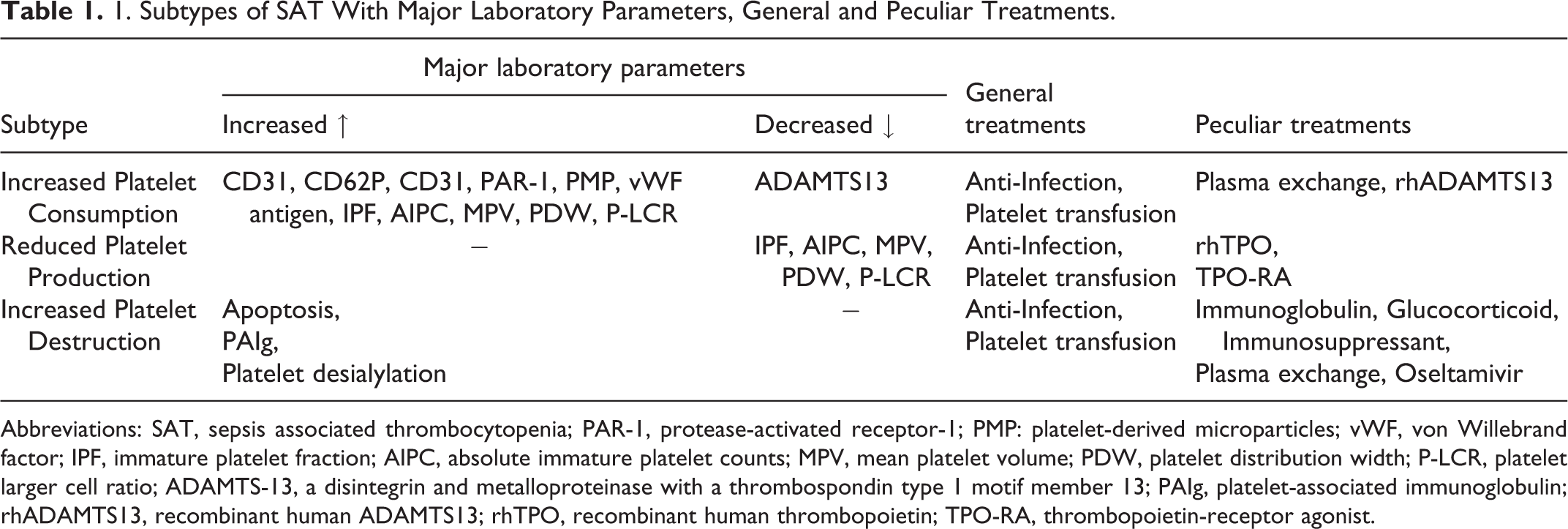
Abbreviations: SAT, sepsis associated thrombocytopenia; PAR-1, protease-activated receptor-1; PMP: platelet-derived microparticles; vWF, von Willebrand factor; IPF, immature platelet fraction; AIPC, absolute immature platelet counts; MPV, mean platelet volume; PDW, platelet distribution width; P-LCR, platelet larger cell ratio; ADAMTS-13, a disintegrin and metalloproteinase with a thrombospondin type 1 motif member 13; PAIg, platelet-associated immunoglobulin; rhADAMTS13, recombinant human ADAMTS13; rhTPO, recombinant human thrombopoietin; TPO-RA, thrombopoietin-receptor agonist.
Conclusions
The present review summarized the pathogenesis of SAT and attempted to categorize SAT into 3 subtypes based on the main mechanisms of SAT. Epidemiological investigation, diagnosis and treatment according to subtypes of SAT should be used in our clinical practice. The incidence, proportion and the difference in prognosis of SAT subtypes, as well as novel indicators and subtype-targeted precise treatment still need to be investigated.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No.81671896), the PLA Logistics Research Project of China (18CXZ032) and Guangdong Provincial Science and Technology Plan Project (Grant No.2017A020215055). The funding bodies had no specific role in the design of the review and manuscript writing.