
Abstract
Thrombosis has been recognized as one of the most significant risk factors of high mortality and disability in patients with Philadelphia (Ph) chromosome negative myeloproliferative neoplasms (MPNs). However, the risk factors of thrombotic events in these patients have not been completely understood. In this study, the clinical data of 58 patients with Ph-MPNs were obtained and analyzed, including 34 cases of essential thrombocytopenia (ET), 23 thrombotic events happened in 21 (36%) patients, among which 60% (14 of 23) with cerebral infarction, 17% (4 of 23) with coronary heart disease and 23% (5 of 23) with venous thrombosis. There were no significant differences in age, sex, and blood cell count between polycythemia vera (PV) and ET patients who have experienced thrombotic events and those who have not. In ET patients, the incidence of thrombotic events in plasminogen activator inhibitor-1 (PAI-1) genotype 4G4G was significantly higher than that in genotype 4G5G and genotype 5G5G (P < .05). The incidence of thrombotic events in PV and ET patients with infection was higher than those without infection (P < .05). Using logistic regression analysis, we found that PAI-1 genotype 4G4G and infection were associated with thrombotic events (odds ratio 6.744, 95% CI: 1.195-38.056 and 15.641 95% CI: 3.327-73.522). The 4G/4G polymorphism of PAI-1 gene and infection are independent risk factors of thrombotic events in patients with Ph-MPNs. PAI-1 gene 4G4G and infection in ET and PV patients with Janus kinase 2 (JAK2) V617F mutation were shown to be high risk of thrombotic events. Therefore, clinical doctors should put more attention on PAI-1 genotype 4G4G and infection in JAK2 V617F mutated patients with Ph-MPNs to prevent the thrombosis.
Keywords
Introduction
Myeloproliferative neoplasms (MPNs) are a group of hematological malignancies which have been featured in malignant clonal proliferation of multiple hematopoietic stem cells. 1,2 The classic Philadelphia chromosome negative MPNs (Ph-MPNs) include essential thrombocythemia (ET), polycythemia vera (PV), and primary myelofibrosis (PMF). 3,4 Janus kinase 2 (JAK2), thrombopoietin receptor (MPL) and calreticulin gene (CALR) mutations were found in more than 90% of patients with Ph-MPNs. 5,6 For now, the clinical presentation has often been accompanied by thrombosis, hemorrhage, hepatosplenomegaly, and higher rates of transformation to secondary myelofibrosis, bone marrow failure, and acute leukemia. 7,8 Thrombosis has been recognized as one of the most significant risk factors of high mortality and disability. 9,10 A number of studies have shown that the risk factors of thrombosis in patients with Ph-MPNs include advanced age, hyperlipidemia, hyperglycemia, hypertension, smoking, and positive JAK2V617F gene mutation. 11 –14 In addition, the incidence of thrombotic events in patients with positive JAK2V617F gene mutation is significantly higher than that in CALR-mutated patients, 15 –18 but the reasons have not been fully investigated.
Plasminogen activator inhibitor-1 (PAI-1) belongs to the serine protease inhibitor superfamily, which is the main regulator of fibrinolytic enzyme activation in vivo. 19,20 The increase in PAI-1 activity in vivo can inhibit normal fibrinolysis, which significantly trigger fibrin deposit, leading to thrombosis. 21 Due to the insertion or deletion of guanosine at 675 bp upstream of the transcription start site, a 4G/5G gene polymorphism, which exists in the promoter of PAI-1 gene can be found. 22 The genotypes of this gene polymorphism are 4G4G, 4G5G, and 5G5G respectively, which regulate the expression level of PAI-1. 23,24 Abundant existing studies have confirmed that genotype 4G4G is related to the increase in PAI-I gene transcription. 25 –27 As such, it is reason able to suppose that the plasma PAI-1 level is the highest in genotype 4G4G, which is followed by genotype 4G5G, and is the lowest in genotype 5G5G. 28
It is reported that the 4G/5G gene polymorphism and level of PAI-1 protein are closely related to arteriovenous thrombosis. 29,30 Farajzadeh et al 31 considered 4G4G as a risk factor of venous thrombosis. Tang et al 32 confirmed that the plasma PAI-1 level was an independent risk factor of deep vein thrombosis (DVT) after total hip replacement through a prospective study of 214 patients who have undergone total hip replacement.
In this study, firstly, we explore the association between PAI-1 gene polymorphism and thrombosis in patients with Ph-MPNs by analyzing the association between clinical features and thrombotic events in patients with Ph-MPNs. Besides, we further explored the risk factors of thrombotic events in patients with Ph-MPNs through the analysis of clinical data.
Materials and Methods
Patients Information
Fifty-eight (21 PV patients, 34 ET patients, and 3 PMF patients) patients with Ph-MPNs were recruited in this retrospective study, including 36 males and 22 females with an average age of 58.17 ± 14.09 (22-88) years. All of studied patients fulfilled the 2016 World Health Organization (WHO) criteria for the diagnosis of Ph-MPNs. This study complied with Declaration of Helsinki. All bone marrow samples were collected with informed consent, and the study was reviewed and approved by the Institutional Review Board of the Second Affiliated Hospital of Fujian Medical University.
The following clinical and laboratory data were collected: (1) patient demographics: sex, age, white blood cell count, hemoglobin levels, and platelet count; (2) clinical manifestations: thrombotic events identified on diagnostic imaging. Thrombotic events, including coronary heart disease, cerebral infarction, pulmonary embolism, DVT, and splanchnic vein thrombosis, which was diagnosed by color Doppler ultrasound or computed tomography or magnetic resonance imaging, angiography, and D-dimer levels. Infections, including sepsis, septicemia, pulmonary infection, urinary tract infection, and herpes virus infection; (3) mutation of Ph-MPNs driving gene (JAK2 V617F, MPL, and CALR); (4) the 4G/5G polymorphism of PAI-1 gene (4G4G, 4G5G, and 5G5G). The differences between driving gene mutations of Ph-MPNs, PAI-1 gene 4G/5G polymorphism, thrombotic events and infection were analyzed, respectively.
Detection of 4G/5G polymorphism of PAI-1 gene
Detection of PAI-1 gene 4G/5G polymorphism was performed according to the instructions of sequencing reaction kit (Beijing Huaxia times Gene Technology Development Co., Ltd). The performing steps are as follows: firstly, we add 1 mL 1× NH4Cl pretreatment solution into 1.5 mL centrifuge tube, which is followed by adding 200µL anticoagulant-treated whole blood in the same tube. After mixing, they will leave those tubes at room temperature for 5 minutes, and centrifuge for 5 minues at 3000 r/min. When most of the transparent red liquid in the upper layer is absorbed, put centrifuge for further 30 seconds at 3000 r/min until the transparent red liquid in the upper layer is absorbed; we add 100 µL 1×NH4Cl repeatedly and gently blow the impurities on the surface of white blood cells, remove the clean liquid in the upper layer liquid; add 30µL analysis preservation solution to the centrifuge tube with rich white blood cells, blow and mix successively. Lastly, we will take 1.5 µL treated white blood cell sample and add it to the gene detection reagent tube. Detection is then performed with fluorescence detector.
Detection of driving gene mutation type
Of all, 4 to 5 mL of bone marrow or peripheral blood of all recruited patients were collected. The mutation types of JAK2 V617F, JAK2 exon12, MPL W515L/K, and CALR exon9 gene were detected by polymerase chain reaction fragment analysis and Sanger sequencing as previously described. 5,33
Statistical analysis
SPSS version 20.0 statistical software was used to analyze the data. The measured data were expressed by X ± S. Fisher exact test and the χ2 test were used to compare categorical variables, and the Mann-Whitney U test was used for continuous variables. Logistic regression equation was used for statistical test. P < .05 was considered statistically significant.
Result
General Clinical Data of Patients With Ph-MPNs
In the samples of patients with Ph-MPNs, 23 thrombotic events were found in 21 patients (36%), among which 60% (14 of 23) were cerebral infarction, 17% (4 of 23) were coronary heart disease, and 23% (5 of 23) were venous thrombosis. In the sample of PV patients, the average age of patients experienced thrombotic events was 67.57 ± 7.79 years, including 4 males and 9 females; the average age of patients without thrombotic events was 53.93 ± 11.45 years, including 8 males and 4 females. There was no statistical difference in the incidence of thrombosis in PV patients with different sex or age (P = .51, P = 1). In ET patients, the average age of patients experienced thrombotic events was 59.67 ± 8.27 years, including 7 males and 5 females; the average age of patients without thrombotic events was 55.27 ± 18.03 years, including 14 males and 8 females. There was also no statistical difference in the incidence of thrombotic events in different sex and age in ET patients (P = .12, P = 1; Table 1).
Correlation Analysis of Clinical Data and Thrombotic Events in Patients With Ph-MPNs.a
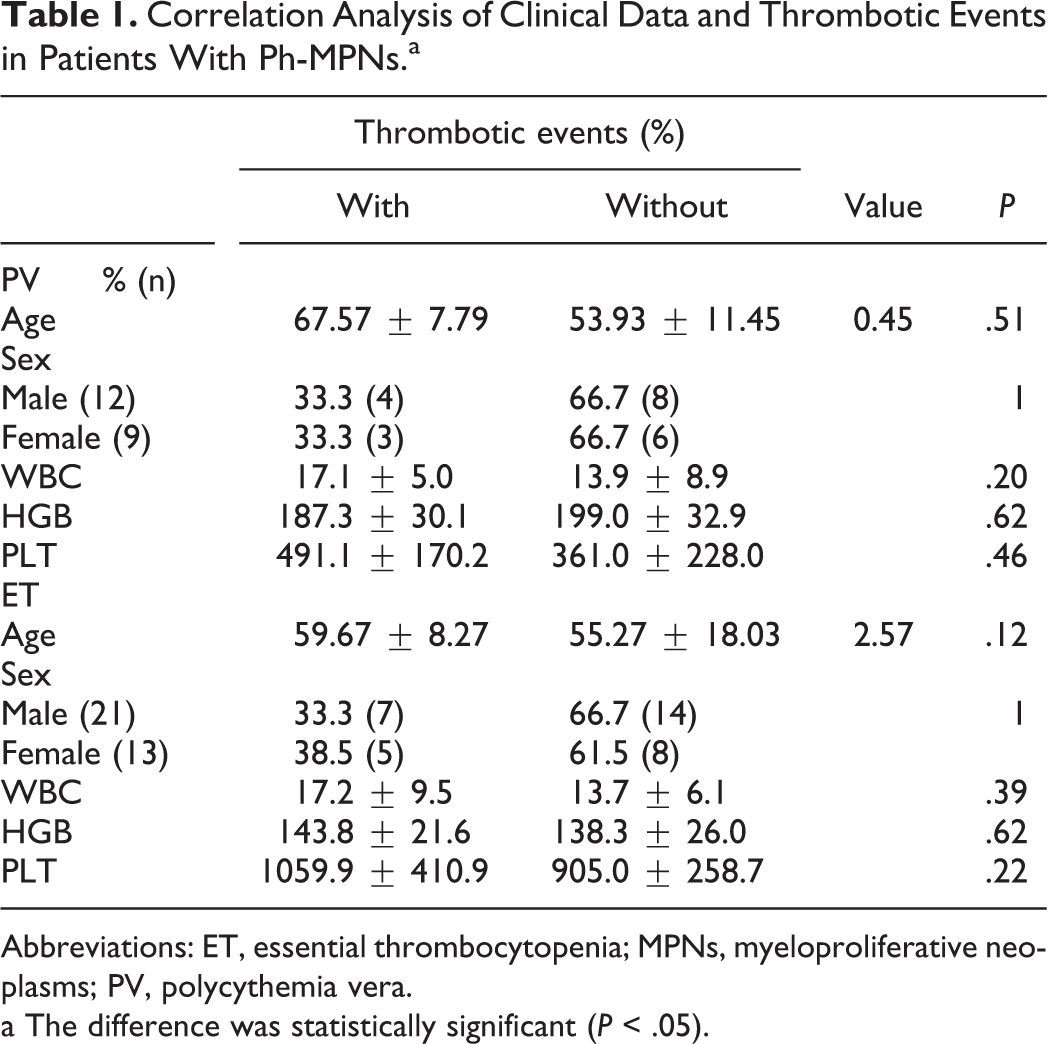
Abbreviations: ET, essential thrombocytopenia; MPNs, myeloproliferative neoplasms; PV, polycythemia vera.
a The difference was statistically significant (P < .05).
The Relationship Between Infection and Thrombosis in Patients With Ph-MPNs
In this study, the correlation between infection and thrombosis was analyzed. Among PV patients, the incidence of infection was 52% (11 of 21) with a total of 13 infections, among which 46% (6 of 13) were pulmonary infections, 31% (4 of 13) were viral infections, 15% (2 of 13) were urinary tract infections, and 8% (2 of 13) were sepsis. The incidence of thrombotic events in PV patients was 63.6% (7 of 11), all of them had concurrent infection, whereas there were no thrombotic events in patients without infections. Moreover, the incidence of thrombotic events in patients with infections was higher than that in those without infections, the difference between them was statistically significant (P = .004 < .05; Table 2).
Correlation Analysis Between Infection and Thrombosis.

Abbreviations: ET, essential thrombocytopenia; PV, polycythemia vera
In ET patients, the incidence of infection was 32% (11 of 34) with a total of 11 infections, among which 64% (7 of 11) were pulmonary infections, 9% (1 of 11) were sepsis, 9% (1 of 11) were urinary infection, 9% (1 of 11) were ear fistula infection and 9% (1 of 11) were trauma infection. The incidence of thrombotic events was 35% (12of 34), 63.6% (7 of 11) were with infections and 21.7% (5 of 23) were without infections. There was a significant difference between 2 groups (P = .015 < .05; Table 2).
Correlation Analysis Between PAI-1 Gene Polymorphism and Thrombosis
The correlation between PAI-1 genotypes and thrombotic events will be analyzed in this section. In PV patients, 4G4G, 4G5G, and 5G5G genotype accounted for 29% (6 of 21), 38% (8 of 21), and 33% (7 of 21) of all patients, respectively. While for patients with thrombotic events, 4G4G, 4G5G, and 5G5G genotypes were seen in 66.7% (4 of 6), 12.5% (1 of 8), and 28.6% (2 of 7), respectively. The incidence of thrombotic events in PAI-1 genotypes was 4G4G > 5G5G > 4G5G, but there was no significant difference among them (P = .06; Table 3).
Correlation Analysis Between PAI-1 Gene Polymorphism and Thrombosis.

Abbreviations: ET, essential thrombocytopenia; PAI-1, plasminogen activator inhibitor-1; PV, polycythemia vera
As for ET patients, 4G4G, 4G5G, and 5G5G genotypes accounted for 41% (14 of 34), 41% (14 of 34), and 18% (6 of 34) of all patients respectively. The incidence of thrombosis in 4G4G genotype was 50% (7 of 14), 35.7% in 4G5G genotype (5 of 14), and 0% in 5G5G genotype. The incidence of thrombotic events of PAI-1 genotypes was 4G4G > 4G5G > 5G5G, whereas the difference was not statistically significant (P = .3).
However, the incidence of thrombotic events in the PAI-1 4G4G genotype group was higher than 4G5G and 5G5G groups (P = .015; Table 3).
Correlation Between Ph-MPNs Driving Gene Mutation Type and PAI-1 4G/5G Polymorphism
The incidences rate of JAK2 V617F mutation gene in PV and ET patients were 77% (16 of 21), 79% (27 of 34), the mutation rates of CALR gene were 0%, 15% (5 of 34), and the rates of triple negative mutation were 23% (5 of 21) and 3% (2 of 34), respectively.
In PV patients, the incidence rate of PAI-1 genotype in JAK2 V617F gene mutation positive patients was 4G5G (37.5%) = 5G5G (37.5%) > 4G4G (25%). Compared with JAK2 V617F gene mutation negative patients, the difference was not statistically significant (P = .59; Table 4).
Correlation Analysis of Driving Gene Mutation Type and PAI-1 Gene 4G/5G Polymorphism.

Abbreviations: CALR, calreticulin gene; ET, essential thrombocytopenia; JAK2, Janus kinase 2; PAI-1, plasminogen activator inhibitor-1; PV, polycythemia vera
In ET patients, the frequencies of PAI-1 genotype were 4G4G (48.2%) > 4G5G (33.3%) > 5G5G (18.5%) in the patients with JAK2 V617F gene mutation. There was no significant difference compared to the patients with no JAK2 V617F gene mutation (P = .19), but there was significant difference compared with the patients with CALR gene mutation (P = .13; Table 4).
Correlation Analysis Between PAI-1 Gene Polymorphism and Infection
In this part, we will analyze the correlation between PAI-1 genotypes and the incidence of infection by comparing the differences of incidence of infection among PAI-1 genotypes.
As for PV patients, the infection rates of different PAI-1 genotypes were 4G4G > 5G5G > 4G5G, but the difference was not statistically significant (P = .12). In ET patients, the infection rates of different PAI-1 genotypes were 4G5G > 4G4G > 5G5G, but the difference was also not statistically significant (P = .64; Table 5).
Correlation Analysis Between PAI-1 Gene Polymorphism and Infection.
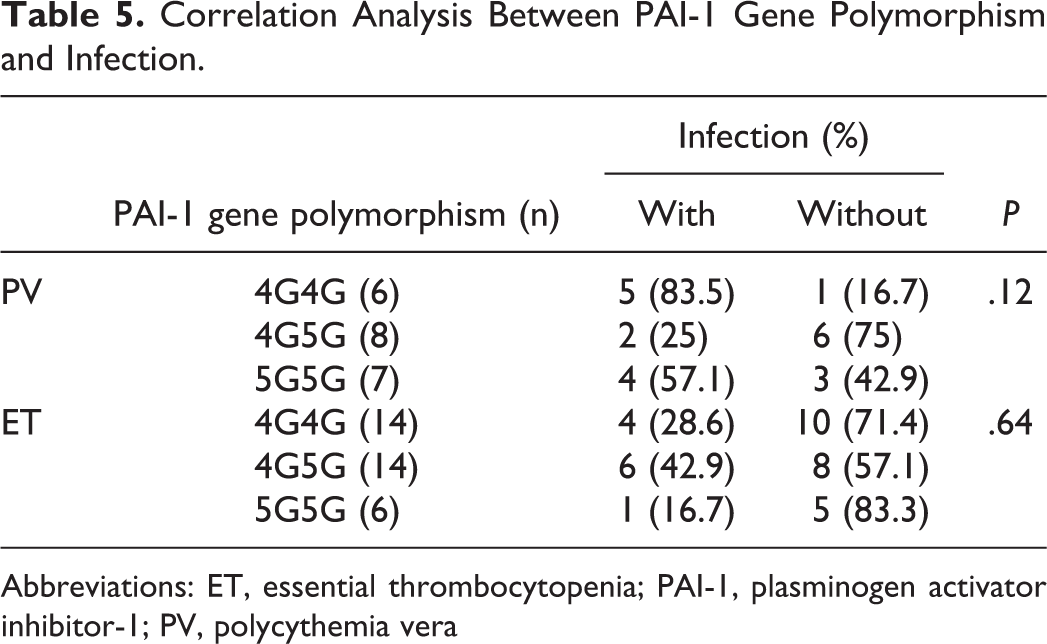
Abbreviations: ET, essential thrombocytopenia; PAI-1, plasminogen activator inhibitor-1; PV, polycythemia vera
Logistic Regression Analysis of Risk Factors Related to Thrombosis in Patients With Ph-MPNs
In logistic regression, the occurrence of thrombotic events was considered as the dependent variable, and confounding factors of JAK2 V617F gene mutation, PAI-1 genotype, infection status, sex, and age confounding factors were considered as the independent variables to analyze whether JAK2 V617F gene mutation, PAI-1 genotype, infection, sex, and age were the independent risk factors for thrombotic events.
Among them, PAI-1 was treated as a dummy variable, and 5G5G genotype was taken as the reference, engendering 2 dummy variables: PAI-1 (1) → 4G4G, PAI-1 (2) → 4G5G. In addition, 2 covariates, sex and age, were included in the analysis. Logistic regression was used to adjust the covariate effect, and then the gene polymorphisms of JAK2 V617F, PAI-1 and the correlation between infection and thrombotic events would be estimated. The regression coefficient of infection was 2.45, the Wald test result was P = .00 and odds ratio (OR) value was 11.60 (95% confidence interval: 3.25-41.44). The result was statistically significant, suggesting that infection was significantly correlated to thrombosis. The regression coefficient of PAI-1 genotype 4G4G was 1.91, the Wald test result was P = .03 and the OR value was 6.74 (95% confidence interval: 1.20-38.06). The results were statistically significant, indicating that 4G4G genotype was associated with higher incidence of thrombotic events. No correlation between 4G5G and 5G5G genotypes was observed since the P value Wald test for 4G5G and 5G5G genotypes were greater than 0.05. The OR values of infection, 4G4G genotype and JAK V617F mutation all changed after we adjust sex and age confounding factors, which suggested that the potential effects of sex and age should also be considered when we explored the correlation between infection, 4G4G genotype and JAK V617F mutation and thrombosis. Additionally, we speculated the P value in Wald test results of JAK2 V617F mutation, age, and sex were greater .05 (Table 6).
Logistic Regression Analysis of Risk Factors of Thrombotic Events.

Abbreviations: JAK2, Janus kinase 2; PAI-1, plasminogen activator inhibitor-1; OR, odds ratio.
Discussion
A total of 40% to 60% patients with Ph-MPNs experience thrombotic events, which are one of the most significant risk factors contributing to complications, high mortality and high disability rate. 9,10 As reported by previous studies, the incidence of cerebral arterial thrombosis is the highest, which dramatically affects the quality of life and survival period of patients. 12,13 In this study, the incidence of thrombotic events was the highest in 4G4G PAI-1 genotype group, which was followed by genotype 4G5G, and genotype 5G5G was the lowest. In PV patients, PAI-1 genotype 4G4G was also associated with the highest incidence of thrombotic events, but the difference was not statistically significant. The view that PAI-1 activity level and 4G/5G polymorphism of PAI-1 gene are closely related to arteriovenous thrombotic diseases has been widely recognized by previous studies. 34 –36 Tofler et al 37 prospectively investigated 3203 patients without cardiovascular diseases, and found out that the incidence of cardiovascular events was higher in patients with high PAI-1 levels. Akhter et al 38 reported that the increase in PAI-1 activity and genotype 4G4G were related to the occurrence of ischemic stroke in Indian population. Prabhudesai A et al 39 studies also showed that 4G4G genotype was an independent risk factor for DVT. The high incidence of thrombotic event in patients with Ph-MPNs with 4G4G genotype was consistent with the previous studies. Although, there has no statistical significance in patients with ET and PV separately.
We also found out that in PV and ET patients, the incidence of thrombotic events patients with infections was higher than that in those without infections, and the difference was statistically significant. As is widely acknowledged, infection and inflammation are predisposing factors for thrombosis, which is closely related to tissue factor exposure, endothelial cell destruction, platelet activation, changes in white blood cell, and red blood cell function. 40 Meanwhile, patients with cancer are more likely to suffer from thrombosis, since cancer cells can secrete a variety of coagulants, including inflammatory factors, which triggers off thrombosis. 41 The main function of PAI-1 in vivo is to inhibit t-PA and U-PA activity. Additionally, PAI-1 is an acute phase protein during acute inflammation, and inflammatory response significantly boost PAI-1 level. 42 Tumor necrosis factor-α,interleukin (IL)-1, IL-6, Transforming growth factor inflammatory mediators have been proved to stimulate PAI-1 production. 43 Therefore, we infer that the increased PAI-1 level in the plasma of patients with infections can promote the deposition of microvascular and extravascular fibrin, and then affect the fibrinolytic system in vivo, which predisposes patients to thrombosis. Apart from that, it is reported that chemokines and cytokines produced by inflammatory reaction cause genetic instability, leading to the occurrence and development of tumors, and play an important role in the pathogenesis of Ph-MPNs. 44 Therefore, it is reasonable to confirm that infection plays an important role in the development of thrombotic events in patients with Ph-MPNs. In this study, patients with various age, sex, and blood cell showed no significant difference in the occurrence of thrombotic events, which showed that PAI-1 gene 4G/5G polymorphism and infection were related to thrombotic events. Therefore, the PAI-1 gene polymorphism can be used as a routine screening item along with infection status in patients with Ph-MPNs to evaluate patients’ risk for thrombotic events in the future.
In addition, previous studies acknowledged that inflammation can lead to genetic instability; however, the relationship between infection and PAI-1 gene 4G/5G polymorphism needs further study.
The occurrence of thrombotic events is closely related to the prognosis of patients with Ph-MPNs. Some studies have shown that the incidence of thrombotic events in JAK2 V617F mutation positive patients is higher than that in CALR mutation positive patients. 10,45 However, the reason of it has not been fully investigated. In this study, we consider whether there is a potential relationship between the mutation type of Ph-MPNs driving gene and the polymorphism of PAI-1 gene in the occurrence of thrombotic events by comparing them. From the results of Table 4, it is found that the PAI-1 genotype 4G4G expression rate is the highest in ET patients with JAK2 V617F gene positive mutation, which is followed by the genotype 4G5G and the genotype 5G5G expression rate is the lowest. However, the expression rate of PAI-1 genotype with CALR gene positive mutation compared with JAK2 V617F mutated counterparts is not statistically significant (P = .13). More JAK2 V617F and CALR-mutated patients will be enrolled to further investigate whether the PAI-1 genotype is the risk factor of thrombotic events or not. The high frequency of PAI-1 genotype 4G4G in JAK2 V617F mutated patients leads to the high incidence of thrombotic events, which may be one of the reasons for the high incidence of thrombotic events in these patients. However, there is no significant difference between JAK2 V617F gene positive mutation and JAK2 V617F gene negative mutation.
The small numbers in the subgroups is the limitation of the study. As such, it is expected to expand the number of cases included in the study to better understand the risk factors of thrombotic events in patients with Ph-MPNs.
In conclusion, thrombosis is an important complication in patients with Ph-MPNs. The study clarifies that the PAI-1 genotype 4G/4G and infection are the risk factors of thrombotic events in patients with Ph-MPNs. Philadelphia chromosome negative MPNs patients with JAK2 V617F mutation can be further tested for PAI-1 genotype 4G/5G polymorphism. Besides, PAI-1 genotype 4G4G and infection in JAK2 V617F mutated Ph-MPNs patients should attract more attention in thrombosis prevention in the future.
Footnotes
Authors’ Note
XYZ, XRC, and JXP conceived and designed the study. XYZ and XRC conducted study procedures (patient recruitment, blood sampling). XYZ and XRC collected data. XYZ and XRC analyzed the data. XYZ and XRC interpreted the results. XYZ XYZ wrote the first draft of the manuscript. XYZ, XRC, and JXP contributed to the writing of the manuscript. The study was approved by the local ethics committee (ethics committee of the Second Affiliated Hospital of Fujian Medical University) and conducted in accordance with the declaration of Helsinki.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Fujian Province [grant number 2018J01278].